
Abstract
Introduction:
Single port (SP) robot-assisted partial nephrectomy (RAPN) can be successfully performed via an extraperitoneal low anterior access (LAA), with the patient in a supine position. To our knowledge, no data on the learning curve (LC) of SP RAPN performed with the LAA are available in the literature.
Methods:
Supine LAA SP RAPNs performed by a single experienced SP surgeon from 2019 to 2025 were retrospectively reviewed. A cumulative summation (CUSUM) methodology in terms of operative time was used for the assessment of the surgical learning curve. After identifying the number of cases required for proficiency achievement, a comparison of perioperative and postoperative outcomes of the learning and proficiency phases was conducted.
Results:
After determining the CUSUM value for each of the 66 included cases, a cubic polynomial regression with a high goodness of fit coefficient (R2 = 0.987) was adopted to plot the LC. The resulting third-degree polynomial equation was solved to extract the inflection point of the curve, representing the case threshold for achieving competence, which corresponded to the 33rd case. The learning curve was accordingly divided into a learning phase (cases 1–33) and a proficiency phase (cases 34–66) to compare perioperative and postoperative outcomes. Preoperative tumor and patient characteristics were similar between the groups. Procedures performed in the learning phase demonstrated significantly longer median operative times (210 minutes [interquartile range [IQR] 175–250] vs 164 minutes [IQR 148.5–202.5], p < 0.001) and ischemia times (26 minutes [20.5–31.5] vs 19 minutes [17.5–22], p < 0.001) and lower rates of trifecta achievement (n = 16 [48.5%] vs n = 26 [78.8%], p = 0.01). Finally, at multivariate analysis, being operated in the proficiency phase was independently and significantly associated with a higher likelihood of trifecta achievement (odds ratio: 8.53, 95% confidence interval 1.6–45.6, p = 0.012).
Conclusions:
The LC of LAA SP RAPN can be mastered safely with a relatively attainable number of cases by an experienced robotic surgeon.
Introduction
Robot-assisted partial nephrectomy (RAPN) has become the most frequently performed intervention for the treatment of renal cell carcinoma (RCC). 1 Multiport RAPN (MP RAPN) has been traditionally performed via a transperitoneal access and with the patient in a full flank position. Access to the peritoneum carries a series of drawbacks, mainly the risk of bowel injury, the increased complexity in the case of an hostile abdomen, postoperative ileus, and anesthesiologic complications associated with the pneumoperitoneum.2–4 Retroperitoneal MP RAPN is feasible, but the increased complexity and conflicts between instruments limited its widespread adoption. Regarding positioning, a prolonged flank position has been associated with increased postoperative pain and rare serious complications, such as brachial plexus neuropraxia and rhabdomyolysis, in addition to respiratory distress.5,6 Moreover, patient positioning is a critical and time-consuming step, which requires expertise, extra care (especially when maneuvering the patient’s head and pressure points), and additional operating room (OpR) staff (particularly for obese patients, with the risk of occupational back pain). Since the introduction of the single port (SP) robotic platform, efforts have been made to fully exploit its potential, reducing invasiveness to the lowest level. In the field of upper urinary tract (UUT) procedure, such efforts included the development and refinement of the low anterior access (LAA).7,8 This technique standardizes OpR setup, simplifies patient positioning, and avoids complications associated with the flank position and transperitoneal access. Ultimately, the LAA reduces anesthesia times, respiratory distress, and postoperative pain.9,10 The array of urologic interventions successfully described with the LAA is expanding to comprise virtually every UUT surgical procedure. SP RAPN via a LAA is safe and feasible and has been associated with lower operative times and complication rates, especially in elderly and frail patients. 10 Despite the overall increase in adoption, specific data on the learning curve (LC) of SP RAPN performed via a LAA are lacking. LC analysis, in addition to establishing the number of cases required to reach proficiency, is crucial to plan efficient training programs. 11 The cumulative summation (CUSUM) of continuous variables, particularly of operative times, is one of the most frequently adopted methods to assess the learning curve.12,13 It provides an efficient visual representation of the learning process and the number of cases required to achieve proficiency.
In the present study, we aim to use the CUSUM method to assess the LC of SP RAPN performed with a LAA and supine position, in a single center and for a single experienced robotic surgeon.
Materials And Methods
Population
All patients who underwent SP RAPN with the Da Vinci Single-Port Platform (Intuitive surgical Inc., Sunnyvale, CA, USA) from 2019 to 2025 were retrospectively reviewed. The electronic database of hospital records (EPIC system) was adopted for data collection. After screening and case selection, only procedures performed with a supine retroperitoneal LAA were included. The study was approved by the Institutional Review Board of University of Illinois Chicago with the following protocol number: 2020–1428. One case has been temporarily excluded from the series because of pending litigation. All procedures were performed by the same primary surgeon with >10 years of experience with robot-assisted kidney operation in the same institution. Preoperative clinical, anthropometric, and demographic data were collected. After adequate counseling on the possible relevant therapeutic choices and surgical approaches, all included patients chose SP RAPN performed via a LAA as primary treatment option. Preoperative staging was performed in all cases with abdominal computed tomography, magnetic resonance imaging, or both. Tumor side, size, and location were recorded. RENAL and Padua nephrometry scores were used to calculate renal mass complexity.
Surgical procedure
Surgical technique of LAA RAPN has already been described. 14 Intraoperative images or the surgical incision and access are shown in Supplementary Figure S1. Briefly, with the patient in a supine position and a bump under the ipsilateral flank (reaching an approximately 10° ipsilateral elevation), a single incision is made at the level of the McBurney point. After reaching the preperitoneal fat through the abdominal wall, the small Da Vinci SP access port (Intuitive Surgical System, Sunnyvale, CA, USA) is positioned and the robot is docked. An additional 12 mm assistant port is routinely placed through the same skin incision but different fascia incision, with the so-called “sidecar” technique. The intervention is normally performed with the camera at the 6 o’clock position, monopolar curved scissors in the right hand, Maryland Bipolar forceps in the left hand, and fenestrated bipolar at the 12 o’clock position. The first step is the identification of the Psoas muscle, which is followed cranially to reach and incise the Gerota fascia. The lesion is then exposed, and the margins are marked. Attention is then turned to the hilum, and the renal artery is clamped using SP Bulldog clamps before proceeding with tumor resection. Renorrhaphy is then performed according to the surgeon’s preference.
CUSUM curve construction
The construction of the surgical learning curve was performed according to the risk-adjusted CUSUM methodology previously described, on the basis of operative time [15]. The mean operative time (μ) was used as reference value for CUSUM calculation. The formula adopted to compute the CUSUM value for each case was the following:

In which μ is the mean operative time, CUSUMn is the CUSUM value for each n case, and Xn represents the operative time for case n. CUSUM1, namely the CUSUM value of the first case, was set to zero. To see the trend in operative time, the CUSUM curve was then constructed by plotting the CUSUM values on the y-axis against the case sequence on the x-axis. A better visualization of the nonlinear nature of the data is obtained by performing a polynomial regression. Regression analysis was carried out with different polynomial degrees to determine the order of the polynomial that fitted best the distribution of the CUSUM values. The coefficient of determination (R2) for each polynomial regression was adopted to quantify the adaptability of the regression to the variability of the data. The closer the R2 value to 1, the stronger the fit of the curve (i.e., the better the model captures the trend in the learning curve).
An upward trend (Positive Slope) indicates that operative times are consistently longer than the expected mean (μ), representing the initial learning phase. The inflection point (the point at which the tangent to the curve is parallel to the x-axis) represents a change in performance trend and corresponds to the number of cases required to achieve proficiency. A downward trend (negative slope) indicates that operative times are becoming consistently shorter relative to the mean (μ). A stable trend near zero is interpreted as consistent performance.
Statistical analysis
Stata version 18.1 (Stata Corporation, College Station, TX, USA) and SPSS version 27.0 (IBM SPSS Statistics for Windows, Version 27.0, Armonk, NY: IBM Corp) were used to perform statistical analysis. Categorical variables were expressed as absolute numbers and percentages, and continuous data were reported as mean ± standard deviation or median and range. The Mann–Whitney test or the Analysis of variance (ANOVA) one-way test was used for quantitative data comparison and pairwise intergroup comparisons of variables. A Fisher’s exact test and a chi-square test were adopted for qualitative data comparison. The level of significance was set at p value <0.05.
Results
Study cohort characteristics
General characteristics of the study population are described in Table 1. A total of 66 LAA SP RAPN were included for final analysis, n = 33 (50%) males and n = 33 (50%) females. Median age was 60 years (interquartile range [IQR] 52–67), and median body mass index (BMI) was 30 kg/m2 (IQR 26.1–36.5). Preoperative and postoperative estimated glomerular filtration rate (eGFR), calculated with the Cockcroft–Gault equation, were, respectively, 70.4 mL/min (IQR 55.9–93.9) and 74.6 mL/min (IQR 60.1–93.8), with a median delta of 1.9 (IQR −4.7–10.4). N = 31 (47%) of the study cohort had a positive history of tobacco smoke, either current or former smokers. The African American was the most represented ethnic group (n = 30 [45.5%]), followed by Caucasian (n = 23 [34.8%]) and Hispanic (n = 7 [10.6%]). Regarding comorbidities, diabetes, hypertension, and obesity were present in n = 18 (27.3%), n = 22 (33.3%), and n = 45 (68.2%) of patients, respectively.
General Characteristics of the Study Population
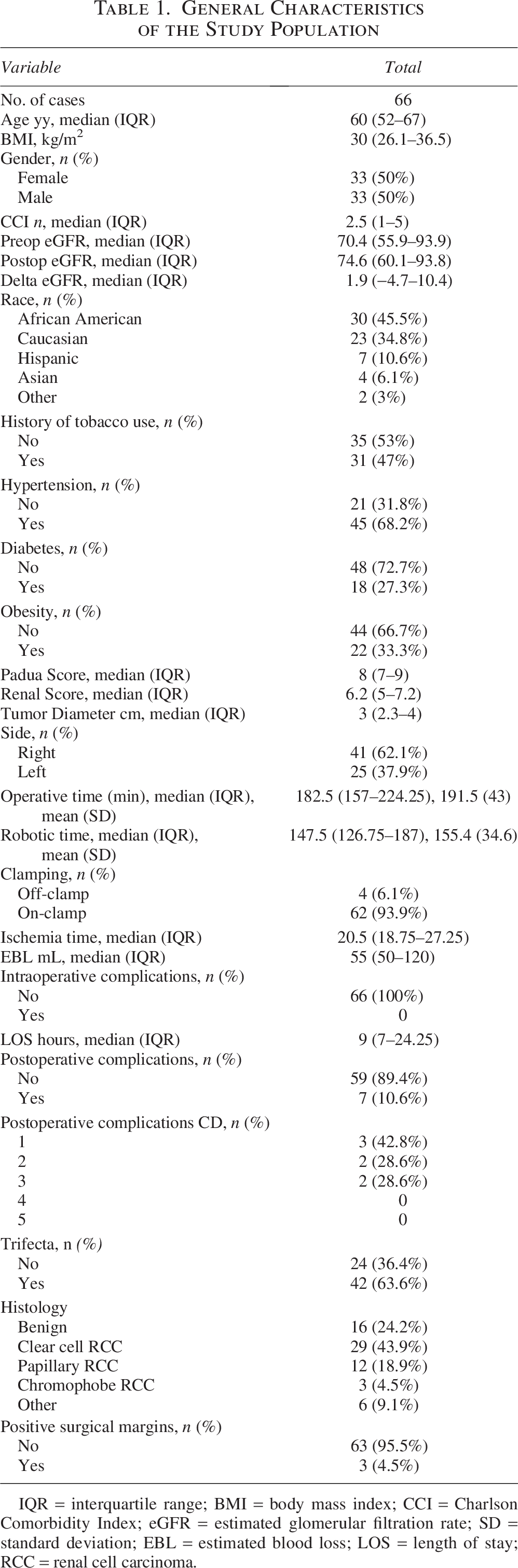
IQR = interquartile range; BMI = body mass index; CCI = Charlson Comorbidity Index; eGFR = estimated glomerular filtration rate; SD = standard deviation; EBL = estimated blood loss; LOS = length of stay; RCC = renal cell carcinoma.
A right-sided lesion was more frequent (62.1% right side vs 37.1% left side). Median tumor diameter, Padua score, and RENAL score were, respectively, 3 cm (IQR 2.3–4), 8 (IQR 7–9), and 6 (5–7). Total median and mean operative time were 182.5 minutes (IQR 157–224.25) and 191.5 ± 43 minutes, with median 147.5 minutes (IQR 126.75–187) of robotic time. An on-clamp approach was the approach of choice for the vast majority of cases (n = 63 cases [93.9%]), with a median ischemia time of 20.5 minutes (IQR 18.75–27.25). No intraoperative complications were registered. Median estimated blood loss was 55 mL (IQR 50–120). Patients were discharged after a median of 9 hours (IQR 7–24.25). Only n = 7 (10.6%) patients experienced postoperative complications at 30 days; the majority (n = 3 [42.8%]) of Clavien–Dindo (CD) grade 1, n = 2 CD grade 2 (n = 1 bleeding necessitating blood transfusion and n = 1 postoperative delirium), n = 2 CD grade 3 (n = 2 retroperitoneal hematomas), and no CD grade 4 or 5 complications were recorded. Regarding final pathologic analysis, a clear cell renal cell carcinoma was the most represented histologic subtype (n = 29 [43.9%]), and a positive surgical margin (SM) was found in n = 3 (4.5%) patients.
Ultimately, the “trifecta” (i.e., negative SMs, warm ischemia time <25 minutes, no postoperative complications of CD grade ≥3) was achieved in n = 42 (63.6%) cases.
The learning curve
The learning curve for operation time of SP RAPN performed with a LAA is shown in Figure 1. After CUSUM calculation and learning curve construction, with an R2 of 0.987 the cubic polynomial demonstrated the best fit. The third-degree polynomial equation resulting from the cubic regression was the following:

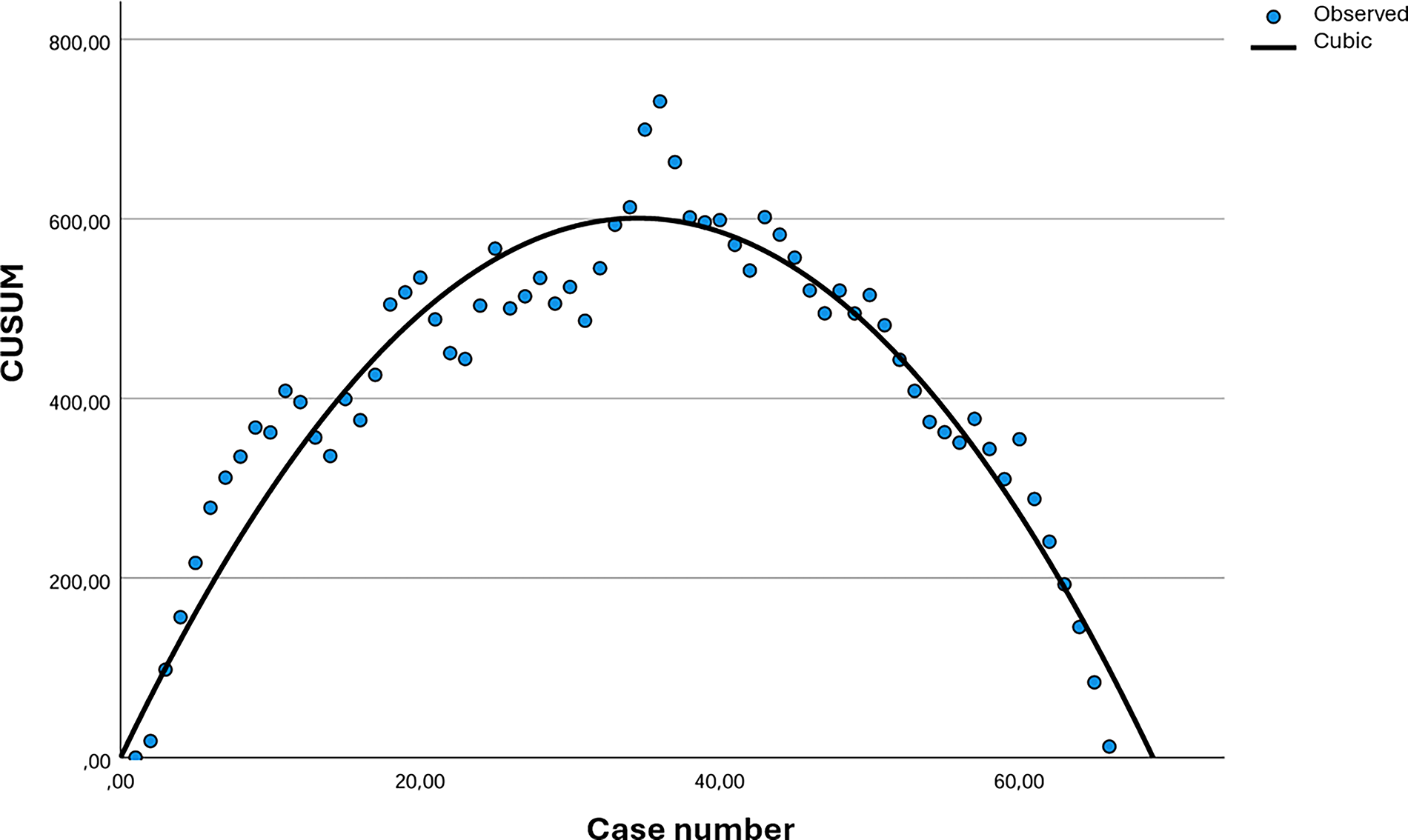
CUSUM learning curve for operative time of LAA SP RAPN. The sequential number of cases is represented on the x-axis and the CUSUM of deviation from the mean operative time on the x-axis. The positive slope (upward trend) represents cases with consistently longer operative times than the expected mean (Μ). The slope becomes negative (downward trend) when operative times become consistently shorter relative to the mean (Μ). CUSUM = cumulative summation; LAA = low anterior access; SP = single port; RAPN = robot-assisted partial nephrectomy.
The first derivative was set equal to zero to find the maximum of the function (i.e., the turning point of the curve):

After solving the equation, the calculated inflection point corresponded to the 33rd case (X = 33.2), which was used as a surrogate for the number of cases required to achieve proficiency.
Comparative analysis of learning and proficiency phases
After identifying the number of cases required to reach the inflection point of the CUSUM curve, the LC was divided into a learning phase (cases 1–33, the “learning group”) and a proficiency phase (cases 34–66, the “proficiency group”). A comparison of patients’ characteristics and perioperative and postoperative outcomes between cases in the learning and proficiency groups was performed, to determine the impact of the proficiency level on the likelihood of obtaining favorable surgical outcomes (Table 2).
Comparison of Preoperative, Perioperative, and Postoperative Data Between Cases in the Learning and Proficiency Groups

Significant data is in bold.
IQR = interquartile range; BMI = body mass index; CCI = Charlson Comorbidity Index; eGFR = estimated glomerular filtration rate; SD = standard deviation; EBL = estimated blood loss; LOS = length of stay; CD = Clavien–Dindo; RCC = renal cell carcinoma.
Preoperative characteristics were similar between the two groups. Patients in the learning phase group had significantly higher rates of tobacco use (60.6% vs 33.3%, p = 0.02) and obesity (45.5% vs 21.2%, p = 0.037). Conversely, cases in the proficiency group had higher median Charlson Comorbidity Index (4 [2–6] vs 2 [1–3], p < 0.001) and rates of hypertension (78.8% vs 57.6%, p = 0.06). Both median total operative time and robotic time were significantly shorter in the proficiency group compared with the learning group (164 [IQR 148.5–202.5] vs 210 [IQR 175–250], p < 0.001 and 134 [IQR 121.5–165.5] vs 172 [IQR 139.5–193.5], p = 0.04). Only on-clamp procedures were performed in the proficiency group vs n = 4 (12.1%) clampless procedures in the learning group (p = 0.039). The median ischemia time was significantly shorter in the proficiency group compared with the learning group (19 [17.5–22] vs 26 [20.5–31.5], p < 0.001). Moreover 30-day postoperative complication rates were significantly higher in the learning group (n = 6 [18.2%] vs n = 1 [3%], p = 0.046), which also demonstrated higher rates of readmissions (15.2% vs 0), despite the difference not reaching the level of significance (p = 0.06). Ultimately, the trifecta was achieved in only n = 16 (48.5%) cases in the learning group vs n = 26 (78.8%) in the proficiency group (p = 0.01).
Multivariable logistic regression for the achievement of the trifecta
Results of a multivariable binary logistic regression model exploring the effect of different preclinical and operative variables on the odds of achieving the trifecta are shown in Table 3. An increasing BMI and tumor diameter negatively impacted the odds of trifecta achievement (odds ratio [OR]: 0.87, 95% confidence interval [CI] 0.76–0.98, p = 0.03 and OR: 0.22, 95% CI 0.09–0.55, p = 0.001). In contrast, having an operation performed in the proficiency phase was a significant positive predictor of trifecta achievement (OR: 8.53, 95%CI 1.6–45.6, p = 0.012).
Results of Multivariable Regression Analysis Exploring the Effect of Different Predictors on the Likelihood of Trifecta Achievement

Significant data is in bold.
BMI = body mass index; CCI = Charlson Comorbidity Index; OR = odds ratio; CI = confidence interval.
Discussion
Partial nephrectomy (PN) has become the most frequently performed surgical intervention for the treatment of RCC. Current guidelines recommend surgeons to opt for a nephron sparing strategy whenever technically feasible. 15 Particularly in the case of small lesions (cT1a), active surveillance and tumor ablation (TA) are popular alternative options.16,17 For such selected single and small masses, TA demonstrated similar oncologic results to surgical treatment. 16 In this scenario, and with an increasing rate of RCC diagnosed in a localized and early stage, safety and minimal invasiveness are mandatory requirements of novel surgical treatment options. RAPNs have been successfully performed for more than a decade. To further reduce invasiveness, a SP approach has been proposed both for laparoscopy and RAPNs. Nonetheless, the high surgical complexity of a PN, together with the technical challenges of laparoendoscopic single site surgery, has limited its widespread adoption. Similarly, the challenges of adapting a MP console to a single entry site have restricted the diffusion of SP RAPN performed with a MP surgical system. With the same aim of reducing the level of invasiveness, MP RAPNs have been successfully described with a retroperitoneal approach, avoiding the complications of access to the peritoneal cavity. Even in this case, however, the multiarmed robotic system just partially adapted to the confined retroperitoneal space. The SP robotic system has been developed to overcome such limitations. The multijointed instruments and the three-dimensional high-definition (3DHD) articulating scope allow the SP robotic system to efficiently work in confined spaces, such as the retroperitoneum. Moreover, the versatility of the single robotic arm, with its 360° rotation, allows virtually every urologic procedure to be performed with the patient in a supine position. The LAA was developed with the aim to offer a reproducible and standardized access for different UUT surgical procedures performed with the SP robot, particularly with the patient in a supine position. An increasing number of robotic surgeons are adopting this technique, and multiple series of SP RAPNs performed with a LAA are available in the literature, with favorable outcomes.8,18 Although the initial emphasis of the literature of the SP system has been on safety and feasibility, focus is now shifting toward evaluation of the surgical LC. A determination of the learning process is crucial to develop efficient and evidence-based training programs. This is particularly true in the case of the SP robotic system since, after an initial phase dominated by experienced robotic surgeons, residents and young attending surgeons are now gaining increasing hands-on experience in SP robotic OpRs. Different LC evaluation methods have been described in the literature, and they can generally be classified into four categories: graphical inspection, split-group, CUSUM, and regression.13,19 Among these, CUSUM is one of the most frequently used for surgical LC construction, thanks to its visual appeal and the adoption of clinically relevant continuous variables, such as operative time (OT) and estimated blood loss. 20
This is the first study to evaluate the surgical LC of SP RAPNs performed specifically with a LAA. After CUSUM curve construction based on OT, we found that 33 cases were required to master the LC. This number is not far from that reported for MP RAPN. Indeed, a previous analysis on 500 consecutive transperitoneal MP RAPNs revealed a significant improvement in postoperative outcomes after 35 procedures. 21 Another study reported that at least 25 independent procedures are required to perform MP RAPN with low complication rates, acceptable positive margin rates, and sustainable cost-effective durations. 22 When comparing operations performed in the learning and proficiency phases, we found a higher likelihood of not achieving the trifecta in the learning phase. Although oncologic safety was maintained throughout the study period (no significant differences in positive SM rates), patients in the learning group demonstrated significantly longer operative times and ischemia times. Moreover, at multivariate regression, being operated after proficiency achievement was a significant independent predictor of trifecta achievement. A previous study adopting the CUSUM methodology to evaluate the surgical LC of extraperitoneal SP RARP found longer OTs and length of stay of cases performed in the learning phase, but no difference in complication rates [15]. Our results on the LC of LAA retroperitoneal SP RAPN provide a guide for future development of training curricula in kidney procedure as well.23–25
We acknowledge several limitations of our study. First, because of the methodology adopted and the relatively small sample size, we could not control for tumor and patients’ characteristics that could have influenced the duration of the procedure. However, previous studies showed that the higher complexity of a renal mass does not correlate with longer operative times, but rather with higher complication rates and worse oncologic outcomes.24,26,27 Moreover, no significant differences in terms of nephrometry scores and tumor size and side were found between the learning and proficiency groups. Second, the previous experience of the primary surgeon with flank SP RAPNs as well as other retroperitoneal surgeries performed with a LAA during the study period could have speeded the learning process. Nonetheless, the influence of other concomitant operation is a well-known limitation of every LC analysis, which reflects clinical practice. More importantly, consecutive series from different expert robotic surgeons show that beginning with a transperitoneal approach and a flank position is the standard, rather than starting with LAA.28,29 This pragmatic stepwise progression is common practice in surgical training. This way the learning process is focused on the novel elements of the technique (e.g., the robotic platform), whereas other variables, such as patient positioning and anatomical orientation, are intentionally kept constant. Accordingly, considering the just recent (2024) approval of the SP robotic platform in the European Union, our analysis may be particularly relevant for European urologic robotic surgeons who are beginning to adopt the SP system, to offer additional guidance for approaching the LAA. However, the learning curve of surgeons approaching SP RAPNs directly with a LAA could be longer than that reported for a surgeon who’s already proficient with the SP console. Finally, the CUSUM methodology has been criticized for its simplified visual representation which could lead to excessively confident conclusions. 30 However, the use of a polynomial regression model with a high R2 coefficient mitigates the risk of arbitrary evaluations, ensuring an adequate representation of real data trends.
Conclusions
In the present study, we used CUSUM methodology to evaluate the learning curve of SP RAPN performed specifically with a LAA. We found that 33 procedures are required for an experienced MP robotic surgeon with practice with SP transperitoneal and flank retroperitoneal operation to master this technique. The learning process is manageable and safe with findings of lower rates of trifecta achievement for cases performed during the initial learning phase. We believe that LC studies can pave the way for the development of a standardized training curricula, and future multicenter collaborations could help strengthen our results.
Authors’ Contributions
Conceptualization: V.S., H.B.H., and L.A.M.; data curation: F.C. and A.T.; formal analysis: V.S. and F.T.; methodology: F.M.V. and F.C.; project administration: S.C. and G.B.D.P.; writing—original draft: V.S. and H.B.H.; writing—review and editing: S.C. and L.A.M.; and supervision: A.T., F.M.V., and S.C.
Footnotes
Author Disclosure Statement
All authors declare no conflicts of interest.
Funding Information
No funding was received for this article.
Supplemental Material
Abbreviations
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.