
Abstract
Purpose:
Compare the long-term effectiveness of appendiceal interposition ureteroplasty (AIU) and appendiceal onlay ureteroplasty (AOU) in addressing complex proximal ureteral (CPU) strictures in children.
Patients and Methods:
A retrospective review of patients who underwent minimally invasive AIU and AOU for CPU strictures between March 2010 and August 2020. Patients were stratified into two groups based on the surgical technique: AIU group (n = 11) and AOU group (n = 29). Baseline characteristics, perioperative variables, and follow-up data were assessed in both groups.
Results:
All procedures were completed effectively without the need for conversion. There were no significant differences for the AIU versus AOU groups in median age at operation (p = 0.686), disease side (p = 0.715), preoperative split renal function of the affected kidney (p = 0.906), type of surgical procedure (laparoscopy- vs robot-assisted, p = 0.498), and the mean stricture length (p = 0.166). Operation time was significantly longer in the AIU group (p < 0.001). There were no intraoperative complications, and the estimated blood loss (p = 0.579), postoperative hospital stay (p = 0.557), and Grade I–Ⅱ complications (AIU: 8/11 vs AOU: 18/29, p = 0.715) were similar between the two groups. At a median follow-up of 6 years, the success rates for the AOU group were significantly higher than the AIU group (96.6% vs 54.6%; p = 0.004).
Conclusion:
AOU is a safe and effective technique for managing CPU strictures in children, whereas AIU is not recommended for pediatric patients because of its potential for decreased success rates over time, primarily because of complications such as anastomotic stenosis and progressive hydronephrosis.
Keywords
Introduction
Complex proximal ureteral (CPU) strictures can create difficult reconstructive problems for the urologist and lead to worse quality of life for the patient. 1 For patients with CPU strictures not suitable for end-to-end anastomosis, ileal ureteral replacement and renal autotransplantation are the conventional reconstructive choices. These procedures are commonly acknowledged as technically challenging and come with significant risks related to bowel substitution and vascular anastomosis.2,3 Other options include buccal mucosal graft ureteroplasty and appendiceal ureteroplasty, which have shown encouraging results in selected patients.4–7
The appendix presents a potentially superior choice for a bowel substitute because of its smaller absorptive mucosal area, avoidance of complex bowel anastomosis requirements, and comparable diameter with the native ureter. 6 It has been clearly demonstrated by us and others the safety and viability of appendiceal ureteroplasty, whether performed as an onlay (appendiceal onlay ureteroplasty, AOU) or interposition (appendiceal interposition ureteroplasty, AIU) technique.6–11 Nevertheless, the most effective technique for CPU stricture repair remains unclear because of the absence of any long-term outcome comparative study published to date. Therefore, we conducted a multicenter retrospective study to evaluate the long-term outcomes of laparoscopy- and robot-assisted appendiceal ureteroplasty and compare the therapeutic effects of AOU and AIU, offering a revised perspective on these innovative techniques in the pediatric population.
Patients and Methods
Between March 2010 and August 2020, 40 patients underwent laparoscopy- or robot-assisted laparoscopic appendiceal ureteroplasty by five experienced surgeons at seven medical centers, following institutional review board approval (No. 2023-043-001). Patients were segregated into two groups depending on the surgical technique utilized: the AIU group (n = 11) and the AOU group (n = 29). The inclusion criteria encompassed CPU strictures or defects that were not suitable for end-to-end anastomosis, flap pyeloplasty, ureterocalicostomy, or Boari flaps, provided that the appendix met the necessary length and health requirements. Patients with insufficient appendix length for repairing ureteral defects, those with a history of appendicitis, and individuals who have had an appendectomy were excluded according to the criteria.
Strictures were diagnosed based on ultrasound findings, antegrade urography and/or retrograde urography, magnetic resonance urography/CT urography, as well as 99mTc DTPA scans. Patients with severe hydronephrosis underwent placement of a percutaneous nephrostomy tube before undergoing a renal scan. Patients with urinary tract infections (UTIs) received preoperative antibiotics for treatment. A urinary tract reconstruction procedure in cases of trauma should be delayed until 6 months after the resolution of concomitant injuries.
Surgical techniques and postoperative management
Under general anesthesia, the location and/or length of the stricture were preliminarily confirmed through ureteroscopy, as passing a ureteroscope through a tight stricture is often unfeasible. Whenever possible, a ureteral catheter was inserted up to the level of the stricture to facilitate identification. If this was not achievable, a ureteral catheter was positioned at the distal point of obstruction to act as a marker for locating the ureter during a subsequent ureter reconstruction procedure. A Foley catheter was placed for bladder decompression. All cases were conducted using the transperitoneal approach, positioning patients in a lateral decubitus ranging from 45° to 80°. During laparoscopic procedures, the camera trocar was placed through the umbilicus on the side contralateral to the pathology, with two extra ports inserted under direct vision 3 cm above and below the umbilicus along the midline. A fourth trocar was then introduced in the upper quadrant along the midclavicular line if needed. Three robotic ports were positioned along the median line in robot-assisted procedures, accompanied by two 5 mm assistant ports placed laterally to the rectus line between the robotic trocars. With the aid of the previously inserted ureteral catheter, the ureter was identified. Following the dissection and tailoring of the renal pelvis and upper ureter, patients underwent appendiceal ureteroplasty using the techniques outlined in prior literature.10,11 In cases of strictured ureters with long completely obliterated lumens or extensive defects, an appendiceal interposition tube was used after resecting the diseased ureter to connect the pelvis and the healthy ureter ends (Fig. 1A). When managing partially obliterated lumens, the appendix was detubularized and placed as an onlay flap over the affected portion (Fig. 1B). In instances where a constricted renal pelvis resulted in calix dilation, the appendiceal onlay flap was mobilized and subsequently sutured to the opened renal pelvis. In situations of severely narrowed lumens where the ureter could be reconnected to the pelvis after removing the obliterated segment, the obliterated ureter was excised, and the dorsal ureteral wall was sutured together. Following this, an augmented anastomotic ureteroplasty was performed using an onlay appendiceal technique (augmented onlay). A Double-J stent (Fr 4.7) was placed in an antegrade manner before the completion of the anastomosis.
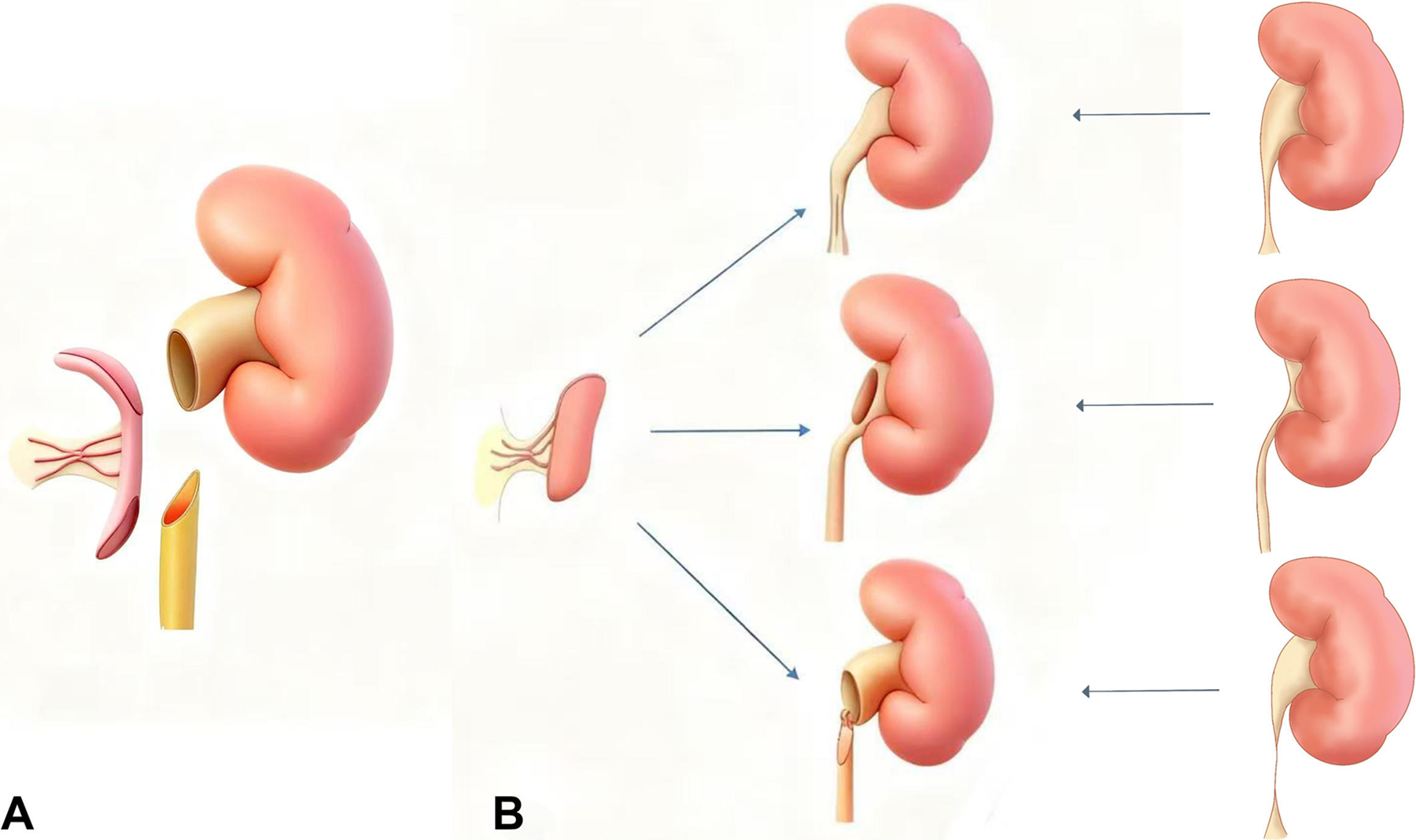
The techniques of appendiceal ureteroplasty.
Intravenous antibiotics were administered to the patients during the operation and were continued for 5 days after the procedure. The Foley catheter was removed on the fifth day following the operation. In cases where patients had a percutaneous nephrostomy tube before operation, the nephrostomy tube will be removed 2 weeks postoperation if no extravasation was observed in antegrade urography or if the patient remains asymptomatic following the clamping of the nephrostomy tube. The stents were removed 8 weeks postoperation, with all patients slated for a ureteroscope examination upon Double-J catheter removal. Following a surgical procedure, patients were monitored at the clinic at 1-, 3-, 6-, and 12-month intervals, with yearly evaluations thereafter. The follow-up protocol comprised urinalysis, urine culture, ultrasound assessments of the urinary system, and symptom evaluations at every appointment. A 99mTc DTPA scan was conducted 6 months postoperatively. Symptomatic relief and the absence of obstruction on imaging assessments confirmed the success. Postoperative complications were evaluated using the Clavien–Dindo classification. 12 Intraoperative and postoperative data, including ureteral stricture length, operative time, estimated blood loss, additional ports required or conversion, postoperative hospital stay, complications, and follow-up outcomes, were thoroughly recorded. A comparison analysis of perioperative and postoperative follow-up data was conducted in both groups, AOU and AIU.
Statistical analysis was performed using GraphPad Prism 10.1.2. Categorical variables were presented as percentages, and continuous variables as mean ± standard deviation (SD) or median with interquartile range (IQR). Group comparisons utilized the chi-squared and Fisher’s exact tests for categorical variables, and Student’s t-test or Mann–Whitney U test for continuous variables. A p-value below 0.05 was deemed statistically significant throughout the study.
Results
Baseline patient characteristics are listed in Table 1. There were no significant differences for the AIU versus AOU groups in median age at operation (60 months, IQR: 38–146 vs 48 months, IQR: 36–69; p = 0.506), gender (p = 0.686), disease side (p = 0.715), and preoperative split renal function of the affected kidney (38.0 ± 7.7 vs 37.7 ± 6.6; p = 0.906). Failed pyeloplasty with endoscopic procedure was the predominant cause of strictures in both the AIU and AOU groups, with prevalence rates of 72.7% and 82.8%, respectively (p = 0.021). Out of 37 patients who experienced failed pyeloplasty, 32 had undergone two or more retrograde endoureterotomy or balloon dilatation procedures before that. The ureteropelvic junction and proximal segments were the most common sites of stricture in both the AIU and AOU groups, with a higher prevalence in the AOU (93.1%) compared with the AIU group (72.7%) (p = 0.025).
Baseline Characteristics of Patients Who Underwent Appendiceal Interposition Ureteroplasty Versus Appendiceal Onlay Ureteroplasty
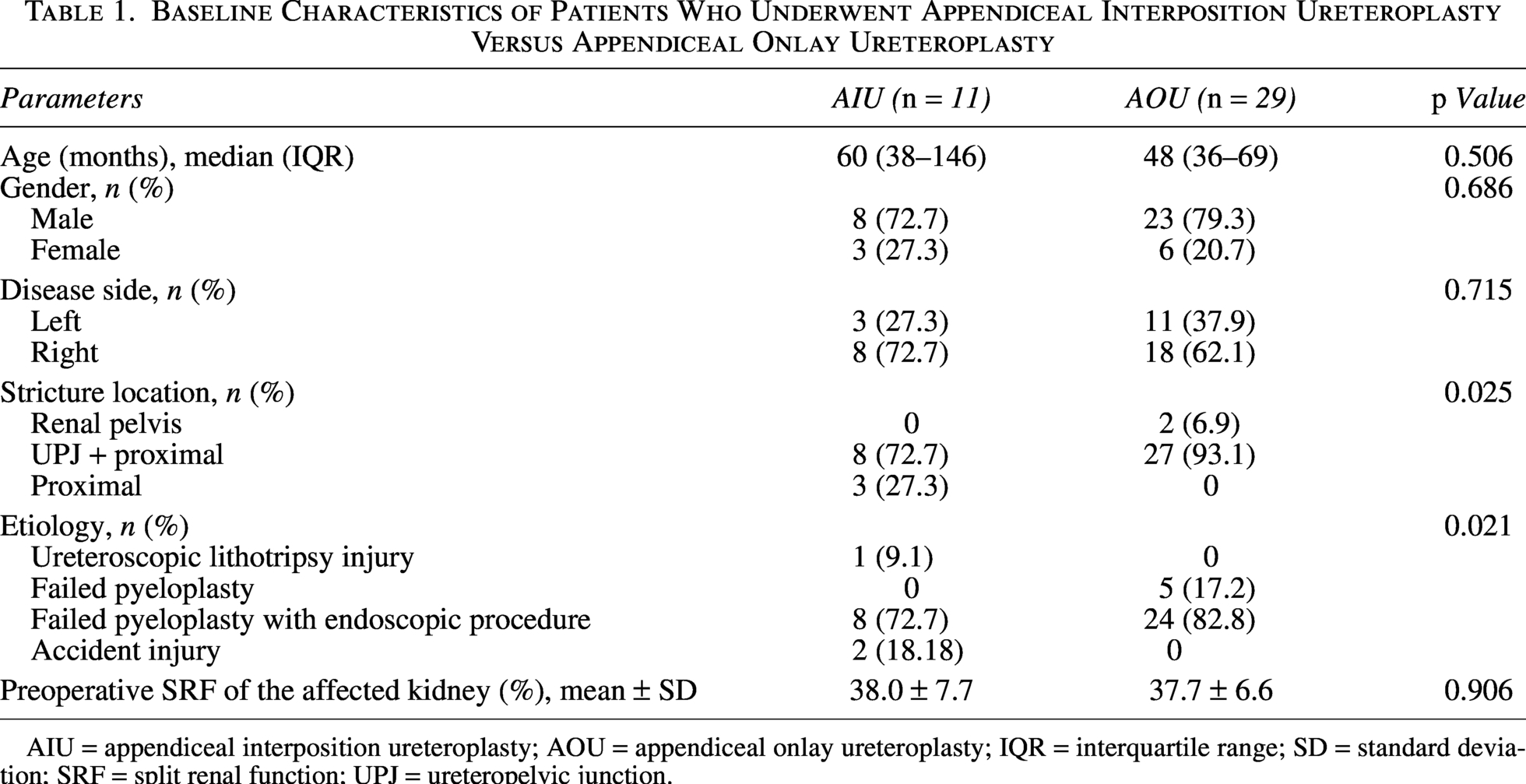
AIU = appendiceal interposition ureteroplasty; AOU = appendiceal onlay ureteroplasty; IQR = interquartile range; SD = standard deviation; SRF = split renal function; UPJ = ureteropelvic junction.
Table 2 outlines the comparison between the AIU and AOU groups in perioperative and follow-up data. All procedures were effectively completed without conversion, with laparoscopic procedures requiring an additional port for anastomosis or appendix mobilization. There were no significant differences between the AIU and AOU groups in the type of surgical procedure (p = 0.498) and mean stricture length (4.8 ± 1.1 cm vs 4.2 ± 1.4 cm; p = 0.166). The operation time was significantly longer in the AIU group (216.0 ± 27.8 minutes vs 161.2 ± 27.6 minutes; p < 0.001). There were no intraoperative complications, and the estimated blood loss (p = 0.579) and postoperative hospital stay (p = 0.557) were similar between the two groups. Comparing the preoperative values, there was an increase in the mean split function of the affected kidney (n = 38; from 37.7% ± 6.7% to 40.6% ± 7.7%, p = 0.008). During the ureteroscope inspection 8 weeks postoperatively, all patients exhibited patent appendiceal grafts with minimal or no mucus in the lumen, and no instances of stone formation were detected.
Comparison of Appendiceal Interposition Ureteroplasty and Appendiceal Onlay Ureteroplasty in Perioperative and Follow-Up Data
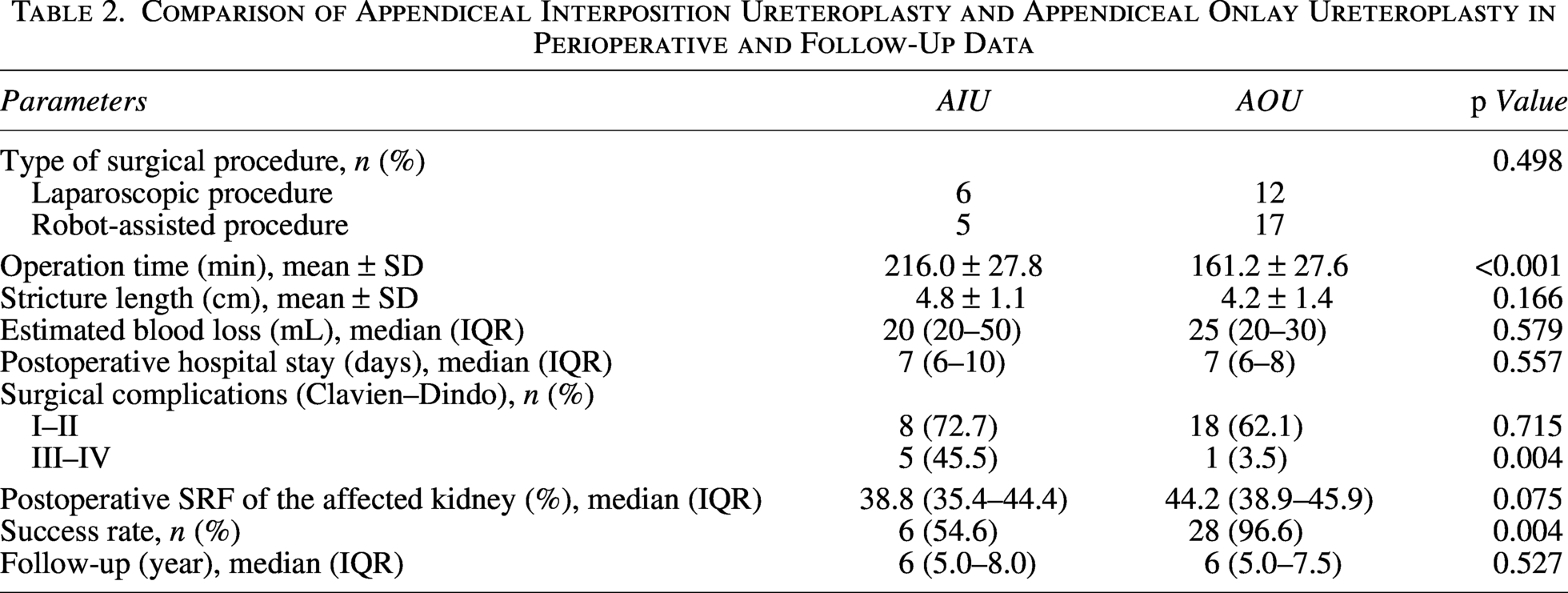
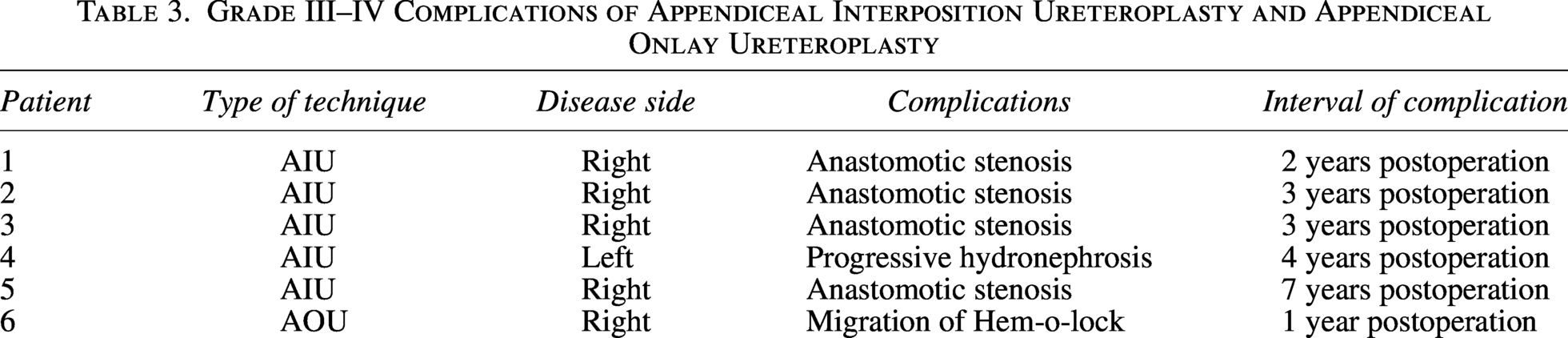
Clavien–Dindo complications showed no significant differences for Grades I–Ⅱ in 72.7% of AIU patients and 62.1% of AOU patients (p = 0.715). Grade III–IV complications were high for the AIU group (p = 0.004). In the AIU group, one case of recurrent UTI and fever was observed 2 years after the initial procedure, with two additional cases occurring 3 years after the initial procedure. Magnetic resonance urography revealed proximal anastomotic stenosis, with subsequent unsuccessful attempts at endoscopic balloon dilation. Consequently, intestinal ureteral replacement therapy was performed. One patient presented with hydronephrosis and renal enlargement 4 years postoperatively, despite remaining asymptomatic for clinical symptoms. Ureteroscopy revealed no urinary tract obstruction; however, renal function deteriorated progressively, necessitating nephrectomy. Another patient experienced flank pain 7 years postoperation and was diagnosed with proximal stenosis of the ureteral anastomosis, which improved following an endoscopic intervention. The patient is currently under rigorous monitoring. Within group AOU, an individual experienced recurring flank pain postoperation at the 1-year mark. Examination via ureteroscopy revealed the migration of the Hem-o-lock clip, which was originally used to fasten the lateral peritoneum, into the ureter. With a median follow-up period of 6 years, the AOU group demonstrated a significantly superior success rate compared with the AIU group (96.6% vs 54.6%; p = 0.004).
Complications were observed in 71.43% (10/14) of left-sided procedures and in 73.08% (19/26) of right-sided procedures, with no statistically significant difference (p = 0.911). It is noteworthy that five out of six Grade III–IV complications were associated with right-sided AIU patients (Table 3), underscoring the predominance of AIU on the right side (8 out of 11 AIU cases were right-sided). Subgroup analysis for AOU showed that the success rate for pure onlay was 13/14 (92.9%) and for augmented onlay was 15/15 (100%), with no significant difference (p = 0.483).
Grade III–IV Complications of Appendiceal Interposition Ureteroplasty and Appendiceal Onlay Ureteroplasty
Discussion
Complex ureteral strictures, typically indicative of ureteral stricture disease unsuitable for end-to-end anastomosis, have posed a long-standing challenge for urologists. 13 Common causes of CPU strictures comprise congenital diseases, trauma, iatrogenic injury, and radiation therapy.1,14 The incidence of this condition has increased in parallel with the rising use of endoscopic procedures. 15 For cases of proximal ureteral stenosis <2 cm, ureteral end-to-end anastomosis is an appropriate treatment option. However, when end-to-end anastomoses are not suitable for CPU strictures, ureteral substitution becomes necessary. The tissue chosen for ureteral repair and reconstruction should possess histological characteristics such as absence of hair, ease of harvesting, adequate vascularity, and resistance to urine exposure. Alternative substitution tissues utilized for ureter reconstruction presently include the ileum, colon, buccal mucosal graft, and appendix. When end-to-end anastomosis is not feasible for patients, conventional reconstructive options include ileal ureteral replacement and renal autotransplantation. The Monti procedure, which involves utilizing a reconfigured ileal segment, has been shown to be a valuable alternative for long-segment ureteral substitution in many reports.16,17 Nonetheless, the intricate nature, high costs, and potential complications of these conventional surgical approaches often dissuade patients from pursuing the high-risk procedures, prompting them to opt for palliative measures such as nephrostomy or ureteral stent placement.2,3
The appendix has long been regarded as a vestigial structure, with a diameter similar to that of the native ureter. Appendiceal ureteroplasty offers advantages over traditional autotransplantation and bowel interposition procedures, including reduced trauma, avoidance of functional intestinal or vascular damage, and a significant decrease in severe complications (Clavien–Dindo III–IV). Furthermore, the risk of metabolic issues and malabsorption syndromes is considered to be lower with the appendix in contact with urine than with the ileum because of its lower surface area and minimal physiological electrolyte transport. 6 In comparison with oral mucosa, the appendix displays a distinct peristaltic function (using appendiceal interposition) and maintains a separate blood supply. The utilization of pedicle appendiceal ureteroplasty obviates the necessity for omentum or perirenal fat coverage, potentially decreasing the risk of ischemic necrosis. In addition, its harvest is relatively simple and does not cause any supplementary complications at the donor site, establishing it as the optimal selection for ureteral replacement reconstruction. Numerous studies have explored the effectiveness of appendiceal repair in treating complex strictures in the upper and lower urinary tracts using techniques including appendiceal interposition, augmented anastomotic repair, onlay, and bypass methods.6–11,18–21 Although medical centers have reported promising short- or medium-term outcomes, there is a scarcity of extensive cases and data regarding the long-term efficacy of appendiceal ureteroplasty in children, with many studies focusing on a singular technique. This study introduces the preliminary comparative evaluation of AIU and AOU, accompanied by long-term follow-up findings from multiple centers.
Our study revealed no significant variances in estimated blood loss, postoperative hospital stay, and low-grade complications (Clavien–Dindo I–II) between the AIU and AOU groups, suggesting the safe feasibility of both procedures through minimally invasive approaches. The application of laparoscopic and robotic platforms in these complex reconstructions provides well-documented advantages, including reduced morbidity, accelerated recovery, and enhanced cosmesis, which are particularly beneficial in the pediatric population.11,22 The robotic platform, used in a portion of our cases, may further facilitate these delicate procedures through enhanced visualization and instrument dexterity.11,23,24 Our results reveal that AIU was associated with a significantly longer operative time. This finding was anticipated, given that AIU involves the complete resection of the stricture and the creation of two separate anastomoses, making it a more intricate and time-intensive procedure compared with the single, long suture line required for an onlay flap.
Our findings demonstrate a notable discrepancy in long-term effectiveness, with AOU showing a markedly superior success rate of 96.6% in contrast to AIU’s 54.6% at a median follow-up of 6 years. This indicates that although both procedures are feasible using a minimally invasive method, AOU emerges as a more enduring and dependable remedy for CPU strictures in pediatric patients. Our findings on AOU align with previous studies in both adult and pediatric populations, consistently demonstrating favorable outcomes for minimally invasive AOU, with success rates exceeding 90%.8,11,25 Analysis of subgroups for AOU revealed a success rate of 92.9% for pure onlay and 100% for augmented onlay, with no statistically significant variance. The superior outcome of the onlay technique likely stems from various factors, based on the fundamental principles of reconstructive procedure. A key advantage of the AOU is the conservation of the native ureteral strip, preserving its intrinsic vascularity and peristaltic function. 8 Despite being fibrotic, the strictured ureteral segment may offer a structural scaffold that could support urothelial coverage and lessen tension on the anastomosis, even if its intrinsic vascularity is compromised. The unsatisfactory long-term outcomes of AIU in our investigation contradict our previous findings and some reports from adult patients,10,25,26 possibly attributed to various factors. First, although we performed generous spatulation of both the ureteral and appendiceal ends, creating a wide anastomosis, the two end-to-end anastomoses in AIU are inherently more susceptible to ischemia and scarring than the long, spatulated onlay suture line, which distributes tension over a larger area. In addition, insufficient mobilization of the appendix and its mesentery may result in angulation or torsion at the anastomosis, particularly as the child grows and the relative position of the kidney and bladder changes. The potential impact of long-term child growth on the spatial relationship between the appendix and the urinary tract remains uncertain regarding its role in failure. An escalation in stenosis rates has been observed in Mitrofanoff appendicovesicostomy patients during prolonged follow-up, as shown in previous studies. 27 Finally, the tubularized interposition graft relies entirely on its mesenteric blood supply. Any compromise in perfusion, however subtle, can endanger the viability of the entire segment, especially at the anastomoses. The elevated rate of late failures observed in our AIU cohort, occurring 2–7 years after operation, strongly indicates a gradual process of ischemic fibrosis and anastomotic contracture. The difference between the prior study and our current outcomes is likely because of the considerably longer follow-up period in our investigation and the distinct features of continuous growth and development in children. This highlights the crucial need for extended monitoring of individuals undergoing intricate ureteral reconstruction procedures and indicates that the initial efficacy of AIU may not endure in the long term.
Several limitations of our study must be acknowledged. The retrospective, multicenter design of the study may lead to selection bias and variations in the surgical technique and postoperative care across participating surgeons. The primary confounding variable is the nonrandomized allocation of surgical techniques. The decision between AOU and AIU depended on the surgeon’s intraoperative evaluation of the stricture, typically opting for AIU in cases of fully occluded lumens or extensive ureter defects. Moreover, the etiologies varied between the groups, with the AIU group showing a higher incidence of traumatic and iatrogenic injuries (3/11) compared with the AOU group (0/29). In the AOU group, failed pyeloplasty was the primary cause. These baseline variations likely introduce confounding factors into the comparison and may partially elucidate the poorer outcomes of AIU, irrespective of the technique itself. Although we found no significant difference in stricture length, the qualitative nature of the obstruction remains a variable that was not entirely controllable. In addition, the limited sample size hampers the statistical power of the analysis. Without randomization, we cannot conclusively attribute the increased failure rate solely to the interposition technique.
Conclusions
This comparative study concludes that minimally invasive AOU is a safe, effective, and durable treatment for CPU strictures in children, exhibiting an outstanding long-term success rate. Conversely, AIU is linked to a high incidence of delayed failure and should be used with caution in the pediatric population. Further prospective large-scale studies are necessary for validation.
Footnotes
Acknowledgments
The authors thank Professor Kan Liu, Wei Cheng, and all the colleagues who helped in the preparation of this article.
Authors' Contributions
P.L., H.Z., and D.L.: Contributed to the study design. Y.Z., Q.Z., Y.Y., N.A., B.L., Z.C., H.C., X.Z., and J.W.: Contributed to data analysis, writing and preparation of this manuscript. All authors contributed to data collection and assisted with manuscript preparation. P.L.: Contributed to the research question and assisted with manuscript revision.
Ethical Approval
This study was approved by the Multicenter Joint Institutional Review Committee (No. 2023-043-001).
Author Disclosure Statement
All authors confirm that they have no affiliations with, or involvement in, any organization or entity that has a financial or nonfinancial interest in the subject matter or materials discussed in this article.
Funding Information
This study was supported by China Capital’s Funds for Health Improvement (2022-2-5083) and the Self-Funded Project by the Municipal and State Health Commission (20253860).