
Abstract
Peritoneal dialysis (PD) is being promoted worldwide, but nearly half of all patients who start PD will no longer be on therapy at two years, representing an important barrier to maximizing the safe and effective use of the therapy. Loss most commonly occurs due to HD transfer, death, or the receipt of a kidney transplant, but can also occur because patients recover kidney function, transfer to another dialysis program, or are lost to follow-up. Historically, the term “technique failure” has been used to describe loss from PD, but there has been no consistent definition, and as a consequence, it has been unclear whether the observed variability in the reported risk is related to differences in patient characteristics, practice patterns, or simply differences in the way it was defined, measured, analyzed, or reported. The International Society for Peritoneal Dialysis (ISPD) convened a working group to provide recommendations around key issues related to measuring time on PD therapy. These included standardizing definitions for causes of loss, as well as their measurement, analysis, and reporting. Key performance indicators were proposed for the purpose of benchmarking and to facilitate quality improvement and research. The target audience of this document includes physicians and other healthcare providers, dialysis programs, researchers, and national registries.
This is a visual representation of the abstract.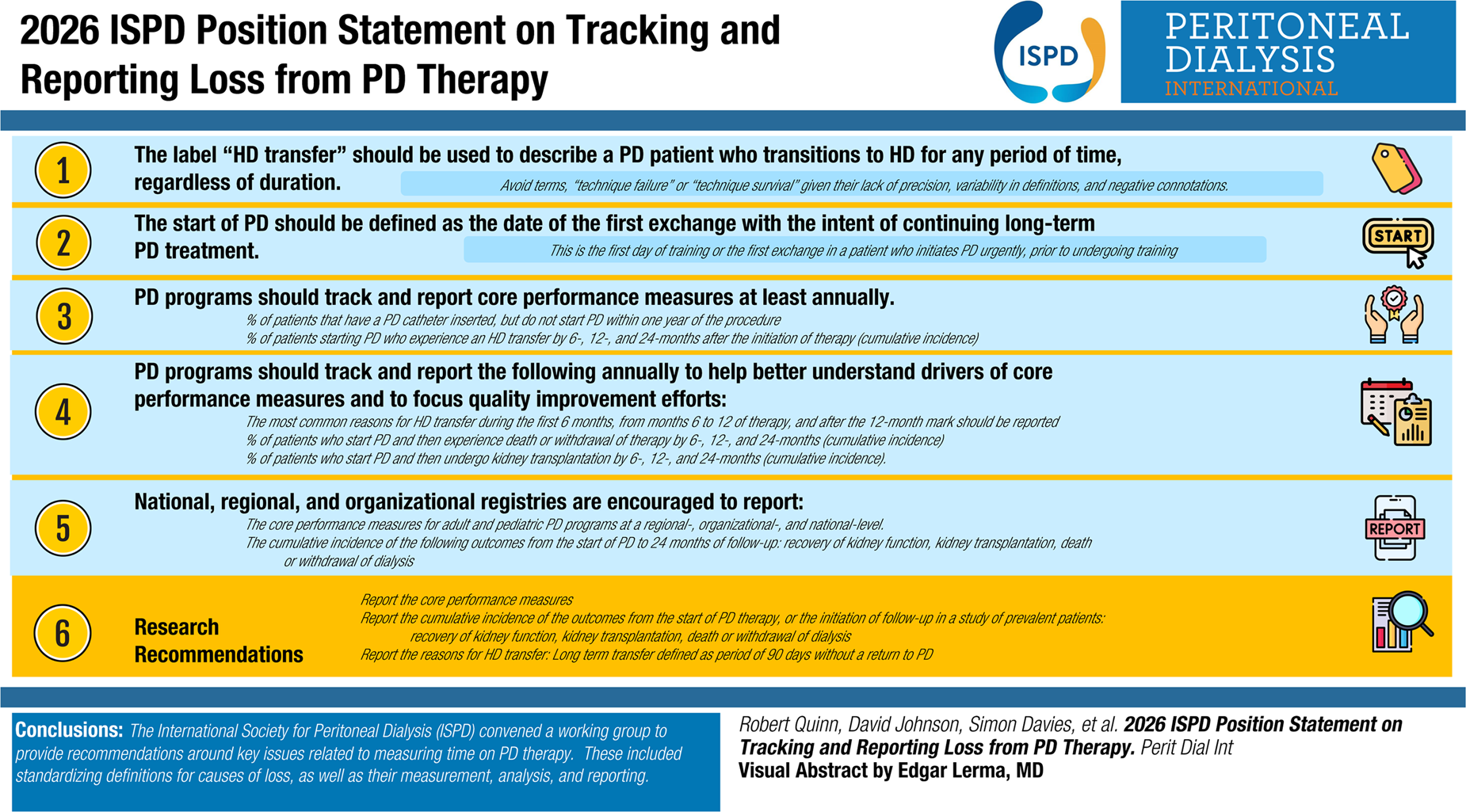
Key recommendations
The label “HD transfer” should be used to describe a PD patient who transitions to HD for any period of time, regardless of duration. Terms such as “technique failure” or “technique survival” should be avoided given their lack of precision, variability in definitions, and negative connotations.
The start of PD should be defined as the date of the first exchange with the intent of continuing long-term PD treatment. This is the first day of training or the first exchange in a patient who initiates PD urgently, prior to undergoing training.
PD programs should track and report the following core performance measures at least annually:
The percentage of patients that have a PD catheter inserted, but do not start PD within one year of the procedure. The percentage of patients starting PD who experience an HD transfer by 6-, 12-, and 24-months after the initiation of therapy (cumulative incidence). As an alternative to the latter, programs may choose to report the rate of HD transfer expressed as events per patient-year.
PD programs should track and report the following annually to help better understand drivers of core performance measures and to focus quality improvement efforts:
The most common reasons for HD transfer during the first 6 months, from months 6 to 12 of therapy, and after the 12-month mark should be reported. The percentage of patients who start PD and then experience death or withdrawal of therapy by 6-, 12-, and 24-months (cumulative incidence). The percentage of patients who start PD and then undergo kidney transplantation by 6-, 12-, and 24-months (cumulative incidence). As an alternative, programs may choose to report the rates of death or withdrawal of therapy, and kidney transplantation expressed as events per patient-year.
National, regional, and organizational registries are encouraged to report:
The core performance measures for adult and pediatric PD programs at a regional-, organizational-, and national-level. The cumulative incidence of the following outcomes from the start of PD to 24 months of follow-up:
▪ Recovery of kidney function ▪ Kidney transplantation ▪ Death or withdrawal of dialysis As an alternative, registries may choose to report the rates of death or withdrawal of therapy, and kidney transplantation expressed as events per patient-year.
For the purposes of research, it is recommended that investigators:
Report the core performance measures, as outlined above Report the cumulative incidence of the following outcomes from the start of PD therapy, or the initiation of follow-up in a study of prevalent patients:
▪ Recovery of kidney function ▪ Kidney transplantation ▪ Death or withdrawal of dialysis Report the reasons for HD transfer, according to the framework included in this document. While all HD transfers should be reported for quality improvement and research, regardless of duration, there may be situations where investigators wish to report HD transfers that are more likely to be long-term HD transfers. In these circumstances, we recommend using a period of 90 days without a return to PD to define a long-term transfer.
▪ For consistency in reporting, any patient who transfers to HD, but experiences another outcome during the 90-day period of observation that terminates follow-up (e.g. death, transplantation, recovery of kidney function, transfer out of the program, or loss to follow-up), should not be considered an HD transfer. The intervening event should be the outcome that ends follow-up.
Supporting recommendations
All patients who undergo peritoneal dialysis (PD) catheter insertion should be identified and the date of the procedure recorded.
The proportion of patients who do not start PD within one year of catheter insertion should be recorded and the reason they have not initiated PD documented.
All patients who start PD should be followed for: HD transfer, recovery of kidney function, kidney transplantation, withdrawal of dialysis (with or without palliative care) or death, loss to follow-up, and transfer to another PD program. When an outcome occurs, the date of occurrence should be recorded. Patients who stop PD for longer than 30 days, for any other reason, without commencing another kidney replacement therapy should be recorded as either kidney recovery or withdrawal of dialysis, depending on the expected outcome and reason for stopping PD.
It is suggested that programs document the most immediate reason for HD transfer (e.g. peritonitis requiring catheter removal) as well as other contributing reasons (e.g. patient or caregiver burnout). A suggested framework for documenting them for quality improvement or research purposes is provided.
Introduction
Peritoneal dialysis (PD) is associated with similar clinical outcomes and quality of life to facility-based hemodialysis (HD) but is less expensive to provide in most high-income countries.1–7 Consequently, PD is being promoted worldwide.8–10
Nearly half of all patients who start PD will no longer be on therapy at two years, representing an important barrier to maximizing the safe and effective use of the therapy.11,12 Loss most commonly occurs due to HD transfer, death, or the receipt of a kidney transplant, but can also occur because patients recover kidney function, transfer to another dialysis program, or are lost to follow-up. Historically, the term “technique failure” has been used to describe loss from PD, but there has been no consistent definition, and as a consequence, it has been unclear whether the observed variability in the reported risk is related to differences in patient characteristics, practice patterns, or simply differences in the way it was defined, measured, analyzed, or reported.11,13–15
More recently, patients, providers, and caregivers who participated in the international Standardized Outcome in Nephrology – Peritoneal Dialysis (SONG-PD) initiative highlighted the need to capture important aspects of the outcome, adopt neutral nomenclature, and ensure feasibility and applicability in clinical and research settings. 16 The group proposed replacing the core outcome measure “technique failure” with “transfer to HD,” but did not make firm recommendations regarding the definition or how to operationalize its measurement.
The International Society for Peritoneal Dialysis (ISPD) convened a working group to provide recommendations around key issues related to measuring time on PD therapy. These included standardizing definitions for causes of loss, as well as their measurement, analysis, and reporting. Key performance indicators were proposed for the purpose of benchmarking and to facilitate quality improvement and research. The target audience of this document includes physicians and other healthcare providers, dialysis programs, researchers, and national registries.
Rationale for recommendations
Key recommendation 1
The historical label “technique failure” has important shortcomings that have resulted in calls from patients, caregivers, and providers to abandon it in favor of clearer, more objective descriptors. Technique failure has been defined in different ways and at times has referred simply to HD transfers or to the composite of HD transfer and death, with or without kidney transplantation. 13 Combining outcomes is problematic, and it seems logical to report the risk of transferring to HD separate from the risk of death or receiving a kidney transplant, as they are distinct outcomes, and programs wish to maximize certain forms of loss from PD (e.g. kidney transplantation) but would endeavor to minimize others (e.g. death or HD transfer). Further, the causes of each, as well as the factors that predict them, likely differ, as would the extent to which they are modifiable.
As noted above, a recent SONG-PD consensus workshop was convened to establish a PD core technique survival measure, and the group highlighted the desire to capture important aspects of the outcome, adopt neutral nomenclature, and ensure feasibility and applicability in clinical and research settings. 16 There was a general feeling that technique failure had negative connotations and that it implied that a patient has failed or fallen short of expectations, when in some cases, a transfer to HD could be viewed as a positive outcome (e.g. in the case of inadequate dialysis on PD). The report from the SONG-PD workshop suggested focusing on HD transfers as the primary outcome measure but did not provide explicit guidance as to how to measure it.
HD transfers have been associated with higher morbidity, mortality, and costs and with poorer patient quality of life.17–22 There is also evidence that the risk of HD transfer varies between countries and between programs within a country. 12 It is likely that the issue that leads to HD transfer is responsible for the higher morbidity and mortality (e.g. peritonitis) in most cases, rather than the transfer itself being the culprit. However, it does represent a high-risk time in a PD patient's journey and supports the notion that taking steps to better understand and minimize the risk after HD transfers is important.
Transfers to HD are common, with up to 32% experiencing this event within two years of initiating PD. 11 Transfers may result from conditions, such as peritonitis, that require a temporary switch to HD, but patients may choose to return to PD after the infection clears, if possible. This has led to debate as to the length of time a patient must spend on HD before they are unlikely to return to PD. It has been shown that the likelihood of experiencing a permanent transfer to HD decreases, and median time on PD increases, as the required period of observation to qualify as a permanent transfer gets longer.11,14 In addition, the likelihood of returning to PD declines the longer patients spend on HD, and there are situations where resource constraints or logistical issues prolong time on HD, independent of the cause of the transfer.11,14
The issue of deciding the duration of time that a patient must spend on HD for the transfer to be considered a permanent switch is further complicated by the fact that patients may experience events that terminate follow-up while they are being observed for a return to PD. Several of these events are competing events (death, transplant, and recovery of kidney function) that make it very unlikely or impossible that a patient could have experienced permanent HD transfer had they continued to have been observed. The remaining events (transfer out of the program and end of follow-up) are censoring events after which it was still possible to experience transfer to HD. How one handles patients that experience events during the period of observation can change the estimated risk of transfer to HD by 4% at two years of follow-up. 11
The Working Group debated this issue at length, and in the end, the majority (by a vote of 11 to 6) felt that all transfers to HD should be reported for the purpose of performance measurement and quality improvement as they impact patients, caregivers, providers, and the health system. They disrupt and impact patient quality of life, lead to access procedures, are associated with morbidity and mortality, and result in a period of HD treatment that is generally more costly to the health system. In situations where patients transition from PD to a combination or hybrid of PD and HD, this should be considered an HD transfer for consistency. From the standpoint of data collection, the majority of programs will record outcomes in some form of database, and documenting all transfers to HD is less incremental work than identifying all transfers, monitoring their duration, and only counting them as transfers if they meet a minimum time on HD without experiencing any other competing events. Of note, there was general consensus that the terminology “permanent transfer to HD” should be avoided as it is not known if a transfer is going to be truly permanent or not, in many cases.
Some members of the Working Group felt that only transfers of a certain duration should be reported (e.g. HD for 30 days or more), although there was again disagreement regarding the required period of time.
Key recommendation 2
The Working Group felt it was important to have a consistent definition of the start of PD therapy that aligned with prior ISPD guideline statements. 23 The start of PD therapy is defined as “the day when the first PD exchange is performed with the intention of continuing long-term PD treatment from that day (i.e. first day of PD training or PD treatment in a hospital or at home with the intention of continuing PD long-term, whichever occurs first).” This date marks the end of the “Pre-PD” period and the start of follow-up for HD transfers and other causes of loss. Of note, this cohort includes incident PD patients, patients with a failed transplant who are starting PD, and individuals who are switching from HD to PD (Figure 1).
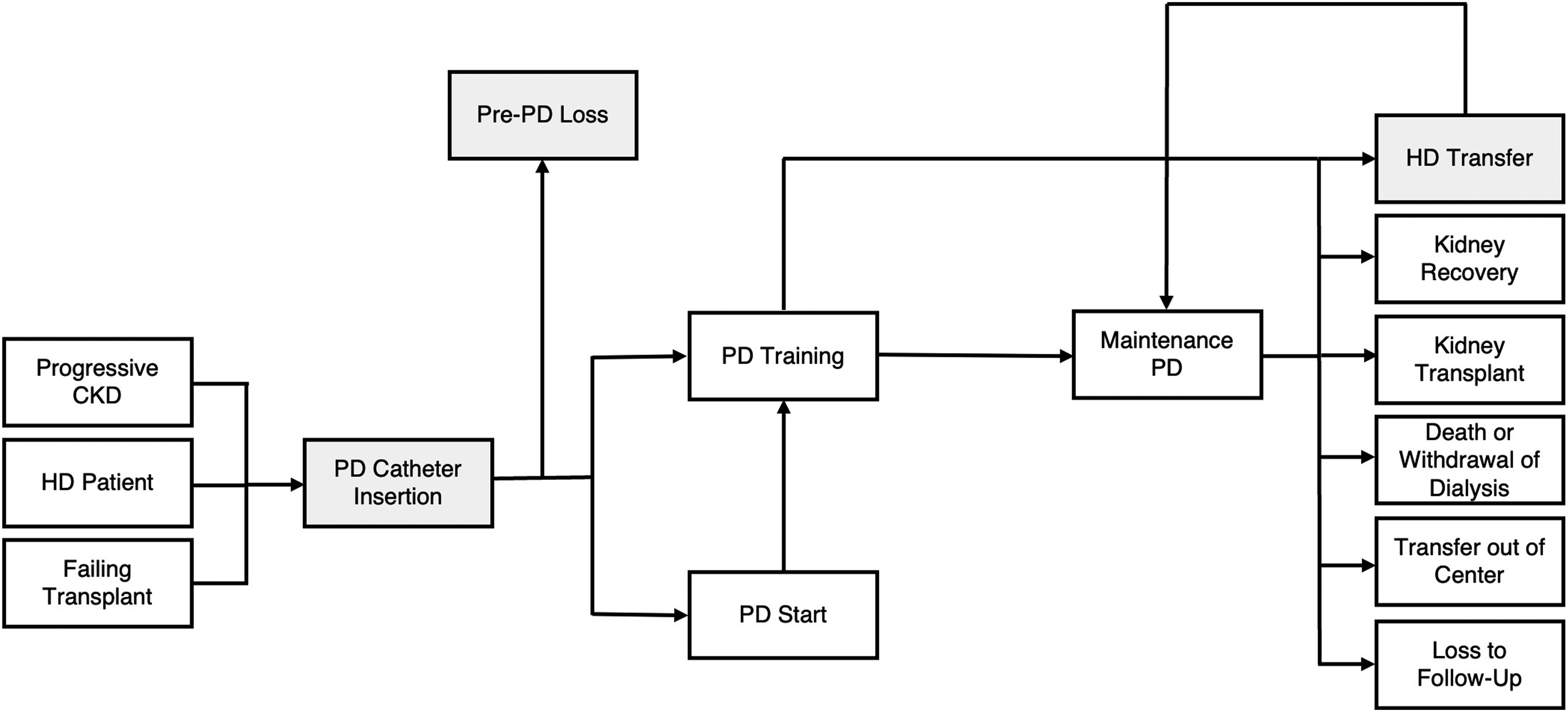
The potential trajectories of incident peritoneal dialysis (PD) patients. Incident PD patients may be drawn from several populations: individuals with progressive CKD approaching dialysis; HD patients who are transitioning from HD to PD; and those with failing transplants who are transitioning to PD. Once a PD catheter is inserted, some patients will go on to initiate PD, while others will not due to medical and social reasons, or death. Patients can initiate PD training or be started on PD urgently and subsequently undergo training if they continue on PD. Once training is completed, patients begin “maintenance” PD and are tracked for the occurrence of: HD transfer, recovery of kidney function, kidney transplant, transfer out of center, loss to follow-up, or death. Of note, some patients who experience HD transfers will return to PD after a period of time.
Key recommendation 3
Patients will be tracked from the time of the PD catheter insertion. To determine the ultimate fate of every catheter placed, patients would have to be followed for a prolonged duration, making the reporting of timely performance measures challenging. The rationale for using one year of follow-up is outlined in supporting recommendation 2. The issue of embedded PD catheters was also discussed as they are often placed earlier than traditional, non-embedded catheters. In published series, the median duration that the catheter was embedded prior to exteriorization ranged from 3 to 9 months, and the optimal time to exteriorization appeared to be between 6 weeks and 5 months with respect to minimizing mechanical complications and catheter loss.24–27
There is no universally agreed upon metric to benchmark program performance with respect to HD transfers, and there was disagreement among members of the expert consensus panel and the co-chairs as to the ideal approach. While there was general agreement regarding the importance of reporting the percentage of individuals that have a PD catheter inserted but do not start PD within one year, how to measure and report HD transfers was more controversial.
The two primary methods suggested were to report a rate of transfer to HD in a prevalent population, akin to the approach used for peritonitis, or to report the cumulative incidence of HD transfers in an incident population, which is the same as the proportion of patients who experience this outcome after a given duration of follow-up. Ultimately, the decision was put to a vote, and members voted 11 to 6 in favor of using the cumulative incidence of HD transfers as the primary performance measure. Some Working Group members felt that rates were inappropriate, others felt that both approaches had a role, and some felt that rates should be preferred.
This recommendation is consistent with how the United States Renal Data Systems (USRDS) reports HD transfers. In their 2022 Annual Data Report, they reported the cumulative incidence of conversion from home dialysis modalities (both PD and Home HD) to in-center HD among individuals initiating home dialysis during the time period of interest, treating death and transplantation as competing events. 28 Individuals were followed from the date of home dialysis initiation until the earliest date of transfer to in-center HD, death, kidney transplantation, switch between home dialysis modalities, switch to HD in a nursing home, recovery of kidney function, loss of follow-up, two years, or end of the time period of interest. Of note, an HD transfer was defined by use of in-center HD for at least 60 days. The cumulative incidence of HD transfers from the start of PD therapy to 24 months was presented. The outcomes of the first two years of therapy were visually depicted in 3-month increments, allowing the reader to visualize the proportion of patients on PD, in-center HD, Home HD, alive with a functioning transplant, dead, or lost for other causes.
The Working Group recommended a similar approach but felt that all HD transfers should be captured and reported, regardless of duration. Individuals starting PD should be followed for the earliest of the following events: transfer to HD (of any type), recovery of kidney function, transplantation, death, transfer out of the program, loss to follow-up, two years of follow-up, or the end of the reporting period of interest. The percentage of patients experiencing an HD transfer at pre-specified time points (6-, 12-, and 24-months) should be calculated and presented in a table. In programs with analytical or statistical support, the results can be presented using cumulative incidence curves that plot the proportion of patients experiencing an HD transfer from the start of PD until 24 months of follow-up.
The alternative metric, wherein the rate of HD transfers is reported, is similar to the approach recommended for reporting peritonitis rates. 23 This should be measured as the number of transfers to HD divided by the number of patient years at risk (i.e. number of years on PD starting from the time of PD commencement), reported as episodes per patient-year. Numbers of patient years at risk and of events should be fully inclusive, counting circumstances such as hospitalization episodes where patients may not be performing their own PD. In cases where PD is unsuccessfully retried and HD resumes, this should not be counted as a separate event if this second transfer is due to the unresolved reason for the initial transfer. Otherwise, subsequent transfers to HD after a PD restart should be considered as separate events, and they should all be captured as part of the transfer to HD rate determination.
The Working Group had originally planned to present a brief summary of the key issues raised during the debate as to what primary outcome measure should be proposed, but was not able to draft text that captured the discussion in a manner that was acceptable to members. This will likely be the topic of future work and warrants further discussion and debate.
Key recommendation 4
In patients who do not start PD within one year of PD catheter insertion, it is helpful to understand the reasons, which could include: recovery of kidney function, kidney transplantation, death or withdrawal from dialysis therapy, loss to follow-up, transfer to another dialysis program, initiation of HD, decision to pursue conservative care, or the lack of progression to kidney failure requiring initiation of dialysis therapy (Table 1).
Suggested framework for recording the reasons for not initiating PD within one year of PD catheter insertion.
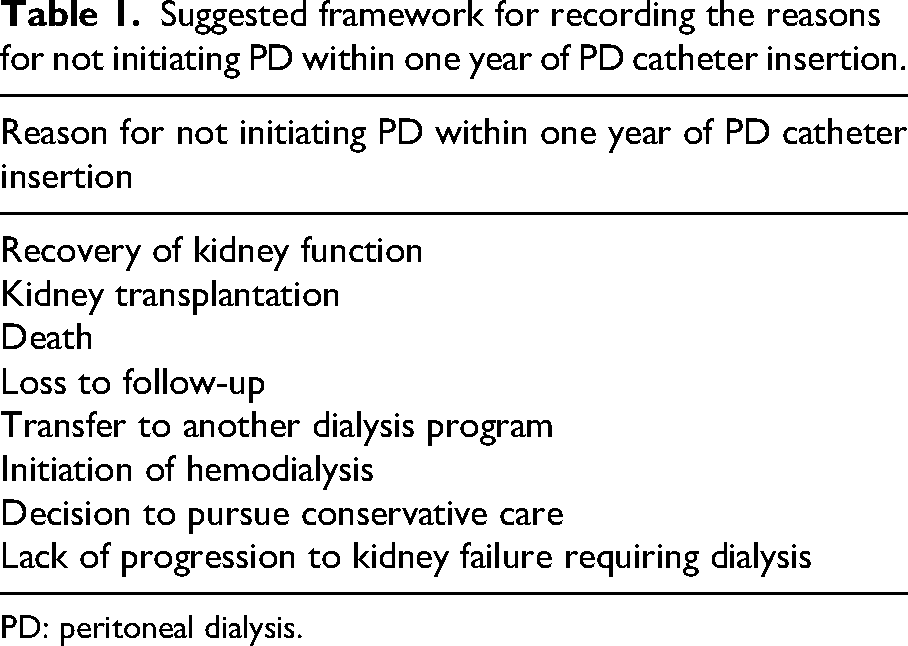
PD: peritoneal dialysis.
As discussed earlier, understanding the reasons for HD transfer and whether they are potentially modifiable is important to facilitate quality improvement initiatives. The Working Group recommends reporting causes of HD transfer that occur in the first 6 months of therapy, months 6 to 12, and after 12 months separately, given that the reasons for transfer will vary over time. Programs may also choose to target causes of early HD transfer preferentially, as they likely have the most negative impact from a patient, provider, and system perspective.
Loss from PD is common and occurs for reasons that are desirable (e.g. kidney transplantation or patient choice) and for reasons that are undesirable (e.g. patient death). Understanding the frequency of these competing events is helpful when interpreting the risk of HD transfer at a given time point and how it compares to other programs, countries, or how it has changed over time. Further, it highlights the total loss of patients from a PD program over time and the high incident rate that is required to maintain home dialysis populations or grow them in the face of that loss.
In programs with analytical or statistical support, the results can be presented using cumulative incidence curves, similar to HD transfers. Alternatively, the percentage of patients experiencing death or transplantation at 6-, 12-, and 24-months can be calculated and presented in a table.
The same approach used to calculate rates for transfers to HD should be used to calculate the rates of death and transplantation, if that measure is chosen.
Key recommendation 5
▪ ▪ ▪
National registries will usually be supported by data analysts or statisticians and would ideally report the performance measures as recommended for individual programs, regions, and for the country overall. Using cumulative incidence curves and/or tables reporting the risk of HD transfer, transplantation and death for the first two years of therapy is recommended. 28
Key recommendation 6
▪ ▪ ▪
While all HD transfers should be reported for quality improvement and research, regardless of duration, there may be situations where investigators wish to report HD transfers that are more likely to be long-term HD transfers. In these circumstances, we recommend using a period of 90 days without a return to PD to define a long-term transfer.
▪ For consistency in reporting, any patient who transfers to HD, but experiences another outcome during the 90-day period of observation that terminates follow-up (e.g. death, transplantation, recovery of kidney function, transfer out of the program, or loss to follow-up), should not be considered an HD transfer. The intervening event should be the outcome that ends follow-up.
The Working Group recommendations for reporting in research were largely in line with what was recommended for the purposes of quality improvement or registry reporting. It was, however, acknowledged that there might be situations where researchers might want to report the frequency of HD transfers of a certain duration (more likely to be long-term HD transfers). The ideal period of observation for a return to PD is not known and will always be a trade-off, with shorter periods leading to higher event rates and a greater likelihood that an individual will return to PD but requiring less time to capture. With longer periods of observation, the event rates will be lower, and individuals will be less likely to return to PD but require more time to observe. A 90-day period of observation for return to PD was felt to be a reasonable compromise.
One of the nuances of this type of analysis is the fact that patients are observed for a return to PD for a period after an HD transfer. If, during that period of observation, they experience another event that terminates follow-up (e.g. death, transplantation, recovery of kidney function, transfer out of a program, or loss to follow-up), it is not clear if they should be counted as an HD transfer or not. Prior work has shown that the risk of HD transfer differed by as much as 4% at two years, depending on whether individuals who experienced events during the observation period were counted or not. 11 To avoid ambiguity and to ensure consistency in reporting, it was the Working Group's recommendation that individuals who experience such an event during the observation period not be treated as an HD transfer. In some cases, it would not be possible to know if they would have returned to PD if they had continued to have been observed.
Supporting recommendation 1
Working Group agreed that all individuals who undergo PD catheter insertion with the intent of starting PD therapy should be identified and the date of the procedure recorded. This cohort should not include those who have a PD catheter placed for drainage of ascites or the management of heart failure in the absence of kidney failure, or for reasons other than the initiation of dialysis. This will ensure that a consistent cohort of patients is identified in all programs and ensures that all causes of loss from PD are captured and quantified.
Historically, outcome studies have tracked patients for the risk of events from the start of PD. However, there are patients who intend to do PD that never start on therapy and are therefore not captured when measuring loss from PD therapy. This group represents individuals who undergo an unnecessary procedure and never receive their intended form of dialysis. A population-based study from Ontario, Canada suggested that up to 17% of patients who underwent PD catheter insertion did not receive PD therapy during the study period. 29 Reasons included death, transplantation, lack of progression to kidney failure requiring dialysis, and the receipt of HD. Another Canadian cohort study estimated that 13% of patients who had chosen PD and had a PD catheter attempted never received PD at home. 30
The term “Pre-PD” is used to define the period between PD catheter insertion and the start of PD therapy.
Supporting recommendation 2
The time from PD catheter insertion to the start of PD is highly variable. In some cases, such as with urgent-start PD, the catheter is used immediately. In other cases, embedded catheters are placed and may not be used for months to years. The median time to use likely varies depending on several factors, including the method of placement, whether the catheter is embedded or not, and whether they are placed in pre-dialysis patients versus individuals on HD planning to transfer to PD.27,29,31–33 To determine the ultimate fate of every catheter placed, patients would have to be followed for a prolonged duration, which makes the reporting of timely performance measures challenging. Given that the reported median time from insertion to the start of PD therapy ranges from 29 days to 5 months in the literature and the upper bound of the interquartile range can approach 292 days, it was assumed that most patients who will start PD therapy would do so within one year of placement.27,29,31–33
In some cases, patients will experience events such as recovery of kidney function, kidney transplantation, death, loss to follow-up, transfer to another dialysis program, initiation of HD, or the decision to pursue conservative kidney management following catheter insertion that mean they will no longer pursue PD therapy. Such events should be termed “Pre-PD loss,” and the reasons for loss would ideally be reported. This metric provides insight into the proportion of patients who have a PD catheter placed that are unlikely to receive PD (Table 1).
In other cases, patients will still be under observation as they have not progressed to kidney failure requiring the initiation of dialysis therapy. These patients will be labelled as “not yet requiring dialysis” (Table 1).
Supporting recommendation 3
The events listed above terminate follow-up and represent outcomes of interest. Interruptions of PD therapy for any other reason that last more than 30 days typically reflect recovery of kidney function or the intention to withdraw from dialysis therapy. The Working Group felt it was important to clearly indicate that gaps of 30 days or longer are handled consistently across programs.
There was discussion about capturing periods where PD was put on hold for shorter periods of time. However, this would add to the burden of data collection without impacting the calculation of the proposed performance metrics. For programs that would like to capture periods where PD is put on hold (interruptions in therapy), a period of 7 days duration is recommended, as it is of sufficient duration that it reflects a response to a clinically relevant adverse event (e.g. leak). In situations where incremental prescriptions are used, patients may take several days off during the week, and this would not constitute an interruption of therapy, but rather a variant of an incremental prescription.
Supporting recommendation 4
The reasons for HD transfers are important to understand and should be recorded and reported to facilitate benchmarking and quality improvement efforts. Understanding the reasons for HD transfers and whether or not they are modifiable are key to interpreting local metrics and driving practice change. Classifications for causes of HD transfers have been developed for the Peritoneal Dialysis Outcomes and Practice Patterns Study (PDOPPS), 9 the Starting Dialysis on Time, At Home on the Right Therapy (START project),10,11 and the North American PD Catheter Registry. The Working Group felt that causes should be grouped by category, and a suggested list of reasons for HD transfers is included (Table 2). This guidance is also consistent with the SONG-PD technique survival consensus workshop findings. Of note, the reasons recorded at the time of HD transfer may differ from reasons recorded during a retrospective review of events, so they should be recorded at the time of the event, if at all possible.
Suggested framework for recording the cause of an HD transfer.
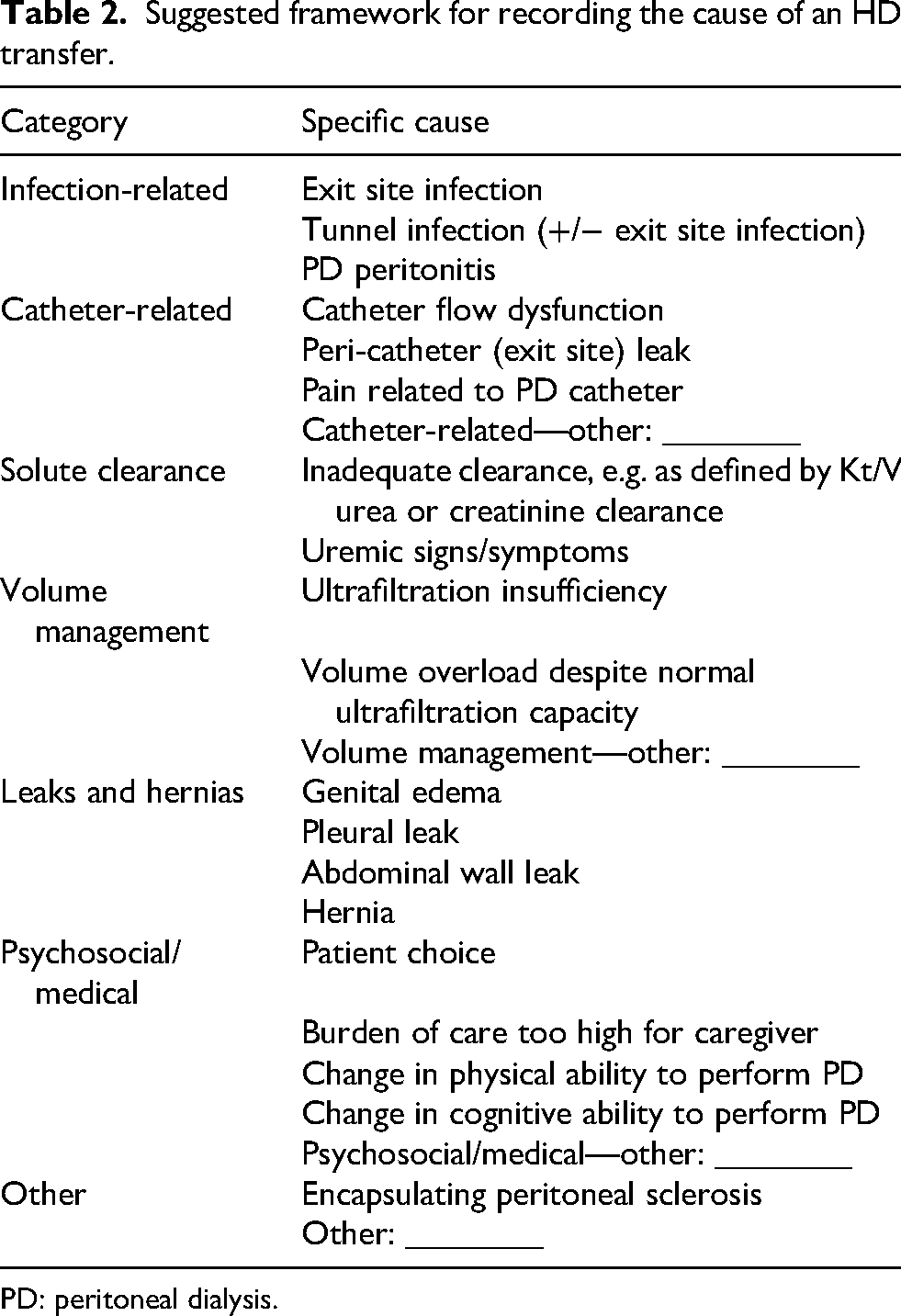
PD: peritoneal dialysis.
It is important to consider that a significant proportion of HD transfers will have an immediate cause but will also have other contributing factors. For example, a patient who is struggling to do PD at home may have an episode of peritonitis and choose to switch to HD, rather than re-attempt PD because they do not feel they can continue on therapy. In this case, the most immediate reason for the transfer to HD would be peritonitis, but the high burden of performing PD for that patient would be a contributing reason. The Working Group felt that it is important to identify the most immediate cause for transfer to HD (the complication that led to the switch) at a minimum. However, for programs with the capacity to track multiple potential reasons for the transfer, it is encouraged and may help to inform quality improvement initiatives to extend time on PD.
Summary and conclusions
The intent of this ISPD Position Statement is to standardize the reporting of causes of loss from PD therapy for the purposes of performance measurement, quality improvement, and research. The development of a common, pragmatic framework for approaching this problem was felt to be a necessary first step in understanding and improving practice. Further research and debate will help to shape future iterations and ensure that recommendations achieve their intended goal. The Working Group welcomes any, and all feedback.
Footnotes
Acknowledgements
We would like to acknowledge the contributions of Teresa (Tess) Harris, who was a member of the Working Group, but sadly passed away on 1 March 2024, prior to completion of the position statement.
ORCID iDs
Author contributions
RRQ and ML were the primary and senior authors, respectively, and were responsible for drafting the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interest
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Rob R. Quinn has a Canadian patent for the Dialysis Measurement Analysis & Reporting (DMAR) system and has received speaker's honoraria from Baxter Healthcare/Vantive. Mark Lambie is Co-Investigator on unrestricted investigator grant from Baxter Healthcare, Associate Editor for PDI, has participated in Medical Advisory Boards for Fresenius Medical Care and Vantive, and is a National Investigator for CSL Behring Study POSIBIL-6. David W Johnson has received consultancy fees, research grants, speaker's honoraria and travel sponsorships from Baxter Healthcare and Fresenius Medical Care, consultancy fees from AstraZeneca, Bayer and AWAK, speaker's honoraria from ONO and Boehringer Ingelheim & Lilly and travel sponsorships from Ono and Amgen. He is a current recipient of an Australian National Health and Medical Research Council Leadership Investigator Grant. Rajnish Mehrotra is currently Editor-in-Chief of the Journal of the American Society of Nephrology, the Senior EIC of the ASN Journal Portfolio, and the President of the International Society for Peritoneal Dialysis. Simon J Davies has received honoraria from Baxter HealthCare and Fresenius Medical Care and is on the steering group for the Behring CSL300_2301 POSIBIL₆ESKD trial. Angela Y-M Wang has received speaker honoraria from AstraZeneca, Fresenius Kabi and Bayer AG. She has served on the advisory board for Fresenius Kabi. She serves as a steering member for a phase 3 global clinical trial sponsored by CSL Behring. She has received a research grant from the International Society of Peritoneal Dialysis. Annie-Claire Nadeau-Fredette holds a scholarship from Fond de recherche du Québec – Santé and received an honorary for CME from Baxter. Jeffrey Perl serves on a speaker's bureau for Baxter Healthcare and Fresenius Medical Care and has received speaker fees from ARA, US Renal Care, Davita Healthcare, and has served as a consultant for Bayer, Baxter Healthcare, GSK, Otsuka, AstraZeneca, Amgen, Outset Medical as well as stock/stock options in iREN Medical. He has received salary support from Arbor Research Collaborative for Health, The International Society for Peritoneal Dialysis, and The American Society of Nephrology. He serves as Editor-in-Chief of Peritoneal Dialysis International and played no role in the editorial handling of the present manuscript. Ali K. Abu-Alfa has consulted and/or received honorarium from Baxter Healthcare/Vantive and Fresenius Medical Care. Olof Heimbürger has taken part in clinical trials sponsored by: AstraZeneca, Bayer, CSL Vifor, Hansa Biopharma, Iperboreal Pharma, Novartis, Travere Therapeutics, Triomed AB, Vertex Pharmaceuticals; received lecture honoraria from: Ewimed, Baxter Healthcare, Fresenius Medical Care, AstraZeneca, Vantive, Vifor, Bayer for presentations at company-organized courses; participated in speakers bureaus for: AstraZeneca. He also is on the editorial board of Peritoneal Dialysis International and a member of ISPD, ERA, and Svensk Njurmedicinsk Förening. Annabel Boyer has received speaker honoraria from Vantive and Fresenius. Arpana Iyengar has no disclosures. Danielle E Fox has no disclosures. Thyago Proença de Moraes has received speaker honoraria (1) and consultant fees (2) from: Vantive (1 and 2); AstraZeneca (1 and 2); Lilly (1 and 2); Boehringer (1 and 2); Novo Nordisk (1 and 2); CSL Vifor (1); Merck (1); Servier (1); Bayer (1); Pfizer (2). Mignon McCulloch, Patricia Gooden, and Nancy Verdin have no disclosures.