
Abstract
Purpose:
To evaluate the safety and efficacy of a novel combined retrograde intrarenal surgery (RIRS) technique utilizing a tip-bendable suction ureteral access sheath (S-UAS) and ±20° gravity-assisted (Trendelenburg/reverse Trendelenburg) supine positioning for treating renal stones ≥3 cm.
Methods:
A retrospective multicenter study (3 centers) was conducted in 73 patients between October 2023 and January 2025 with renal stones ≥3 cm. A two-phase surgical approach was employed: initial lithotripsy in 20° Trendelenburg position, followed by fragment evacuation in 20° reverse Trendelenburg using S-UAS suction. All procedures utilized flexible ureteroscopy and a 12/14F S-UAS. Perioperative variables—including operative time, hemoglobin drop, need for second-stage procedures, 3-month stone-free rate (SFR), and complications (fever, subcapsular hematoma, and septic shock) graded by the Clavien–Dindo system—were recorded.
Results:
A total of 73 patients (mean stone size ∼34 mm) were included. Mean operative time was 125 ± 39 minutes. A second-stage RIRS was required in 32.9% of cases. The overall SFR at 3 months was Grade A (60.3%), Grade B (90.4%), and Grade C (97.3%) after one or two sessions. Postoperative fever occurred in 12.3% and subcapsular hematoma in 1.4% of patients; one patient (1.4%) developed urosepsis (septic shock, Clavien IVa) requiring intensive care unit care. No patients had long-term sequelae or required open surgery. On subgroup analysis, patients with high stone density (≥700 Hounsfield units) had higher second-stage RIRS rate.
Conclusion:
RIRS with a tip-bendable suction sheath combined with gravity-assisted supine positioning (±20° Trendelenburg/Reverse Trendelenburg) for renal stones appears to be a feasible option for managing stones >3 cm and may be particularly suitable for lower-density calculi. Further studies are needed to validate its effectiveness and safety in broader populations.
Introduction
Urolithiasis is a common condition worldwide, and large renal stones often necessitate surgical intervention. Percutaneous nephrolithotomy (PCNL) is considered the first-line treatment for renal stones larger than 2 cm because of its high stone-free rate (SFR).1–3 However, retrograde intrarenal surgery (RIRS) has gained traction as a less invasive alternative, even for stones over 2 cm. 4 Studies comparing RIRS and PCNL indicate that although PCNL achieves higher single-session SFRs for large stones, multiple RIRS sessions can yield comparable overall clearance with lower morbidity.
Despite these advances, RIRS for large stones still faces significant challenges. Reported SFRs vary widely, and many patients with stones ≥2–3 cm require multiple procedures to achieve complete clearance. Moreover, high intrarenal pressure during RIRS can increase the risk of complications such as infection and sepsis.5,6 To address these limitations, one major technological innovation is the suction ureteral access sheath (S-UAS). 7 This novel device connects to a vacuum source and features a flexible tip, enabling active evacuation of stone fragments and reducing intrarenal pressure during RIRS. Early clinical reports suggest that using S-UAS can enhance fragment clearance and improve SFRs, especially in patients with a larger stone burden. 8
Additionally, gravity-assisted supine positioning (±20° Trendelenburg/Reverse Trendelenburg) has been explored to improve RIRS outcomes. Performing RIRS in a Trendelenburg or reverse Trendelenburg position leverages gravity to prevent fragments from accumulating in inferior calyces and facilitates their drainage toward the ureteral sheath.9,10 Clinical studies report that such positioning can increase SFRs and reduce the number of sessions needed for larger stones, without raising complication rates. 11 Our team recently reported improved outcomes using S-UAS with ±20° positioning in stones up to 3 cm; however, stones ≥3 cm pose unique challenges that have not been specifically examined. However, managing renal stones exceeding 3 cm remains difficult. 3 There is still a paucity of high-level evidence supporting RIRS for stones ≥3 cm, and these large calculi often necessitate staged surgeries or alternative approaches. 12
In light of this gap, we designed the present study to evaluate the efficacy and safety of an enhanced RIRS strategy for stones ≥3 cm, incorporating both S-UAS and gravity-assisted supine positioning (±20° Trendelenburg/Reverse Trendelenburg). We aimed to determine whether these adjunctive techniques can improve RIRS outcomes for large stones, potentially approaching the success rates achieved with PCNL.
Methods
Study design and patient selection
We performed a multicenter retrospective review of consecutive patients who underwent RIRS with a tip-bendable S-UAS for renal stones ≥3.0 cm in maximum diameter. Three high-volume urology centers contributed cases between October 2023 and January 2025. Institutional review board approval was obtained at each center, and informed consent was waived because of the retrospective nature of the study. All procedures were performed by three senior endourologists from the participating centers, each with over 10 years of experience and high annual RIRS volumes. To ensure consistency, all surgeons adhered to a standardized protocol involving the use of the tip-bendable S-UAS combined with ±20° body positioning for both the lithotripsy and fragment retrieval phases.
Inclusion criteria were adult patients with preoperative noncontrast computed tomography (NCCT)-verified renal stones ≥3 cm in cumulative burden. Exclusion criteria included: (1) untreated urinary tract infection; (2) severe orthopedic or cardiopulmonary comorbidities precluding Trendelenburg positioning; (3) conversion to percutaneous or open surgery; and (4) significant ureteral strictures or anatomical abnormalities precluding sheath placement. All patients underwent preoperative assessment including history, physical examination, laboratory tests (e.g., urine culture), and imaging to determine stone size, number, location, and density. Urinary tract infections were treated and sterilized per institutional protocols before surgery.
Stones were categorized into two groups based on density: low density (<700 Hounsfield units [HU]) vs high density (≥700 HU). We selected 700 HU as the cutoff for practical purposes—it provided two comparably sized groups in our cohort—even though prior studies suggest ∼750 HU as a fragmentation efficiency threshold. This slight adjustment in threshold did not affect the overall trends. 13
Surgical technique
All procedures were performed under general anesthesia in the dorsal lithotomy position using an adjustable operating table. After guidewire placement under fluoroscopy, a tip-bendable S-UAS (12/14F) was advanced to the renal pelvis or target calyx; when resistance was encountered, we gently up-sized or performed brief semirigid Ureteroscopy predilation (1–2 weeks). A flexible ureteroscope was introduced through the sheath, and a two-phase “dusting-first” technique was used to optimize fragmentation and clearance (Fig. 1):
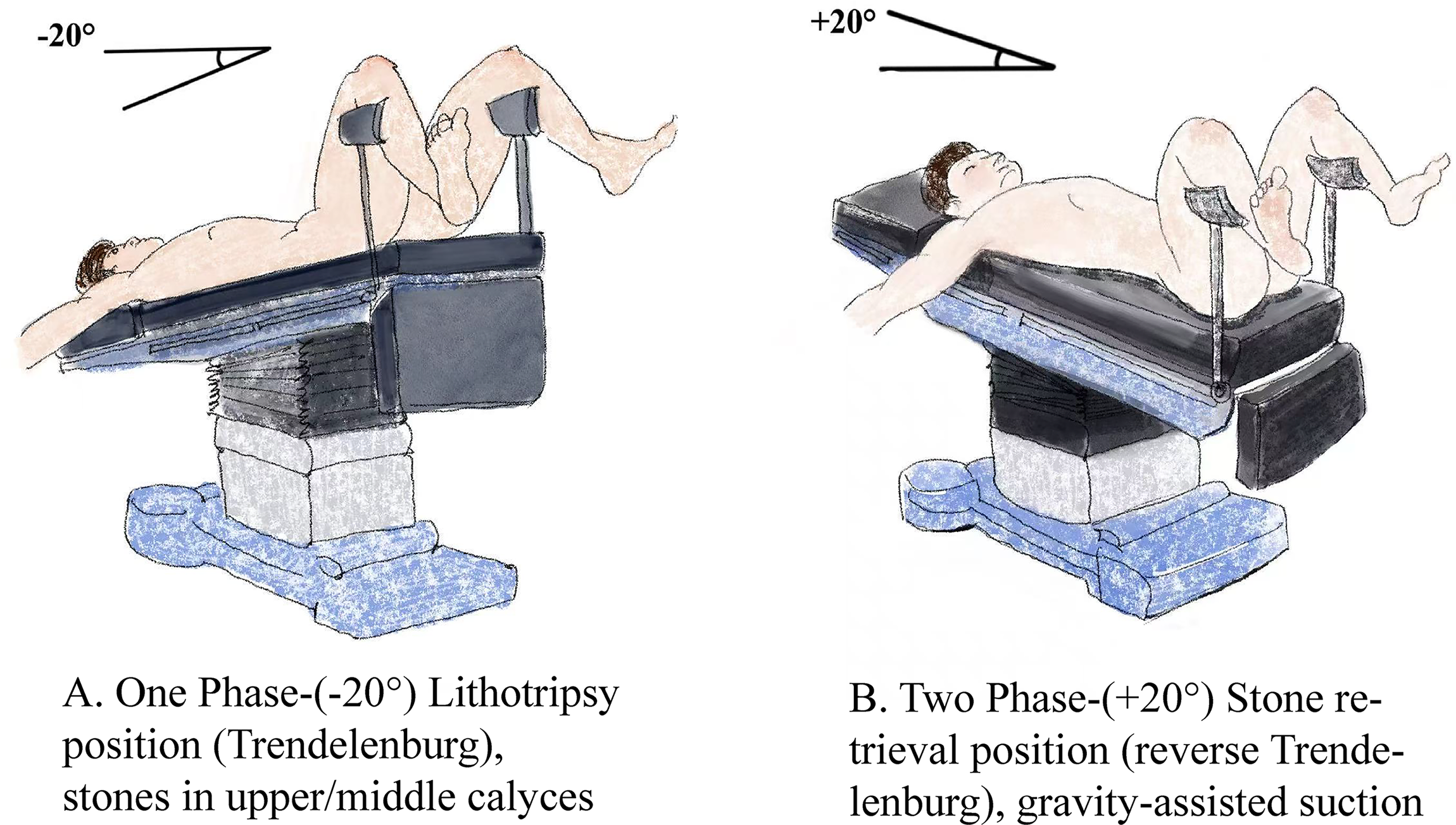
Illustration of surgical positioning during RIRS in the study. RIRS = retrograde intrarenal surgery.
Phase 1: Lithotripsy (Trendelenburg, 20° head-down; Fig. 1A):
With the table tilted 20° head-down, lithotripsy was performed under continuous irrigation and active suction via the tip-bendable S-UAS (regulated negative pressure). A holmium:YAG laser in dusting mode at a fixed setting of 0.8 J × 30 Hz was used throughout this phase. During dusting, fine debris (“stone dust”) was simultaneously aspirated through the S-UAS, helping maintain a clear field and low intrarenal pressure. Routine basketing was avoided to preserve visibility and efficiency; a nitinol basket was used selectively to relocate fragments or whole stones from unfavorable lower-pole positions to upper/middle calyces when access or deflection was suboptimal. If visualization deteriorated, limited fragment removal through the sheath was permitted to restore a clear field. The aim of Phase 1 was to reduce the stone to dust/fine debris while maintaining low intrarenal pressure.
Phase 2: Fragment evacuation (reverse Trendelenburg, 20° head-up; Fig. 1B):
The table was then tilted 20° head-up. Continuous suction via the S-UAS, combined with gravity, promoted downward movement of stone dust and small fragments into the sheath. Irrigation flow was adjusted to facilitate debris evacuation. Stone baskets were used selectively to reposition fragments to more accessible calyces.
At the end of the procedure, residual stones were evaluated endoscopically, and a ureteral stent was placed at the surgeon’s discretion (Supplementary Video S1).
Data collection and analysis
Patient demographics, stone characteristics, and operative details were extracted from records. Data collected included age, sex, stone size, location, and density, as well as operative parameters (total time, sheath diameter, etc.). Intra- and postoperative complications were documented and graded according to the Clavien–Dindo classification. Statistical analyses were performed using standard software: continuous variables were expressed as mean ± standard deviation or median (interquartile range) and compared by t-test or Mann–Whitney U-test as appropriate; categorical variables were compared using chi-square or Fisher’s exact test. For subgroup analysis, outcomes were compared between high-density stones (≥700 HU) and low-density stones (<700 HU). This cutoff was chosen based on prior evidence correlating higher HU with lower fragmentation success. 13 We assessed whether stone density influenced operative time, SFR, second-stage necessity, or complication rates. All analyses were conducted with SPSS v26.0 (IBM Corp.) or equivalent statistical software.
Outcome assessment and follow-up
Residual stone fragments were assessed using NCCT scans (1 mm slice thickness), and stone-free (SF) grade was categorized into: Grade A (no stones on CT scan), absolute SF, Grade B (Grade A stones plus ≤2 mm fragments) relative SF, Grade C (Grade A and B stones plus 2.1–4 mm fragments) relative SF, and Grade D as ≥4 mm fragments (not SF). Clinical follow-up also included assessment of any ancillary procedures and recording of perioperative morbidity.
Given the irregular morphology of many stones in this cohort, we did not apply the standard ellipsoid volume formula. Instead, stone volume was estimated using ITK-SNAP software by manually outlining the region of interest on sequential CT slices, which provided a more individualized approximation based on three-dimensional reconstruction (Supplementary Fig. S2).
Patients not achieving adequate clearance on initial RIRS were scheduled for a second-stage RIRS, typically 2–4 weeks after the initial procedure. Final SF status at 3 months was assessed after completion of any planned second-stage procedure.
Results
Patient and characteristics
Seventy-three patients with large renal stones (≥3 cm) were included (Supplementary Fig. S1). The median age was approximately 55 years (range ∼30–75), and mean body mass index was about 27.7 kg/m2. All patients had single or multiple renal stones with a median maximal diameter of ∼34 mm on preoperative imaging. The median stone density was around 778 HU (Table 1).
Patient Demographics and Baseline Characteristics
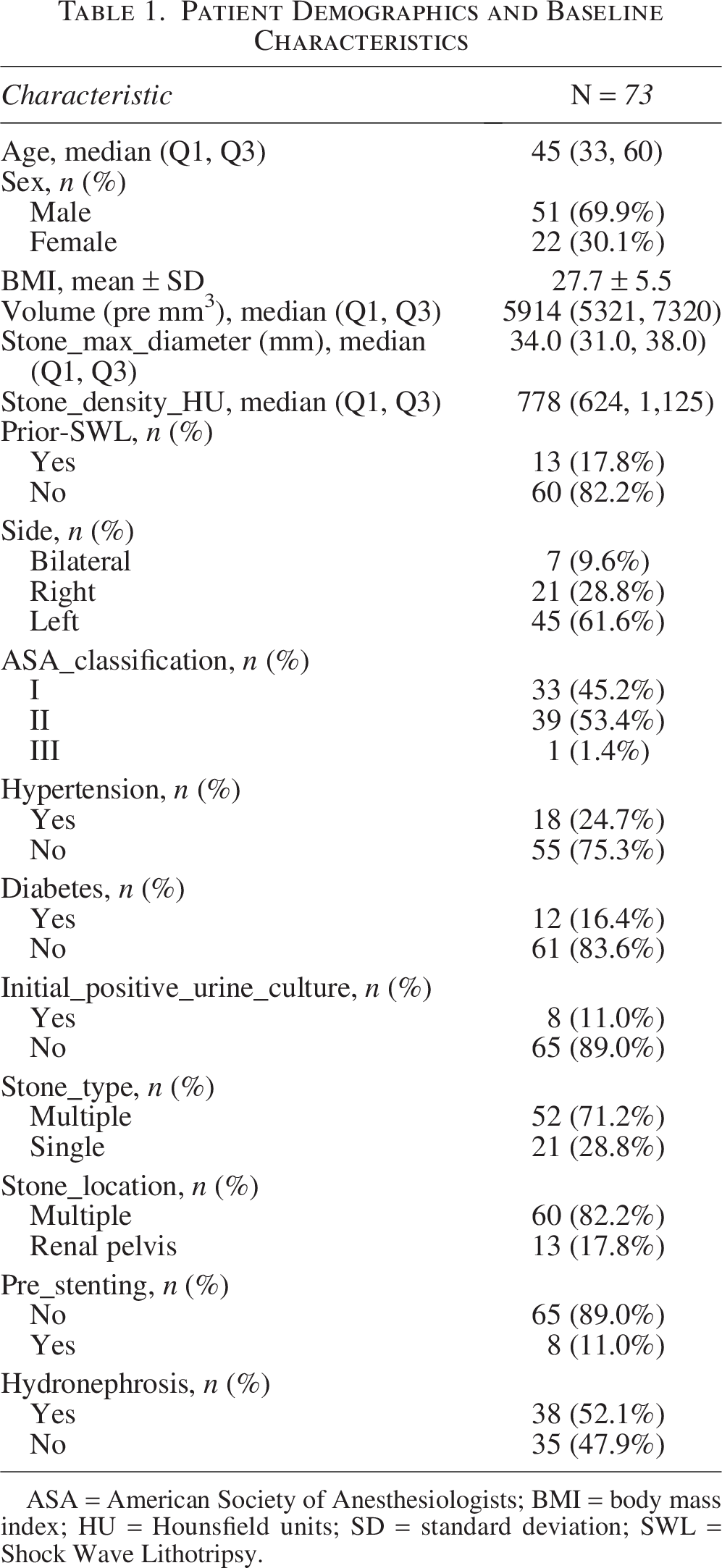
ASA = American Society of Anesthesiologists; BMI = body mass index; HU = Hounsfield units; SD = standard deviation; SWL = Shock Wave Lithotripsy.
Operative outcomes
All procedures were performed by experienced surgeons, with patients positioned in a ±20° gravity-assisted (Trendelenburg/reverse Trendelenburg) supine position. A tip-bendable S-UAS was used in every case. The mean operative time was approximately 125 minutes, and mean postoperative hospital stay was roughly ∼3 days. No patient required blood transfusion, and all ureteroscopic procedures were completed uneventfully with the use of the S-UAS. Perioperative morbidity was low. Nine patients (12.3%) developed postoperative fever, all of whom were treated with antibiotics. One patient (1.4%) developed a small subcapsular renal hematoma, which resolved spontaneously without intervention. Another patient (1.4%) developed septic shock postoperatively and was treated in the intensive care unit. No other major complications occurred (Table 2).
Overall Postoperative Outcome
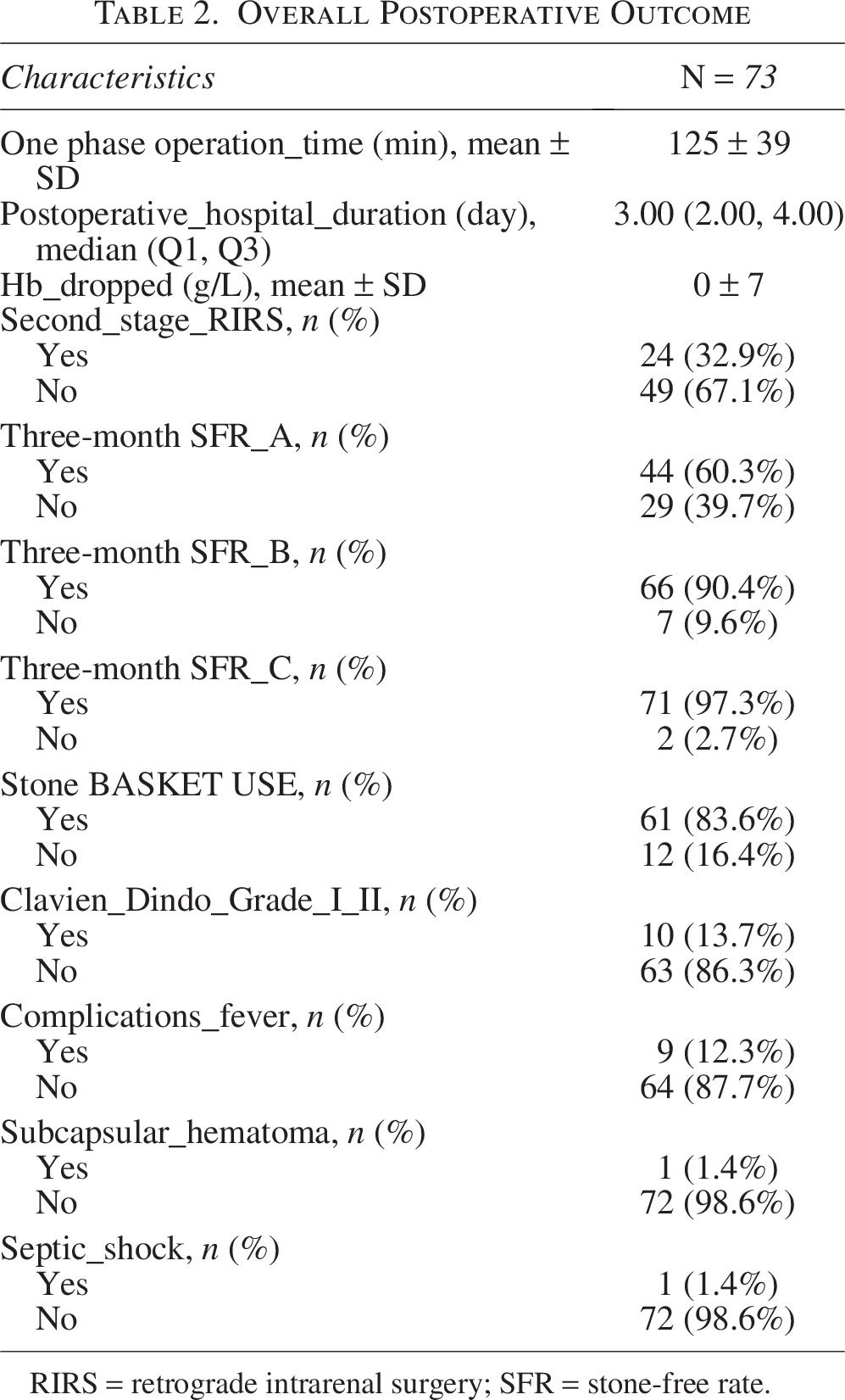
RIRS = retrograde intrarenal surgery; SFR = stone-free rate.
SF outcomes
At 3-month follow-up, NCCT imaging showed excellent stone clearance. Forty-four patients (60.3%) achieved complete clearance (Grade A), and two patients (2.7%) had residual fragments ≥4 mm (Grade D, not SF). The overall SFR (better than Grade C) at 3 months was 97.3%. A planned second-stage RIRS was performed in 24 patients (32.9%; Table 2).
Subgroup analysis by stone density
Patients were stratified by stone density into high-density (≥700 HU, n = 39) and low-density (<700 HU, n = 34) groups. Operative time was similar between groups (128 ± 42 vs 121 ± 34 minutes, p = 0.454). Second-stage RIRS was more frequently required in the high-density group (46.2% vs 17.6%, p < 0.01). The Grade A SFR was slightly higher in the low-density group compared with the high-density group (64.7% vs 56.4%, p = 0.47). Combined Grade A + B SFR also favored the low-density group (94.1% vs 87.2%, p = 0.438). Basket use was frequent in both groups (88.2% vs 79.5%, p = 0.314). However, these results are no significantly statistical differences. Postoperative complications occurred at similar rates in both groups, including fever (11.8% vs 12.8%, p > 0.999) and the single case of septic shock. One patient also developed a subcapsular hematoma. Overall, both subgroups achieved satisfactory outcomes, although denser stones may present slightly greater procedural challenges (Table 3).
Subgroup Postoperative Outcome (Stone Density)
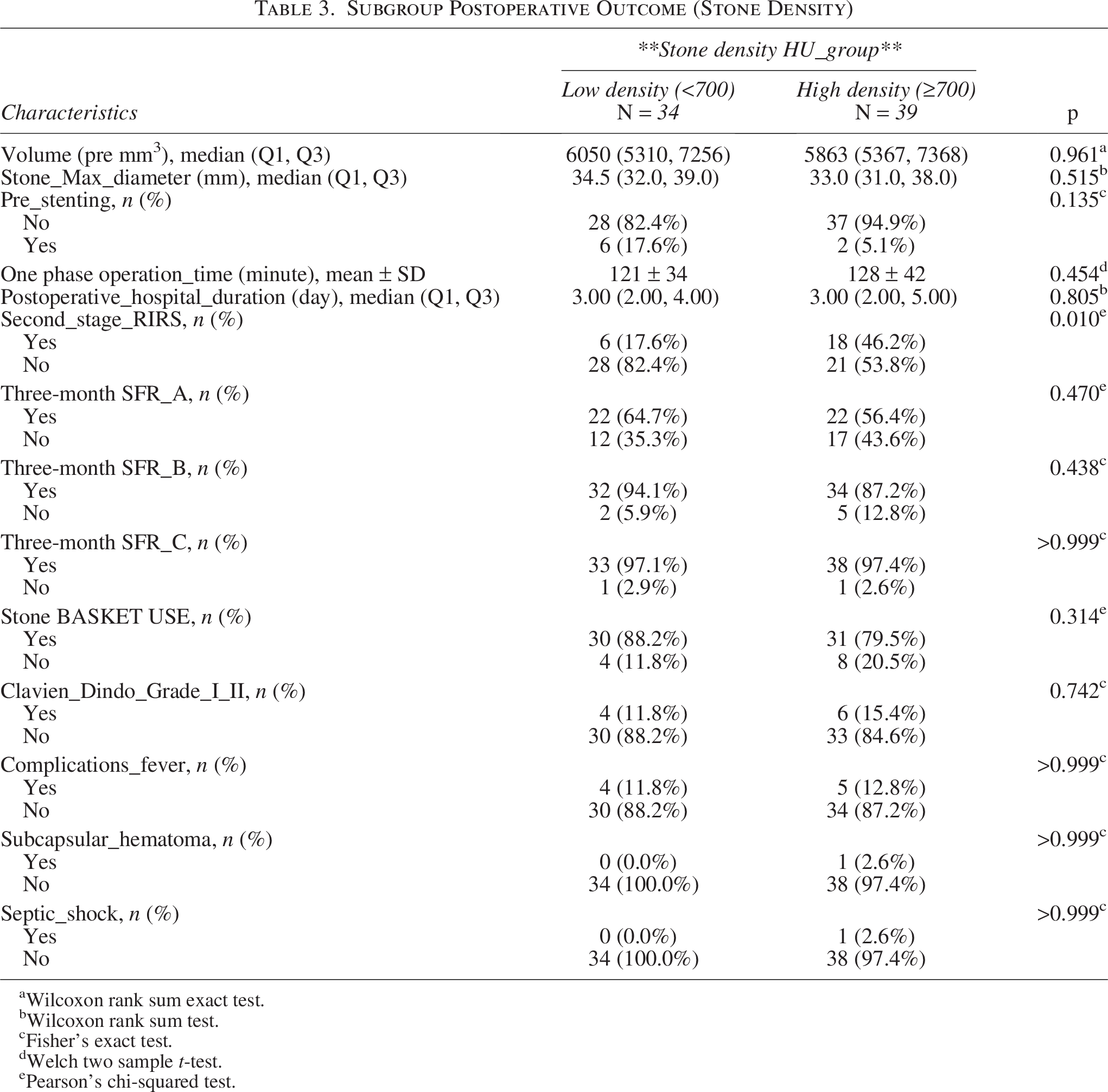
Wilcoxon rank sum exact test.
Wilcoxon rank sum test.
Fisher’s exact test.
Welch two sample t-test.
Pearson’s chi-squared test.
Discussion
Managing renal stones larger than 3 cm endoscopically presents a formidable challenge—PCNL remains the gold standard for its high clearance rates, but it carries notable risks: significant bleeding (with transfusion rates up to ∼55%) and other complications such as urinary leaks and even pleural injury.14,15 By contrast, RIRS is a flexible ureteroscopic approach through the natural urinary tract and is far less invasive. Multiple analyses show RIRS yields shorter hospital stays and lower morbidity than PCNL. For example, a systematic review found that all comparative trials reported reduced hospitalization time with RIRS vs PCNL, 16 and the majority showed fewer overall complications with RIRS. 16 In practice, this translates to less blood loss and quicker recovery, which often drives the preference for RIRS in clinical practice. (Indeed, European guidelines still favor PCNL for stones ≥2 cm, 17 reflecting traditional practice.) However, the steady advance of ureteroscopic technology has extended RIRS even into the 2–3 cm range. For example, one study reported SFRs around 73.6% when RIRS was applied to 2.0–3.5 cm stones. 16 Taken together, these data emphasize that RIRS’s reduced invasiveness makes it an appealing alternative for moderately large stones, with the potential to challenge the traditional PCNL threshold.
Recent innovations have sought to push RIRS boundaries further. In particular, the use of a tip-bendable S-UAS has shown clear benefits. A multicenter randomized controlled trial found that S-UAS dramatically improved stone clearance compared with a standard UAS, achieving an immediate SFR of 81.3% vs 49.4% and a 3-month clearance of 87.5% vs 70.0%. 5 Even more strikingly, adding gravity-assisted positioning augments these gains. Our approach, integrating a tip-bendable S-UAS with ±20° gravity-assisted positioning, aimed to overcome these limitations, the “±20° gravity-assisted position improves immediate SFR” in RIRS, and that combining this tilt with S-UAS is an “effective strategy” to optimize outcomes. Taken together, the combination of suction access and gravity-assisted tilt is especially promising for mid-size stones (2–3 cm) and may even extend RIRS utility into the ≥3 cm range. Interestingly, the rate of postoperative fever in our ≥3 cm cohort (12.3%) was not higher than in our prior series with 2–3 cm stones (∼15%). This could be attributed to the effective suction reducing intrarenal pressure and bacterial load even in large-stone cases, although this difference might also be because of sample size and patient selection. 3 In other words, these techniques may allow RIRS to safely address stones at sizes traditionally reserved for PCNL.
In the present study, we applied RIRS with a suction UAS and ±20° gravity tilt to renal stones ≥3 cm. Our preliminary findings suggest this approach is feasible and yields encouraging results. We observed high stone-clearance rates after a single session and a low incidence of major complications, indicating that RIRS with S-UAS and positional adjustment can approach the outcomes of more invasive techniques in this demanding cohort. Notably, the overall second-stage requirement was 32.9%; however, it was markedly lower in the low-density subgroup (17.6%) than in the high-density subgroup (46.2%). The ∼3-day mean stay—longer than an overnight ureteroscopy—reflects our centers’ policy of keeping large-stone patients under observation for early complications before discharge. It should be noted that although gravity-assisted supine positioning (±20° Trendelenburg/Reverse Trendelenburg) aids fragment evacuation regardless of stone composition, the fundamental challenge of harder stones remains the slower fragmentation. In our series, higher-density calculi (≥700 HU) inherently required more laser energy and often a staged approach, which explains their lower single-session clearance. Conversely, lower-density (softer) stones fragmented readily, allowing gravity and suction to clear debris in one session more often. We chose 700 HU because it produced two groups of comparable size; re-running the analysis with the 750 HU threshold proposed by Aksoy et al. 13 yielded a similar trend, suggesting that modest changes in the cutoff do not meaningfully alter our overall observations. After completion of a planned second stage, both density groups achieved satisfactory SFRs, underscoring the value of a staged strategy when residual fragments persist. These data imply that modern enhancements to RIRS—particularly the combination of suction-access sheaths and gravity-assisted supine positioning (±20° Trendelenburg/Reverse Trendelenburg)—may replicate some benefits traditionally associated with PCNL while potentially reducing its morbidity. For patients with lower-density stones, this protocol appears more likely to achieve single-stage clearance with acceptable safety, whereas a preplanned second stage can still deliver favorable final outcomes in denser stones. Although preliminary, our results support the feasibility of this technique for selected patients with large renal calculi (≥3cm); confirmation in larger, prospective studies remains necessary.
This study has important limitations. It was a retrospective, multicenter study (three centers) with a relatively small sample and no randomized control group (no formal power calculation was performed). Our analysis was exploratory in nature and that the results should be interpreted with appropriate caution given the sample size. Imaging follow-up was limited (no routine early postoperative CT scan), so immediate clearance may have been under- or overestimated. There may have been selection bias in case inclusion, and although all surgeons were highly experienced endourologists, the adoption of a new device/technique could entail a learning curve that might have subtly influenced outcomes (e.g., efficiency improvements as familiarity grew). Considering these caveats, our results must be interpreted with caution. Larger, prospective studies will be needed to confirm these findings. In fact, a recent systematic review notes that many existing comparisons of RIRS and PCNL suffer from sample size and design limitations, and they call for well-powered prospective trials to validate the evolving trends. 16 Future research should include multicenter trials or registries to evaluate suction-assisted, gravity-assisted RIRS in a more rigorous fashion.
In summary, RIRS offers a less invasive alternative to PCNL, with lower risks of bleeding and shorter hospitalization. 16 The addition of suction UAS and gravity-assisted patient positioning appears to further improve stone clearance and operative efficiency. Our study suggests this combined technique is feasible for large stones, with encouraging SFRs. However, given the limitations noted, these conclusions must remain tentative; further evidence is required before altering practice. Overall, our findings indicate that suction- and tilt-enhanced RIRS has potential as a safe and effective treatment for even large renal calculi, warranting additional study.
Conclusion
RIRS with a tip-bendable suction sheath combined with gravity-assisted supine positioning (±20° Trendelenburg/Reverse Trendelenburg) for renal stones appears to be a feasible option for managing stones >3 cm and may be particularly suitable for lower-density calculi. Further studies are needed to validate its effectiveness and safety in broader populations.
Authors’ Contributions
M.-H.W. and X.Z. were responsible for study design, data analysis and interpretation, and article writing. M.-H.W., H.L., and X.-L.Z. contributed to data collection. All authors approved the final version of the article.
Footnotes
Funding Information
No funding was received for this article.
Ethics Statement
This study was approved by the Ethics Committee of Beijing Chaoyang Hospital and was carried out in accordance with the ethical principles outlined in the Declaration of Helsinki. All patients provided written informed consent before participation in the study. The confidentiality of patient information was maintained throughout the study, and all personal identifiers were removed from the data to protect patient privacy. The study was conducted with the highest level of integrity and adherence to ethical standards (DXZXY20230608).
Data Availability
Declaration of Generative AI and AI-Assisted Technologies in the Writing Process
During the preparation of this work, the authors used ChatGPT 4.0 in order to improve the readability and language of the article in the writing process. After using this tool/service, the authors reviewed and edited the content as needed and take full responsibility for the content of the published article.
Authors’ Disclosure Statement
The authors declare no conflicts of interest for this article.
Supplemental Material
Supplemental Material
Supplemental Material
Supplemental Material
Supplemental Material
Supplemental Material
Supplemental Material
Supplemental Material
Abbreviations
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.