
Abstract
Current intracranial pressure (ICP)-related parameters monitoring is invasive and tends to cause complications, which limit their use to predict patients’ intracranial status and prognosis. To utilize post-operative computed tomography (CT) images radiomic features techniques to predict abnormal ICP-related parameter levels consisting of an index of cerebrospinal compensatory reserve (RAP) and a pressure reactivity index (PRx) in patients with traumatic brain injury (TBI) noninvasively, 60 patients were enrolled and randomized to training (n = 42) and test (n = 18) sets. Data of 20 patients from another hospital were used to validate the model. A total of 107 radiomic features were extracted from each patient’s CT image. Their clinical and imaging data were collected and analyzed to establish prediction models of RAP and PRx, respectively. Univariate regression analysis and least absolute shrinkage and selection operator method were used for feature selection, and multivariate logistic regression was used to develop the predictive models. The nomogram was assessed with respect to its calibration and clinical usefulness. The RAP model showed a good discrimination with the area under the receiver operating characteristic curve (AUC) of training and test sets was 0.789 (95% confidence interval [CI]: 0.635–0.944) and 0.818 (95% CI: 0.578–0.998). The performance of PRx model was inferior to the RAP model, but still had a significant discrimination with the AUCs of training and test were 0.713 (95% CI: 0.676–0.920) and 0.667 (95% CI: 0.554–0.803). Application of the nomogram and calibration curve also showed that the two models had excellent model predictions and clinical usefulness. The external validation results of RAP and PRx showed a good discrimination with an AUC of 0.813 (95% CI: 0.586–1) and 0.781 (95% CI: 0.565–0.997). The study illustrated that CT radiomic features as a clinical aid may have the ability to predict ICP-related parameters to reflect the intracranial condition of patients with TBI noninvasively given its potential for clinical treatment guidance and prognosis indication.
Introduction
Traumatic brain injury (TBI) is one of the common critical diseases in neurosurgery and also one of the major public health problems in the world. There are more than 50 million people suffering a TBI each year, according to a previous report, 1 which makes high mortality and disability, especially on young adults. 2 Therefore, it is significant for doctors to monitor post-operative condition for patients with TBI and do prompt treatment to improve prognosis. Intracranial pressure (ICP) monitoring is widely used to evaluate intracranial status in neurosurgery department, 3 but a large randomized trial recently could not show any benefits of ICP monitoring compared with clinical examination and images, 4 which indicated that a single ICP value could not reflect comprehensive information about intracranial status for patients with TBI. On the contrary, ICP-related parameters such as an index of cerebrospinal compensatory reserve (RAP) and a pressure reactivity index (PRx), which reflect the status of intracerebral circulation, cerebrospinal compensatory reserve, and brain compliance, have attracted more attention to guild the treatment and predict the outcome of patients with TBI recently. 5,6
However, the ICP-related parameters still need invasive medical operations via ICP probe placement and radial artery puncture, which can cause inevitable complications such as infection and hemorrhage. 7,8 Computed tomography (CT) scanning is one of the common medical techniques to assist neurosurgeons in evaluating the severity of patients with TBI. High efficiency and noninvasiveness give it potential to evaluate ICP-related parameters by using radiomic analysis, which is a process of converting digital medical images into mineable high-dimensional data via extraction of quantitative features and subsequent data analysis for decision support. 9 Radiomics has shown promise for extracting image features to evaluate neurosurgical diseases, such as the diagnosis of tumors, 10 and the prediction of hematoma enlargement, 11 which gives it potential to assess ICP-related parameters based on some pilot research. 12 The aim of our study is to seek optimal radiomic models to discover whether CT radiomic features could have the ability to predict ICP-related parameters (RAP and PRx are included) in patients with TBI by developing prediction model using training set, which was validated by testing set.
Materials and Methods
Study design and setting
Participants with a clinical diagnosis of TBI from the Shanghai General Hospital were retrospectively retrieved during January 2022 to June 2023. Their demographic data, clinical characteristics, post-operative CT images, and ICP-related parameters were collected and analyzed. The main inclusion criteria were (1) patients older than 18 years old and younger than 80 years old; (2) emergency department admission for acute closed craniocerebral injury; (3) received invasive ICP and arterial pressure monitoring and their data were complete; (4) received cranial CT scan within 1 h after surgery. Main exclusion criteria were (1) patients with previous intracranial anatomical structural changes caused by TBI, cerebral infarction, brain tumors, or other neurological diseases or cranial surgical intervention; (2) with previous coagulopathy and blood system-related diseases; (3) patients’ data were incomplete or lost. The eligible patients were randomly allocated to training and testing sets according to 7:3 proportion. Models were fitted on the training set and were independently tested on the testing set. The detailed enrollment process is depicted in Figure 1. All patients were treated according to the Clinical Guidelines for the Management of Head Injury. 13
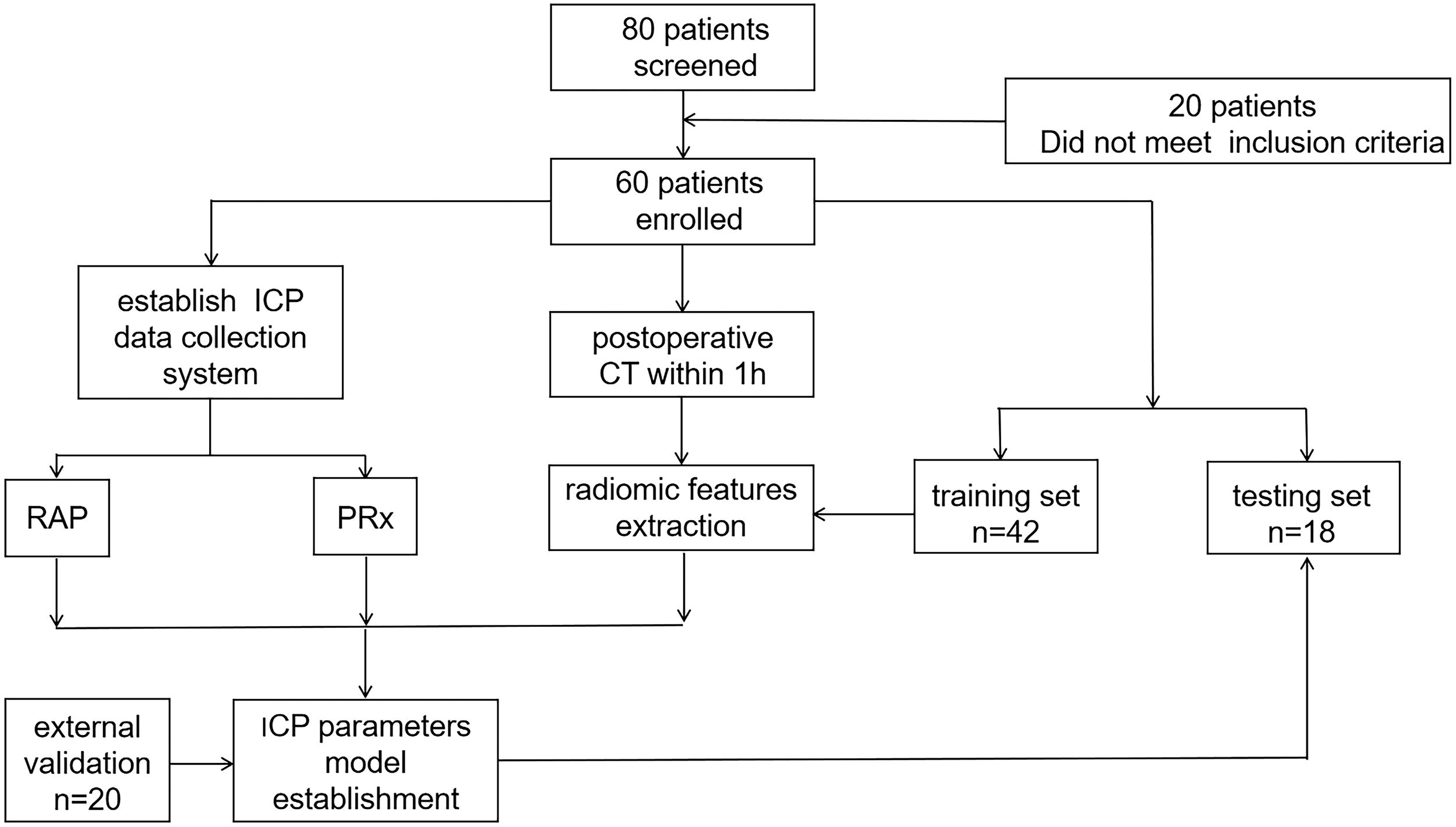
Flowchart illustrating the process of case collection and data analysis for developing the model for ICP parameter prediction. ICP, intracranial pressure; PRx, pressure reactivity index; RAP, index of cerebrospinal compensatory reserve.
The study protocol conformed to the ethical guidelines of the Declaration of Helsinki, and his study was approved by the Ethics Committee of Shanghai General Hospital, Shanghai Jiao Tong University School of Medicine. Participants’ right to know was fully guaranteed and indicated in the ethical approval document. All included patients and their family had fully informed consent right.
The external cohort of 20 patients was selected following the same criteria mentioned above from January 2024 to December 2024 at the Department of Neurosurgery of Xinhua Hospital.
ICP-related parameters acquisition
All patients with TBI underwent invasive ICP monitoring by using an ICP sensor (Integra LifeSciences, USA) placed in the frontal corner of the ventricle and returned to intensive care unit. Then arterial line placement was performed on patients’ left or right artery for continuous ICP and arterial blood pressure (ABP) monitoring. All RAP and PRx data collected within 1 h after the start of monitoring (monitoring sampling frequency is 6 s, a total of 50 data points in 5 min) were recorded, and their mean values were taken into analysis. RAP was derived by calculating linear correlation between consecutive, time-averaged data points of the amplitude (AMP) of ICP and ICP (50 of such samples are used), which reflected the degree of correlation between AMP and mean ICP over 5 min. Similarly, PRx was determined by calculating the correlation coefficient between 50 consecutive, time-averaged data points of ICP and ABP.
CT examination and brain segmentation
The cranial CT image was performed after the surgery and before the ICP parameters recording. As per the routine protocol of a CT scan, the CT slices were parallel to the orbitomeatal plane from the foramen magnum to the vertex. The scanning slice thickness was 1 mm. The brain segmentation was acquired from the Digital Imaging and Communications in Medicine (DICOM) file of post-operative CT scan within 1 h. The DICOM files of the CT were imported into the 3D slicer software (3.6.0, www.slicer.org) to segment the volume of interest (VOI) slice by slice manually and reconstruct the CT-segmented brain (Supplementary Appendix Fig. A1).
Radiomic features extraction and selection
The radiomic features were extracted from the VOI using PyRadiomics module in the 3D slicer software. The software could extract first-order features, second-order features, higher-order features, and shape features from the CT original images. Two experienced radiologists were randomly assigned 24 CT images for VOI-based feature extraction. Intraclass correlation coefficient (ICC) analysis was used to assess reproducibility and consistency of measurements. Features with an ICC >0.75 were chosen for future analysis.
The value of radiomic features data was then standardized using a z-score transformation. To avoid overfitting and maximize model generalizability, feature selection needs to be done before model establishment, and the number of selected features should be about one-tenth of the cases in the training set. First, univariate logistic regression analysis between the radiomic features data and ICP-related parameters (RAP and PRx groups) was conducted to screen the features whose p value was <0.2, respectively, then the least absolute shrinkage and selection operator (LASSO) method, applicable for the high-dimensional data, was used to select the most valuable features in the two groups. After that, the remaining features having significant correlation differences with ICP-related parameters were considered in subsequent multivariate logistic regression models.
Establishment and performance of prediction models
According to the features selected in RAP and PRx groups, multivariate logistic regression models were established to evaluate their levels of patients in training set and validate in testing set. In RAP group, 0.5 was chosen as the threshold value according to the previous study, which indicated RAP <0.5 has an unfavorable outcome in patients with TBI. 14 Also, 0.2 was selected as a dichotomous judgment for PRx bigger than 0.2 considered to be an indicator of poor prognosis. 15 A nomogram was constructed based on the radiomic features selected by the multivariate logistic regression test. Accuracy, specificity, recall, and F1 score were used to evaluate the performance of each model. Both models used the area under the receiver operator characteristic (ROC) curve (AUC) to assess the discriminative power. Calibration curves were plotted to assess the calibration of the prediction models, accompanied by the Hosmer–Lemeshow test.
Statistical analysis
Data analysis and nomogram establishment were statistically performed using R version 3.3.1 (R Project for Statistical Computing) and Statistical Package for Social Sciences (SPSS 22.0; IBM, USA). Continuous variables subject to normal distribution were expressed as mean ± standard deviation, continuous variables not subject to normal distribution were expressed as the median and interquartile range, and categorical variables were expressed as frequency and percentage. A two-sided p < 0.05 was considered a statistically significant difference.
Results
Clinical characteristics
Our study comprised 60 patients with TBI after excluding 20 patients based on the inclusion criteria, with 42 (70.00%) in training set and 18 (30.00%) in testing set. There were 41 male patients (68.33%) and 19 female patients (31.67%) with a mean age of 62.38 years, ranging from 37 to 80 years. The causes of injuries included traffic accidents (27, 56.25%), fall from heights (8, 16.67%), and falls (13, 27.08%). In addition, 31 patients had brain contusion, 24 had intracranial hematoma, 19 had subdural hematoma, 4 had epidural hematoma, and 6 had subarachnoid hemorrhage. There were no statistically significant differences in clinical characteristics between RAP and PRx groups (Supplementary Appendix Table A1), which excluded clinical effect on the performance of models.
CT radiomic features selection and model building
After intra- and interreader ICC analysis, a total of 107 radiomic features were considered robust and consistent. Then features whose p value >0.2 were discarded using univariate regression analysis. In the RAP group, 22 features were finally reduced to 5 by the LASSO method, with nonzero coefficients representing weight among all features. In this condition, mean square error was the lowest to minimize the error and improve the performance of the model (Fig. 2A and B). The five features and their coefficients are shown in Table 2. Similarly, 34 features were screened to 3 potential predictors in the PRx group (Fig. 3A and B) and were features with nonzero coefficients in the LASSO method (Table 1). Univariate regression analysis indicated RAP levels were correlated with three shape features and two second-order features, and two second-order and one higher-order features were considered predictor factors of PRx levels. Five and three different features were, respectively, screened in multivariate logistic regression models establishment of RAP and PRx (Tables 1 and 2). The two models that incorporated the above radiomic features were developed and presented as the nomograms (Supplementary Appendix Figs. A2 and A3).
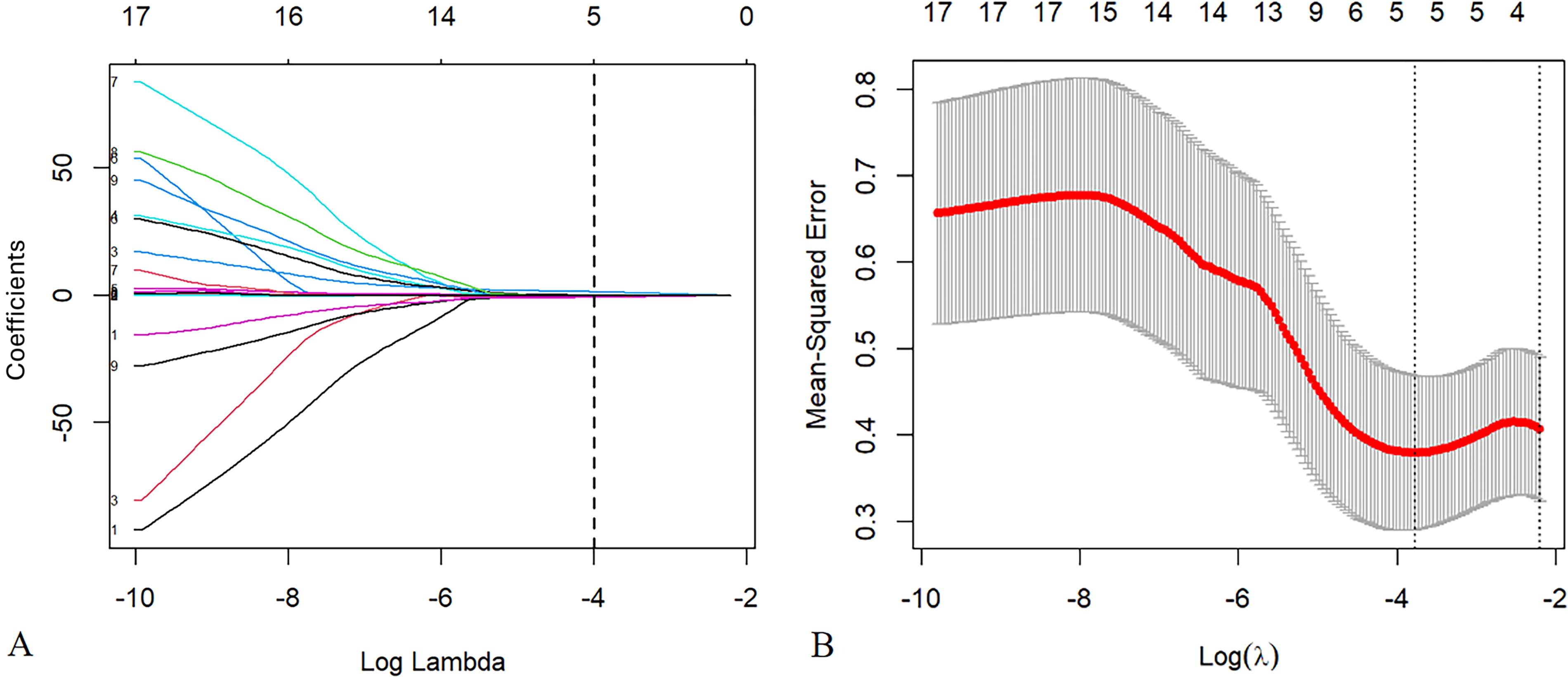
Radiomics feature selection using the least absolute shrinkage and selection operator (LASSO) binary logistic regression model in RAP group.
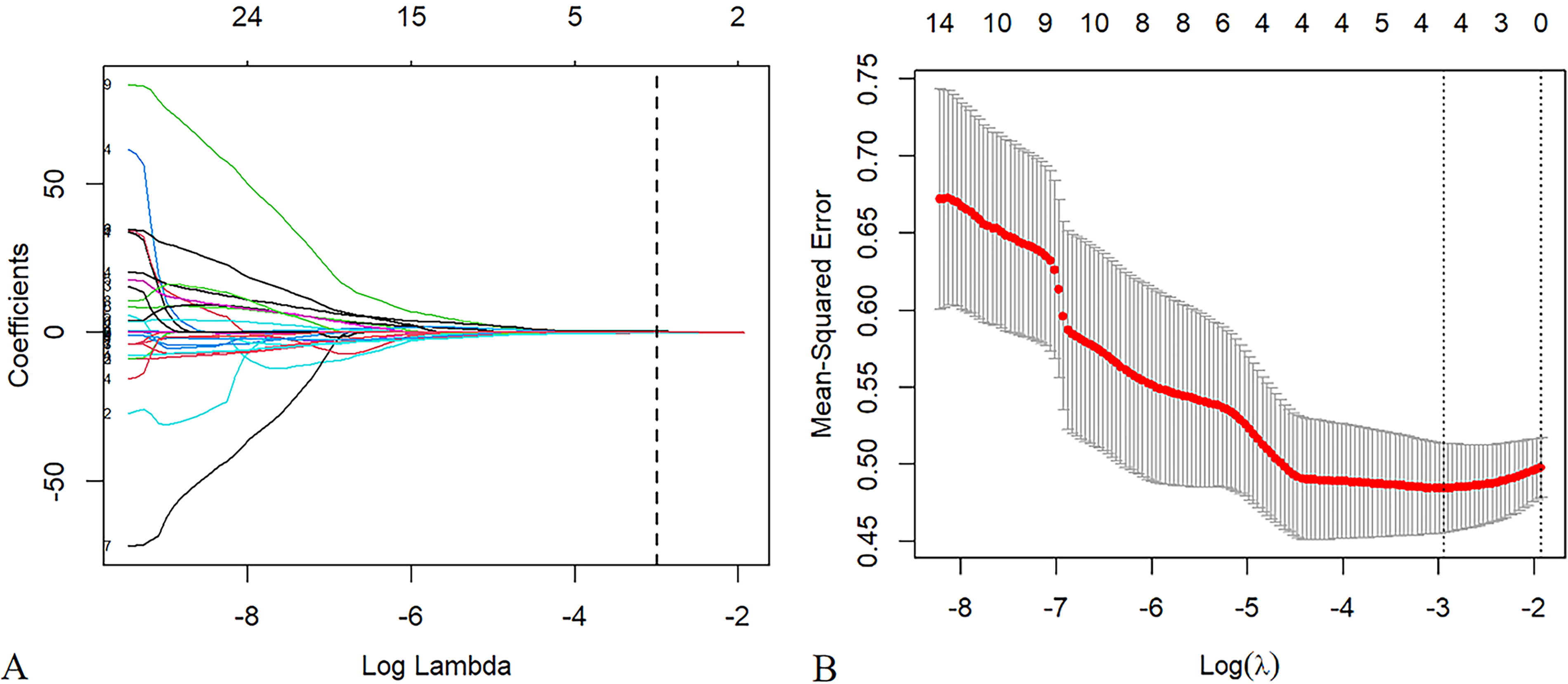
Radiomics feature selection using the least absolute shrinkage and selection operator (LASSO) binary logistic regression model in PRx group.
Results of Least Absolute Shrinkage and Selection Operator Selection Multivariate Logistic Regression Analysis for Evaluation of Abnormal RAP Value Based on Radiomic Features
CI, confidence interval; Lasso, least absolute shrinkage and selection operator; RAP, index of cerebrospinal compensatory reserve; Sig., level of significance.
Results of Least Absolute Shrinkage and Selection Operator Selection and Multivariate Logistic Regression Analysis for Evaluation of Abnormal Pressure Reactivity Index Value Based on Radiomic Features
CI, confidence interval; Lasso, least absolute shrinkage and selection operator; RAP, index of cerebrospinal compensatory reserve; Sig., level of significance.
The performance of two models
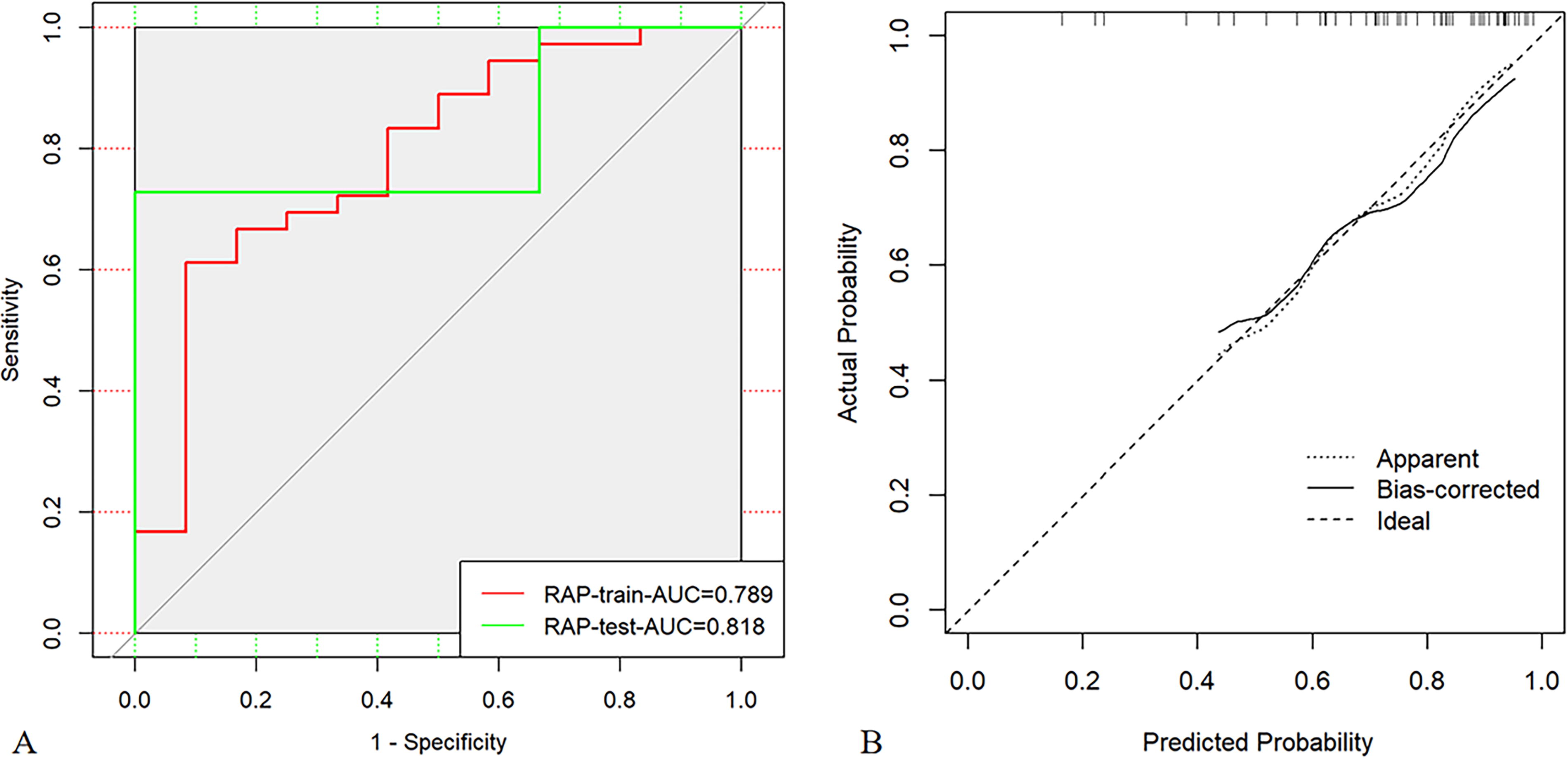
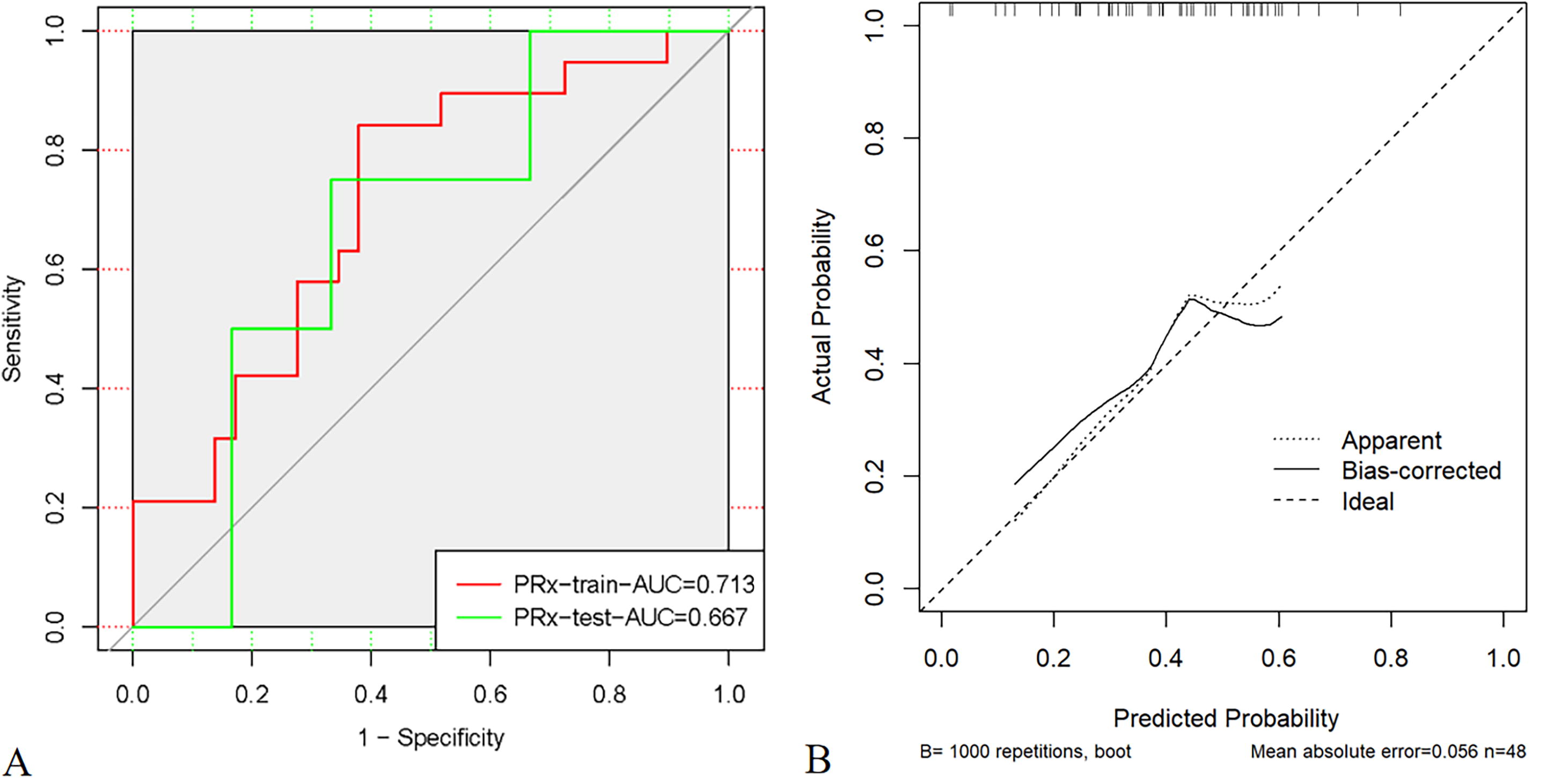
The AUC of RAP model with four radiomic features finally included in the training and testing set were 0.789 (95% confidence interval [CI]: 0.635–0.944) and 0.818 (95% CI: 0.678–0.998) to distinguish abnormal RAP levels (Fig. 4A). Calibration plot was used to illustrate the goodness of fit in testing set to determine the agreement between the predicted and observed RAP levels (Fig. 4B). The Hosmer–Lemeshow test showed a nonsignificant difference, which suggested a small difference from perfect fit between the predicted and observed RAP levels. The performance of PRx model was inferior to RAP model, the AUC was 0.667 (95% CI: 0.554–0.803) in testing set (Fig. 5A), and calibration plot and Hosmer–Lemeshow test still showed a good model fit (Fig. 5B). Besides, the accuracy, specificity, recall rate, and F1 score of two models were shown in Table 3.
Performance of Two Testing Models Based on Radiomic Features
PRx, pressure reactivity index; RAP, index of cerebrospinal compensatory reserve.
Twenty patients with TBI were screened in the external cohort to validate the prediction ability of two models. There were 12 male patients and 8 female patients with a median age of 60.2 years. The ROC curve analysis of external validation showed that the AUCs of RAP and PRx models were 0.813 (95% CI: 0.586–1) and 0.781 (95% CI: 0.565–0.997), respectively (Supplementary Appendix Figs A4 and A5). In addition, the calibration curves both revealed a good agreement in the validation cohort.
Discussion
In this study, we enrolled 60 patients with TBI and analyzed their post-operative CT images to predict their RAP and PRx levels by establishing CT radiomic features-related regression models, and the performance of RAP and PRx models was compared. The results demonstrated that CT radiomic features could have the ability to predict RAP and PRx levels in patients with TBI, and RAP levels have better advantages to be predicted according to the performance of two models.
ICP monitoring is regarded as a significant clinical process for neurosurgical patients to maintain their static pressure parameter, mean ICP <20–25 mmHg. 16 Nowadays, the focus of ICP monitoring is mainly on the mean ICP value while ignoring other parameters, which may carry risks of inaccuracy or delay. 4,17 On the contrary, the ICP-derived parameters such as ICP waveform, RAP, and PRx are reported to have great significance in predicting prognosis and guiding proper treatment. 18 –20 Nevertheless, all these parameters require multimodality monitoring and big data acquisition and analysis, which takes a lot of time and effort. A previous study also had some attempts to evaluate these parameters using noninvasive ways. Bernhard and his colleagues found that PRx could be assessed by using cerebral blood flow velocity and ABP based on a mathematical model. 21 Liu also showed that the RAP levels could be judged by using a machine learning model based on texture features analysis. 12 Approach to measuring retinal arteriole and venule diameter ratio on fundus photography also exhibits a good ability to predict ICP levels. 22 Limited by low accessibility and effectiveness, none of these methods could be widely applied in clinical practice. On the contrary, CT images make it possible to evaluate and determine the abnormal ICP-related parameter levels with their convenience and noninvasiveness. In fact, many scholars have discovered the CT’s potential value to assess intracranial status in patients with TBI. Pappu illustrated that the ratio of cerebrospinal fluid volume to the size of the intracranial vault or volume inside the skull could predict the risk of increased ICP. 23 CT images were also utilized to evaluate the severity and prognosis of patients with TBI based on CT scoring systems such as Marshall classification and Rotterdam CT score. 24 We took these theoretical research results for reference and compared their advantages and drawbacks, and radiomic analysis, which was manipulated digitally, was introduced into our study to increase the accessibility and reduce the subjective bias on ICP-related parameters assessment.
Radiomic analysis was first systematically proposed by Lambin in 2012. 25 It describes the relationship between gray values in an image through features extracted from commercially available or internal software tools. Features mainly fall into the following categories: shape features, first-order features, second-order features, and higher-order features. 26 In RAP model, we included three shape features into analysis, which indicated that the change of brain spatial volume may affect the ability of cerebrospinal compensatory reserve. In PRx model, two first-order features were taken into model establishment, suggesting that the pixel intensity in the total brain changed in the condition of poor cerebral autoregulation. The advantage of higher-order features is that the relationship between adjacent voxels is fully considered. Both RAP and PRx models have one or two second- and higher-order features to predict intracranial status, which placed emphasis on the differences between local pixels in VOI. The structure and density changes in the brain tissue in patients with TBI can be reflected through our method for analyzing feature data on CT images. The research of radiomics in TBI is limited due to the uncertainty and irregularity of its lesions, making it difficult to extract the image VOI using a standardized process. Therefore, the VOI is often more inclined to be selected in brain tissues surrounding lesions. Zhang has successfully predicted the progress and clinical results of hematoma in patients with brain contusion by using the radiomic features model. 27 In our study, we extracted the whole brain tissues as a VOI to minimize the subjective factors of CT images segmentation and improve the validity in predicting ICP-related parameters.
In patients with TBI, intracranial hypertension is a typical pathophysiological result caused by secondary injury after brain trauma. RAP, namely the correlation coefficient between ICP AMP and ICP mean value, ranges from −1 to 1, mainly reflecting the compensatory reserve capacity of the cerebrospinal reserve. 16 In theory, compensatory reserve can be studied through the relationship between mean ICP and brain space volume changes. Our study results showed that selected shape-order features are the predominant factors to reflect the changes of brain space volume, and with the AUC of 0.82 in testing set and 79.17% accuracy, CT radiomic features had an excellent ability to predict RAP levels in patients with TBI. The prediction of PRx levels was not, as well as the RAP, with its AUC of 0.67 in testing set and 62.50% accuracy, which suggested that the difference of CT images in different cerebrovascular reactivity could not be described perfectly through CT radiomic features. The first-order and second-order features may be associated with the PRx levels according to our results. PRx is an index obtained by calculating the ratio between the mean ICP value and the mean ABP value. It observes the response of ICP to the spontaneous changes of ABP to evaluate the cerebrovascular pressure reactivity, 15 reflecting the ability of smooth muscle tension in the cerebral artery and arteriole wall to respond to changes in transmural pressure. The deterioration of brain vessels leads to the ischemic cerebral status, which could be detected through radiomic features to find the pixels and density differences.
In summary, our study gives the CT radiomic features possible to predict the ICP parameters noninvasively to guide clinical decisions and prognosis. However, there are also some limitations to improve. First, the sample size in our study was relatively small and from a single center; it lacks external validation of data from other centers. The number of radiomic features that our models could contain was also limited, which could reduce the accuracy as a result. Second, since the post-operative cranial CT scan and the ICP-related parameters were measured nonconcurrently, the time gap between the two could yield discordance between the results. Third, the surgical operation, such as decompressive craniectomy, could also affect the collected parameters. 28 Last, individual factors of patients with TBI may also have different thresholds in RAP and PRx levels, which introduce inaccuracy in the results.
Conclusions
Our study illustrated that radiomic analysis may have great potential to predict RAP and PRx levels to reflect the comprehensive cerebral status noninvasively. Given that the AUC of RAP and PRx still have the place for improvement, the results derived from the models need to be further validated in other independent datasets to achieve more robust prediction ability. The finding of this study gives it possible to serve CT radiomic features as a clinical aid for clinical treatment guidance and prognosis indication. This also gives promise for further study to improve and perfect the performance of models to save medical resources.
Transparency, Rigor, and Reproducibility Statement
The study was preregistered at clinicaltrials.gov (NCT03087981). A total sample size of 60 subjects was planned to allow a model development set, yielding 80% power prognostic accuracy for primary clinical outcome with a p value <0.05. Eighty potential participants were screened, imaging data were obtained from 80 and successfully analyzed in 60. Participants were told the results of the imaging assessments after the final clinical observations had been made. Imaging quality control decisions and analyses were performed by investigators who were aware of the relevant characteristics of the participants. All equipment and software used to perform imaging and preprocessing are widely available from commercial sources. The key inclusion criteria and outcome evaluations are established standards. External validation studies are ongoing. De-identified data from this study are not available in a public archive. De-identified data from this study will be made available by emailing the corresponding author. The analytic code used to conduct the analyses is available in GitHub. The authors agree or have agreed to publish the article using the Mary Ann Liebert Inc. “Open Access” option under appropriate license.
Footnotes
Acknowledgments
The authors would like to thank all colleagues in the Department of Neurosurgery for their work. An earlier version of the article named “Noninvasive Prediction for Intracranial Pressure Related Parameters in Traumatic Brain Injury Patients Using Computed Tomography Radiomic Features” was submitted to a preprint server, “Research Square.” The website of the server is ![]() , and the DOI of the article is 10.21203/rs.3.rs-2797523/v1.
, and the DOI of the article is 10.21203/rs.3.rs-2797523/v1.
Authors’ Contributions
Y.L.: Conceptualization (equal), formal analysis (lead), methodology (lead), resources (equal), validation (equal), writing—original draft (lead), and writing—review and editing (equal). Y.Z.: Conceptualization (equal), resources (equal), validation (equal), and software (lead). Y.S.: Conceptualization (equal), resources (equal), and supervision (equal). X.W.: Conceptualization (equal), resources (equal), and supervision (equal). J.Z.: Conceptualization (equal), resources (equal), and supervision (equal). S.L.: Conceptualization (equal), resources (equal), and supervision (equal). G.G.: Conceptualization (lead), funding acquisition (lead), project administration (lead), and writing—review and editing (equal).
Ethics Approval
The study protocol conformed to the ethical guidelines of the Declaration of Helsinki, and this study was approved by the Ethics Committee of Shanghai General Hospital, Shanghai Jiao Tong University School of Medicine.
Consent to Participate
Informed consent was obtained from all individual participants included in the study.
Data and Code Availability
Author Disclosure Statement
The authors have no relevant financial or nonfinancial interests to disclose.
Funding Information
This work was supported by the National Natural Science Foundation of China (Grant Numbers 81671198 and 81971699) and the Clinical Research Innovation Plan of Shanghai General Hospital.
Supplementary Material
Supplementary Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.