
Abstract
Purpose:
We aim to determine if ureteral rest is necessary prior to distal ureteral reconstruction with reimplantation with or without psoas hitch and/or Boari flap.
Methods:
We retrospectively reviewed all patients who underwent ureteral reimplantation at a single institution from December 2016 to April 2023. We included all reimplantation techniques, including psoas hitch and Boari flap. Patients were stratified based on if they had ureteral rest, defined as the absence of a ureteral stent for at least 4 weeks prior to the operation. Patient demographics, stricture characteristics, and perioperative outcomes were compared between the two groups. Patients were scheduled for 3 and 12 month postoperative ultrasounds to assess for stricture recurrence. Renal scintigraphy was used if significant or worsening hydronephrosis was seen.
Results:
Our cohort consisted of 50 patients, among whom 29 (58%) underwent ureteral rest before reimplantation. Demographics, stricture characteristics, and use of psoas hitch and/or Boari flap were comparable between the two groups. Stricture etiology was significantly different in patients with and without ureteral rest (p = 0.002). The cohort without ureteral rest had a higher percentage of radiation-induced ureteral injury (47.6%), while the cohort with ureteral rest had a higher percentage of iatrogenic ureteral injury (75.9%). Other/idiopathic causes were split relatively evenly. Median follow-up for the cohort was 8.6 months (interquartile range: 4.6–17.4 months). Postoperatively, there were no significant differences in 30-day complication rate, postoperative hydronephrosis, or stricture recurrence rate.
Conclusions:
Our data suggest that ureteral rest does not confer an advantage for distal ureteral reconstruction. Thus, operation should not be delayed in order to achieve ureteral rest when reimplantation is expected.
Introduction
Urethral rest prior to urethral stricture repair is now the standard of care and included in updated urologic professional guidelines. 1 Urethral rest allows for tissue recovery and stricture maturation needed for an accurate assessment and repair, while urethral instrumentation has been shown to profoundly alter stricture characteristics.2,3 Application of this same principle has been put forth in ureteral reconstruction. 4 While recent studies have demonstrated the advantage of ureteral rest in repairing proximal and mid-ureteral strictures, there is little evidence on the utility of ureteral rest prior to distal ureteral stricture repair.5,6 We hypothesized that ureteral rest may not confer an advantage in this setting given that the stricture is completely bypassed during a repair. Here, we present the results of a retrospective study aimed at assessing if ureteral rest was associated with better postoperative outcomes after ureteral reimplantation.
Materials and Methods
We performed a retrospective review of all patients who underwent ureteral reimplantation with a single surgeon at our institution between 12/19/2016 and 4/11/2023. This study was approved by the Washington University in St. Louis IRB. We included all patients who underwent ureteral reimplantation with or without a psoas hitch and/or Boari flap. Ureteral rest was defined as use of a percutaneous nephrostomy tube (PCNT) and the absence of a ureteral stent for at least 4 weeks prior to the operation. No ureteral rest was defined as the use of an indwelling ureteral stent within 4 weeks of operation. Patients were not recommended into either group, but all patients underwent attempted ureteral stent placement prior to repair. Preoperative patient characteristics collected included age at time of operation, sex, preoperative renal function as measured by estimated glomerular filtration rate, and history of urinary tract infection (UTI). Stricture characteristics included etiology, laterality, ureteral location (mid or distal), and length (in centimeters).
All patients underwent preoperative cross-sectional imaging, cystoscopy, cystogram, retrograde/antegrade pyelogram, and/or ureteroscopy prior to reconstruction to evaluate the length and location of the stricture as well as the reconstructive feasibility and suitability of using the bladder for possible psoas hitch/Boari flap. Ureteral stent placement was attempted in all patients, including those with prior PCNT. If stent placement was successful, patients were designated as the non-ureteral rest group. In all cases with ureteral stents, we were easily able to identify the location of the stricture in the distal to middle ureter. Patients with multifocal or extensive stricture disease that would have required ureteral reconstruction were not included in this cohort. All patients then proceeded to ureteral reimplantation.
We compared peri- and postoperative outcomes between patients who underwent ureteral rest vs no ureteral rest prior to ureteral reimplantation. Scheduled follow-up included a renal ultrasound at 3 and 12 months postoperatively to monitor for postoperative hydronephrosis. Postoperative hydronephrosis was defined as any degree of hydronephrosis by renal ultrasound. Additionally, renal scintigraphy was used to evaluate patients if significant or worsened hydronephrosis was present on renal ultrasound. Our primary outcome was evidence of ureteral stricture recurrence on postoperative imaging. Our secondary outcomes were operative time, estimated blood loss (EBL), use of psoas hitch/Boari flap, postoperative hydronephrosis, and 30-day complication rate. Complications assessed within 30 days postoperatively included readmission to the hospital, return to the operating room, ileus, UTI, or urinary retention, etc.
Continuous and categorical variables were compared using the Mann-Whitney U-test and chi-square test, respectively. A p-value <0.05 was considered statistically significant.
Results
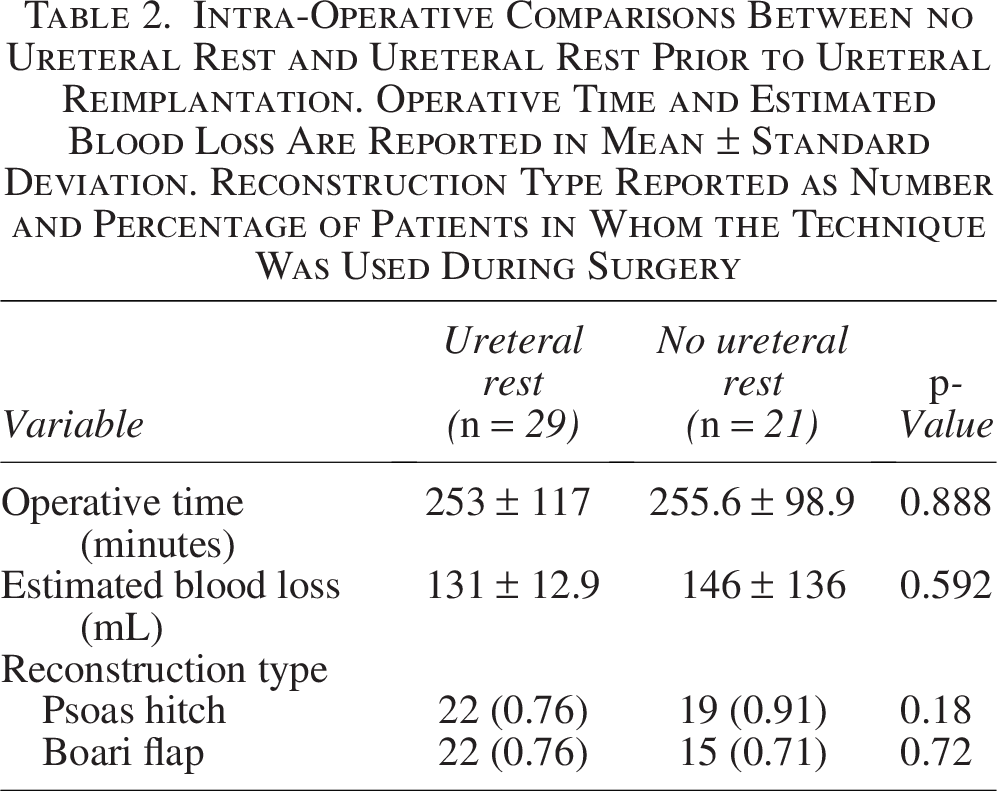
Our final cohort consisted of 50 patients, among whom 29 (58%) underwent ureteral rest prior to ureteral reimplantation. There was no significant difference identified between the two groups in mean age (p = 0.791) or percent female sex (p = 0.82). There were no significant differences identified in preoperative renal function, history of UTI, stricture laterality, location, or length (Table 1). Stricture etiology was significantly different between groups. The cohort without ureteral rest had a higher percentage of radiation-induced ureteral injury (47.6%), while the cohort with ureteral rest had a higher percentage of iatrogenic ureteral injury (75.9%) (p = 0.002) (Table 1). Intraoperatively, there were no significant differences in EBL, operative time, or use of psoas hitch and/or Boari flap between the two groups (Table 2). A total of 35 patients (70%) underwent both psoas hitch with Boari flap, while 6 patients underwent psoas hitch only, and 2 patients underwent Boari flap only.
Patient Demographics and Preoperative Stricture Characteristics in Patients with and without Ureteral Rest. Age, eGFR, and Length of Stricture Are Reported as Mean ± Standard Deviation. Other Variables Are Reported as Number and Percentage of Patients. Stricture Etiology Was Significantly Different Between Groups

eGFR, estimated glomerular filtration rate; UTI, urinary tract infections.
Intra-Operative Comparisons Between no Ureteral Rest and Ureteral Rest Prior to Ureteral Reimplantation. Operative Time and Estimated Blood Loss Are Reported in Mean ± Standard Deviation. Reconstruction Type Reported as Number and Percentage of Patients in Whom the Technique Was Used During Surgery
Median follow-up for the cohort was 8.6 months (interquartile range: 4.6–17.4 months). There was not a significant difference in the rate of ureteral stricture recurrence after ureteral rest (0%) and no ureteral rest (4.8%) (p = 0.420). There was no significant difference in the 30-day complication rate (p = 0.432) or presence of postoperative hydronephrosis at any time within the study period (p = 1.000) between the two groups (Table 3).
Perioperative Outcomes After Ureteral Reimplantation Between Patients With and Without Ureteral Rest Reported in Number and Percentage of Patients

Discussion
Recent studies have demonstrated the advantage of ureteral rest prior to repair of proximal and mid-ureteral strictures.5,6 Like urethral rest, the primary goal of ureteral rest is to allow for stricture maturation for accurate surgical planning. Lee et al. (2021) outlines how ureteral rest promotes stricture maturation by stopping the cycle of wound healing. Wound healing has an inflammatory phase initiated by vascular injury, a proliferative phase, and a maturation phase, during which the contracted healing tissue is strengthened. A ureteral stent across the stricture continues to impart vascular injury, thereby restarting the inflammatory phase.5,7–10 In proximal ureteral reconstruction, a substitution ureteroplasty with a buccal graft or appendix on-lay is often used. While ureteral rest confers the benefit of stricture maturation in substitution ureteroplasty, it may not be as useful when bypassing the stricture completely, such as in ureteral reimplantation. We therefore postulated that ureteral rest would not confer an advantage in ureteral reimplantation since the stricture is completely bypassed.
Our data demonstrated no significant difference in stricture recurrence between ureteral rest and no ureteral rest prior to the repair of distal ureteral strictures with or without psoas hitch and/or Boari flap. The surgical success rate was high in both groups and comparable to previously published surgical success rates in ureteral rest groups of proximal and mid-ureteral strictures.5,6 The low rate of stricture recurrence after ureteral reimplantation is likely explained by the highly vascularized blood supply of the bladder, subsequent collaterals to the anastomosis, and increased mobility of the bladder.
A major practical application of our findings is that in patients who present with a distal stricture and a ureteral stent already in place, it may not be necessary to remove the stent and place a PCNT for 4–6 weeks prior to reimplantation, provided the stricture can be easily identified. In our cohort, we were able to easily identify the stricture with retrograde pyelography or ureteroscopy despite the presence of a stent. Furthermore, during reconstructive operation, stricture identification is aided by the relative ease of dissection. Typically, the ureter will dissect away from the retroperitoneum more easily above the stricture but becomes more challenging at the level of the scar.
Urethral rest in most studies is defined as freedom from urethral instrumentation, most often for between 4 and 6 weeks. 1 Four weeks has subsequently been adopted as the standard by existing ureteral rest studies and in this study.5,6 When compared to existing studies, our cohort is similar with regard to age, proportion of female sex, and laterality. Our patients tended to have longer strictures than other studies, and accordingly, Boari flap and psoas hitch were used in more cases.5,6,11
Stricture length was not significantly different between the ureteral rest and no ureteral rest cohorts. This is likely because we selected for patients who underwent ureteral reimplant, which is only feasible in distal and occasionally, mid-ureteral reconstruction. Stricture etiology was significantly different in patients with and without ureteral rest. The cohort without ureteral rest had a higher percentage of radiation-induced ureteral injury, while the cohort with ureteral rest had a higher percentage of iatrogenic ureteral injury. In our experience, iatrogenic injuries often result in complete transection or occlusion of the ureter, and therefore stent placement is not possible, thus necessitating placement of a PCNT. In contrast, radiation-induced strictures are often slow in onset and not fully obliterative, thereby allowing placement of a ureteral stent.
One major concern in ureteral reimplantation is the ability of the bladder to reach proximal to the stricture and the subsequent change in bladder capacity after reconstruction. For this reason, we assessed the suitability of the bladder for the Boari flap preoperatively. The rate of Boari flap in this study is relatively high, likely because of a personal low threshold to create a small flap if there was even slight tension on the anastomosis. We did not measure the size of the Boari flap in all cases; however, we have not found that a small Boari flap significantly alters postoperative voiding complaints. This is an area of debate among reconstructive urologists given concern for postoperative lower urinary tract symptoms (LUTS) after Boari flap. For example, Hardesty et al. (2024) found a rate of 27.6% for postoperative LUTS among female patients after Boari flap. 12 However, limited data are available, and a prospective study using validated measures for LUTS and symptoms of reflux is needed.
A more recent trend in ureteral reconstruction is to remove the ureteral stent 7–14 days prior to reconstructive operation. This confers an anecdotal benefit of the ureter being less “sticky” during operation without the morbidity of a PCNT. However, given that it takes roughly 3 weeks to reach extracellular matrix and collagen remodeling equilibrium, 10 it is unlikely to be as effective as 4–6 weeks of ureteral rest with a PCNT when not excising the stricture completely. This approach represents an area of future study to assess its effect on stricture recurrence.
Limitations of our study include those with any single-surgeon retrospective cohort, including our small sample size and moderate median follow-up of 8.6 months. There was a significant difference in stricture etiology between groups, which should be controlled for in a future prospective study. These data should additionally be replicated in a multi-institution, multi-surgeon study to increase the sample power and investigate the generalizability of our results.
Conclusions
Although ureteral rest is popular prior to ureteral reconstruction for proximal ureteral strictures, our data demonstrate that it does not confer an advantage for more distal ureteral reconstruction. Thus, operation should not be delayed in order to achieve ureteral rest when reimplantation with or without psoas hitch/Boari flap is expected.
Authors’ Disclosure Statement
No competing financial interests exist.
Authors’ Contributions
K.C.: Methodology, investigation, data curation, visualization, writing—original draft, writing—review and editing. S.M.S.: Writing—original draft, writing—review and editing. J.V.: Software, formal analysis, and resources. F.L.V.: Investigation, writing—review and editing. J.A.B.: Writing—review and editing. A.P.: Software, data curation, and project administration. G.P.M.: Conceptualization, methodology, resources, writing—review and editing, supervision, and project administration.
Footnotes
Funding Information
No funding was received for this article.