
Abstract
Urologists face a significant challenge when presented with cases in which complete, yet reversible, urinary diversion is desirable. With multidisciplinary collaboration, we have used a novel technique involving the antegrade deployment of distally-ligated covered metal (Allium®) ureteral stents, achieving ureteral occlusion and complete urinary diversion via nephrostomy tubes. We have used this technique, with good early results, in complex cases, including that of a young male patient with complex pelvic injuries after polytrauma and a female patient with a malignant vesicovaginal fistula, neither of whom were candidates for definitive surgical reconstruction or diversion at the time of treatment. We describe our experience, which we believe may be of interest to urologists and interventional radiologists managing similarly challenging cases.
Introduction
Urinary diversion may be indicated in a number of clinical scenarios. In some of these, definitive surgical reversal, for example, by ileal conduit formation, 1 is not appropriate, either because a temporary reversible solution is sought or because patient or disease factors preclude major surgical intervention. However, complete, reversible, antegrade urinary diversion is challenging to achieve. Although this is often attempted with the insertion of bilateral percutaneous nephrostomies, 2 this approach does not produce complete diversion when performed in the context of unobstructed ureters.
Having been confronted by this clinical challenge several times, we have developed and utilized a technique that overcomes many limitations of alternative management strategies. By performing a bench modification of expandable metal stents, followed by their antegrade ureteral deployment and placement of nephrostomy tubes, we have achieved complete, reversible urinary diversion.
Discussion of the technology
This technique was developed as a collaboration between colleagues in interventional radiology and endourology. To begin, modification of a covered metal stent is performed ex vivo, to create a removable ureteral occlusion device. Our experience involves use of the Allium® Ureteral Stent (Allium Ltd.), which is a self-expandable, covered metal stent. We have used size 10 × 120 mm stents for this purpose.
In the first instance, ultrasound-guided percutaneous renal access is obtained, with creation of a nephrostomy, if one is not already in place.
Once nephrostomy access has been effectively obtained, the covered metal stent is prepared on the operating table. The metal stent, within its delivery system, is passed through a 10F vascular access sheath. The olive tip of the delivery system is removed, by a transverse cut with a scissors. Partial deployment of the stent is performed, exposing the distal end. The exposed end is then ligated, approximately 10 mm from the edge, with a hand-tied 1,0 polyethylene terephthalate (Ethibond®) suture (Fig. 1). The modified stent is then reverse loaded back into the 10F sheath, ready for use. If bilateral ureteral occlusion is required, as is often the case, this process is repeated on a second stent.
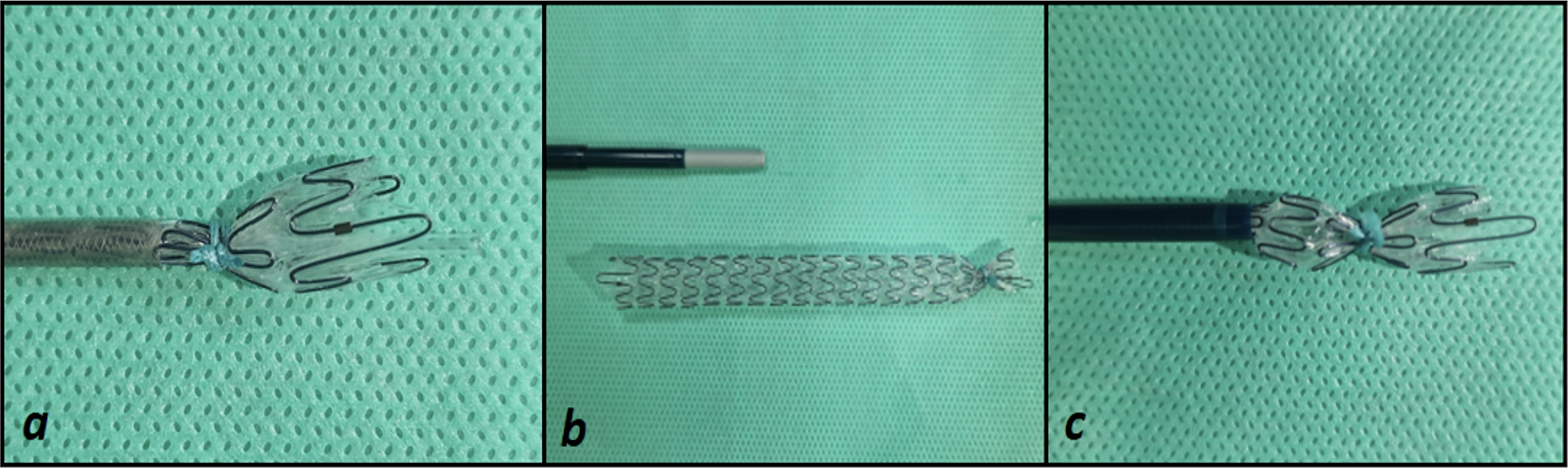
Bench modification of self-expandable metal stents. This figure presents an ex vivo image of a covered self-expandable metal stent after bench modification:
The nephrostomy tract is dilated to accommodate a 12F vascular access sheath, which is placed in the tract. The modified ureteral stent is then deployed antegradely via this 12F vascular access sheath, under fluoroscopic guidance, advanced to the level of the distal ureter, and deployed.
The metal stent is allowed to expand, and an antegrade nephrostogram is then performed, to confirm appropriate positioning of the metal ureteral stent, and adequate occlusion to the passage of contrast, without peri-stent or trans-luminal leakage (Fig. 2). A nephrostomy tube, typically an 8.5F locking pigtail, is placed on free drainage. The procedure is repeated on the contralateral side, when bilateral diversion is required.

Subsequent nephrostograms. This figure shows a still fluoroscopic image of bilateral nephrostograms performed after antegrade deployment of bilateral self-expandable metal stents, ligated distally to result in ureteral occlusion. This patient had suffered complex pelvic trauma, with an open-book pelvic fracture evidenced here by the disruption of the symphysis pubis visible on this image.
Our experience
We have applied this technique in two recent challenging cases that presented to our institution.
The first was a 32-year-old male patient, who presented to our regional trauma unit after a fall from an approximately 27 m (90-foot) height, resulting in complex blunt polytrauma. He sustained multiple musculoskeletal injuries, including an open-book pelvic fracture with an associated extraperitoneal rectal injury and American Association for the Surgery of Trauma 3 Grade 4 posterior urethral injury. His management was made more difficult by morbid obesity (body mass index [BMI] 45.71 kg/m2). He was managed according to trauma principles 4 and with a multidisciplinary team approach. His urological management was challenging. He underwent laparoscopic placement of a suprapubic catheter, at the time of defunctioning colostomy, followed by bilateral 8.5F nephrostomy insertion. However, despite nephrostomy and suprapubic catheter drainage, he developed complex pelvic fistulation and infection with confirmed urine leakage via a pelvic drain. CT abdomen/pelvis with cystogram (Fig. 3) demonstrated an inability to distend the urinary bladder, with persistent large volume contrast extravasation tracking to the anterior abdominal wall skin surface.

Computed tomography (CT) cystogram. This figure shows a contrast-enhanced CT abdomen and pelvis combined with a CT cystogram, with contrast instillation via the suprapubic catheter. Failure to distend the bladder (a + b), and contrast extravasation (b), with tracking to the abdominal wall (a), are demonstrated.
In response to this, the nephrostomy tubes were upsized to 12F, rendezvous urethral access was obtained, and a urethral catheter was sited in addition to the suprapubic catheter. However, the urine leak persisted, necessitating a novel total occlusion of the ureters to achieve full antegrade diversion.
The technique described above was performed, with antegrade placement of a modified Allium stent, achieving complete urine diversion via the nephrostomy tubes. After this, the pelvic drain output dropped immediately and was subsequently removed, with healing of the cutaneous fistulae seen. At 16 weeks, and again at 28 weeks after stent insertion, bilateral nephrostograms were performed, confirming the persistence of adequate ureteral occlusion, and exchange of nephrostomy tubes was performed.
The second case was of a 64-year-old female patient, with a vesicovaginal fistula (VVF) secondary to metastatic gynecological malignancy, for which systemic treatment was ongoing. Her quality of life was significantly impaired by continuous incontinence with large volume leakage, despite a urethral catheter. Given her overall health status because of metastases and limited prognosis, attempted surgical repair of VVF was not deemed appropriate. She underwent bilateral antegrade insertion of modified Allium stents, using the technique described, with bilateral nephrostomy tubes inserted. Nephrostograms confirmed good occlusion of distal passage of contrast, and her incontinence was improved. X-ray KUB at 8 weeks postinsertion confirmed the appropriate position of the Allium stents. At 3 months postinsertion, she passed away from her disease, with stents in situ.
Role in endourology
Temporary, reversible urinary diversion can be desirable in a range of clinical scenarios. These include ureteral obstruction, malignancy with potential for curative treatment, 2 postsurgical anastomotic leaks, 5 traumatic injury to the lower urinary tract, 6 lower tract fistulae,7,8 severe cases of bladder dysfunction, 9 and refractory radiation cystitis. 10
In cases of ureteral or distal obstruction, nephrostomy tubes usually achieve satisfactory urinary diversion when required. However, where there is loss of integrity of the lower urinary tract with extravasation or fistulization, complete urinary diversion becomes more challenging to achieve if surgical reconstruction is not possible. In the first case presented above, a large-sized lower urinary tract defect because of complete disruption of the membranous urethra, further complicated by poor tissue healing in the context of ongoing pelvic sepsis, meant that attempts to achieve urinary diversion with bilateral nephrostomies, a suprapubic and urethral catheter, were ultimately inadequate. A pelvic environment completely free from urine was clearly desirable, to allow resolution of pelvic collections and fistulization. It was felt that forming an ileal conduit would have been an exceptionally challenging procedure, in view of this patient’s BMI and concomitant injuries. Furthermore, in a trauma patient of a young age with uncertainty about the long-term outcomes, any urinary diversion technique undertaken was required to be potentially reversible at a later date. The Allium stents described can be removed using ureteroscopy in an antegrade or retrograde manner.
In the second case described above, disease factors and the need to rapidly resume systemic treatment meant that VVF repair or formal surgical urinary diversion were not appropriate.
In the absence of an established technique for ureteral occlusion in this context, several options have been tried and reported in the literature. Many have significant limitations. Antegrade ureteral embolization, using embolization coils, along with histoacryl or NBCA (N-butyl-cyanoacrylate) glue,11,12 has been described. This is expected to incite a ureteral inflammatory process, resulting in fibrosis and stricture formation with “complete and permanent occlusion.” 13 Ureteral occlusion utilizing AmplatzTM vascular plugs has also been reported,14,15 although often with a requirement for additional glue or coil deployment to achieve complete dryness, and with a small number of recanalization occurrences necessitating repeat treatment. This too is considered an irreversible treatment and has largely been described in palliative settings. Urinary diversion by means of urethrally exteriorized 5F ureteral stents alongside a urethral catheter has been proposed as a temporizing measure in the instance of a protracted anastomotic leak postradical prostatectomy. 5 This technique may not be feasible in cases of complex lower urinary tract trauma and would be unlikely to achieve complete diversion. Balloon catheters have been used with a view to achieving temporary ureteral occlusion. Small case series describe antegrade passage of small Fogarty or angioplasty balloon catheters with ureteral balloon inflation.16,17 These have been used for only limited time periods, with mean dwell time of 23–94 days,16,17 and limitations include relatively frequent spontaneous balloon deflation and requirement for readjustment, alongside risks of migration and potential concerns of ureteral pressure necrosis. 18 We have previously utilized balloons within covered metal stents to reduce the risk of ureteral wall stricturing, but found the current strategy more technically straightforward.
We describe effective total ureteral occlusion using modified Allium stents resulting in complete urinary diversion via nephrostomy tubes. We acknowledge the limited number of patients to date, but feel that the technique is promising and merits sharing with other clinicians. We also acknowledge the relatively short follow-up period (4 months), but feel that it is adequate to suggest efficacy of an intervention intended primarily as a short- to medium-term measure, as a proof of concept. We have extensive experience with the use of Allium stents for other indications. Although failure of stent removal, should removal or replacement become desirable, is at least a theoretical risk of Allium stent use, we have found tissue ingrowth to be uncommon, and removal of the stents to generally be straightforward, with postremoval ureteral patency confirmed in our experience, consistent with the experiences of other authors. 19 Our removal technique involves retrograde ureteroscopy, if the anatomy of the urinary tract permits, and gentle traction via a ureteroscopic grasping forceps. If a retrograde removal is not possible, antegrade ureteroscopy and removal via the nephrostomy tract are performed. Supplementary Figure S1 shows a ureteroscopic view of an Allium stent during removal. Accordingly, we are confident of the reversible nature of this intervention. Stent migration is a recognized risk of Allium stent use, with a migration rate of as much as 27% reported. 20 It has been noted that a significant risk factor for migration is a higher glomerular filtration rate of the stented kidney. 20 We would, therefore, anticipate a lower migration rate with patent nephrostomy diversion; however, nonetheless advocate close follow-up with a view to stent replacement if position becomes suboptimal.
Our ongoing management plan for patients with modified Allium stents in situ is tailored toward the individual patient, but includes regular clinical review and regular (average 12 weekly) nephrostomy tube changes with antegrade nephrostograms. Although significant encrustation of these stents is not common in our experience because of the polymer coating, we note that the risk may increase in this context, because of urinary stasis within the stents, and possibly because of the presence of the ligation suture, although it should have minimal contact with urine if full occlusion is achieved, as it sits on the external side of the stent. Accordingly, we are performing interval unenhanced CT (CT-KUB) as part of our monitoring strategy. If significant encrustation were to occur, our management strategy would be ureteroscopic stent removal, with laser lithotripsy if necessary, and stent replacement if felt appropriate, depending on the time interval to encrustation, overall management goals, and patient preferences. Allium stents are licensed to remain in situ for as much as 3 years. Although this technique is most likely to be used for shorter intervals, stent replacement would be possible after removal.
Conclusions
There is limited evidence to guide attempts to achieve complete, reversible urinary diversion. With multidisciplinary collaboration, we have used a novel technique involving the antegrade deployment of distally-ligated covered metal (Allium) ureteral stents, achieving ureteral occlusion and complete urinary diversion via nephrostomy tubes. We believe our experience may be of interest to urologists and interventional radiologists managing similarly challenging cases.
Authors’ Contributions
Conception: S.M.C., N.E., A.L., C.S., M.S., R.W., and A.R. Design: S.M.C., R.W., and A.R. Supervision: M.S., R.W., and A.R. Data collection: S.M.C., N.E., A.L., C.S., M.S., R.W., and A.R. Analysis: S.M.C., M.S., R.W., and A.R. Literature review: S.M.C., N.E., A.L., and C.S. Writing first draft: S.M.C. Reviewing draft: N.E., A.L., C.S., M.S., R.W., and A.R.
Footnotes
Author Disclosure Statement
None of the authors has any conflict of interest to declare in relation to this article.
Funding Information
S.M.C. is an endourology fellow at the Freeman Hospital Newcastle on a Richard Steeven’s Scholarship (Health Service Executive of Ireland) and supported in the role by a David Thompson Fellowship (The Urology Foundation).
Supplemental Material
Abbreviations
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.