
Abstract
Objective:
To evaluate the safety, feasibility, and outcomes of ureteroscopic (URS) lithotripsy for distal ureteral stones under patient-controlled sedation (PCS) in a large single-center cohort.
Methods:
This retrospective observational study included 414 patients who underwent 429 URS lithotripsies under intravenous PCS with propofol and alfentanil between 2017 and 2023. Pre-, peri-, and postoperative variables were assessed, and outcomes were analyzed according to stone-free status using graded definitions. Grade A indicated complete stone-free status with no residual stones on postoperative CT, Grade B included Grade A with residual fragments ≤2 mm, and Grade C included Grades A and B with residual fragments measuring 2.1–4 mm.
Results:
The overall absolute stone-free rate was 95% (n = 406; Grade A); when relative stone-free definitions were applied, the rates were 95% (n = 408; Grade B) and 97% (n = 414; Grade C). The rate of complications (Clavien–Dindo ≥III) was 1%, and no adverse events occurred. The procedure was aborted in 1% of cases, and 99% of procedures were completed on an outpatient basis without anesthesiology support. Non-stone-free patients (5%) more frequently had multiple or larger stones and a history of stone disease, although no associations were identified with sedation volume or surgeon experience.
Conclusion:
URS lithotripsy under PCS is safe and effective for distal ureteral stones, with a high stone-free rate and low complication rate, and may offer practical advantages in clinical practice.
Keywords
Introduction
The global incidence of urolithiasis has increased steadily over recent decades, particularly in developed countries, reflecting lifestyle and metabolic changes. 1 This rise has led to a growing number of ureteroscopic (URS) lithotripsy procedures worldwide. Traditionally, URS lithotripsy is performed under general anesthesia (GA) to ensure patient immobility and optimal surgical conditions. 2 However, GA requires anesthesiology oversight, airway management, and substantial perioperative resources, while carrying inherent procedural risks, particularly among older patients or those with significant comorbidities. 3
Advances in endoscopic technology and perioperative care have prompted growing interest in less resource-demanding anesthetic approaches. Several centers have reported the feasibility of performing URS lithotripsy under conscious or moderate sedation, with comparable stone-free and complication rates to GA in selected patients.1,3–5 Notably, Jain et al. recently provided proof-of-concept data showing that both proximal and intrarenal URS lithotripsy can be performed effectively under urologist-directed conscious sedation, achieving an 83.8% overall success rate and 80.8% stone-free rate, without intraoperative complications or postoperative admissions. 4 These findings, together with earlier reports of high efficacy for distal ureteral URS lithotripsy under intravenous or loco-sedative anesthesia,5–7 suggest that sedation-based techniques can be a safe and feasible alternative to GA in many cases.
In parallel, developments in procedural sedation across other fields have introduced patient-controlled sedation (PCS) as a patient-centered alternative to clinician- or anesthesiologist-controlled sedation. The use of PCS has been described for many procedures such as burn wound dressing changes, endoscopic procedures, and dental treatment.8–10 Similar to URS lithotripsy, these procedures involve painful stimuli that are difficult to tolerate without analgesia, making moderate procedural sedation necessary. Early studies combining propofol with the short-acting opioid alfentanil demonstrated that PCS is practical for endoscopic procedures and facilitates rapid recovery.11,12 A subsequent randomized trial confirmed that propofol–alfentanil PCS provided effective sedation with significantly faster recovery compared with the midazolam–pethidine regimens. 13 Moreover, a systematic review and meta-analysis found that PCS with propofol reduced the need for rescue interventions for sedation-related adverse events and lowered the risk of oversedation compared with clinician-controlled propofol sedation. 14
Despite previous studies, data are still limited for PCS in URS lithotripsy. This study aimed to evaluate the safety, efficacy, and feasibility of PCS for distal URS lithotripsy in a large consecutive cohort, providing the first large-scale assessment of this technique in endourology.
Materials and Methods
Study design and patient cohort
This retrospective observational study included all patients undergoing URS lithotripsy with PCS at Norrköping Hospital, a secondary referral center in mid Sweden, between January 2017 and December 2023. Patients were identified via electronic medical records using the Swedish Classification of Health Interventions (KVÅ) for ureterolithotomy (KBE12) and PCS (ZXC20). Written study information was provided with the option to opt out. The study was conducted in accordance with the Declaration of Helsinki and approved by the Swedish National Ethics Committee (approval number 2024-02568-01).
A total of 466 procedures were initially identified. After exclusion due to declined participation (n = 12), deceased patients (n = 17), incomplete notification (n = 7), and miscoding (n = 1), the final study cohort included 429 procedures performed in 411 unique patients (Fig. 1).
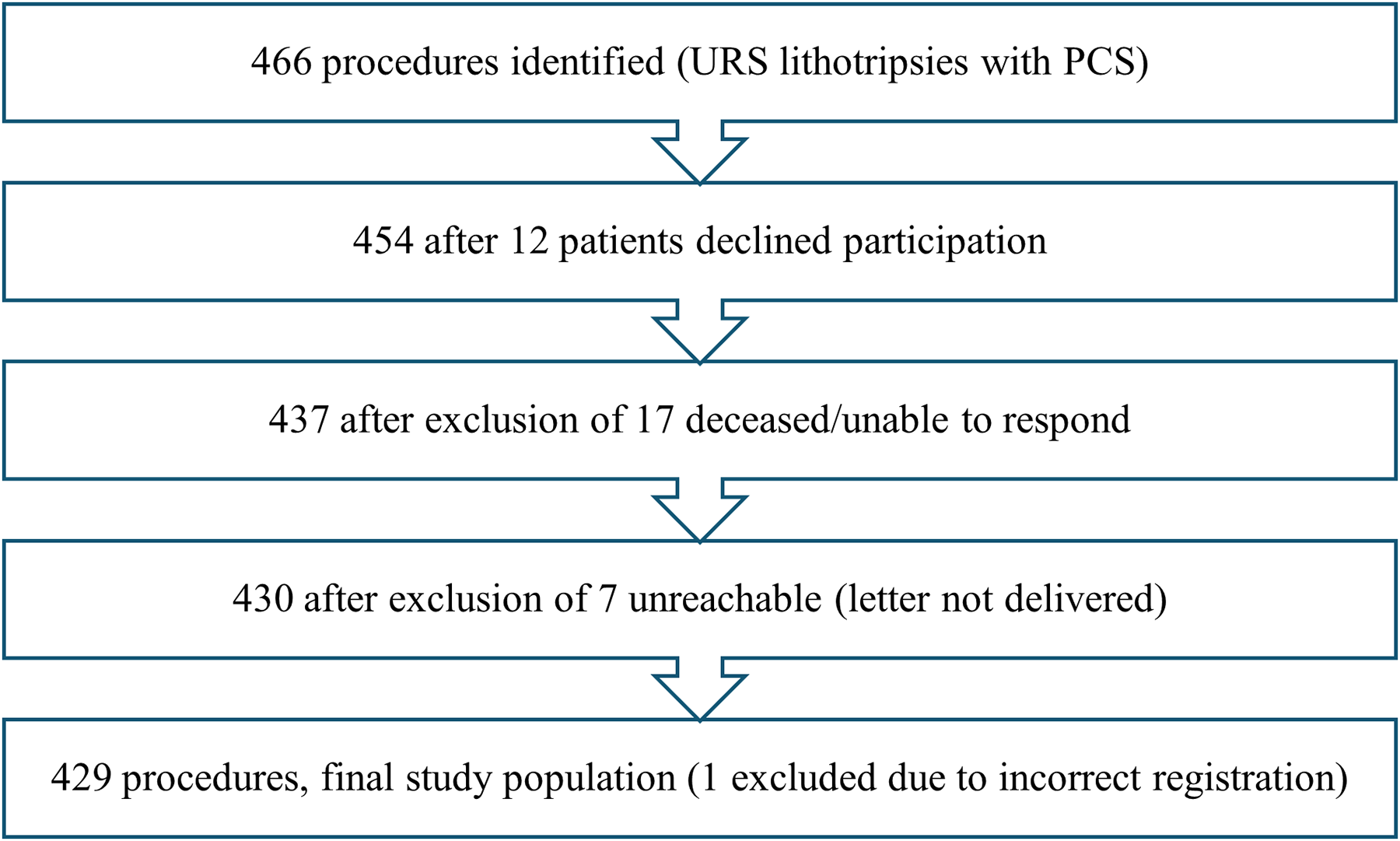
Flow diagram of procedure inclusion. The flowchart illustrates the selection process for procedures included in the final study population. URS = ureteroscopy; PCS = patient-controlled sedation.
Indication for surgical treatment
Selection for URS lithotripsy with PCS was based on referral. Patients ≥18 years with distal ureteral stones ≥6 mm, or smaller stones ≤5 mm persisting on imaging performed approximately 30 days after diagnosis, were considered eligible if medically suitable. Eligibility was assessed by the operating urologist using standardized guidelines developed in collaboration with an anesthesiologist (Supplementary Table S1).
Procedure
URS lithotripsy with PCS was performed on an outpatient basis. Patients fasted for at least 6 hours for solid foods or milk-containing beverages, and 2 hours for clear fluids before the procedure. Stone position was confirmed by CT on the day of operation. Preoperative urine culture was obtained before admission, and appropriate prophylactic antimicrobial therapy was administered. Patients with a negative urine culture received a single prophylactic dose of sulfamethoxazole–trimethoprim before the procedure. Patients received detailed procedural information from the operating urologist and assisting nurse.
Preoperative analgesia included naproxen 500 mg and paracetamol 1000 mg. Intraurethral local anesthesia was administered using Xylocaine gel. Sedation was achieved with a mixture of 50 mL propofol (10 mg/mL) and 10 mL alfentanil (0.5 mg/mL) prepared in a syringe connected to intravenous access. A carrier fluid, NaCl 100 mL, was used to ensure correct administration of bolus doses. The syringe was connected to a syringe pump (Syramed® µSP6000, Acromed). Sedation was patient-controlled, with 0.5 mL bolus doses delivered via a handheld button activation with a 12-second lockout interval. The combination of propofol and alfentanil allowed patients to self-titrate to moderate sedation. Alfentanil provided analgesia for expected painful stimuli and PCS enabled purposeful responses to verbal or tactile stimulation while minimizing respiratory and circulatory effects.15,16 Supplemental oxygen was provided through a nasal cannula, and continuous monitoring included oxygen saturation, heart rate, and level of alertness (Supplementary Table S1).
All procedures were performed in a dedicated cystoscopy suite equipped with fluoroscopy. Patient were positioned in the lithotomy position and draped with sterile surgical drapes. Initial access was obtained using a 22 Charrière cystoscope, after which a safety guidewire was advanced to the renal pelvis under fluoroscopic guidance. Ureteral stones were managed using 6 French semirigid ureteroscopy with holmium yttrium aluminum garnet laser lithotripsy or basket extraction. Standard settings for laser lithotripsy were 0.3 J at 40 Hz for dusting and 0.5 J at 20 Hz for fragmentation. Double-J stent placement was not routinely performed and was undertaken selectively based on intraoperative assessment.
No anesthesiology staff were present in the operating room. Two experienced urology nurses assisted: one the surgeon, whereas the other monitored the patient’s level of consciousness, operated the fluoroscopy equipment, and provided patient support throughout the procedure.
Variables
Preoperative data included the following: Age, sex, body mass index (BMI), Charlson Comorbidity Index17,18 (Supplementary Table S2), history of stone treatment, number of ureteral stones, laterality (right, left, bilateral), stone size (length and width), HU, distance between stone and urinary bladder, preoperative ureteral stenting and stent dwelling time, presence and duration of percutaneous nephrostomy, urine culture results, and antibiotic prophylaxis.
Perioperative data: Total administered sedation volume, surgeon’s level of training, ureter orifice intubation strategy (single guidewire, double guidewire, access sheath).
Postoperative data: Use and dwelling time of postoperative stent, reasons for procedure discontinuation if applicable, outpatient vs inpatient setting, hospital readmissions within 30 days and underlying causes, complications according to the Clavien–Dindo classification, 19 stone-free status on follow-up CT, time to follow-up, alternative assessments of stone-free status, and size of residual stones.
Definitions
Stone size (length and width) was measured on low-dose noncontrast CT scan (120 kV) using the soft tissue window in axial and coronal planes with 3 mm cuts. Maximum stone attenuation expressed in HU was measured on axial CT images, with the highest recorded value rounded to the nearest 10. Distance to the urinary bladder was measured from the stone to the expected ureteral orifice and rounded to the nearest centimeter.
Stone-free status was assessed for the treated stone only and classified as follows: Grade A: No residual stones detected on postoperative CT scan or complete basket extraction under direct visualization. Grade B: Grade A plus residual fragments ≤2 mm. Grade C: Grade A and B plus residual fragments measuring 2.1–4 mm.
Follow-up imaging was primarily noncontrast CT scan with 3 mm cuts. In four cases, antegrade pyelography or plain radiography of the urinary tract was used.
Statistical methods
Descriptive statistics were used to summarize data. Group comparisons were performed using appropriate parametric or nonparametric tests. Categorical variables were compared using chi-square or Fisher’s exact tests. A sensitivity analysis was performed, including only the first procedure per patient and excluding patients assessed with alternative imaging modalities. A p-value ≤0.05 was considered statistically significant. Analyses were performed using SPSS version 29.0.2.0 (20).
Results
Patient characteristics, pre- and perioperative data
A total of 429 URS lithotripsy procedures under PCS were performed. The mean (SD) age was 58 (15), and 259 patients (60%) were male. The mean (SD) BMI was 28 (5) and 125 patients (29%) had a history of stone disease. Preoperative ureteral stents and nephrostomies were present in 86 (20%) and 43 (10%) of patients, respectively (Table 1). Procedures were performed primarily by consultants (67%), followed by specialists (23%) and residents (10%). A semirigid ureteroscope was used in 99% of cases. The median (IQR) sedation volume was 5.5 mL (3.5–8). Primary stone size mean (SD) was 5.7 (1.9) × 4.6 (1.4) mm and stone attenuation was 686 (264) HU (Table 2, Supplementary Table S3).
Baseline Characteristics of Patients Undergoing Ureteroscopic Lithotripsy with Patient-Controlled Sedation (n = 429)
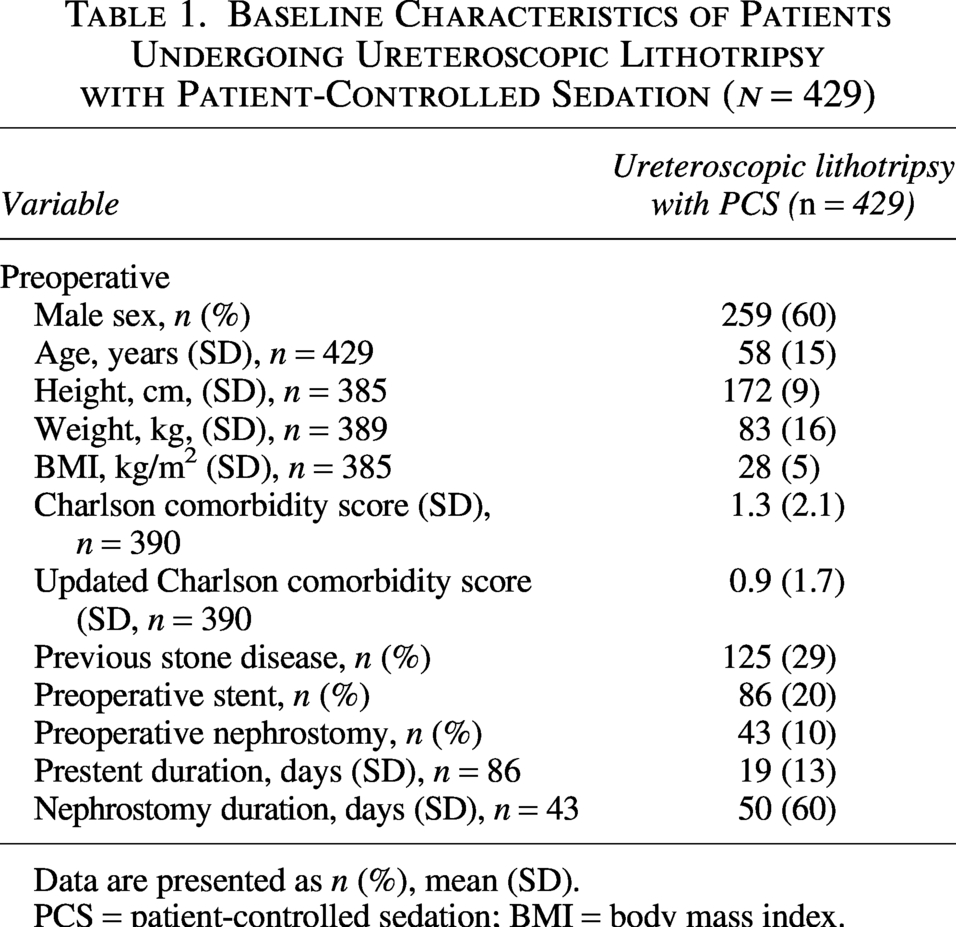
Data are presented as n (%), mean (SD).
PCS = patient-controlled sedation; BMI = body mass index.
Intraoperative and Postoperative Characteristics of Patients Undergoing Ureteroscopic Lithotripsy with Patient-Controlled Sedation (n = 429)
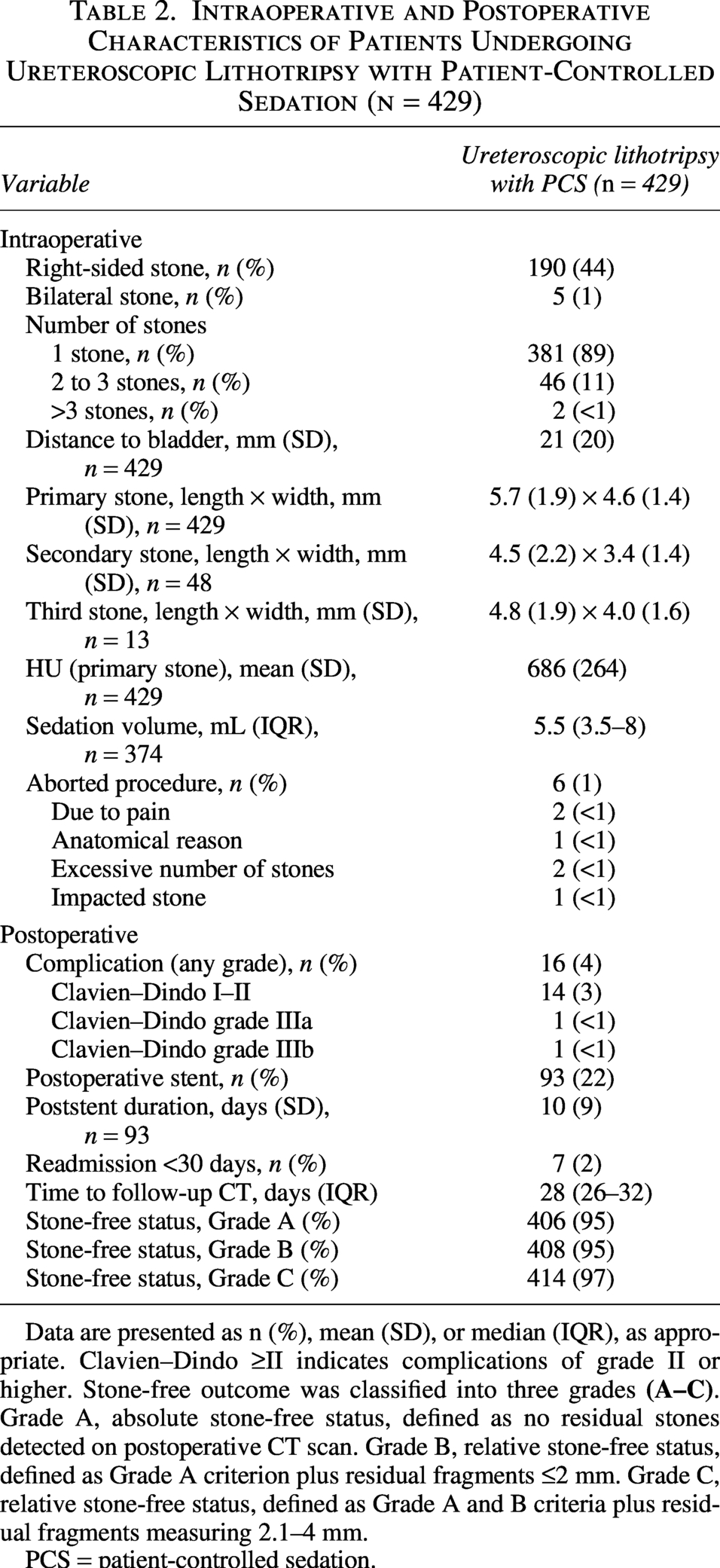
Data are presented as n (%), mean (SD), or median (IQR), as appropriate. Clavien–Dindo ≥II indicates complications of grade II or higher. Stone-free outcome was classified into three grades
PCS = patient-controlled sedation.
Complications and aborted procedures
The procedure was aborted in six patients (1%), most commonly due to excessive stone burden or pain. Postoperative complications occurred in 16 patients (4%), with Clavien–Dindo grade ≥III complications in two patients (<1%). Postoperative ureteral stenting was performed in 93 patients (22%), with a mean (SD) duration of 10 (9) days. Seven patients (2%) were readmitted within 30 days, primarily due to pain or infection. The median (IQR) time to follow-up CT was 28 days (26–32) (Table 2).
Stone-free outcomes
At follow-up, 406 of 429 patients (95%) achieved absolute stone-free status (Grade A); verification was performed by postoperative CT in 278 patients (65%), intraoperative inspection in 124 patients (29%), and alternative imaging in four cases (1%). Relative stone-free rates were 95% for Grade B and 97% for Grade C. Overall, 15 patients (4%) were not stone free at follow-up. Among these, eight patients (2%) had residual fragments >4 mm. Three patients (1%) did not attend the follow-up CT, and four patients (1%) were never referred for follow-up CT examination (Table 2). A minority of patients underwent repeated procedures (n = 18) or were assessed using alternative imaging modalities (n = 4). Sensitivity analyses confirmed the robustness of the primary findings (Supplementary Tables S4, S5, and S6).
Factors associated with non-stone-free status
Patients who were not stone free (5.4%) more often had a history of stone disease 48% vs 28% (p = 0.043) and tended to have a preoperative nephrostomy 22% vs 9% (p = 0.054). Stone size was larger in the non-stone-free group. Primary stone size mean (SD) was 6.6 (2.1) × 5.3 (1.6) mm vs 5.6 (1.9) × 4.6 (1.4) mm (p = 0.011). Patients with more than three stones were exclusively found in the non–stone-free group 9% vs 0% (p = 0.006). Maximum stone attenuation value, mean (SD), tended to be higher in non-stone-free patients, 789 (273) HU vs 680 (263) HU (p = 0.054). Procedures were more frequently aborted in the non-stone-free group 22% vs 0% (p = 0.035), mainly due to excessive stone burden (p < 0.001). No significant differences were observed regarding sex (p = 0.625), age (p = 0.665), BMI (p = 0.153), surgeon experience (p = 0.653), sedation volume (p = 0.653), postoperative complications (p = 0.593), or 30-day readmission rates (p = 0.322) (Table 3 and Supplementary Table S7).
Comparison of Preoperative, Intraoperative, and Postoperative Variables Between Stone-Free and Not Stone-Free Patients
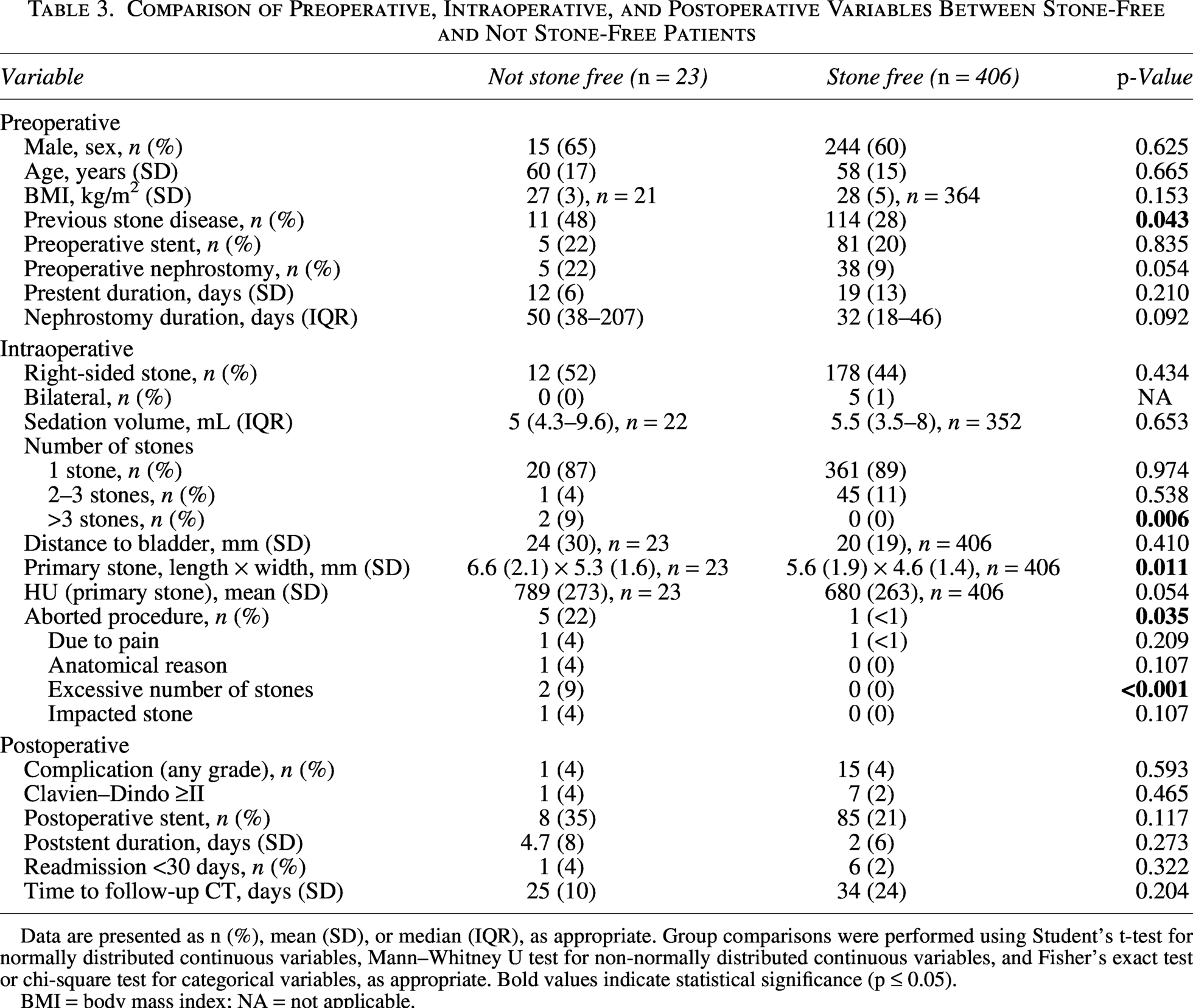
Data are presented as n (%), mean (SD), or median (IQR), as appropriate. Group comparisons were performed using Student’s t-test for normally distributed continuous variables, Mann–Whitney U test for non-normally distributed continuous variables, and Fisher’s exact test or chi-square test for categorical variables, as appropriate. Bold values indicate statistical significance (p ≤ 0.05).
BMI = body mass index; NA = not applicable.
Discussion
This large single-center study demonstrates that PCS is a safe and effective alternative to GA for distal URS lithotripsy. The high absolute stone-free rate (95%) and the low rate of complications (Clavien–Dindo ≥III in 1%) are comparable with outcomes reported for URS lithotripsy under GA and are consistent with previous smaller studies on sedation-based URS lithotripsy1,3–5; furthermore, this study extended the existing evidence by presenting the largest cohort to date using PCS in an endourologic setting. The safety profile observed is notable given the absence of anesthesiology personnel. Almost all procedures were completed on an outpatient basis (99%), with low sedation volumes. The low rate of intraoperative complications, as well as the rare need for aborted procedures (1%), suggests that PCS provided sufficient patient comfort and immobility for effective stone management. These results align with prior research in gastrointestinal and gynecological endoscopy, where propofol–alfentanil PCS has been associated with stable hemodynamics, low risk of oversedation, and rapid recovery.11–14 The fact that deceased patients were not included in the study may have influenced the reporting of complications, as patients could theoretically have died or experienced a severe complication as a result of the procedure. To our knowledge, however, no such serious complication or death has occurred since the method was first implemented. Variability in sedation requirements between patients reflects differences in anxiety, pain perception, body composition, and procedure duration, observed in this study. PCS allows patients to self-titrate sedation, optimizing comfort while minimizing total drug exposure. Previous studies indicate that PCS generally requires lower total doses and produces lower peak sedation compared with anesthetist-controlled sedation.8,9,20–23 Although Nilsson et al., 2012, reported increased respiratory events when alfentanil complemented propofol in PCS, the highest total dose in that early study conducted with anesthesia personnel present was 10 times higher than the maximum dose given in the present cohort, highlighting the safety of our regimen. The overall stone-free rate of 95% is in line with previously reported outcome for URS lithotripsy under GA.1,3–5,24 Nearly all procedures were performed by urologists or residents without anesthesiology support, highlighting the potential of PCS to maintain excellent clinical outcomes while optimizing resource utilization. To account for potential bias from patients undergoing multiple procedures and the few cases assessed with alternative imaging modalities, sensitivity analyses were performed. These analyses confirmed the robustness of the primary findings.
Patients who did not achieve stone-free status more frequently exhibited indicators of increased stone complexity, including a history of recurrent urolithiasis, multiple stones, and larger stone size. These findings are consistent with previous studies as known risk factors for not achieving stone-free status.25–27 The higher prevalence of preoperative nephrostomy likely reflects more complex baseline anatomy or stone burden, as further supported by the proportion of aborted procedures. No associations were observed between outcomes and sedation volume or operator experience, indicating that PCS does not compromise efficacy. These results support PCS as a practical and resource-efficient method for distal URS lithotripsy. By enabling urologist-directed sedation without anesthesiology staff, PCS may improve procedural logistics and reduce health care costs while maintaining high patient safety. The rapid recovery profile and low readmission rate (2%) further support the suitability of PCS for outpatient URS lithotripsy in well-selected cases. However, regulatory framework may limit the feasibility of performing URS with PCS, as this approach is not permitted in all health care systems.
Future studies should evaluate patient-reported outcomes, satisfaction, and recovery experience compared with conventional anesthesia, as well as explore whether PCS can be safely extended to mid-, proximal ureteral, or intrarenal procedures in selected cohorts. This study is limited by its retrospective, single-center design, missing data, and the absence of a GA or regional anesthesia control group. Moreover, all procedures were performed at a single high-volume center with extensive PCS experience, which may limit generalizability. The lack of preoperative anesthesiology assessment may pose a potential risk if conversion to GA is required. To mitigate this, a safety guidewire was routinely placed to allow rapid termination with JJ stent insertion if necessary, and patients with discontinued procedures were subsequently evaluated before planned URS under GA. Another limitation was the lack of standardized assessment of stone complexity, anatomy, and long-term follow-up, as complications such as ureteral stricture may have been missed without routine postoperative CT. Patient-reported outcomes, including satisfaction, comfort, and recovery experience, were not systematically assessed, which limits the evaluation of the patient-centered aspect of PCS. Nonetheless, the large sample size, consistent procedural technique, and detailed clinical data provide a robust overview of PCS for URS lithotripsy in routine clinical practice.
Conclusion
In this study, PCS for URS lithotripsy was safe and effective, achieving a 95% stone-free rate with a low rate of complications. Failure to achieve stone-free status was primarily related to stone complexity rather than sedation or operator factors. These results support PCS as a feasible alternative to GA for distal ureteral stones in selected patients.
Footnotes
Acknowledgments
The authors thank the clinical staff involved in this study.
Authors’ Contributions
J.E. and M.H. contributed to all stages of article development. N.K. verified statistical analyses. J.E., N.K., J.S., F.A., and M.H. contributed to project planning and methodology. All authors participated in the drafting and revising, and approved the final article.
Author Disclosure Statement
M.H. is a member of the National Program Area for kidney and urinary tract diseases. T.T. is a member of the national program group for stone treatment guidelines. All other authors declare no conflicts of interest.
Funding Information
No funding was received for this article.
Supplemental Material
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.