
Abstract
Background and Objective:
Percutaneous nephrolithotomy (PCNL) is the standard of care for treating complex renal stones, but only a minority of urologists in the United States independently obtain percutaneous access. The MONARCH™ Platform, Urology, is an FDA-cleared robotic platform that may simplify percutaneous access and efficiently treat complex renal stones. In this study, we evaluate the clinical, procedural, and patient-reported outcomes using this technology.
Methods:
In a preliminary prospective study in two institutions (University of Wisconsin and Indiana University), patients were enrolled to undergo robotic-assisted mini-PCNL with combined ureteroscopic lithotripsy and followed up to 90 days post-procedure. Percutaneous access was gained using electromagnetic guidance while the patient was in a modified supine position. Stones were removed using a handheld controller to manipulate multiple instruments (i.e., retrograde ureteroscope, laser fiber, basket, flexible antegrade suction catheter) and control a fluid management system.
Results:
Fifteen patients with median (range) linear stone burden of 32.6 (15.0–72.8) mm were enrolled. In 100% of cases, percutaneous access was successfully gained using this technology, and in 73.3% of cases this was achieved within a single attempt. Within this limited and highly heterogeneous study population, we achieved a postoperative day 30 median (range) volume reduction in stone burden of 98.8 (51.9–100.0)% and a stone-free rate (≤4 mm) of 50.0%. One perioperative Grade 3 complication occurred.
Conclusions:
Our initial experience suggests a future where the MONARCH™ Platform may provide urologists with expanded capabilities for safe and effective treatment of select patients with nephrolithiasis.
Introduction
Kidney stones are a common medical condition, affecting 11% of the population in the United States, leading to significant pain, complications, and costly treatments. 1 Percutaneous nephrolithotomy (PCNL) is the standard of care for the removal of complex kidney stones, but it requires advanced skill and is associated with complications including bleeding, infection, and prolonged recovery times. 2 Furthermore, only a minority of urologists in the United States independently obtain percutaneous nephrostomy access3,4 without support from interventional radiology.
Minimally invasive techniques within endourology are transforming the treatment of kidney stones, and robotic-assistance may offer better access, precision, and control, which has the potential to improve patient outcomes, reduce complications, and shorten recovery times. The MONARCH™ Platform, Urology (Johnson & Johnson MedTech Surgery, Santa Clara, California, USA) is an FDA-cleared robotic platform that may enhance the treatment of complex renal stones. The use of this system in a clinical setting is limited to a single-center study, 5 and the study reported here further evaluates the safety and performance of the technology with additional users and patient profiles.
Materials and Methods
Patient selection
Between January and December 2024, following approval by the University of Wisconsin and Indiana University Institutional Review Boards, subjects underwent robotic-assisted combined intrarenal surgery (RACIRS) using the MONARCH™ Platform by two endourology-trained urologists. Adult patients (≥22 years old) were eligible if they had a renal stone burden ≥1 cm identified on a computed tomography (CT) scan with normal upper tract anatomy amenable to PCNL and ureteroscopy and a percutaneous tract length <15 cm.
Patients were excluded from the study if they had any condition that would be contraindicated for conventional ureteroscopy or PCNL, a solitary functioning kidney, impacted ureteral stone, ureteral obstruction, untreated urinary tract infection, renal mass, complete staghorn stone, or implanted electrically or magnetically activated device.
Robotic-assisted combined electromagnetic access, mini-PCNL, and ureteroscopy using the MONARCH™ platform
Patients were positioned in a modified Valdivia-Galadko position (Fig. 1A). The posterior axillary line, the costal margin, and the iliac crest were marked to identify the anterior, superior, and inferior margins for a safe puncture.
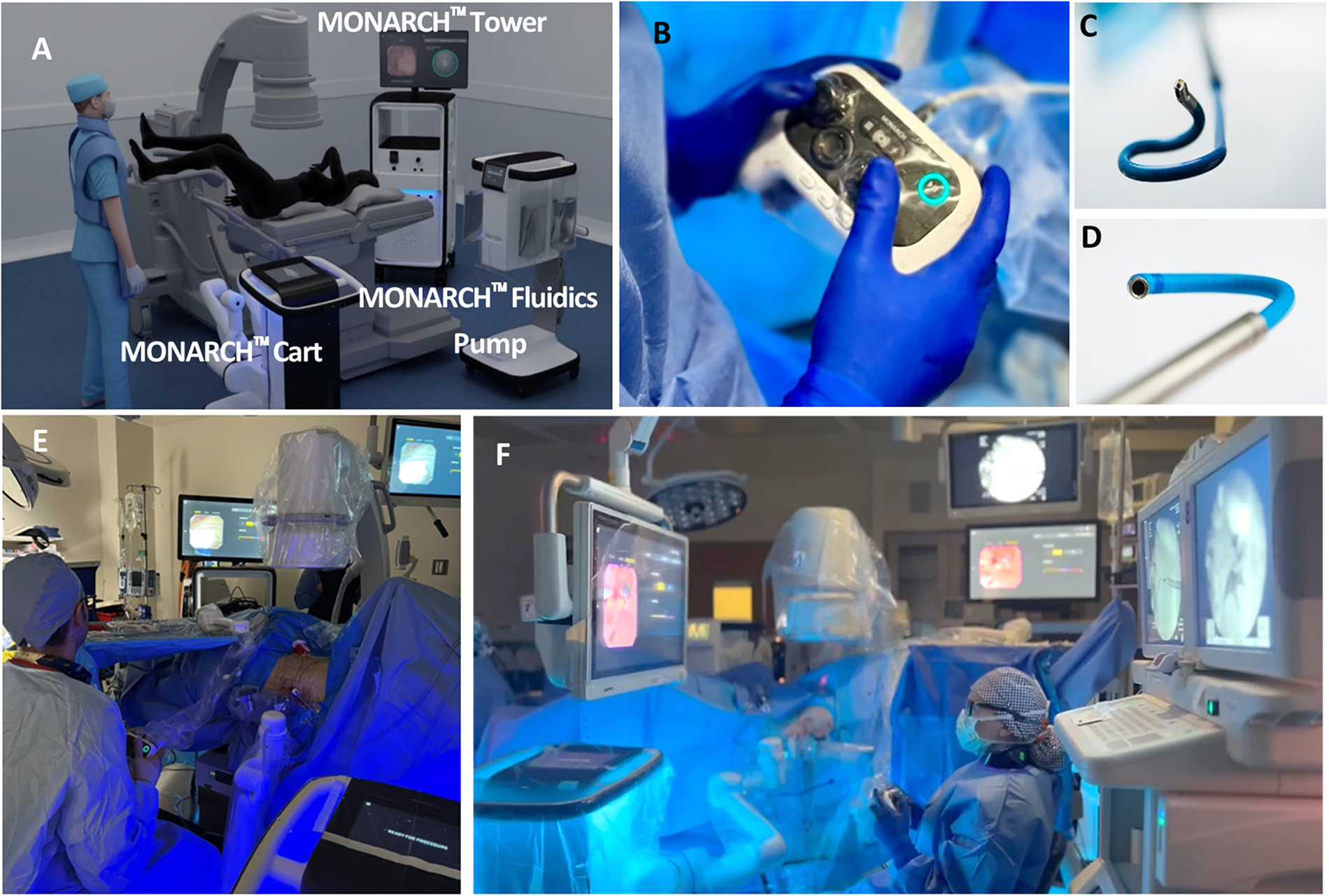
Setup of the operating room to perform mini-PCNL with combined lithotripsy using the MONARCH™ Platform, Urology.
Retrograde access was achieved via conventional cystoscopy techniques. After placing a ureteral access sheath, a 9F ureteroscope was docked onto the robotic arm and manipulated via a handheld controller (Fig. 1B–C) to survey the kidney and locate the stones.
The urologist targeted an appropriate calyx for percutaneous access using the ureteroscopic view and knowledge of the patient’s anatomy from preoperative CT imaging and intraoperative fluoroscopy. An electromagnetic (EM) field generator was mounted by the patient’s flank to detect the relative positions of a manually controlled percutaneous needle and flexible ureteroscope, with EM sensors integrated at the tips of each device. The platform’s software provided guidance to a targeted rendezvous point within the calyx of interest, which was visualized through a novel bullseye graphical user interface. Access was gained under direct ureteroscopic visualization, and fluoroscopy was used as needed.
The percutaneous tract was dilated to accommodate a < 24F (outer diameter) percutaneous sheath. A steerable suction catheter (<16F outer diameter, Fig. 1D) was advanced into the sheath. A laser fiber was introduced into the working channel of the ureteroscope to initiate lithotripsy. Concurrently, the antegrade suction catheter was positioned to relocate stones and actively suction stone fragments and debris during lithotripsy. As needed, a robotically driven basket was introduced to reposition or remove stones. The urologist manipulated all instruments (ureteroscope, basket, laser, and suction catheter) and adjusted irrigation and suction pressures with a handheld controller (Fig. 1B–D).
Postoperative outcomes and data analysis
Subjects were followed until 90 days post-procedure, which included assessments of stone clearance at postoperative days (POD) 1 and 30. The primary end point was procedural completion. Secondary endpoints included POD30 stone-free rate and safety. Additionally, patient-reported outcomes using the Wisconsin Stone Quality of Life Survey (WISQOL) and the Patient-Reported Outcomes Measurement Information System-29 (PROMIS-29) were assessed at screening and POD 1, 30, and 90. The difference in mean score at each POD timepoint was compared to that at screening and evaluated against conservative thresholds for minimally important clinical differences: 9 points for the WISQOL 6 and 5 points for PROMIS-29. 7 Statistical computing was performed using Statistical Analysis Software (SAS Institute, Inc., Cary, North Carolina).
Results
Of the 18 enrolled subjects, 2 subjects were excluded as screen failures (intraoperative discoveries of a caliceal diverticulum and a benign mass in the renal pelvis), and 1 withdrew consent prior to the surgical procedure. The 15 remaining enrolled and treated subjects had a median (range) age of 61 (32–73) years and BMI of 30.6 (22.9–37.7) kg/m2. Most subjects (66.7%) presented with stones in multiple locations within the kidney. In one case, it was discovered intraoperatively that the single stone was fused with the parenchyma, requiring the case to be converted to standard ureteroscopy because of the complexity of the case. In another case, it was discovered that a lower pole stone was impacted within a complex lower pole calyceal system and the entire stone burden could not be reached with the ureteroscope or the percutaneous suction catheter. These two subjects were removed from stone clearance and ablation efficiency assessments because of these confounding factors but were included in summaries of all other parameters. Preoperatively, the remaining subjects had a median (range) linear and volumetric preoperative stone burden of 32.6 (15.0–72.8) mm and 2732.9 (692.5–9349.2) mm3, respectively. Demographic data are summarized in Table 1.
Demographics and Preoperative Characteristics of the N = 15 Subjects Who Underwent Robotic-Assisted Percutaneous Nephrolithotomy Combined with Ureteroscopic Lithotripsy
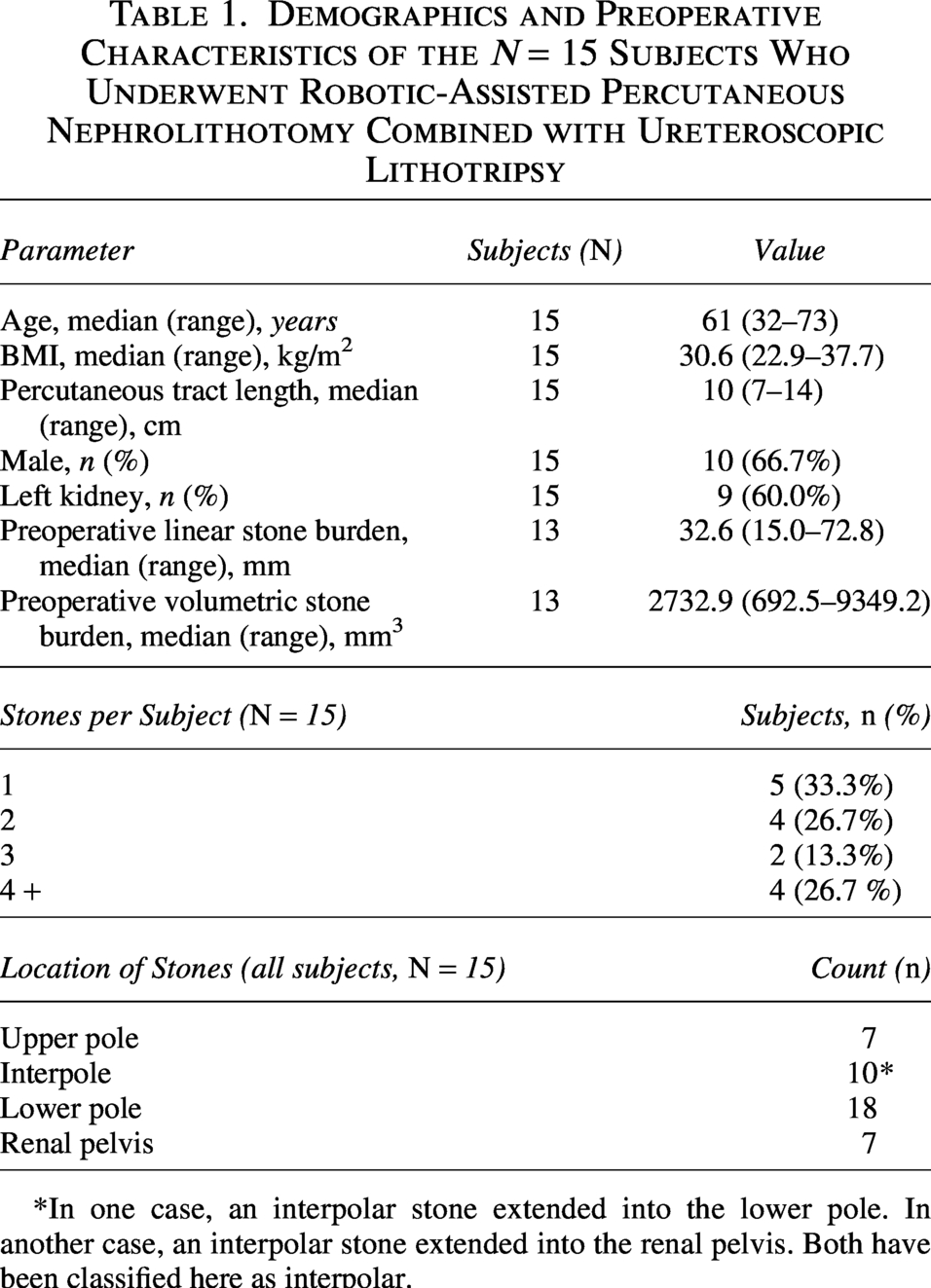
*In one case, an interpolar stone extended into the lower pole. In another case, an interpolar stone extended into the renal pelvis. Both have been classified here as interpolar.
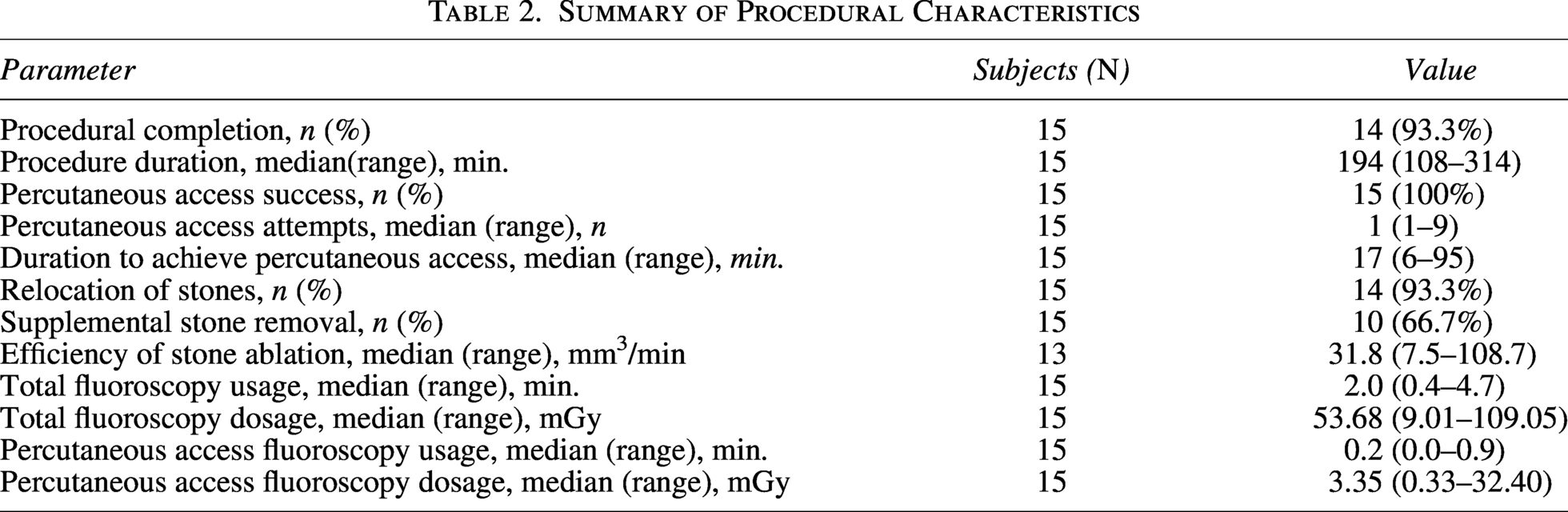
The procedure was successfully completed without conversion in 93.3% (14 of 15) cases. The median (range) total procedure duration, defined from cystoscopy to closure of the percutaneous wound, was 194 (108–314) minutes. Percutaneous access was achieved within 17 (6–95) minutes and was done within a single attempt for 73.3% (11 of 15) of cases. Access was gained within the papilla for 86.7% (13 of 15) of cases, and within the fornix for 13.3% (2 of 15) of cases. Stones were relocated prior to lasing in 93.3% (14 of 15) of cases using: the MONARCH™ Suction Catheter in 60.0% (9 of 15) of cases, the MONARCH™ Basket in 46.7% (7 of 15) of cases, and off-the-shelf tools in 13.3% (2 of 15) of cases. Additional tools were used to facilitate stone removal in 66.7% (10 of 15) of cases: the MONARCH™ Basket was used in 53.3% (8 of 15) of cases, and off-the-shelf tools were used in 13.3% (2 of 15) of cases. The median (range) total dosage of fluoroscopy used was 53.68 (9.01–109.05) mGy. Procedural data are shown in Table 2.
Summary of Procedural Characteristics
Upon procedure completion, 86.7% (13 of 15) of subjects received a ureteral stent, and 13.3% (2 of 15) received a nephrostomy tube per patient preference. The median (range) length of hospital stay was 1 (1–3) night. On POD1, the stone-free rate (≤4 mm) was 53.8% (7 of 13 cases), and the median volume of stone clearance was 99.4% (49.1%−100.0%). One additional subject withdrew from the study prior to POD30. Among remaining subjects, the POD30 stone-free rate (≤4 mm) and volume of stone clearance were 50.0% and 98.8% (51.9%–100.0%), respectively. Notably, 5 of 6 subjects with preoperative linear stone burden of 30 mm or less were stone-free at POD30. An additional subject discontinued prior to POD90. Postoperative data are shown in Table 3. There was not a clear trend between early and late cases in terms of percutaneous access time, stone clearance, or complication rates.
Postoperative Outcomes Following Robotic-Assisted PCNL Combined with Ureteroscopic Lithotripsy Using the MONARCH™ Platform
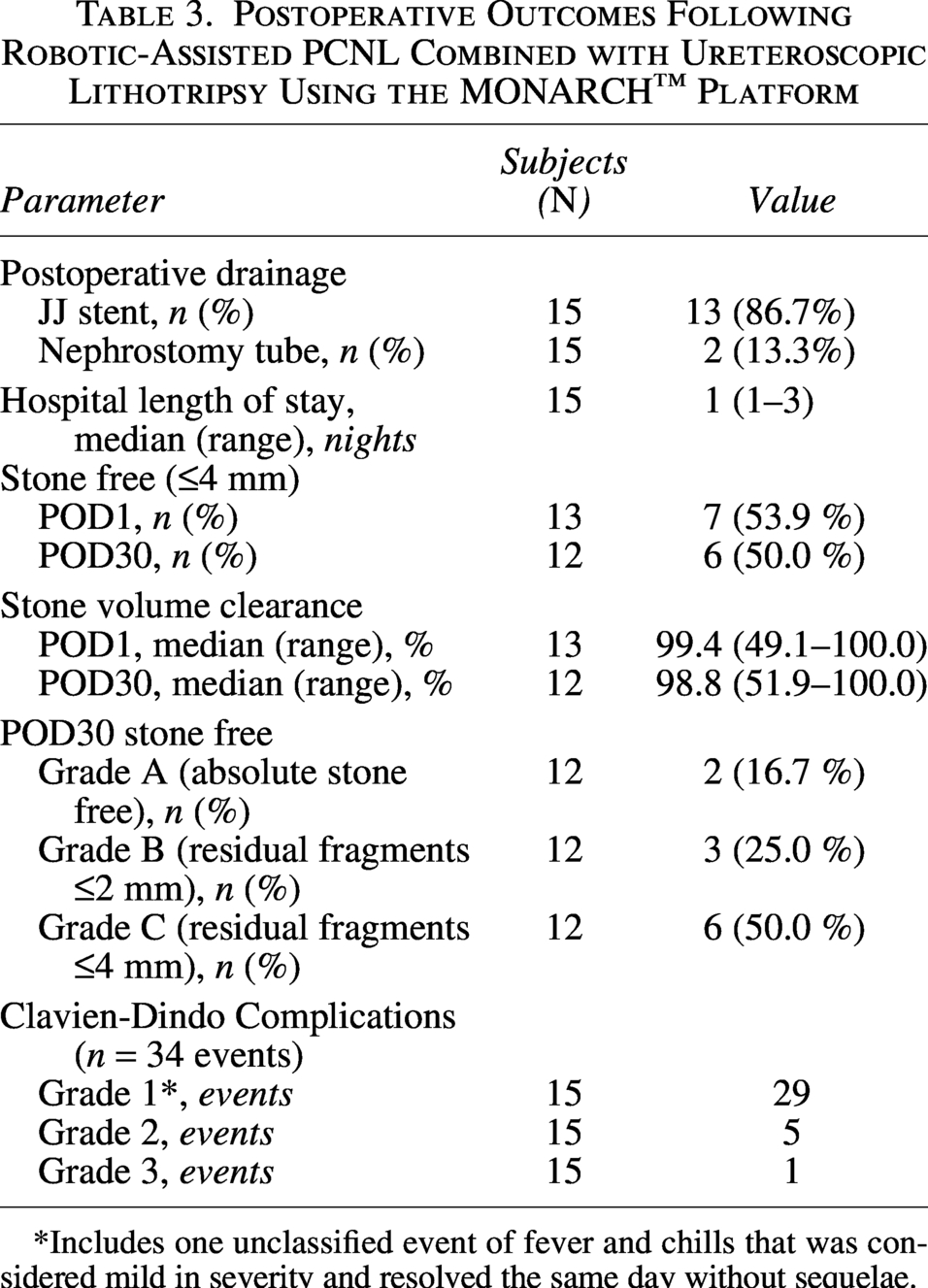
*Includes one unclassified event of fever and chills that was considered mild in severity and resolved the same day without sequelae.
Safety was assessed up to POD90. A single Clavien-Dindo Grade 3 event of intrabdominal fluid accumulation occurred. This was considered a serious adverse event and deemed related to both the device and procedure, required fluid drainage, and resolved without sequelae 3 days later. All other events were classified as either Grade 1 or 2, with the most common being flank pain (7 subjects, 46.7%), bladder spasm (3 subjects, 20.0%), and hematuria (3 subjects, 20.0%).
Analysis of patient-reported outcomes showed that by POD90, significant improvements were observed across total WISQOL scores and Disease Impact and Emotional domains (Fig. 2A). By POD30, subjects exhibited improvements in pain intensity scores (numerical rating scale 0–10, corresponding from “no pain” to “worst imaginable pain”) (Fig. 2B), where 69.2% (9 of 13) subjects rated their pain intensity as “0”. By POD90, 83.3% (10 of 12) of subjects rated themselves as having no pain. By POD90, significant improvements were also observed in the fatigue domain of the PROMIS-29 survey. Other domains and timepoints showed no statistically and clinically significant change from baseline values, though numerical improvements were noted on average for each assessment.
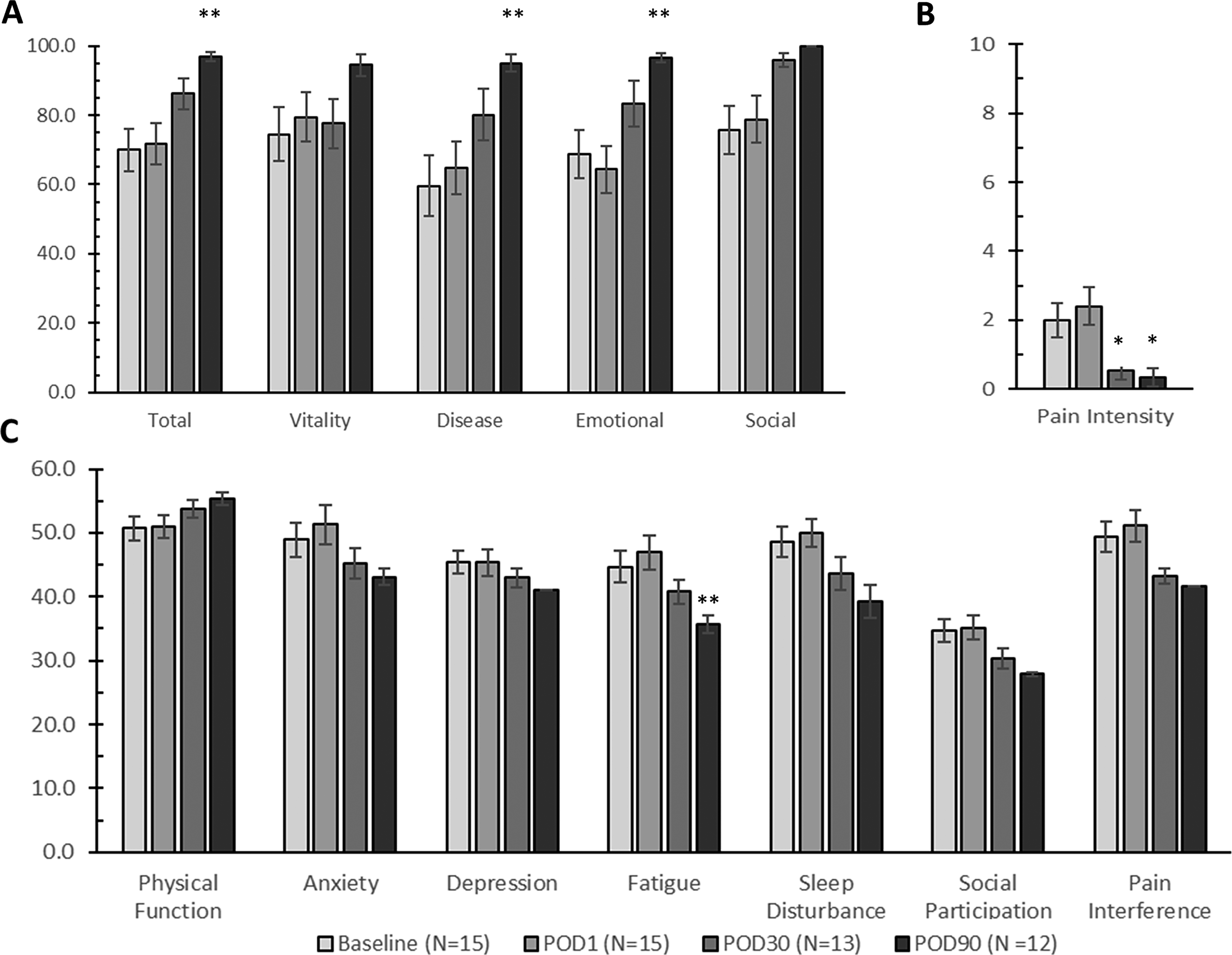
Time course of patient-reported outcomes assessed by the WISQOL and PROMIS surveys.
Discussion
In this series of complex RACIRS cases, we achieved a stone-free (≤4 mm) rate of 50.0%, and a 98.8% reduction in stone volume by POD30. A single Grade 3 safety event of intrabdominal fluid collection occurred. These promising results represent a significant advancement in the field of urology.
The MONARCH™ Platform aims to simplify percutaneous access for urologists. A prior study in cadavers demonstrated that, while using the MONARCH™ Platform, even urologists not typically gaining access independently can do so with a high success rate compatible with urologists who typically gain percutaneous access independently. 8 Both operating urologists in this present study are endourology-trained and perform a high volume of PCNLs. One of the urologists typically utilizes an interventional radiologist for access during traditional PCNL procedures. With the MONARCH™ Platform both urologists were able to independently gain access in each case.
Additionally, we learned that the MONARCH™ Platform allows for more versatility when planning percutaneous access. For a standard PCNL or mini-PCNL, it is ideal to gain access directly on the stone or with the best straight line to the stone. When approaching the case with the MONARCH™ Platform, we can take advantage of the flexibility of these instruments. This allows for percutaneous access in a calyx adjacent to a stone with the ability to move the flexible suction catheter into multiple calyces.
For example, in this study, one subject presented with a large posterior upper pole stone alongside a smaller posterior lower pole stone (Fig. 3A). If the procedure had been performed using a traditional mini-PCNL approach, the urologist would have chosen to gain access in the upper pole. However, with the MONARCH™ Platform, the urologist chose the interpole calyx (Fig. 3B–E) and used this tract to navigate to both the upper and lower poles. This allowed for more flexibility in reaching the stones in multiple locations and decreased the risk of pleural complication by avoiding an upper pole access location.
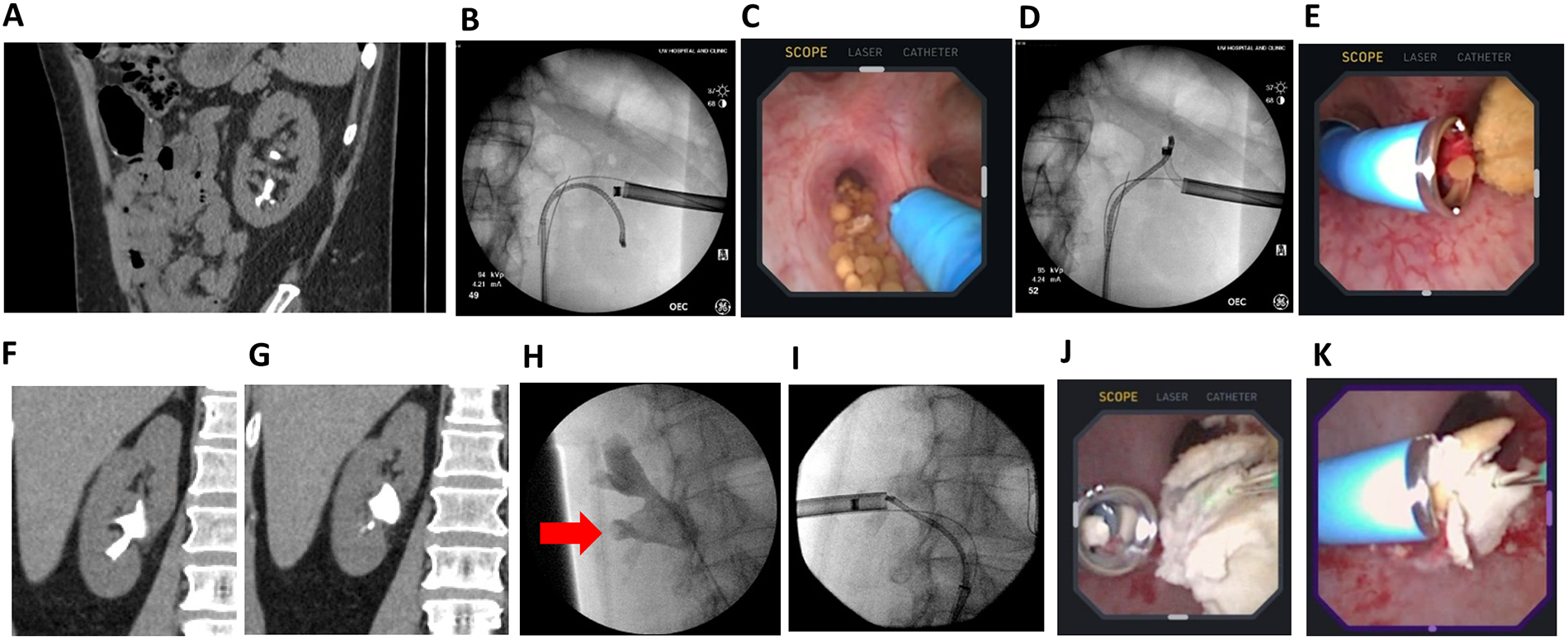
In certain cases, we chose to select a different calyx for percutaneous access while using the MONARCH™ Platform, than we might have selected for a traditional mini-PCNL.
Similarly, another subject presented with a single large stone primarily in the posterior lower pole and extended into the interpole and renal pelvis (Fig. 3F, G). Traditional access would have been through the lower pole, where most of the stone was located. This could have led to challenges accessing the interpolar stone given the acute infundibular angle. However, with the MONARCH™ Platform, the urologist chose to gain access into a posterior interpolar calyx (Fig. 3H, I), and navigate the suction catheter into the lower pole to approach the stone at various angles (Fig. 3J, K). Altogether the MONARCH™ Platform offers greater flexibility while selecting a calyx for percutaneous access.
In recent years, technologies for ureteroscopic stone removal that incorporate suctioning capability have emerged.9–12 In contrast, the MONARCH™ Platform utilizes suction to remove stones through the percutaneous tract. Traditional PCNL procedures also offer percutaneous evacuation of stone fragments via commercially available lithotripters. However, the MONARCH™ Platform allows for the removal of stone fragments of up to 3.3 mm through the suction catheter (Fig. 1D) within the approximately 18 F (inner diameter) percutaneous sheath (i.e., this makes it comparable to a mini-PCNL, instead of standard PCNL with lithotripter). We also found that the flexibility of the suction catheter was well-suited for cases with multiple stones. Additionally, the suctioning capabilities of this tool enable holding larger stones in place during lithotripsy, as well as repositioning smaller fragments (done in 93.3% of cases). The operating urologists frequently relocated stones with the assistance of the suction catheter to allow for more efficient working angles between the ureteroscope and the suction catheter. Furthermore, the balance between suction and aspiration, which can be fine-tuned at the fingertips of the operating urologist, contributes to a very clear visual field during the stone removal procedure. However, it is important for the urologist to use visual cues to avoid over-pressurizing the collecting system, in a similar manner to other endourology procedures. We did experience one serious adverse event where the patient had an accumulation of intrabdominal fluid. It is possible that this was partially related to the fluid pressures. Finally, the MONARCH™ Platform provides an ergonomic advantage in that lithotripsy and stone removal steps are performed by manipulating a handheld controller, allowing the urologist to work in a seated position (Fig. 1E–F). In our study, we found similar stone clearance rates at POD1 and POD30, suggesting that the majority of stone fragments, and dust removal is the result of the procedure itself. Additional studies are needed to compare the ablation and procedural efficiencies with those offered by other technologies.
Measures of patient-reported outcomes are not well studied in this therapeutic field, with limited reports that describe the perioperative impact of specific stone surgical procedure on patient-assessed quality of life.7,13–15 As an exploratory analysis, this study quantified the impact of RACIRS on patient quality of life utilizing the WISQOL and PROMIS-29 surveys. Following treatment with the MONARCH™ Platform, we found significant improvement in pain intensity by POD30. By POD90 patients experienced a significant improvement in the PROMIS-29 Fatigue score, akin to an improvement in this domain demonstrated in a prior longitudinal study following ureteroscopy. 15 Following RACIRS, patients experienced a postoperative total WISQOL score similar to that which has been reported post-ureteroscopy13,14 and PCNL. 14 Additional evaluation in a larger population and across an extended timeframe is needed to validate these findings. This study is limited by its small population of subjects. While the two sites are high-volume centers, they are both tertiary referral centers with a high number of complex cases. Not as many cases fit the inclusion criteria as expected, specifically the percutaneous tract length requirement of <15 cm. The urologists were still on the learning curve of this technology, completing their first 10 and 5 cases, respectively, which may have affected some of the results. Additional experience is needed to assess outcomes, but also to continue to refine surgical technique. The patients treated within this study were heterogeneous when considering the linear stone burden (15.0–72.8 mm) and the number (1–7) and distribution of stones. Further studies with a larger sample size are required to evaluate outcomes in different stone sub-groups more comprehensively. Ultimately, urologists may benefit from this experience to identify ideal patient profiles appropriate for this procedure.
Conclusions
With the MONARCH™ Platform, Urology, we demonstrated promising results of efficient, safe stone treatment in patients with complex stones. This technology offers urologists and their surgical teams an ergonomic and minimally invasive platform through which to provide care. Ultimately, this technology may become a new standard in the treatment of complex kidney stones.
Authors’ Contributions
M.A.K.: Investigation, writing—original draft, editing and reviewing, formal analysis, and supervision. E.C.S.: Investigation. D.C.D.: Investigation. N.L.S.: Conceptualization, writing—original draft, editing and reviewing, and formal analysis. P.T.M.: Conceptualization. M.L.S.: Conceptualization, writing—editing and reviewing, and formal analysis. A.A.: Investigation. M.E.R.: Investigation, writing—original draft, editing and reviewing, formal analysis, and supervision.
Footnotes
Author Disclosure Statement
Margaret A. Knoedler is a paid consultant of Johnson & Johnson MedTech Surgery.
Emily Serrell has no relevant disclosures.
David C. Dalton has no relevant disclosures.
Nancy L. Sehgel is a full-time employee of Johnson & Johnson MedTech Surgery.
Paul T. Morris is a full-time employee of Johnson & Johnson MedTech Surgery.
Michael L. Schwiers is a full-time employee of Johnson & Johnson MedTech Surgery.
Ali Antar has no relevant disclosures.
Marcelino E. Rivera is a paid consultant of Johnson & Johnson MedTech Surgery.
Funding Information
This study was sponsored by Johnson & Johnson MedTech Surgery.