
Abstract
Purpose:
To characterize the etiology and clinical course of patients with subcapsular renal hematoma (SRH) in order to better understand and manage patients in the acute and chronic settings.
Materials and Methods:
A natural language processing algorithm screened computed tomography and magnetic resonance imaging studies for “subcapsular renal hematoma” across 10 inpatient facilities from 2011 to 2021. Patients with at least three cross-sectional exams were included. Retrospective chart review assessed etiology, clinical course, and management of SRH.
Results:
A total of 105 patients with acute SRH were included. The underlying etiologies involved traumatic (21%), spontaneous (32%), and iatrogenic causes (47%). Three patients developed Page kidney with hypertension secondary to renin-angiotensin-aldosterone system activation. Notably, two of these patients had solitary kidneys, with one necessitating temporary hemodialysis and the other undergoing hematoma evacuation. Additionally, six patients developed infected hematomas; five required drainage by interventional radiology (IR), and one patient underwent nephrectomy. Angiography by IR was recommended in 21 patients, 17 of whom underwent renal artery embolization. One patient developed intractable pain, requiring operative hematoma evacuation. Another patient developed abdominal compartment syndrome requiring decompressive laparotomy. Repeat imaging was done within 1–10 months in 69 patients, with 11 (16%) demonstrating complete hematoma resolution. In 16 patients who had further imaging between 10 and 15 months, an additional 8 had resolved. The average time to complete resolution was 368 days.
Conclusion:
Subcapsular hematoma is a rare finding, most commonly occurring after iatrogenic causes. In our series, roughly 1/3 (34%) of all hematomas require intervention, including hemodialysis, embolization, and nephrectomy. One third (33%) of spontaneous SRH required embolization, most commonly those with underlying renal masses. Three patients developed the Page kidney phenomenon, which was more common in patients with a solitary kidney.
Introduction
Subcapsular renal hematoma (SRH) is a rare radiographical finding, but with significant potential risks in the acute and chronic settings. On cross-sectional imaging, SRH appears as crescentic or lentiform-shaped fluid collections confined by the renal capsule. 1 Some SRH cases are found incidentally, while other cases can be associated with clinically significant anemia, pain, infection, or simultaneous acute kidney injury and hypertension, known as the Page kidney phenomenon. 2 Subcapsular hematomas can be commonly caused by iatrogenic trauma. There are various case reports describing SRH after different urologic and non-urologic procedures.3–5 Others occur spontaneously, due to suspected tumor hemorrhage, vascular malformations, or vasculitis, however, the underlying cause may never be elucidated.6,7 Although exploration was commonly used in the past for management of SRH, most patients with SRH are now managed conservatively in contemporary series. 8 Nonetheless, it is not always predictable which patients will require intervention, and it is important to exercise clinical judgement when deciding if and when intervention is needed. To that end, given the large volume of imaging performed on a daily basis at our institutions, we required an efficient means through which patients with relevant imaging findings were identified and could then be monitored for progression. Natural language processing (NLP) provides an efficient means for extracting relevant clinical findings and converting this into structured data and has been used in a variety of urological realms.9–12 Our objective was to identify the etiology and clinical course of patients with SRH on imaging over a 10-year period at multiple hospitals to better understand the natural history of SRH.
Methods
Using a software analytics platform, Nuance mPower Clinical Analytics (Nuance Communications, Inc., Burlington, MA), an NLP program, we created a Boolean search algorithm. This algorithm searched free-text radiology reports for a “subcapsular renal hematoma,” “perinephric hematoma,” and “renal hematoma.” The algorithm retrospectively screened computed tomography and magnetic resonance imaging (MRI) studies across 10 inpatient New York City metro area facilities, including Level 1 Trauma Centers, from 2011 to 2021. Images were reviewed by authors to ensure that an SRH was indeed seen. Patients aged 18 and older, with at least 3 serial cross-sectional exams, were included to track progression and time to resolution. Patients with renal allograft and those with medical records, prior to electronic charts, or incomplete medical records were excluded. Of the 175 patients initially identified by the NLP algorithm, 70 were excluded: 35 had fewer than 3 serial cross-sectional imaging studies required for longitudinal follow-up, 20 had incomplete or pre-electronic medical records, and 15 had renal allografts, yielding a final analytic cohort of 105 patients. Retrospective chart review assessed etiology of hematoma, interventions, and management of clinical sequelae.
Results
We reviewed 175 adult patients’ charts with a documented radiographical diagnosis of SRH. One-hundred-and-five patients were included in the final analysis. The average patient age was 61 years (20–94 years), with a male-to-female ratio of 1.9:1. Etiologies were traumatic in 19% (20/105), spontaneous in 33% (35/105), and iatrogenic in 48% (50/105) of patients (Table 1). Of the 20 trauma cases, 12 were due to falls, 1 due to penetrating trauma (gunshot wound), and 7 due to blunt traumas (scooter, motorcycle, car accidents, or pedestrians struck by motor vehicles). Sixty-five percent of spontaneous hematomas (23/35) did not have clear underlying causes, with less than half of patients having associated cystic (11%, 4/35) or solid (23%, 8/35) masses. Renal biopsy was the most common iatrogenic etiology (38%, 19/50), followed by nephrostomy tube placement/exchange (18%, 9/50) and percutaneous nephrolithotomy (PCNL) (14%, 7/50). Other less common urologic etiologies included extracorporeal shockwave lithotripsy (SWL) (6/50, 12%), ureteroscopy (4/50, 8%), and partial nephrectomy (1/50, 2%).
Etiology of Subcapsular Renal Hematoma
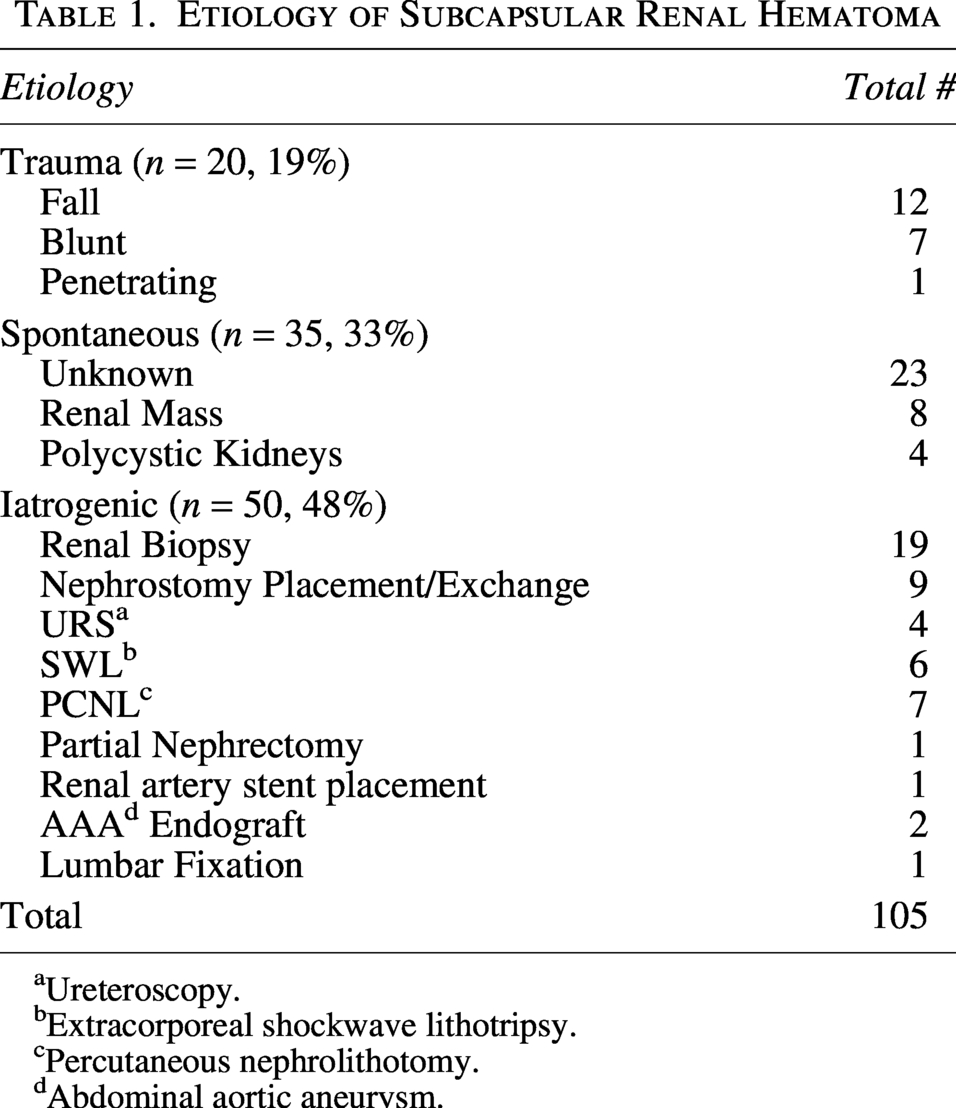
Ureteroscopy.
Extracorporeal shockwave lithotripsy.
Percutaneous nephrolithotomy.
Abdominal aortic aneurysm.
Fifty-six of the included patients had recorded dimensions of the hematoma thickness, which revealed a mean initial hematoma thickness of 8.63 centimeters (cm). Mean initial thickness values stratified by etiology were 10.24 cm for iatrogenic cases, 8.17 cm for spontaneous cases, and 5.79 cm for trauma cases. Patients who received an intervention had a significantly higher average thickness on initial imaging 9.86 cm compared to those who were managed conservatively (6.58 cm). Within each etiologic category, patients requiring intervention demonstrated greater mean thickness than those managed conservatively: 11.76 cm vs 7.96 cm for iatrogenic; 8.81 cm vs 6.68 cm for spontaneous, and 7.55 cm vs 3.68 cm for trauma.
Thirty-six patients (34%) with SRH developed complications requiring intervention (Fig. 1). Three patients developed Page kidney with hypertension secondary to renin-angiotensin aldosterone system activation. Two of these patients had solitary kidneys. Initial documented hematoma thicknesses for these patients were (1) “moderate”; (2) 10.1 × 5.5 cm; and (3) 3.4 cm. Page patient #1 was spontaneous in a solitary kidney, required intervention with temporary hemodialysis and had 8 month follow-up without resolution of hematoma. Page patient #2 was spontaneous with a 4 cm renal mass, required intervention with embolization on day 1, and only had follow-up for a week with multiple computed tomographies (CTs) and did not document resolution. Page patient #3 was spontaneous in a solitary kidney, required operative hematoma evacuation 1 day after initial diagnosis and then follow up imaging 4 days later showed resolution.
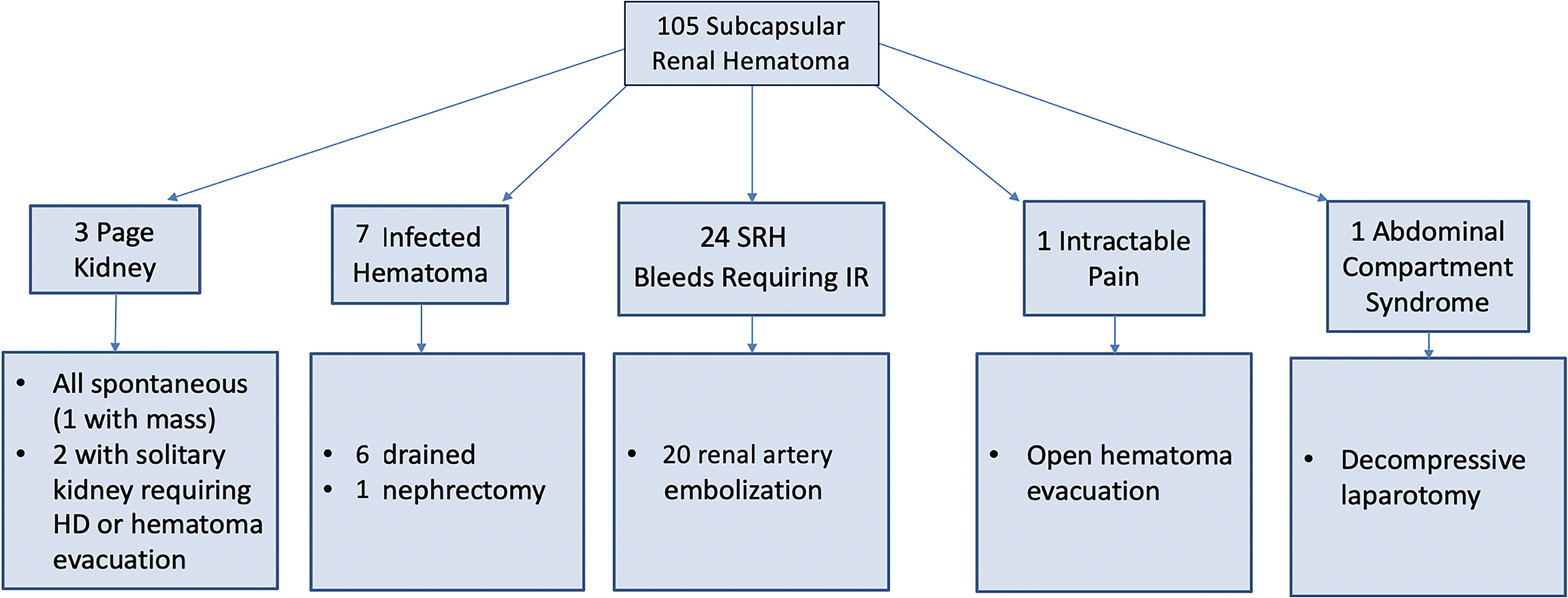
Clinical Sequela and Intervention for 105 patients with SRH. Thirty-six patients developed complications including page kidney, infected hematoma, uncontrolled bleeding, pain, and abdominal compartment syndrome.
Seven patients developed infected SRH, on average within 3 months, most of which (71%, 5/7) were iatrogenic in etiology after PCNL (n = 2), URS, nephrostomy tube placement, nephrostomy tube exchange, and two SRH from unknown spontaneous etiology. All patients with infected hematoma underwent intervention. Six required IR drainage and one required nephrectomy.
Twenty-four SRH patients were hemodynamically unstable, and their retroperitoneal hematomas required IR angiography, 20 of which identified a renal artery branch that was successfully embolized. The remainder of these patients were resuscitated and monitored carefully until their hemodynamics normalized. Given the negative renal arterial angiogram, the hematoma was suspected to be from venous bleeding. Of the 20 patients requiring renal artery embolization, the etiology was iatrogenic in 9, traumatic in 4, spontaneous and unknown in 4, and spontaneous with underlying renal mass in three.
Two SRH patients required operative intervention. One SRH patient developed intractable pain, requiring operative hematoma evacuation on day 34, while another patient developed abdominal compartment syndrome requiring decompressive laparotomy. Sixty-nine patients had repeat imaging within 1–10 months, and 11 (16%) demonstrated hematoma resolution during that time period. Sixteen patients had follow-up imaging between 10 and 15 months, in which an additional 8 had radiographically resolved. Eleven patients had resolution documented after 15 months of diagnosis, with 6 patients recording interval imaging demonstrating decreasing hematoma size. The average time to resolution was 368 days.
Discussion
For us to efficaciously identify patients with this relevant clinical finding, we sought a means to rapidly identify patients with SRHs and follow these patients’ clinical course. NLP provides a means to automatically capture clinical information from narrative radiological reports. Ambiguous radiology reports could be potentially interpreted in more than one way depending on how search algorithms are created. 13 Given that we used a Boolean search mechanism, it identified more patients than were ultimately included. That being said, medical workflows that require analysis of large datasets can be analyzed efficiently through NLP techniques. Manual annotations, structured reporting, and now even large language models provide augmented methods to improve text recognition and interpretation.12,14 Moving forward, techniques like NLP will likely become more widely used for the extraction of relevant data from a variety of clinical documentation—such as operative reports, pathology reports and even progress notes.
SRHs are a rare albeit important radiographical finding to recognize and manage appropriately. There is a paucity of literature regarding the natural history of subcapsular hematoma. In the acute setting, they appear as crescentic or lentiform-shaped fluid collections confined by the renal capsule. They typically demonstrate between 30 and 90 Hounsfield Units on CT or decreased signal on T1 and T2 on MRI. 1 Doppler ultrasound can be used to monitor renal perfusion changes caused by the parenchymal compression from the encapsulated hematoma. Significant compression of the renal vasculature can lead to resistance to flow and a variety of velocities ranging from increased peaks to loss or reversal of the diastolic waveform. 15
Prompt recognition of the SRH, in addition to identifying the cause of the bleed, can significantly impact the prediction of outcomes. In our series, the most common etiology of SRH was iatrogenic (48%, 50/105), specifically secondary to renal biopsy (38%, 19/50). A prospective study of 471 patients by Manno et al., reported a 33% rate of post-biopsy SRH in native kidneys; however, 90% of these hematomas were clinically silent. 16 In our study, 58% of post-biopsy hematomas required intervention, ranging from multiple transfusions to renal artery embolization. While several case reports have described Page kidney after transplant biopsies, the incidence of patients with post-biopsy subcapsular hematomas progressing to develop Page kidney is not clear.17–19 Wanic-Kossowska et al. reported 3 cases (0.3%) of Page kidney in 800 renal biopsies performed over 10 years. 20 In our study, none of the post-biopsy SRH cases developed Page kidney.
Iatrogenic renal subcapsular hematoma has been described following PCNL and SWL.4,21 In our study, PCNL (7/50) and SWL (6/50) were the most common iatrogenic surgical causes of SRH. Additionally, placement or exchange of a nephrostomy tube had a similar rate of occurrence (9/50). SRH after ureteroscopic lithotripsy (URSL) was first mentioned in the literature in 2010, with relatively few cases reported since.22,23 Our study reports four SRH in the setting of URSL, of which two patients had baseline end-stage renal disease (ESRD) on dialysis, three patients required packed red blood cell transfusion, and 1 required IR drainage of hematoma. A systematic review by Whitehurst et al. of 9000 patients who underwent URSL found the incidence of SRH to be 0.45%. It has been postulated that SRH are more likely to form after URS in the setting of hydronephrosis leading to deformed vasculature and loss of parenchymal elasticity, which may also be the case for patients with ESRD. In addition, trauma from the guidewire and prolonged high-pressure flow in the pelvicaliceal system may contribute to the risk of SRH. 3
After iatrogenic etiologies, spontaneous bleeds resulting in SRH were the next most common cause, occurring in about one-third of the hematoma cases, unrelated to trauma or iatrogenic etiology. Of the 35 spontaneous SRH, 8 were related to renal masses and 4 to polycystic kidneys. The acute onset of spontaneous, nontraumatic renal hemorrhage into the subcapsular and perirenal spaces has been described as Wunderlich syndrome. It is traditionally clinically characterized by Lenk’s triad: acute flank pain, flank mass, and hypovolemic shock. 24 More than half of spontaneous SRH patients in our study were asymptomatic and were only noted radiographically.
Initial hematoma imaging suggests that hematoma thickness is an important clinical indicator for the subsequent need for intervention. The consistent association between larger hematoma dimensions and interventional requirements across all etiologic groups indicates that thickness at presentation is a robust prognostic marker. Incorporating standardized thickness measurements into initial clinical assessments may improve risk stratification and facilitate earlier identification of patients who are unlikely to be successfully managed with conservative measures alone.
Classically, there has been concern that renal hemorrhage into the subcapsular space may be associated with hemodynamic changes. The historically described features of Page kidney include new-onset hypertension in patients who are normotensive previously, with or without renal impairment. First described in 1939 by Dr. Irving Page, “cellophane perinephritis,” as it was called after his experiments wrapping canine kidneys in cellophane, demonstrated the compression of renal parenchyma led to increased blood pressure. 2 In 1955, Page and Engel then reported a young football player with hypertension that resolved after unilateral nephrectomy of a subcapsular hematoma. 25 The Page kidney phenomenon is now understood to be related to microvascular ischemia from parenchymal compression, which activates the renin-angiotensin-aldosterone system, resulting in hypertension. 26 Despite its well-documented description, we did not note a significant relationship between SRH and the development of Page kidney.
Three patients in our study developed Page kidney, two of whom had solitary kidneys. One solitary Page kidney developed renal failure, requiring temporary hemodialysis. The second solitary Page kidney patient required operative evacuation of the hematoma. The third Page kidney was secondary to a renal mass that underwent IR angioembolization of a bleeding vessel, had a contralateral functional kidney, and was managed conservatively. Significant renal impairment in Page kidney has been described in patients with single functioning kidneys, as exemplified by lone renal allografts. 27 Renal insufficiency is not usually seen with unilateral SRH in the setting of a contralateral functioning kidney since the normal perfusion of the contralateral kidney maintains normal renal function. 28 Therefore, closer follow-up may be recommended for patients with SRH in the setting of solitary kidneys.
There is currently no evidence-based guideline for the management of subcapsular renal hematoma. Early recognition is key, especially in the setting of a solitary or allograft kidney, to prevent progressive ischemic organ damage. While protocols vary, we suggest that multiphase CT best evaluates for active extravasation and/or hypoperfusion/compression of the renal parenchyma. Initial conservative management should include antihypertensive medication with angiotensin converting enzyme inhibitors and fluid restrictions. 29 Indications for intervention as seen in our study include severe anemia and hemodynamic instability, intolerable pain, infected hematoma intractable to antibiotic therapy and Page kidney.
The natural history of the SRH timeline to resolution has not been elucidated in the current literature. In our study, 69 of 105 patients had repeat imaging within 1–10 months, and 11 (16%) demonstrated hematoma resolution. Of these 69 patients with imaging, 16 patients had additional imaging between 10 and 15 months, of which an additional 8 had resolved. The average time to complete resolution of the hematoma was 368 days.
Our study has several important limitations. First, as this was a retrospective study relying on radiological report reads, we were unable to collect standardized clinical data—including patient age, sex, BMI, baseline comorbidities, or anticoagulant use—which are important covariates that may influence hematoma formation, progression, and outcomes. Future prospective studies should incorporate structured data collection at the time of SRH diagnosis to capture these variables. Second, because the study was conducted off radiological reads without structured clinical documentation, we were unable to determine whether hematomas were detected acutely or incidentally—a distinction with important prognostic implications. Third, our study cannot comment on the rate of hematoma growth, as imaging intervals were not standardized. Fourth, of the 175 patients initially identified, 70 were excluded due to insufficient serial imaging or incomplete records, and patients may have undergone imaging at non-affiliated centers, contributing to potential undercounting and miscalculation of time to resolution. We do not have long-term follow-up data for delayed complications such as chronic hypertension. Based on our findings, we recommend that patients with SRH expect imaging follow-up for 1.5–2 years until radiographical resolution is confirmed.
Conclusion
Subcapsular hematoma is a rare finding with only 105 identified in 10 years of a multi-hospital database. Thirty-five percent of patients required intervention, including hemodialysis, embolization and nephrectomy. The most common iatrogenic cause was renal biopsy. One-third of spontaneous SRH required embolization, most commonly those with underlying renal masses. Page kidney phenomenon is rare (3%), but possibly more likely in solitary kidney.
Authors’ Contributions
E.L.: Data curation and investigation (lead); formal analysis, writing—original draft (lead)—review and editing (lead). S.R.: Validation (supporting), writing—review and editing (supporting). W.A.: Supervision (supporting), writing—review and editing (supporting). R.K.: Writing—review and editing (supporting). A.R.: Investigation (supporting). Justin James: Investigation (supporting). K.G.: Writing—review and editing (supporting). M.G.: Writing—review and editing (supporting). Z.O.: Writing—review and editing (supporting). D.H.: Writing—review and editing (supporting). J.W.: Writing—review and editing (supporting). A.S.: Writing—review and editing (supporting). A.R.: Conceptualization (lead); supervision (lead); validation (lead); writing—review and editing (supporting).
Footnotes
Acknowledgment
This research is a product of the New York Endourology Advanced Research Collaborative (EndoARC), which consists of endourologists from a variety of New York City metro area institutions including Northwell Health and Mount Sinai Hospital. We would like to thank all of our members for the time and dedication to this research effort.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was utilized or needed to sponsor this research effort.