
Abstract
Purpose:
Percutaneous nephrolithotomy (PCNL) is the gold standard for treating large and complex renal calculi, but puncture path selection (papillary vs nonpapillary) remains a critical debate because of bleeding risk concerns. This systematic review and meta-analysis aimed to compare the safety and efficacy of nonpapillary vs papillary access in PCNL.
Methods:
A comprehensive literature search was conducted in the PubMed, Embase, Web of Science, Wanfang, and China National Knowledge Infrastructure databases from inception to December 2025, supplemented by an unpublished dataset from our team’s ongoing clinical study. Eligible studies were comparative trials reporting postoperative hemoglobin drop, complication rate, stone-free rate (SFR), or operative time. Quality assessment was performed using the Cochrane Risk of Bias Tool 2.0 and the Newcastle–Ottawa Scale, with statistical analysis conducted in Stata 17.0.
Results:
A total of nine studies involving 1229 patients (787 in the papillary group and 442 in the nonpapillary group) were included. No significant differences were observed between nonpapillary and papillary access in terms of postoperative hemoglobin drop (mean difference [MD] = 0.159, 95% confidence interval [CI] = −0.365 to 0.683, p = 0.5519), overall complication rate (risk ratio [RR] = 0.949, 95% CI = 0.701 to 1.286, p = 0.7371), blood transfusion rate (RR = 0.835, 95% CI = 0.483–1.443, p = 0.5174), or SFR (RR = 0.970, 95% CI = 0.909–1.035, p = 0.3527). Although no significant overall difference in operative time was found (MD = −1.852, 95% CI = −6.745 to 3.040, p = 0.4580), subgroup analysis of prospective studies revealed that nonpapillary access was associated with a significantly shorter operative time (MD = −6.608, 95% CI = −11.573 to −1.643, p = 0.0091).
Conclusion:
Nonpapillary access is a safe and effective alternative to papillary access for PCNL, with comparable bleeding risk, complication rate, and SFR, and potential efficiency benefits in standardized settings. Urologists can flexibly select the puncture path based on clinical scenarios, with Doppler ultrasound preferred for avoiding vascular-rich regions. Future large-scale randomized controlled trials with standardized protocols and studies on artificial intelligence-assisted fused-image-guided puncture are warranted to further optimize PCNL access strategies.
Introduction
Percutaneous nephrolithotomy (PCNL) is widely recognized as the gold standard for the treatment of renal calculi larger than 2 cm, as well as complex stones such as staghorn calculi. 1 However, since PCNL requires percutaneous penetration of the renal parenchyma, it carries a considerable risk of bleeding—making the selection of puncture path a core critical step in the effective implementation of the procedure. 2 Based on anatomical studies of renal vasculature and the cadaveric research by Professor Sampiao,3,4 the optimal and safest puncture path with the lowest bleeding risk is considered to be a vertical puncture through the papilla of the selected calix, targeting Brödel’s avascular plane. This remains the mainstream consensus in current clinical practice.
Despite its theoretical safety advantage, papillary puncture has inherent drawbacks. It is technically demanding, resulting in a prolonged learning curve for novice urologists.5,6 Moreover, puncture through papillae of different calices presents specific limitations: upper calix puncture carries a risk of pleural injury; middle calix puncture fails to address lower calix stones with steep angulation; and lower calix puncture makes antegrade ureteral stent placement challenging. Consequently, in clinical practice, management of large or multicentric caliceal stones often requires multiple access tracts to achieve a high stone-free rate (SFR), increasing procedural complexity and potential morbidity. 7
In response to these limitations, researchers have proposed the concept of nonpapillary puncture. Theoretically, this approach offers several advantages: a larger target area, lower technical difficulty, and shorter operative time; the ability to manipulate stones from the caliceal neck to the calix, preventing stone migration; enhanced nephroscope maneuverability, which reduces the need for multiple access tracts when treating large, multicentric, or staghorn calculi; and easier identification of the ureter for antegrade stent placement.
Kyriazis et al. first validated the clinical safety and feasibility of nonpapillary puncture in a prospective cohort of 137 patients, reporting shorter operative time, higher SFR, minimal bleeding, and low complication rates. 7 Subsequent studies have confirmed the feasibility of nonpapillary puncture in patients with staghorn calculi and renal malformations, and consistent conclusions have been drawn for nonpapillary puncture combined with miniaturized access tracts.8–10 However, conflicting evidence emerged from a porcine study by Hao et al., which found a higher bleeding risk with nonpapillary puncture compared with papillary puncture. 11
In recent years, a growing number of comparative studies have been conducted to further explore the feasibility of nonpapillary puncture. Studies by Kallidonis et al., Budak et al., Tahra et al., Kashi et al., Farshid et al., and Amer et al. have consistently shown no significant differences between the two approaches in terms of bleeding, complication rate, operative time, or SFR, supporting the safety and feasibility of nonpapillary puncture.12–18 In contrast, a recent study by Li et al. and a retrospective analysis of data from our own institution (the First Affiliated Hospital of Nanjing Medical University) suggested that nonpapillary puncture was associated with a higher bleeding risk and complication rate compared with papillary puncture. 19
Given the persisting absence of consensus regarding the comparative safety and efficacy of nonpapillary vs papillary access in PCNL, we conducted this systematic review and meta-analysis to synthesize the available evidence. Our primary objective was to evaluate the impact of access site on postoperative hemoglobin drop, with secondary outcomes including complication rates, SFRs, and operative times, aiming to provide evidence-based guidance for clinical decision-making.
Methods
Data sources
A comprehensive literature search was conducted in the PubMed, Embase, Web of Science, Wanfang database (https://www-wanfangdata-com-cn-s.web.bisu.edu.cn/), and China National Knowledge Infrastructure (https://cn.oversea.cnki.net/) from inception to December 2025. The search terms included the following: “percutaneous nephrolithotomy,” “PCNL,” “renal access,” “papillary puncture,” “non-papillary puncture,” “calyceal puncture,” and “renal puncture” and combined with manually searching the reference lists of published high-quality reviews. The specific search query for the literature database is as follows: ((percutaneous nephrolithotomy [Title/Abstract]) OR (PCNL [Title/Abstract])) AND ((renal access [Title/Abstract]) OR (papillary puncture [Title/Abstract]) OR (non-papillary puncture [Title/Abstract]) OR (calyceal puncture [Title/Abstract]) OR (renal puncture [Title/Abstract])). No language restrictions were applied.
In addition to published literature, one additional dataset was derived from an ongoing clinical study conducted by our research team—this study focuses on other aspects of PCNL for complex renal calculi, has obtained ethical approval from the Ethics Committee of the First Affiliated Hospital of Nanjing Medical University (Approval No. 2022-SR-385), and has secured written informed consent from all patients before a surgical procedure. Notably, this ongoing study contains comparative data on nonpapillary vs papillary access, which fully meets our meta-analysis inclusion criteria and has no overlap with any previously published studies. Detailed characteristics and outcomes of this study are provided in Supplementary Table S1 to ensure full transparency.
For this team-collected dataset, data extraction was performed independently by two reviewers using the same standardized form applied to published literature. To ensure data accuracy, all extracted information was cross verified against the original study’s case report forms; any discrepancies identified during this process were resolved through group discussion. Consistent with the quality assessment protocol for other included observational studies, this dataset was evaluated using the Newcastle–Ottawa Scale (NOS) to ensure methodological rigor.
Study selection
Studies were included if they (1) compared nonpapillary vs papillary access in patients undergoing PCNL; (2) reported at least one of the predefined outcomes (postoperative hemoglobin drop, complication rate, SFR, or operative time); and (3) were randomized controlled trials (RCTs) or observational studies with a comparative design. Animal experiments or in vitro studies, reviews, case reports, and studies without a control group were excluded.
Data extraction
Two independent reviewers extracted the following data: first author, publication year, study design, sample size, patient demographics, stone characteristics, surgical details, and outcome measures. Discrepancies were resolved through consensus.
Quality assessment
The Cochrane Risk of Bias Tool 2.0 (ROB 2.0) was adopted to assess the methodological quality of RCTs. 20 This tool evaluates five core domains of bias, including bias arising from the randomization process, bias because of deviations from the intended interventions, bias because of missing outcome data, bias in measurement of the outcome, and bias in selection of the reported result. Each domain was independently rated as low risk, some concerns, or high risk of bias by two reviewers, with any discrepancies resolved through consensus.
For observational studies (including retrospective cohort, prospective cohort, and case–control studies), the NOS was utilized for quality assessment. This scale comprises three dimensions: selection of study groups (four items, including representativeness of the exposed cohort, selection of the nonexposed cohort, ascertainment of exposure, and demonstration that the outcome of interest was not present at the start of the study), comparability of study groups (two items, focusing on control of the most important confounding factors and additional confounding factors), and outcome assessment (three items, including the method of outcome assessment, sufficiency of follow-up time, and completeness of follow-up). Each eligible item was scored 0 or 1, with a total score ranging from 0 to 9. Studies were categorized into three tiers based on the total score: high quality (7–9 points), moderate quality (4–6 points), and low quality (0–3 points).
Statistical analysis
All analyses were performed using Stata 17.0. For continuous outcomes (postoperative hemoglobin drop, operative time), the mean difference (MD) with 95% confidence intervals (CI) was calculated. For dichotomous outcomes (complication rate, SFR), the risk ratio (RR) with 95% CI was used. Heterogeneity was evaluated using the I2 statistic and χ2 test. A random-effects model was used for I2 >50%, and a fixed-effects model was used for I2 ≤50%. Sensitivity analyses were performed by sequentially excluding individual studies to assess the robustness of results. Publication bias was evaluated using Egger’s and Begg’s tests, along with funnel plots. Subgroup analyses were conducted to explore the potential sources of heterogeneity, including region, study design, and stone size.
Results
Literature search and study characteristics
A total of 847 studies were retrieved through the systematic literature search. After sequential screening based on the inclusion and exclusion criteria, eight published studies and a retrospective analysis of data from our own institution (the First Affiliated Hospital of Nanjing Medical University) were finally included in this meta-analysis, and the detailed literature search process is illustrated in Figure 1.
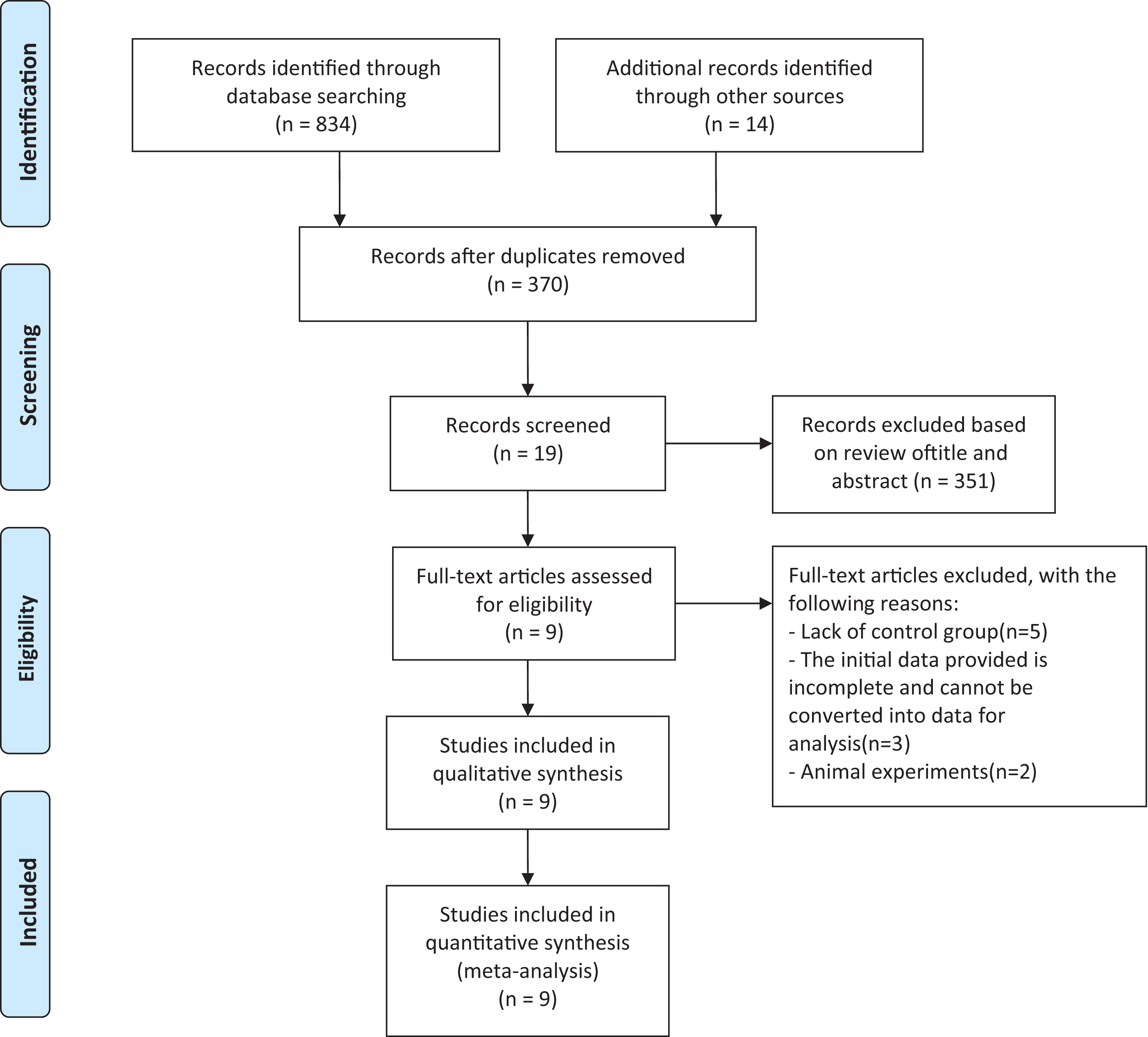
Flow diagram of study selection process.
Among the included studies, two were RCTs and seven were observational studies (one prospective and six retrospective), with publication years ranging from 2017 to 2025. A total of 1229 patients were enrolled, with 787 cases in the papillary access group and 442 cases in the nonpapillary access group. The basic characteristics of the included studies are summarized in Table 1. Specifically, postoperative hemoglobin drop was reported in eight published studies, but only five provided complete data on mean and standard deviation (SD); overall complication rates were documented in seven studies; SFRs were reported in seven studies; and operative time was described in all the nine included studies, with complete mean and SD data available in seven studies (Table 2).
Main Characteristics of Studies Included in This Meta-Analysis
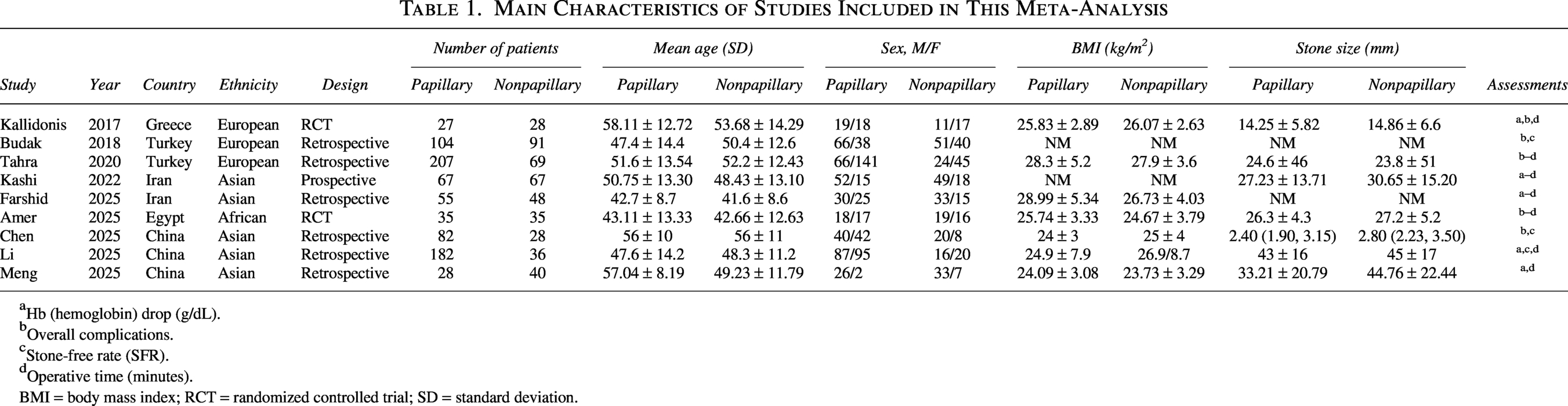
Hb (hemoglobin) drop (g/dL).
Overall complications.
Stone-free rate (SFR).
Operative time (minutes).
BMI = body mass index; RCT = randomized controlled trial; SD = standard deviation.
Summary of Outcome Measures
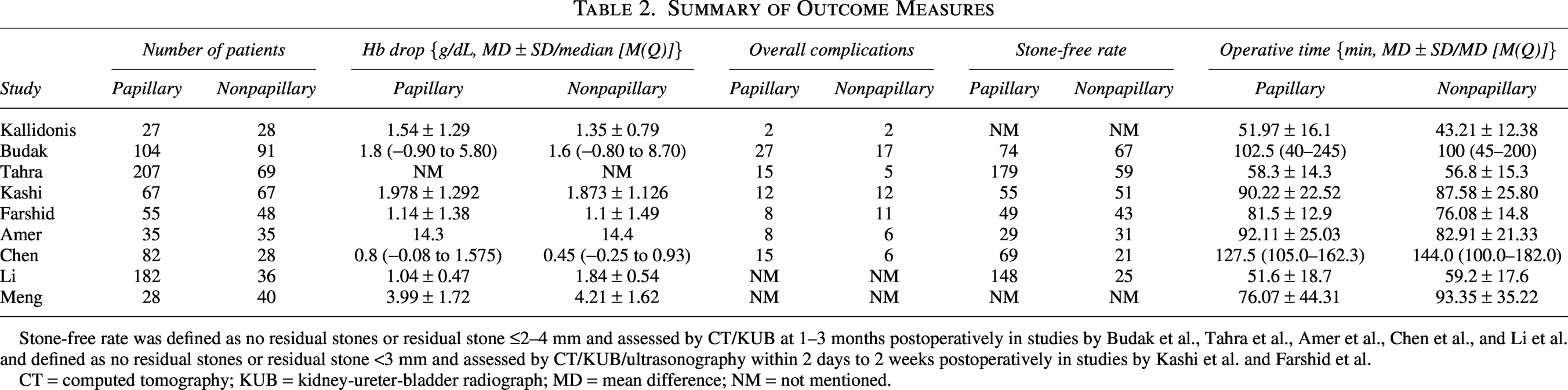
Stone-free rate was defined as no residual stones or residual stone ≤2–4 mm and assessed by CT/KUB at 1–3 months postoperatively in studies by Budak et al., Tahra et al., Amer et al., Chen et al., and Li et al. and defined as no residual stones or residual stone <3 mm and assessed by CT/KUB/ultrasonography within 2 days to 2 weeks postoperatively in studies by Kashi et al. and Farshid et al.
CT = computed tomography; KUB = kidney-ureter-bladder radiograph; MD = mean difference; NM = not mentioned.
The results of quality assessment are presented in Figure 2. For the two included RCTs, the risk of bias was low in the domains of random sequence generation, completeness of outcome data, outcome measurement, and selective outcome reporting (Fig. 2A). All seven observational studies achieved an NOS score of ≥7, thus being classified as high-quality studies (Fig. 2B).
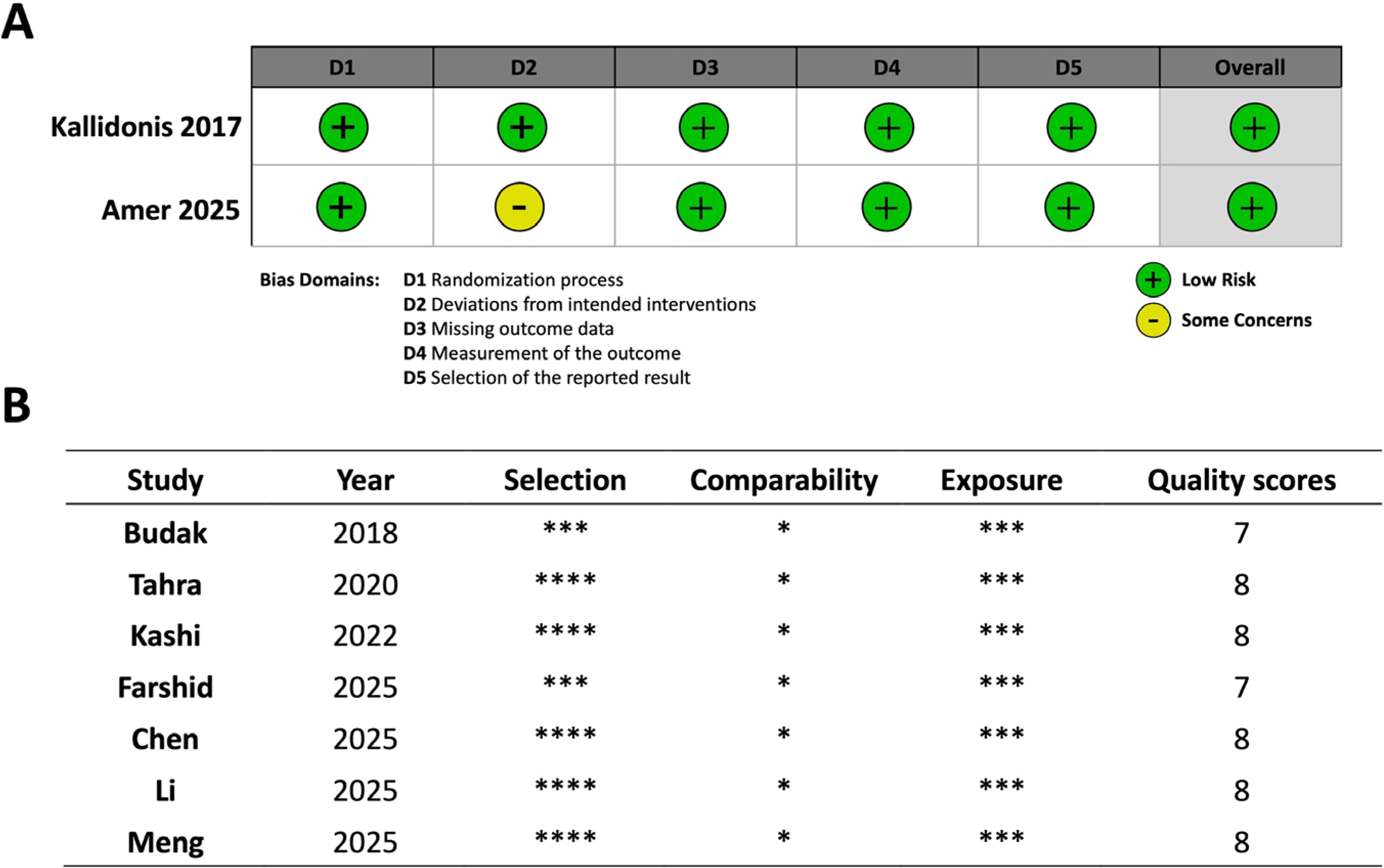
Literature quality assessment results.
Comparative analysis of nonpapillary vs papillary access in PCNL: Hemoglobin drop, complications, SFR, and operative time
Postoperative hemoglobin drop was evaluated across five studies using a random-effects model (Fig. 3A). No statistically significant difference was observed between the nonpapillary and papillary access groups (MD = 0.159, 95% CI = −0.365 to 0.683, p = 0.5519), but high heterogeneity was detected (I2 = 86%, p < 0.0001). This high heterogeneity was primarily attributed to the study by Li et al. (2025) (Fig. 3B). After excluding the primary source of heterogeneity, a fixed-effects model still showed no significant between-group difference (MD = −0.075, 95% CI = −0.345 to 0.194, p = 0.5842), with heterogeneity completely eliminated (I2 = 0%, p = 0.8711; Fig. 3C). No publication bias was identified (Egger’s test p = 0.2884; Begg’s test p = 0.4969; Fig. 3D). In addition, subgroup analyses by region (Fig. 3E) and study design (Fig. 3F) also revealed no significant differences between subgroups.
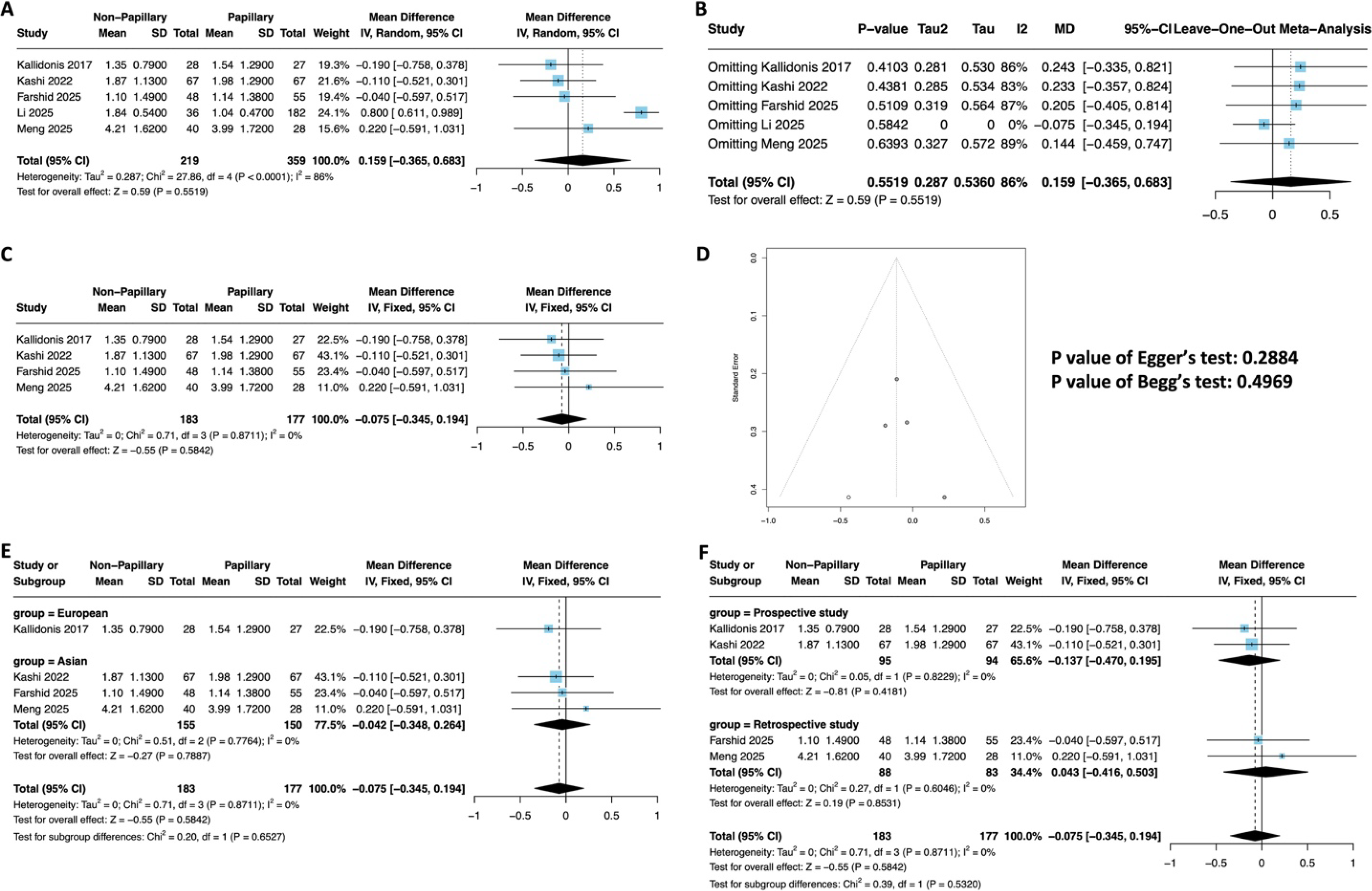
Meta-analysis of postoperative hemoglobin drop between nonpapillary and papillary access groups.
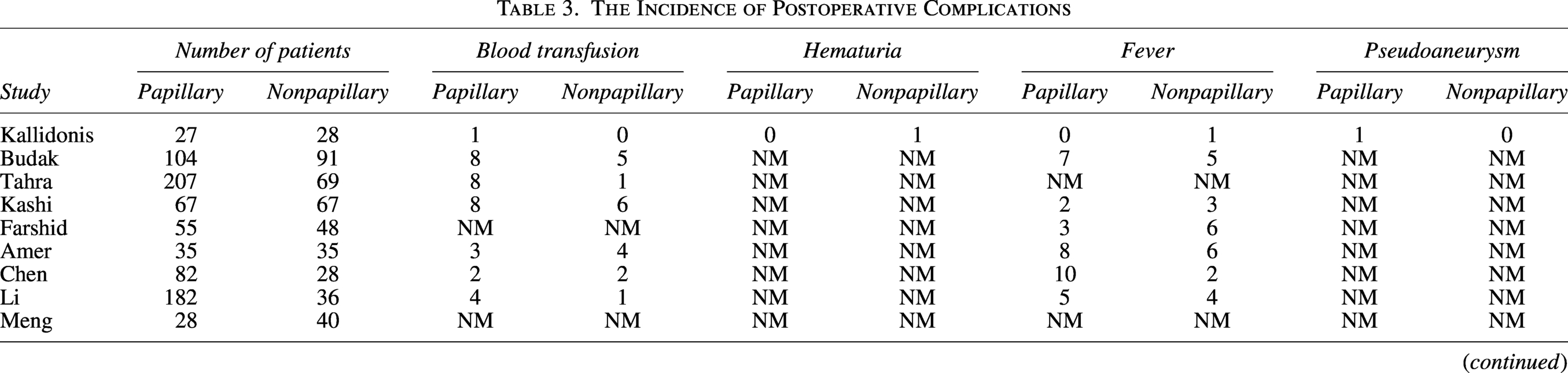
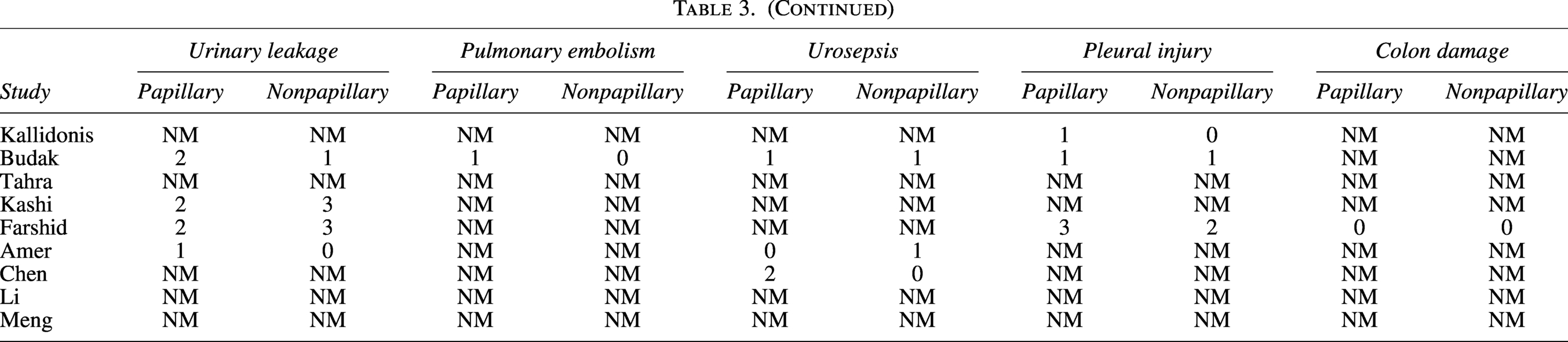
For the overall complication rates, seven studies were pooled using a fixed-effects model. The RR of complications in the nonpapillary group relative to the papillary group was 0.949 (95% CI = 0.701–1.286, p = 0.7371; Fig. 4A), indicating no significant difference. No heterogeneity (I2 = 0%, p = 0.8117) or publication bias (Egger’s test p = 0.4321; Begg’s test p = 0.8806; Fig. 4B) was observed. Table 3 presents the occurrence of complications recorded in the included literature. For blood transfusion rates, seven studies were analyzed using a fixed-effects model (Fig. 4C). The RR of transfusion in the nonpapillary group was 0.835 (95% CI = 0.483–1.443, p = 0.5174), with no significant difference between the groups. No heterogeneity (I2 = 0%, p = 0.7748) or publication bias (Egger’s test p = 0.9167; Begg’s test p = 0.6523; Fig. 4D) was detected.
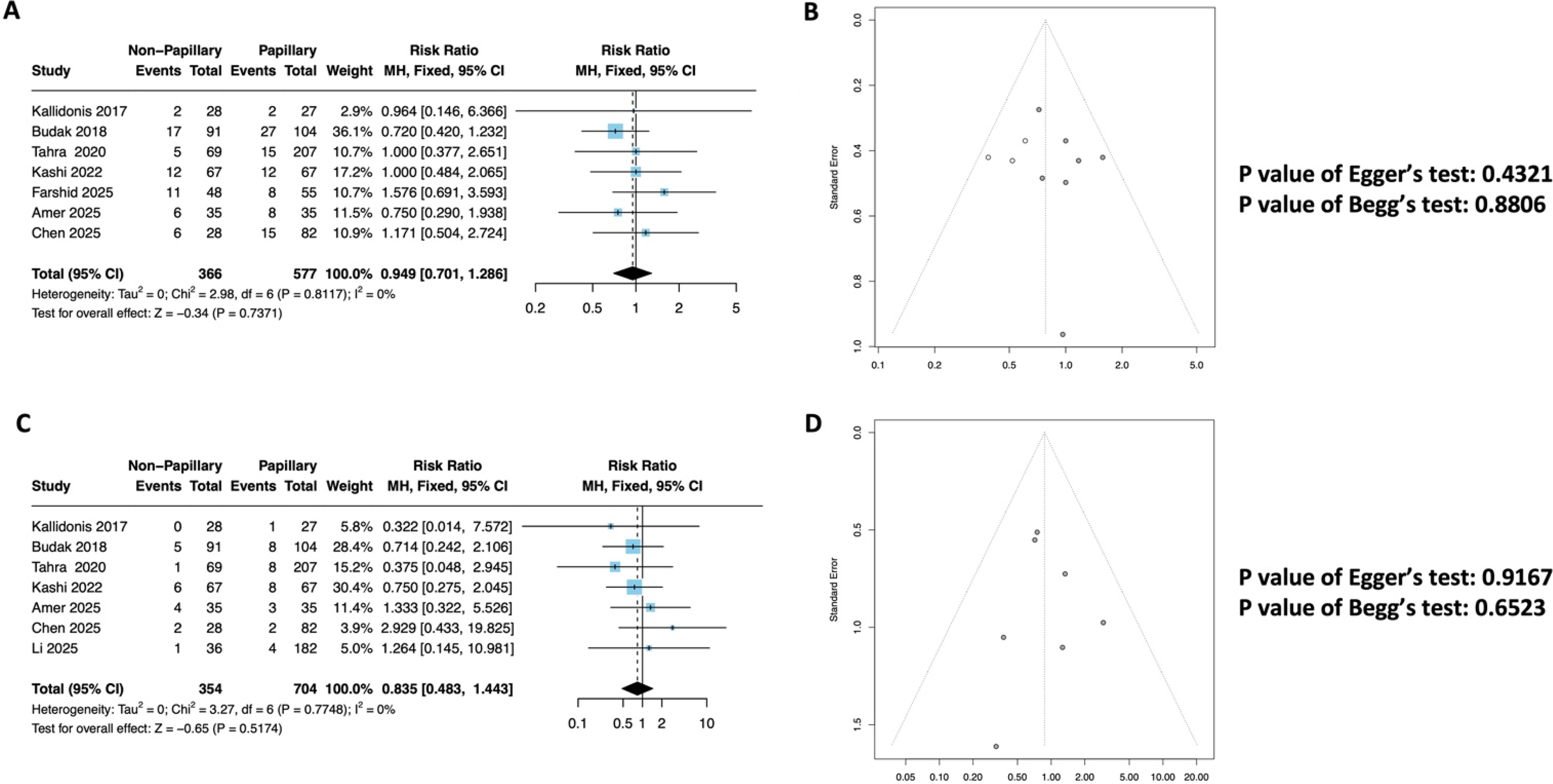
Meta-analysis of overall complication and blood transfusion rates between the nonpapillary and papillary access groups.
The Incidence of Postoperative Complications
Regarding the SFR, a fixed-effects model was applied to seven studies (Fig. 5A). Among the seven included studies that reported an SFR, five studies (Budak et al., Tahra et al., Amer et al., Chen et al., Li et al.) assessed the SFR at 1–3 months postoperatively, primarily using CT, with some cases evaluated by kidney-ureter-bladder radiograph (KUB). SFR was defined as no residual stones or residual stone ≤2–4 mm. The remaining two studies (Kashi et al., Farshid et al.) assessed the SFR within a shorter term (2 days to 2 weeks postoperatively), using CT, KUB, or ultrasonography, with SFR defined as no residual stones or residual stone <3 mm.

Meta-analysis of stone-free rate between the nonpapillary and papillary access groups.
The RR of achieving a stone-free status in the nonpapillary group was 0.970 (95% CI = 0.909–1.035, p = 0.3527), demonstrating no significant difference between the groups. No heterogeneity (I2 = 0%, p = 0.6927) or publication bias (Egger’s test p = 0.2995; Begg’s test p = 0.4527; Fig. 5B) was observed.
Operative time was analyzed across seven studies using a random-effects model. No significant difference was found between the nonpapillary and papillary access groups (MD = −1.852, 95% CI = −6.745 to 3.040, p = 0.4580; Fig. 6A), with moderate heterogeneity (I2 = 68%, p = 0.0046). Sensitivity analysis confirmed the robustness of this finding (Fig. 6B). Subgroup analyses by region (Fig. 6C) and stone size (Fig. 6E) did not identify significant sources of heterogeneity. Notably, in the prospective study subgroup (three studies), the nonpapillary access group was associated with a significantly shorter operative time compared with the papillary access group (MD = −6.608, 95% CI = −11.573 to −1.643, p = 0.0091; Fig. 6D).
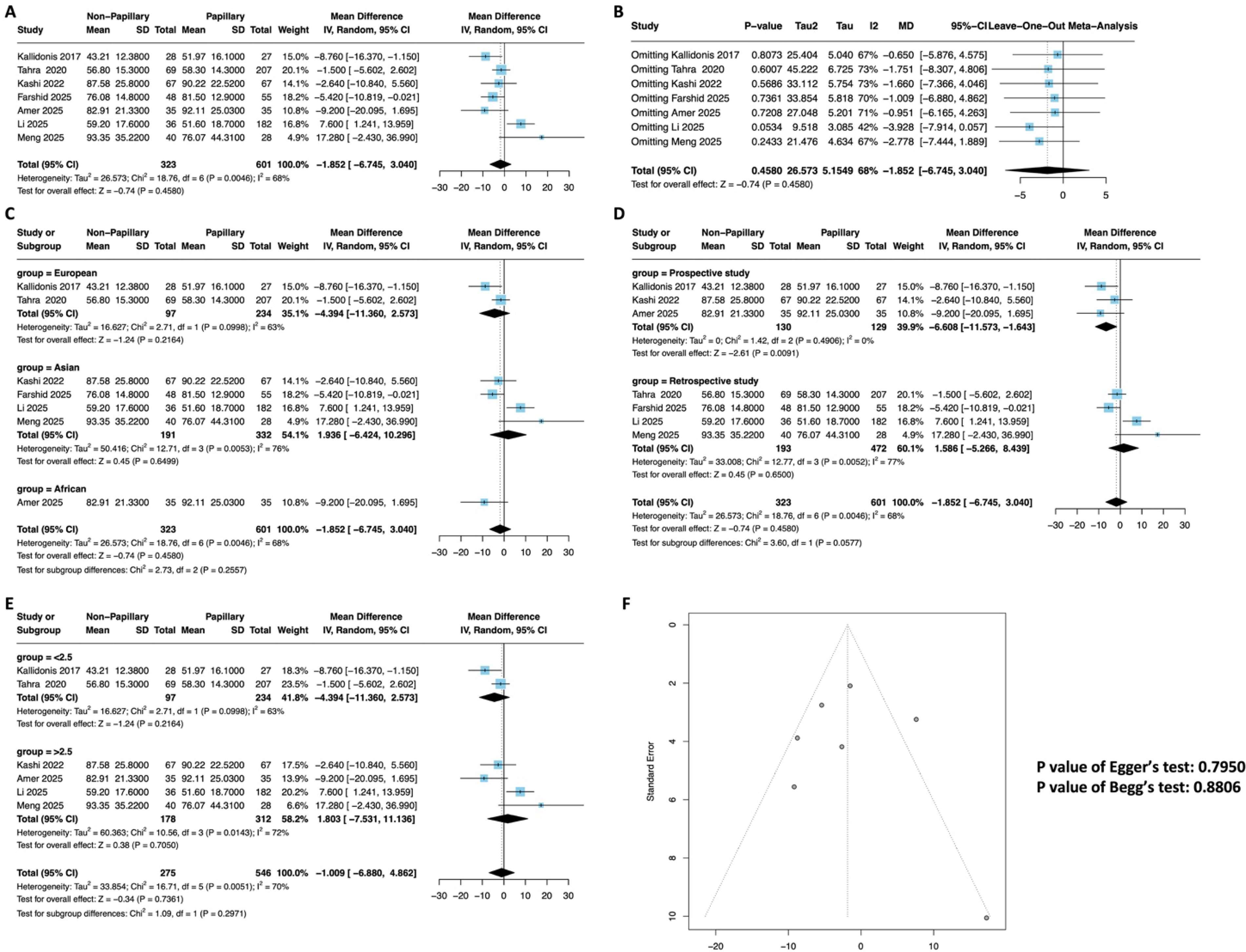
Meta-analysis of operative time between the nonpapillary and papillary access groups.
Discussion
This meta-analysis, encompassing nine studies and 1229 patients, demonstrates that nonpapillary and papillary access for PCNL is comparable in terms of postoperative hemoglobin drop, complication rates, and SFRs. Notably, although no significant overall difference in operative time was observed between the two approaches, subgroup analysis of prospective studies revealed that nonpapillary access was associated with a significantly shorter operative time. This discrepancy between the subgroup and overall results likely reflects the methodological rigor of prospective designs: prospective studies typically standardize procedural workflows (e.g., puncture localization, tract dilation) more consistently than retrospective studies, which may mask the technical efficiency of nonpapillary access. The shorter operative time in prospective nonpapillary cohorts is plausible given the approach’s inherent advantages: a larger target area (reducing puncture attempts), direct trajectory to calculi (minimizing nephroscope manipulation), and easier antegrade stent placement—all of which streamline the surgical process, particularly in the hands of experienced operators. This finding supports the clinical utility of nonpapillary access for optimizing procedural efficiency, especially in standardized, high-volume settings.
The primary outcome of postoperative hemoglobin drop showed no significant difference between groups, even after excluding the outlier study (Li et al., 2025) that accounted for high heterogeneity. Several factors may collectively contribute to this equivalent bleeding risk. First, variations in puncture localization methods across studies should be emphasized: Most European studies adopted X-ray-guided puncture, whereas Asian studies (those conducted in China) predominantly relied on ultrasound guidance. Doppler ultrasound offers a unique advantage of real-time blood flow signal detection, enabling surgeons to proactively avoid puncturing blood-rich regions intraoperatively.21–23 This technical difference may have mitigated potential bleeding disparities between the two access paths, contributing to the nonsignificant pooled result. Second, the anatomical basis of PCNL puncture further explains the comparable bleeding risk: The majority of percutaneous access is performed in the prone position, with the target region mostly located in Brödel’s avascular plane—a relatively blood-sparse area of the renal cortex. 24 Regardless of whether papillary or nonpapillary access is adopted, puncturing within this anatomical plane minimizes vascular injury, which directly aligns with our finding of no significant difference in postoperative hemoglobin drop between the two groups.
Third, it is crucial to recognize that bleeding risk in PCNL is multifactorial; the puncture path is merely one component. Other influential factors include tract dilation technique, access tract diameter, intraoperative manipulation (e.g., stone fragmentation intensity, renal pelvis irritation), and inherent individual differences in renal vascular anatomy.25–28 These confounding variables may have interacted and collectively masked potential subtle differences in bleeding risk between the two puncture approaches, further influencing the judgment of the outcome. Fourth, the ambiguity of puncture accuracy in clinical practice should be considered. In real-world clinical settings, achieving absolute papillary puncture is often challenging. Many cases presumed to be papillary puncture may have been inadvertently converted to nonpapillary access because of the absence of intraoperative CT verification to confirm the puncture site. This clinical reality has been implicitly validated in practice and may partially explain why no significant difference was observed between the two groups in our meta-analysis.
Although papillary puncture is theoretically the safest approach because of its avascular characteristics, it has inherent limitations: It is technically demanding and unfriendly to novice urologists, and exhibits disadvantages in managing multiple caliceal stones and placing ureteral stents via lower caliceal puncture. With the rapid advancement of artificial intelligence (AI) technology, the concept of papillary puncture may be gradually weakened in the near future.29,30 It is plausible that AI, combined with preoperative CT angiography for vascular and anatomical assessment, could integrate with ultrasound to achieve a truly precise fused-image-guided puncture—optimizing access safety and efficiency without being constrained by the traditional distinction between papillary and nonpapillary paths.
The absence of heterogeneity in complication and SFRs further supports the equivalence of the two techniques, confirming that neither approach confers a safety or efficacy advantage in these domains. The moderate heterogeneity observed in operative time, which was not explained by region or study design, likely reflects variations in surgeon experience, stone complexity, intraoperative decision-making, localization method-related efficiency differences, and technical proficiency in puncture approaches across studies.
For urologists, these data confirm that both access techniques are safe and effective, allowing for greater flexibility in surgical planning. Nonpapillary access can be appropriately used for peripheral or complex stones, whereas papillary access remains a reliable option for central caliceal stones. The choice of localization method (ultrasound vs X-ray) should be guided by institutional expertise, stone characteristics, and the need for real-time blood flow assessment—Doppler ultrasound may be preferred in settings where avoiding vascular-rich regions is prioritized. In addition, clinicians should acknowledge the ambiguity of puncture site confirmation in routine practice and the multifactorial nature of bleeding risk. Looking ahead, embracing AI-integrated imaging technology may revolutionize PCNL access planning, transcending traditional puncture classifications to achieve personalized, precision-guided procedures. Future research should focus on large, multicenter RCTs with standardized operative protocols (including uniform localization, dilation techniques, and intraoperative verification of puncture sites) to clarify the interactive effects of puncture path, localization method, and other procedural factors on bleeding risk. In addition, studies exploring AI-assisted fused-image-guided puncture are warranted to validate its clinical utility.
This study has limitations inherent to meta-analyses of observational data: The majority of included studies were retrospective, introducing potential selection bias. In addition, significant heterogeneity in some outcomes (e.g., postoperative hemoglobin drop) may be partially attributed to unmeasured variations in localization methods, puncture accuracy, and other procedural factors, which limits generalizability. The small number of RCTs included reduces the statistical power to detect subtle differences between groups. Individual patient data were not available, precluding adjustment for confounding variables such as stone burden, tract diameter, dilation technique, and individual renal vascular anatomy—factors that may influence bleeding risk independently of puncture path. Finally, another limitation is the inclusion of unpublished data from our team’s ongoing study. Although these data were extracted from a well-designed retrospective cohort with standardized CRFs, and sensitivity analysis excluding this dataset did not alter the primary conclusions, the absence of external peer review for this ongoing study may introduce potential bias in data interpretation. We have provided detailed data of this ongoing study in Table 1 to ensure transparency, and the full study will be submitted for publication separately to avoid data duplication.
Conclusion
Nonpapillary access should be recognized as a viable and valuable option in PCNL practice, offering comparable safety and efficacy to papillary access with potential procedural efficiency benefits. The findings of this meta-analysis provide evidence-based guidance to individualize surgical planning, ultimately improving patient care in the management of large and complex renal calculi.
Authors’ Contributions
X.M. and Y.X.: Protocol/project development. Z.S. and X.W.: Data collection or management. C.J. and X.M.: Data analysis and article writing/editing.
Footnotes
Availability of Data and Materials
All the data (pooled MD with 95% CIs, pooled OR with 95% CIs of incidence of complications) used to support the findings of this study are included within the article. Please contact the author for data requests.
Ethics Approval and Consent to Participate
This study was approved by the Ethics Committee of the First Affiliated Hospital with Nanjing Medical University (No. 2022-SR-385), and informed consent was obtained from all patients before a surgical procedure.
Acknowledgments
The authors thank the researchers and study participants for their contributions.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was funded by the Jiangsu Province Capability Improvement Project through Science, Technology, and Education (No. ZDXK202219) and the Wu Jieping Medical Foundation Clinical Research Special Fund Project (No. 320.6750.2025-25-2).
Supplemental Material
Abbreviations
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.