
Abstract
Introduction:
Robot-assisted radical prostatectomy (RARP) is the standard treatment for localized prostate cancer. Various techniques, including anterior, posterior, and lateral approaches, have been developed to optimize surgical and functional outcomes. This study reports our initial experience with the novel posterior, anterior, and lateral (PAL) approach, designed to integrate their respective strengths into a combined, structured surgical strategy, and evaluates its feasibility, safety, and early outcomes.
Patients and Methods:
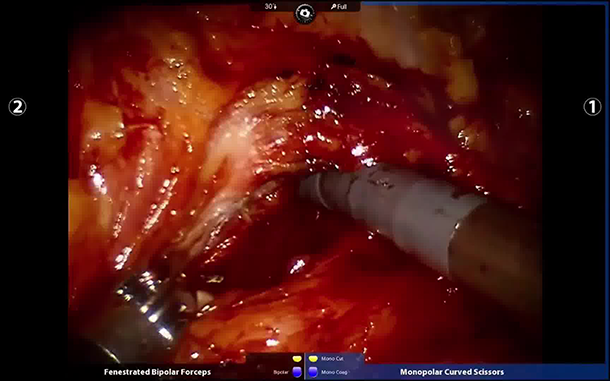
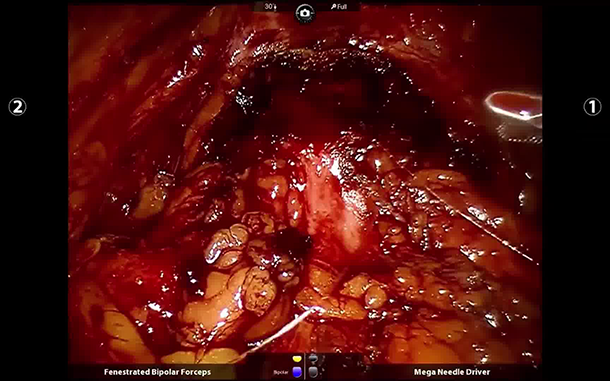
This retrospective study included 46 consecutive patients who underwent RARP performed by a single surgeon between August 2022 and September 2024 using the da Vinci Si surgical system. The PAL technique involved sequential dissection (1) Posterior access—incision of rectovesical peritoneum, dissection of seminal vesicles and vas deferens, and creating a triangular anatomical zone; (2) Anterior access—division of medial umbilical ligaments to enter the retropubic space while preserving endopelvic fascia and puboprostatic ligaments; (3) Lateral access—expansion of the triangular zone between bladder neck, prostate base, and neurovascular bundle, retracting seminal vesicles, and sharply dividing the bladder neck; (4) Neurovascular bundle preservation. Urinary continence was defined as zero to one safety pad per day. Erectile function recovery was defined as erections sufficient for intercourse with/without PDE5 inhibitors. Outcomes were assessed at 1, 3, and 6 months.
Results:
The median age was 69.5 years (IQR: 63.3–73.8), and the median preoperative PSA was 13.7 ng/mL (IQR: 9.0–21.7). All surgeries were completed without conversion. Median console time was 85 minutes (IQR: 76–95), and median blood loss was 70 mL (IQR: 50–100). Positive surgical margins occurred in 19.6% (95% CI: 9.4–34.2), with lymph node metastases in 21.7% (95% CI: 11.2–36.3). Immediate continence was achieved in 54.3% (95% CI: 39.2–68.9), improving to 89.1% (95% CI: 76.4–96.4) at 3 months and 97.8% (95% CI: 88.5–99.9) at 6 months. Erectile function recovery was 80.0% (95% CI: 51.9–95.7) at 6 months. The overall complication rate was 13.1%, with no Grade 4 events.
Conclusion:
The PAL technique demonstrates feasibility and safety in RARP, with favorable perioperative outcomes and promising early functional recovery. It facilitates maximal anatomical preservation by systematically integrating multiple surgical planes, improves intraoperative visualization, facilitates nerve-sparing, and may enhance functional recovery. Further prospective studies with longer follow-up are warranted to confirm its long-term outcomes.
These authors contributed equally to this work.
First: Jinshan, Last: Cui (
First: Gaurab, Last: Pokhrel (
First: Zhenhao, Last: Li (
First: Hao, Last: Liu (
First: Jin, Last: Tao (
First: Yunlong, Last: Liu (
First: Yafeng, Last: Fan (
First: Shuanbao, Last: Yu (
First: Zhaowei, Last: Zhu (
First: Xuepei, Last: Zhang (
Runtime of the video: 6 mins 55 secs.
Jinshan Cui, Pokhrel Gaurab, Zhenhao Li, Hao Liu, Tao Jin, Yunlong Liu, Yafeng Fan, Shuanbao Yu, Zhaowei Zhu, Xuepei Zhang have no conflicts of interest or finincial ties to disclose.
Jinshan Cui, Pokhrel Gaurab, Zhenhao Li, Hao Liu, Tao Jin, Yunlong Liu, Yafeng Fan, Shuanbao Yu, Zhaowei Zhu, Xuepei Zhang have received and archived patient consent for video recording/publication in advance of video recording of procedure.