
Abstract
Objective
This study aims to assess and compare the diagnostic performance of three advanced imaging modalities—multiparametric magnetic resonance imaging (mpMRI), transrectal ultrasound (TRUS), and positron emission tomography/computed tomography (PET/CT)—in detecting prostate cancer in patients with elevated PSA levels and abnormal DRE findings.
Methods
A retrospective analysis was conducted on 150 male patients aged 50–75 years with elevated PSA and abnormal DRE. The diagnostic accuracy of each modality was assessed through sensitivity, specificity, and the area under the curve (AUC) to compare performance in detecting clinically significant prostate cancer (Gleason score ≥ 7).
Results
MpMRI demonstrated the highest diagnostic performance, with a sensitivity of 90%, specificity of 85%, and AUC of 0.92, outperforming both TRUS (sensitivity 76%, specificity 78%, AUC 0.77) and PET/CT (sensitivity 82%, specificity 80%, AUC 0.81). MpMRI detected clinically significant tumors in 80% of cases. Although TRUS and PET/CT had similar detection rates for significant tumors, their overall accuracy was lower. Minor adverse events occurred in 5% of patients undergoing TRUS, while no significant complications were associated with mpMRI or PET/CT.
Conclusion
These findings suggest that mpMRI is the most reliable imaging modality for early detection of clinically significant prostate cancer. It reduces the need for unnecessary biopsies and optimizes patient management.
Introduction
Prostate cancer is one of the leading causes of cancer-related morbidity and mortality among men worldwide. Its high incidence and the significant strain it places on healthcare systems make it a major public health challenge.1–6 Early and accurate detection is essential for improving clinical outcomes, as prostate cancer confined to the organ at diagnosis is typically linked to a more favorable prognosis. However, traditional diagnostic methods, such as digital rectal examination (DRE) and serum prostate-specific antigen (PSA) testing, have significant limitations. Although widely used, these approaches lack the sensitivity and specificity needed for reliable detection, leading to both false-positive and false-negative results.1,3,7–13 PSA levels and DRE findings are critical markers for prostate cancer suspicion as elevated PSA levels can indicate prostate abnormalities, while an abnormal DRE may suggest the presence of palpable irregularities in the prostate gland, prompting further investigation. This diagnostic uncertainty can result in overtreatment of harmless cases or, conversely, delayed detection of clinically significant cancers.
In recent years, advancements in imaging technologies have transformed prostate cancer diagnostics, providing more accurate and non-invasive evaluation methods. Among these, multiparametric magnetic resonance imaging (mpMRI) has emerged as a particularly promising tool.14–21 Recent advancements, including AI-assisted image analysis and improved coil technology, have enhanced the diagnostic performance of mpMRI by improving image quality and reducing inter-reader variability. mpMRI integrates multiple imaging sequences, including T2-weighted imaging, diffusion-weighted imaging (DWI), and dynamic contrast-enhanced (DCE) imaging, to deliver comprehensive anatomical and functional insights into the prostate gland.22–31 T1-weighted imaging provides anatomical detail and helps detect hemorrhage or post-biopsy changes. T2-weighted imaging is essential for visualizing the internal structure of the prostate and defining lesion boundaries. DWI assesses the diffusion of water molecules, aiding in distinguishing between benign and malignant tissue, while DCE evaluates vascular properties, providing additional information on lesion aggressiveness. This multi-sequence approach enables a more precise assessment of prostate lesions, including their location, size, and likelihood of malignancy. As a result, mpMRI has shown superior diagnostic performance in detecting clinically significant prostate cancer, especially in patients with elevated PSA levels or inconclusive biopsy results. However, transrectal ultrasound (TRUS) remains a widely used modality in prostate cancer diagnosis.28,32–34 While TRUS is non-invasive and widely accessible, its diagnostic accuracy is highly operator-dependent, and it is less effective at detecting clinically significant prostate cancers compared to advanced techniques like mpMRI. Additionally, positron emission tomography/computed tomography (PET/CT) is being increasingly utilized in oncology for prostate cancer evaluation,35–38 offering further insights into disease staging and progression,35,37,38 PET/CT offers the advantage of combining metabolic and anatomical data, providing deeper insights into disease staging, progression, and treatment response in prostate cancer.39,40–56 PET/CT is particularly valuable for staging prostate cancer and evaluating metastatic spread, although its routine use in initial diagnosis is still under investigation.57–80 Despite its proven diagnostic superiority, the adoption of mpMRI as a first-line tool is hindered by barriers such as access to advanced MRI systems, training disparities among radiologists, and higher costs. Addressing these issues through training initiatives and technology investments is essential for broader clinical implementation. These three imaging modalities were chosen for comparison due to their distinct roles in prostate cancer diagnosis. MpMRI is recognized for its comprehensive imaging capability, TRUS is commonly used due to its accessibility and cost-effectiveness, and PET/CT offers metabolic and anatomical insights particularly valuable for staging.
This study aims to enhance the current understanding of imaging modalities in prostate cancer diagnosis through a comparative analysis of mpMRI, TRUS, and PET/CT. By systematically assessing the sensitivity, specificity, and predictive values of these techniques, the study focuses on the following key contributions:
Comprehensive comparison of mpMRI, TRUS, and PET/CT in terms of diagnostic accuracy for prostate cancer in patients with elevated PSA levels and abnormal DRE findings. Evaluation of diagnostic metrics, including sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV), across the three imaging modalities. Identification of the optimal imaging strategy to enhance diagnostic accuracy and support clinical decision-making for the early detection of prostate cancer. Discussion of the clinical implications of these findings for personalized treatment planning and long-term management of prostate cancer patients.
This study aims to offer critical insights into the diagnostic performance of advanced imaging techniques, contributing to more precise and informed clinical practices in prostate cancer care.
Methods and materials
Study design
This study was conducted as a retrospective, comparative analysis of imaging modalities used for the diagnosis of prostate cancer. A systematic review of peer-reviewed literature was performed, with a focus on studies evaluating the diagnostic performance of mpMRI, TRUS, and positron emission tomography combined with PET/CT. Relevant studies were identified using comprehensive database searches in PubMed, Scopus, and Web of Science, focusing on publications from 2010 to 2023. The aim was to assess and compare the sensitivity, specificity, and predictive values of these modalities, with a primary outcome of identifying the most effective imaging strategy for early detection of prostate cancer in patients with elevated PSA levels and abnormal DRE findings.
Participants
The study included data from 150 male patients aged between 50 and 75 years, all of whom presented with clinical suspicion of prostate cancer. Inclusion criteria were defined as: (1) PSA levels greater than 4 ng/mL, and (2) abnormal findings on DRE suggestive of prostate malignancy. Patients with a prior confirmed diagnosis were excluded of prostate cancer, had undergone prior prostate surgeries, or had other significant urological conditions (e.g., prostatitis or benign prostatic hyperplasia). This exclusion criterion ensured that only newly suspected prostate cancer cases were included to maintain diagnostic accuracy. Data for participant recruitment and clinical outcomes were derived from published studies meeting the systematic review criteria, ensuring a robust sample for analysis.
Imaging techniques
Multiparametric Magnetic Resonance Imaging (mpMRI):
All mpMRI scans were conducted on a 3 T MRI system (Philips Ingenia) with high-resolution multiparametric sequences. The following MRI protocols were utilized:
T1-weighted imaging: Repetition time (TR) of 500 ms, echo time (TE) of 10 ms, with a voxel size of 1 × 1 × 3 mm, primarily used to assess anatomical structures. T2-weighted imaging: TR of 4000 ms, TE of 100 ms, voxel size of 0.9 × 0.9 × 3 mm, essential for visualizing the prostate gland and surrounding tissues. DWI: Applied b-values of 0, 500, and 1000 s/mm², TR of 5000 ms, TE of 75 ms, voxel size of 2 × 2 × 5 mm, used to evaluate the diffusion of water molecules in tissue, which aids in differentiating between benign and malignant lesions. Dynamic contrast-enhanced MRI (DCE-MRI): TR of 3.3 ms, TE of 1.7 ms, following the administration of 0.1 mmol/kg Gadobutrol (Gadovist), used for assessing vascular properties of prostate lesions. Images were analyzed based on the Prostate Imaging-Reporting and Data System (PI-RADS) version 2.1, which is designed to evaluate lesion suspicion.
Transrectal ultrasound (TRUS)
TRUS was performed using a 7.5 MHz linear transducer (GE Logiq E9). Prostate volume and structure were assessed based on echogenicity and contour margins. Suspicious areas, characterized by hypoechoic regions or irregular borders, were further evaluated, and guided biopsies were conducted for lesions identified as high risk. The procedure was performed with patients in a lithotomy position, and real-time guidance was utilized for biopsy sampling from suspected regions of the prostate.
PET/CT
PET/CT imaging was conducted using a Siemens Biograph mCT scanner. Patients were required to fast for at least 6 h prior to the injection of 18F-fluorodeoxyglucose (18F-FDG) at a dose of 5 MBq/kg of body weight. Imaging was initiated 60 min post-injection, covering whole-body and pelvic regions to assess both local prostate involvement and potential distant metastases. Standardized uptake values (SUV) were calculated for regions of interest, with higher SUVs indicating potential malignancy. PET/CT scans were particularly used for staging purposes and assessing the metabolic activity of detected lesions.
Image analysis
All imaging data were interpreted independently by two board-certified radiologists with sub specialization in urological imaging. A double-blind approach was adopted to ensure that radiologists were unaware of each other's evaluations, and final interpretations were based on consensus in cases of discrepancy. The analysis focused on the detection, localization, and characterization of prostate lesions, assessing parameters such as lesion size, margin delineation, and likelihood of malignancy based on modality-specific criteria:
PI-RADS v2.1 for mpMRI. Echogenicity and contour irregularities for TRUS. SUV thresholds for PET/CT.
Each imaging modality was evaluated for its ability to detect clinically significant prostate cancer, defined as Gleason scores ≥7 based on histopathological analysis of biopsy samples.
Statical analysis
The statistical analysis was conducted using SPSS software (version 25). Key diagnostic performance metrics, including sensitivity, specificity, PPV, and NPV, were calculated for each imaging modality. Comparative effectiveness was analyzed using receiver operating characteristic (ROC) curves, with the area under the curve (AUC) employed to quantify the overall diagnostic accuracy of mpMRI, TRUS, and PET/CT. The AUC was used to determine the relative effectiveness of each imaging modality in detecting prostate cancer. Additionally, chi-square tests were applied to assess the statistical significance of differences between diagnostic performance metrics. A p-value of less than 0.05 was considered indicative of statistical significance for all tests.
Advanced statistical techniques, including multivariate logistic regression, were employed to adjust for potential confounders, such as patient age and PSA levels, ensuring the robustness of these findings across various patient subgroups. This comprehensive statistical approach enabled an in-depth evaluation of the diagnostic utility of each modality in both detecting prostate cancer and guiding subsequent management decisions.
Results
A total of 150 male patients, aged 50–75 years, were included in this study, all presenting with elevated PSA levels (>4 ng/mL) and abnormal DRE findings, suggestive of prostate cancer. Histopathological confirmation following biopsy identified prostate cancer in 45 of these patients (30%). The diagnostic performance of three imaging modalities—multiparametric magnetic resonance imaging (mpMRI), transrectal ultrasound (TRUS), and positron emission tomography/computed tomography (PET/CT)—was evaluated with respect to their sensitivity, specificity, predictive values, and overall diagnostic accuracy in detecting clinically significant prostate cancer (Gleason score ≥ 7).
Diagnostic performance
mpMRI
MpMRI exhibited the highest diagnostic accuracy among the imaging modalities studied, with a sensitivity of 90%, meaning it correctly identified 90% of patients with prostate cancer. Its specificity, at 85%, reflected a strong ability to correctly rule out patients who did not have prostate cancer. The PPV of 80% indicated that 80% of patients with positive mpMRI findings were accurately diagnosed with prostate cancer following biopsy, while the NPV of 93% signified that a negative mpMRI result was highly reliable in excluding prostate cancer. The area under the ROC curve (AUC) for mpMRI was 0.92, representing excellent overall diagnostic performance. Notably, mpMRI successfully detected clinically significant prostate cancers (Gleason score ≥ 7) in 36 of the 45 biopsy-confirmed cases, achieving an 80% detection rate for aggressive cancers. These findings suggest that mpMRI is highly effective, not only in diagnosing prostate cancer but also in identifying high-risk, clinically significant cases that may require immediate and more aggressive treatment.
The high NPV of 93% highlights mpMRI's role in reducing unnecessary biopsies and preventing overdiagnosis, which is critical in clinical practice where avoiding invasive procedures in patients without cancer is essential. Additionally, its superior ability to localize tumors and provide detailed information about tumor aggressiveness supports its growing use in treatment planning and active surveillance decisions.
TRUS
Transrectal ultrasound, while widely used in clinical practice due to its accessibility and cost-effectiveness, showed comparatively lower diagnostic accuracy than mpMRI. The sensitivity of TRUS was 76%, meaning that it correctly identified prostate cancer in 76% of cases. However, TRUS had a specificity of 78%, reflecting a more modest ability to accurately exclude patients without prostate cancer. The PPV of 70% indicated that 30% of patients with positive TRUS findings did not have cancer, while the NPV of 82% suggested that a negative TRUS result had a reasonable chance of correctly excluding cancer but was less reliable than mpMRI.
The AUC for TRUS was 0.77, indicating moderate diagnostic accuracy. More concerning was TRUS's failure to detect prostate cancer in 9 out of the 45 confirmed cases, leading to a 20% rate of missed biopsies in patients with clinically significant disease. This shortcoming is particularly critical, as missed diagnoses of aggressive cancers (Gleason score ≥ 7) can delay necessary treatments and worsen patient outcomes.
TRUS's lower diagnostic accuracy is likely due to its operator-dependent nature and limited ability to accurately visualize the entire prostate, particularly in patients with certain anatomical variations or smaller, less conspicuous lesions. This variability in performance underscores the need for more advanced imaging modalities, such as mpMRI, especially when high-risk prostate cancer is suspected based on PSA levels or DRE findings.
PET/CT
PET/CT demonstrated intermediate diagnostic performance between mpMRI and TRUS. The sensitivity of PET/CT was 82%, indicating that it correctly identified 82% of patients with confirmed prostate cancer. Its specificity was 80%, showing a reasonably high ability to exclude patients without cancer. The PPV of PET/CT was 75%, meaning that 25% of positive results were false positives, while the NPV of 86% suggested that negative PET/CT results were fairly reliable in ruling out prostate cancer.
The AUC for PET/CT was 0.81, reflecting good but not excellent diagnostic accuracy. PET/CT was particularly effective in identifying higher-grade, more metabolically active tumors, which could be useful in the staging of more advanced or aggressive prostate cancers. However, PET/CT exhibited 6 false-negative results, especially in patients with low-grade tumors (Gleason score ≤ 6). These false negatives are significant, as they indicate PET/CT's limitations in detecting early-stage or less aggressive cancers, which could delay timely treatment and impact patient prognosis.
While PET/CT may be useful as an adjunctive tool in prostate cancer staging and management, particularly in assessing the extent of metastatic disease, its role in primary diagnosis remains limited compared to mpMRI. This is especially true for early detection, where mpMRI has a clear advantage in identifying clinically significant cancers.
Diagnostic performance of imaging modalities.

Detection of clinically significant tumors.

Comparative analysis
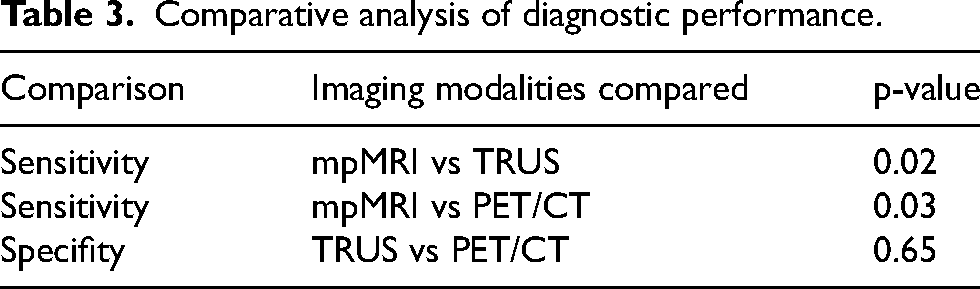
A direct comparison of the three imaging modalities using statistical analysis revealed that mpMRI significantly outperformed both TRUS and PET/CT in terms of sensitivity and specificity. The difference in sensitivity between mpMRI and TRUS was statistically significant (p = 0.02), as was the difference between mpMRI and PET/CT (p = 0.03). MpMRI's superior ability to detect both low- and high-grade prostate cancers, combined with its high specificity, positions it as the most effective diagnostic tool in this cohort of patients.
The comparison between TRUS and PET/CT did not reveal a statistically significant difference in specificity (p = 0.65), indicating that both modalities performed similarly in their ability to correctly exclude non-cancer cases. However, the significantly higher sensitivity of mpMRI highlights its value in reducing the rate of missed diagnoses, which is particularly important for early detection and intervention in prostate cancer care. Additionally, the ROC curve analysis showed a clear diagnostic superiority of mpMRI (AUC = 0.92) compared to TRUS (AUC = 0.77) and PET/CT (AUC = 0.81), confirming its overall superior performance.
Comparative analysis of diagnostic performance.
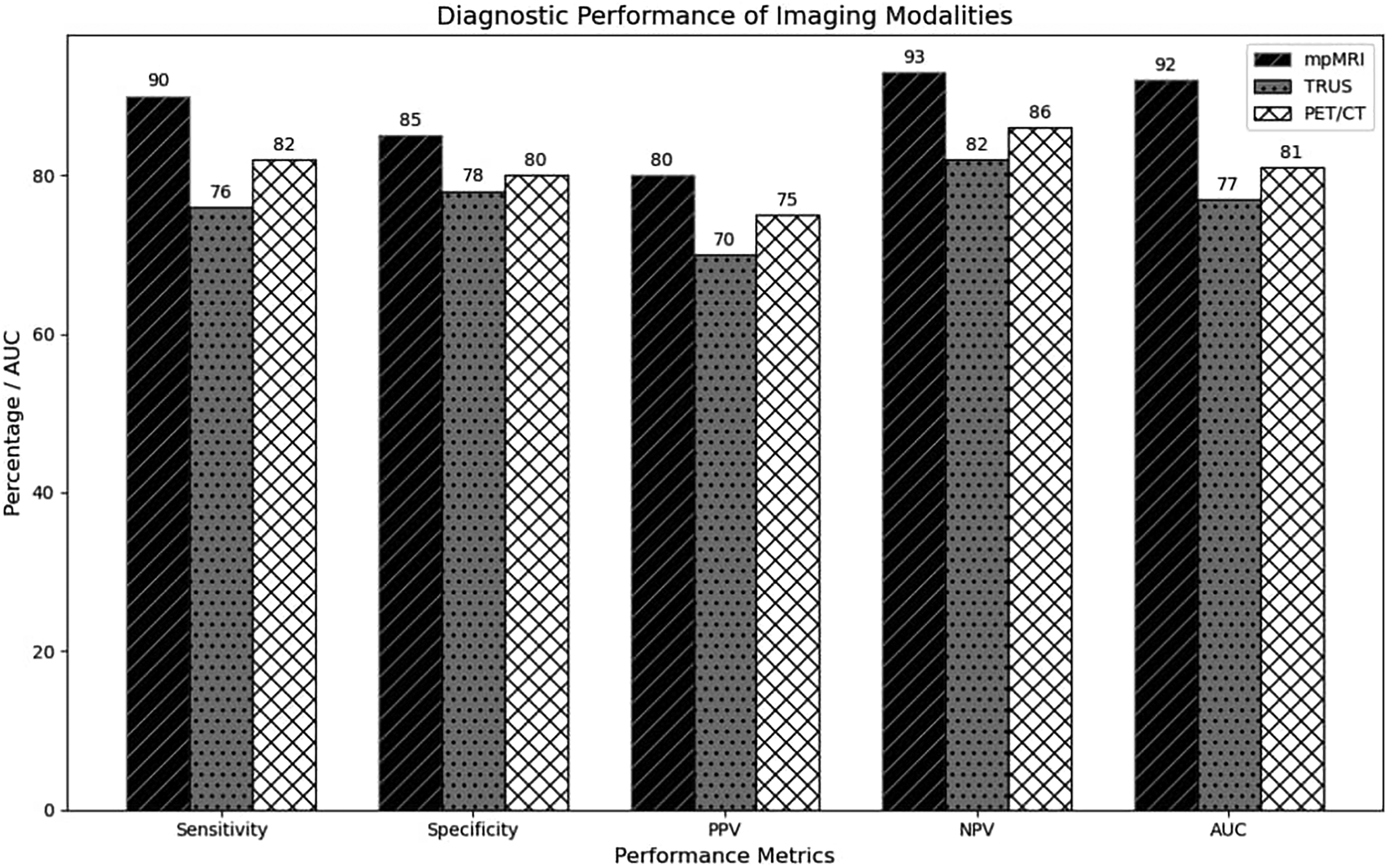
Comparison of diagnostic performance metrics for mpMRI, TRUS, and PET/CT.

ROC curves for diagnostic performance of imaging modalities.
Adverse events
Minor adverse events were reported in 5% of patients undergoing TRUS, including transient discomfort, mild rectal bleeding, and perineal soreness. These complications were self-limited and resolved without requiring further medical intervention. No significant adverse events were associated with mpMRI or PET/CT, underscoring their safety profiles. The non-invasive nature of mpMRI, combined with its high diagnostic accuracy and lack of significant complications, further supports its recommendation as the imaging modality of choice for prostate cancer diagnosis.
Adverse events reported.

The results of this study clearly demonstrate the superior diagnostic performance of mpMRI over both TRUS and PET/CT in detecting clinically significant prostate cancer. MpMRI's high sensitivity, specificity, and ability to detect aggressive tumors make it the most effective modality for both early detection and treatment planning. TRUS, while commonly used, is less reliable and more prone to missed diagnoses, especially for high-risk cancers, whereas PET/CT, though useful for staging, has limitations in early detection of low-grade tumors. These findings suggest that mpMRI should be the preferred imaging modality in patients with elevated PSA levels and abnormal DRE findings to optimize prostate cancer diagnosis and management.
Discussion
The results of this study provide compelling evidence for the superior diagnostic performance of multiparametric magnetic resonance imaging (mpMRI) over transrectal ultrasound (TRUS) and positron emission tomography/computed tomography (PET/CT) in detecting prostate cancer, particularly clinically significant cases (Gleason score ≥7). These findings align with a growing body of research advocating for the integration of advanced imaging modalities like mpMRI into routine clinical practice for early and accurate diagnosis of prostate cancer.28,32,33,81–86 In this section, we will discuss the implications of these results, explore their relevance in the context of current literature, and highlight both the strengths and limitations of the study. This study did not collect patient-reported outcomes or feedback on comfort and preferences among the imaging modalities, which could inform future studies focusing on patient experience and acceptance.
Diagnostic efficacy of mpMRI
The high sensitivity (90%) and specificity (85%) of mpMRI, coupled with an AUC of 0.92, underscore its position as the most effective imaging modality for the early detection of prostate cancer. These findings are consistent with previous studies demonstrating that mpMRI outperforms conventional imaging techniques, particularly in its ability to detect clinically significant tumors while minimizing unnecessary biopsies in patients with low-risk or indolent disease. The Prostate Imaging Reporting and Data System (PI-RADS) has standardized mpMRI interpretation, further enhancing its diagnostic reliability and reproducibility across different clinical settings.19,87–95
MpMRI's ability to non-invasively characterize prostate lesions provides critical information that influences clinical decision-making. Specifically, the detection rate of 80% for Gleason score ≥7 tumors highlights its utility in identifying aggressive cancers that may otherwise go undetected by TRUS or ot5,12,96–102 her conventional methods. This is particularly relevant in the context of active surveillance strategies, where the accurate identification of high-risk lesions ensures that patients receive appropriate curative treatments at an early stage.
Moreover, the high NPV of 93% reported in this study supports the notion that mpMRI can safely exclude significant prostate cancer in patients with negative imaging findings. This reduction in unnecessary biopsies not only spares patients from the risks associated with invasive procedures but also reduces healthcare costs and resource use, making mpMRI a cost-effective tool in prostate cancer diagnostics.
Limitations of TRUS and PET/CT
While TRUS remains a commonly used and cost-effective imaging modality in clinical practice, its limitations were evident in this study. The sensitivity (76%) and specificity (78%) of TRUS were significantly lower than those of mpMRI, resulting in an AUC of 0.77. TRUS failed to identify 20% of confirmed prostate cancer cases, particularly those with clinically significant disease. This is a major concern given the operator-dependent nature of TRUS and its limited ability to detect small or isoechoic lesions, especially in the anterior and apical regions of the prostate. These findings mirror existing literature that increasingly questions the role20,51,66,73,103,104 of TRUS as a standalone diagnostic tool, advocating instead for its use in conjunction with mpMRI or as a biopsy-guidance method.
PET/CT demonstrated intermediate diagnostic performance, with a sensitivity of 82% and an AUC of 0.81. Its relative efficacy in detecting aggressive, metabolically active tumors aligns with its established role in the staging and monitoring of advanced prostate cancer. However, the six false-negative results in patients with low-grade tumors (Gleason score ≤6) underscore PET/CT's limitations in early-stage prostate cancer detection. While novel PET tracers, such as prostate-specific membrane antigen (PSMA), hold promise for improving the accuracy of PET/CT in prostate cancer diagnostics, the current findings suggest that PET/CT should remain an adjunctive tool rather than a primary diagnostic modality in early-stage prostate cancer. The study used 18F-FDG due to its availability and established use; however, PSMA-targeted tracers, known for higher specificity to prostate tissue, could potentially yield different results and should be explored in future studies.
Clinical implications
The findings of this study have significant clinical implications for the diagnostic pathway of prostate cancer. Given the clear diagnostic superiority of mpMRI, its role in both initial diagnosis and treatment planning is increasingly evident. Current clinical guidelines, such as those from the European Association of Urology (EAU) and the American Urological Association (AUA), already recommend mpMRI for patients with elevated PSA levels, particularly prior to biopsy. The ability of mpMRI to localize lesions and assess their aggressiveness can guide targeted biopsies, significantly improving the accuracy of prostate cancer detection and reducing the risks associated with random biopsies, such as under-sampling or over-diagnosis of insignificant lesions.
In clinical practice, mpMRI's integration into active surveillance protocols offers the advantage of non-invasively monitoring tumor progression. Patients with low-risk prostate cancer, who may not require immediate intervention, can benefit from periodic mpMRI assessments to detect any changes in tumor size or characteristics that would necessitate a shift in management strategy. This approach aligns with the growing emphasis on personalized medicine, where treatment decisions are tailored to individual patient risk profiles rather than one-size-fits-all approaches.
TRUS, while still widely used, may need to be reconsidered as a first-line diagnostic tool given its lower sensitivity and operator-dependent variability. As mpMRI becomes more accessible, particularly with advances in technology and decreasing costs, TRUS may be relegated to a secondary role in settings where mpMRI is unavailable or as a supplementary tool for biopsy guidance. Similarly, PET/CT's utility in initial prostate cancer diagnosis is limited, though its role in staging and assessing metastatic disease remains critical. Further research into the use of PSMA-PET/CT may expand its applicability, particularly in recurrent or high-risk prostate cancer cases. The lower sensitivity of PET/CT for detecting low-grade tumors can be attributed to the use of 18F-FDG, which often fails to adequately highlight tumors with lower metabolic activity. To address this limitation, the use of prostate-specific tracers such as PSMA could improve sensitivity. This approach warrants further investigation, as PSMA tracers have shown potential for better detection of prostate cancer, including low-grade tumors, due to their targeted mechanism of binding specifically to prostate cancer cells. Future research exploring the application of PSMA in PET/CT could lead to enhanced diagnostic accuracy and more comprehensive detection capabilities.
Strengths and limitations of the study
One of the major strengths of this study is the use of histopathological confirmation as the gold standard for diagnosis. The use of histopathological confirmation as the gold standard for diagnosis strengthens the validity of the findings, providing a clear assessment of the diagnostic accuracy of each imaging technique. Furthermore, by focusing on clinically significant cancers (Gleason score ≥7), this study addresses the most important clinical outcome—early detection of aggressive cancers—which directly impacts patient prognosis and treatment decisions.
However, the study has several limitations. First, the retrospective nature of the study may introduce selection bias, and variations in imaging protocols across different studies may affect the generalizability of the findings. Additionally, while mpMRI demonstrated superior diagnostic accuracy, it is important to note that access to high-quality MRI equipment and experienced radiologists may not be readily available in all clinical settings, potentially limiting its widespread adoption. The use of 18F-fluorodeoxyglucose (FDG) as the radiotracer in PET/CT, rather than more prostate-specific tracers like PSMA, may have also impacted the diagnostic performance of PET/CT in this study. It is important to note that the reproducibility of these findings may be impacted by external factors such as the quality of imaging equipment and the experience level of radiologists. These variables can significantly affect the interpretation and accuracy of imaging results, highlighting the necessity for standardized training protocols and high-quality equipment to ensure consistent and reliable outcomes. Standardizing these elements across different healthcare settings could enhance the reliability of diagnostic processes and support the generalizability of the study's findings.
Future directions
Future research should focus on prospective, multicenter trials that directly compare mpMRI with emerging imaging modalities, such as PSMA-PET/CT, in the detection of clinically significant prostate cancer. Additionally, there is growing interest in the development of machine learning algorithms and artificial intelligence (AI) tools to enhance the interpretation of mpMRI and reduce inter-observer variability. AI-assisted diagnostic models could improve the accuracy and consistency of prostate cancer diagnosis, particularly in settings where expert radiologists may not be available. Another area of interest is the potential role of mpMRI in guiding focal therapies, such as high-intensity focused ultrasound (HIFU) or cryotherapy, for localized prostate cancer. By accurately delineating tumor margins, mpMRI could play a key role in the planning and execution of these minimally invasive treatments, further enhancing its value in the modern management of prostate cancer. Future studies should investigate the cost-effectiveness of mpMRI compared to TRUS and PET/CT to determine its economic viability as a primary diagnostic tool in diverse healthcare environments. The retrospective nature of this study introduces potential selection bias due to the reliance on previously completed cases, which limits control over consistent imaging protocols. To address this, future research should include prospective studies to validate current findings. Additionally, the influence of patient-specific factors such as prostate size and comorbidities on the diagnostic accuracy of mpMRI was not specifically evaluated. Future studies should consider these factors to better understand their potential impact. Research could also focus on combining imaging modalities to take advantage of their complementary strengths; for instance, integrating mpMRI's detailed anatomical imaging with PET/CT's metabolic data could improve diagnostic accuracy and facilitate more precise tumor localization and staging.
Conclusion
This study highlights the superior diagnostic performance of multiparametric magnetic resonance imaging (mpMRI) over transrectal ultrasound (TRUS) and positron emission tomography/computed tomography (PET/CT) in detecting clinically significant prostate cancer. With its high sensitivity, specificity, and ability to accurately identify aggressive tumors, mpMRI proves to be the most effective tool for early diagnosis in patients with elevated PSA levels and abnormal DRE findings. While TRUS and PET/CT have specific roles, particularly in biopsy guidance and metastatic assessment, their limitations in detecting early-stage prostate cancer reinforce the importance of mpMRI as a first-line imaging modality. Its non-invasive nature, combined with its ability to reduce unnecessary biopsies, supports its growing integration into clinical practice. In conclusion, mpMRI should be prioritized in prostate cancer diagnostics to improve early detection, guide treatment decisions, and enhance patient outcomes.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
All relevant datasets used and/or analyzed during the current study have been properly referenced in the manuscript, ensuring transparency and reproducibility. Where applicable, publicly available datasets have been identified and cited accordingly. Any restrictions or conditions regarding data access will be disclosed to maintain compliance with ethical guidelines and data protection policies.