
Abstract
Spinal cord injury (SCI) is a debilitating condition resulting in the loss of sensorimotor functioning at and below the site of injury. Despite advances in the treatment and management of SCI, there are no current approved pharmacological therapies to augment motor function and functional recovery. NX210c is a 12-amino acid peptide derived from thrombospondin type 1 (TSP1) repeat sequences from the subcommissural organ-spondin protein. TSPs are glycoproteins present in the extracellular matrix, mediating cell–cell and cell–matrix interactions and axon pathfinding. NX210c was previously shown to improve axonal regeneration and functional recovery in thoracic SCI. The aim of this study was to evaluate the ability of NX210c to promote functional recovery and tissue repair in a traumatic cervical SCI rat model. Adult female Wistar rats were subjected to a C6/C7 bilateral clip compression-contusion injury and treated once daily with intraperitoneal injections of NX210c (8 mg/kg) or its vehicle for 8 weeks, beginning 4 h or 8 h post-injury. Administration of NX210c beginning at 4 h post-injury increased forelimb grip strength post-injury and improved several static and dynamic aspects of locomotion, including interlimb coordination. When the first administration was undertaken at 8 h post-injury, NX210c promoted weight gain, improved trunk balance (inclined plane), trended toward accelerated bladder control recovery, and approached significance for skilled reaching at 8 weeks post-injury. Furthermore, for animals that were treated daily with NX210c starting 8 h post-injury, histological analysis demonstrated greater white and gray matter preservation and reduced cavity size, along with the upregulation of neuronal markers. To conclude, NX210c mitigates various aspects of SCI, including motor function and tissue preservation, with preferential results being obtained with the delayed initial administration of NX210c at 8 h post-injury.
Introduction
More than half of spinal cord injury (SCI) cases occur at the cervical level 1 and are often the most severe with the loss of upper extremity motor function, impaired trunk control, autonomic dysfunction, respiratory depression, and impaired bowel and urinary function. These injuries largely impact patients’ autonomy and quality of life, with an estimated lifetime cost of $1.5–3 million per person in Canada 2 accounting for medical costs and loss of productivity.
The initial physical trauma, resulting in compression and contusion of the spinal cord, is followed by the activation of secondary injury cascades within the central nervous system (CNS), characterized by inflammation, impaired blood–spinal cord barrier (BSCB) integrity, and activation of resident parenchymal cells (namely microglia and astrocytes) to reactive, proinflammatory phenotypes. In the chronic phase of the injury, an inhibitory perilesional scar forms with a fibrotic core composed of chondroitin sulfate proteoglycans, fibroblasts, and type A pericytes, along with a reactive astrocyte border, which provides a physical barrier to axonal regeneration. Overall, these secondary cascades result in impaired cellular regeneration and recovery following SCI.1,3
Despite advances in medical, surgical, and rehabilitation treatments for SCI, there are no currently approved neuroprotective or neuroregenerative pharmacological therapies that aid in locomotor recovery post-SCI, which represents a significant knowledge gap. 4 Although methylprednisolone sodium succinate (MPSS), a potent anti-inflammatory medication, is an option for acute SCI, concerns exist around the negative consequences of systemic immunosuppression. 5
NX210c is a chemically synthesized 12-amino acid cyclic peptide derived from type-1 thrombospondin repeat (TSR1) sequences from the subcommissural organ (SCO)-spondin protein. This protein is only present during early ontogenesis in humans but persists post-birth in other vertebrates. 6 It has been proposed to aid in vertebrate spinal cord regeneration.7–9 SCO-spondin is secreted into the cerebrospinal fluid during development and aggregates to form Reissner fibers, which are key to the morphological linear development of the spine. 10 Thrombospondins (TSPs) are glycoproteins present in the extracellular matrix (ECM), mediating cell–cell and cell–matrix interactions and axon pathfinding,11,12 and are involved in various processes such as angiogenesis and inflammation. 13 Therefore, TSPs are thought to be helpful following injury to enhance endogenous regeneration and the recovery of lost neural networks. Accordingly, NX210c was previously shown to improve axonal regeneration and functional recovery in rat models of thoracic SCI. 14 Mechanistically, NX210c triggers neuroprotection via integrins containing the β1 subunit, 15 which are present in various cells in the CNS. Importantly, NX210c was shown to be safe in healthy volunteers. 16 Based on these works, the goal of this study was to determine the neuroprotective impact of NX210c in a clinically relevant bilateral compression-contusion model of traumatic cervical SCI. Here, we report novel evidence that NX210c enhances functional recovery and promotes tissue sparing after cervical SCI in rats.
Materials and Methods
The study protocol and timelines are illustrated in Figure 1.
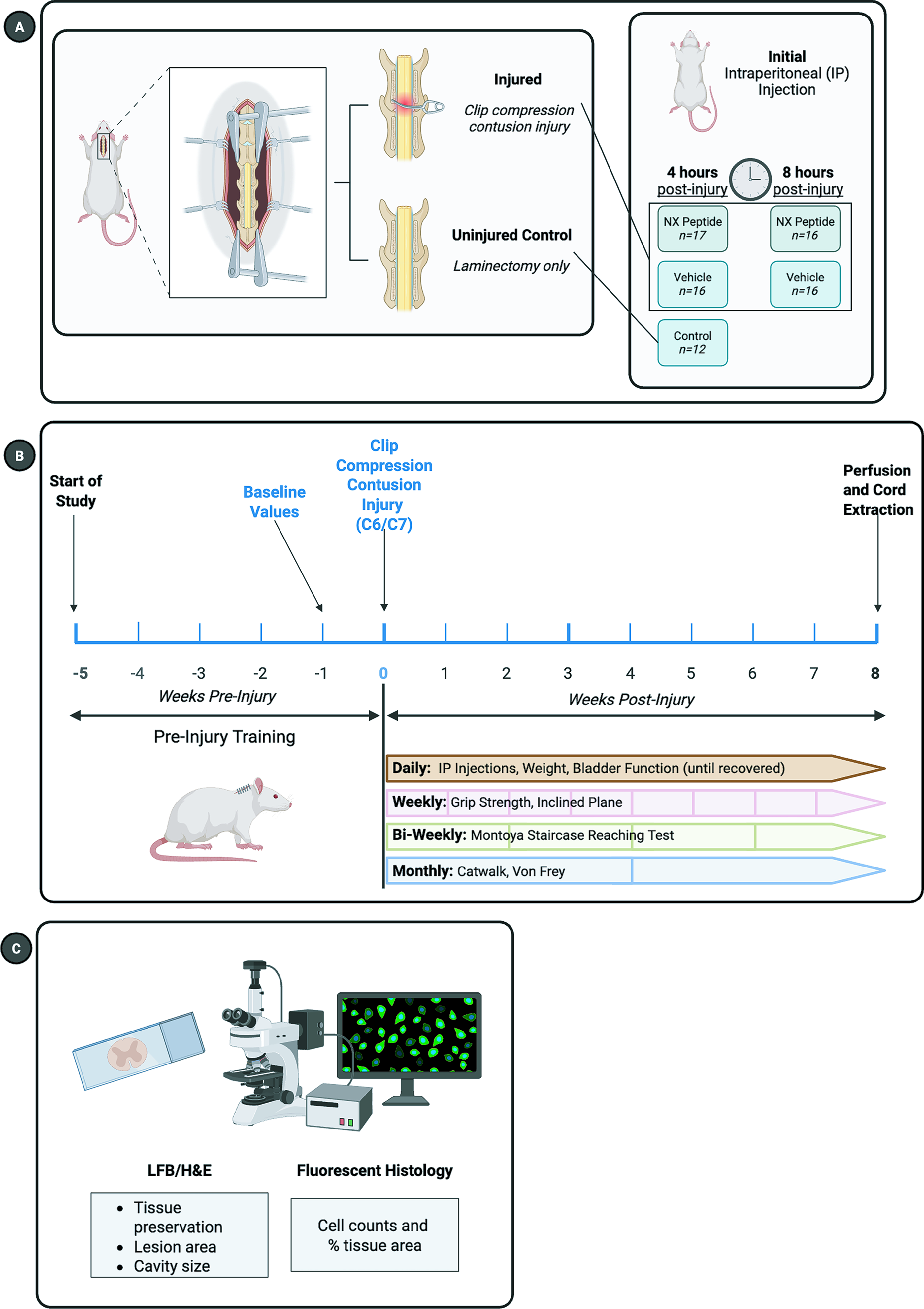
Study experimental design.
NX210c peptide synthesis
NX210c is the oxidized cyclic form of a linear dodecapeptide derived from the most conserved TSR1 consensus sequence of the SCO-spondin protein. The NX210c sequence is H-WSGWSS[CSRSC]G-OH; the brackets represent the disulfide bond between cysteine residues. It was manufactured by GENEPEP (Saint Jean-de-Védas, France) and supplied as an acetate salt lyophilizate, whose purity was assessed as 96% using high-performance liquid chromatography. NX210c was dissolved in sterile water for injection (WFI; DIN 02014882, Baxter, Deerfield, IL, USA) and stored at −80°C for up to 3 weeks. Aliquots were thawed to room temperature prior to injection.
SCI model
This study was conducted in accordance with the University Health Network Animal Resource Centre (ARC) Ethics Committee (Animal Use Protocol [AUP]: #2212). Sixty-five adult female Wistar rats obtained from Envigo (Indianapolis, IN, USA) with a minimum weight pre-surgery of 200 g were subjected to a C6/C7 clip compression-contusion injury (23.5-g clip) for 1 min to model compression-contusion crush injuries characteristic of incomplete traumatic cervical SCI in humans.17,18 Female rats were selected due to the high incidence of urinary tract infection-related complications and difficulties in manual bladder expression in male rat models of cervical SCI. 19 SCI rats were treated with intraperitoneal (IP) injections of NX210c (8 mg/kg) or its vehicle (sterile water for injection), with the first administration 4 h or 8 h post-injury (n = 16–17/group) and then once daily for 8 weeks. NX210c has been tested in other models and studies20–22 and the dose used (i.e., 8 mg/kg) was selected based on a previous preclinical study using the linear form of the peptide in a mouse thoracic model of SCI. 23 Uninjured control rats (n = 12) received a laminectomy surgery with first vehicle administration at 4 h post-injury. For 3 days post-surgery, twice daily, rats received buprenorphine, an analgesic agent, subcutaneously (12 µg in 1 mL; DIN 02531143, Champion Alstoe Animal Health, Whitby, ON, Canada). Meloxicam, a non-steroidal anti-inflammatory drug, was given subcutaneously (0.25 mg in 1 mL; DIN 02240463, Boehringer Ingelheim, Burlington, ON, Canada) once per day for 5 days post-injury. Clavamox®, an antibiotic agent, was added to the drinking water 3 days preoperatively and continued postoperatively for the duration of the study (2 mL reconstituted in 250 mL of sterile autoclaved water; DIN 01916874, GlaxoSmithKline Inc., Mississauga, ON, Canada). This study was double-blinded and randomized for group allocation and drug administration. Rats were allocated to groups using a random number generator (www.randomizer.com). The drug was prepared, and the tubes for the drug and vehicle were assigned letter codes blinded to those conducting surgeries, administering the drug, and performing the neurobehavioral tests. Daily IP injections were conducted by blinded ARC technicians.
Neurobehavioral tests and functional measures
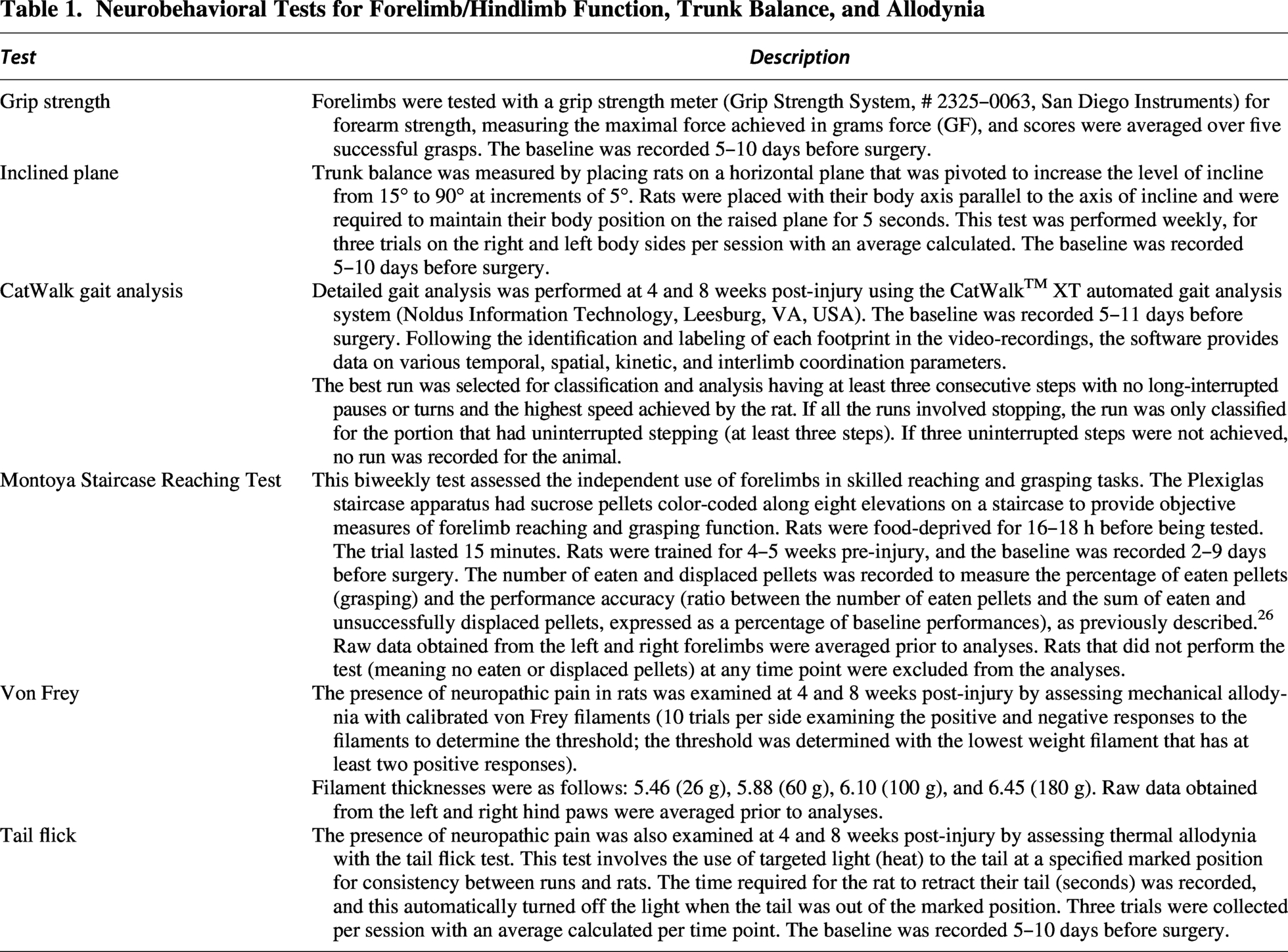
Various neurobehavioral tests were conducted to assess forelimb and hindlimb mobility, trunk balance, gait, skilled reaching, as well as thermal and mechanical allodynia, as previously described.24,25 These specific tests are explained in Table 1, and the frequency of each test is illustrated in Figure 1. Weight gain and recovery of spontaneous bladder function were tracked daily per animal. The need for bladder voiding was checked daily using the Credé maneuver (manual expression of the bladder) as an indicator of the recovery of the micturition reflex. Once rats had 3 consecutive days with no need for manual bladder expression, the number of days post-injury was recorded.
Neurobehavioral Tests for Forelimb/Hindlimb Function, Trunk Balance, and Allodynia
Tissue processing and cryosectioning
At 8 weeks post-injury, transcardial perfusions were conducted. Rats were placed under 5% isoflurane (Fresenius Kabi, Bad Homburg, Germany), starting with 1× phosphate-buffered saline (PBS) at 4°C (10× stock; 311–012-CL Wisent, Saint-Jean-Baptiste, QC, Canada; 60 mL/min), followed by 4% paraformaldehyde (PFA; PAR070.1, BioShop, Burlington, ON, Canada) in 1× PBS (4°C; 60 mL/min), and the spinal cord was extracted ±0.5 cm on either side of the injury site via laminectomy to be used for histology. 27 Higher cervical, thoracic, and lumbar segments were also extracted via laminectomy.
Following perfusion, the cord was placed in a solution of 10% sucrose (SUC507.5, BioShop) in 4% PFA for 6 h. The cords were then rinsed with 1× PBS and transferred to sequential gradients of sucrose (20% once, 25% once, and 30% twice) in 1× PBS to allow the cord to equilibrate to the cryoprotectant solution. Sections were embedded in M-1 Embedding Matrix (Epredia™ SH1310, Fisher Scientific, Waltham, MA, USA). The cords were sectioned at 30-µm thickness on Leica CM3050 (Leica Microsystems Canada, Concord, ON, Canada) onto frosted slides (Fisherbrand™ Superfrost™ Plus Microscope Slides, 1255015, Fisher Scientific). Cord sections were stored at −80°C until use.
Histology
Myelin (Luxol Fast Blue/Solvent Blue 38; S-3382, Sigma-Aldrich, St. Louis, MI, USA), cell nuclei (hematoxylin, 51275, Sigma-Aldrich), and ECM/cytoplasm (eosin, eosin Y disodium salt, E4382, Sigma-Aldrich) (luxol fast blue, hematoxylin, and eosin [LFB/H&E]) colorimetric stains were conducted,28,29 with n = 6/group with five slides per animal (epicenter, ±480 µm, ±960 µm) and distances selected based on previous work demonstrating group differences observed within ±960 µm from the epicenter. 30 The cords were imaged using Nikon Eclipse E800 (Minato-ku, Tokyo, Japan) with a motorized platform, and stitched full tissue brightfield images were collected using Stereo Investigator (MBF Bioscience, Williston, VT, USA). 28 Fiji software (National Institutes of Health, Bethesda, MD, USA) was used to determine the gray matter, white matter, lesion tissue, and cavity area as a percentage of the total tissue area.
Immunofluorescence
Six animals per group, with three slides per animal, near the injury epicenter and ±1920 µm rostral and caudal, were stained with the following markers: neurons (NeuN, β3-tubulin, NF200), synapses (synaptophysin), oligodendrocytes (Olig2), astrocytes (glial fibrillary acidic protein [GFAP]), apoptosis (In Situ Cell Death Detection Kit, TUNEL), perilesional scar (CS-56), microglia (Iba-1), and cell proliferation (Ki-67). Most antibodies were diluted in standard milk block (5% skim milk powder, SKI400, BioShop), 1% bovine serum albumin (bovine serum albumin fraction V; ALB001, BioShop), and 0.3% Triton (Triton X-100; 78787, Sigma-Aldrich), all in 1× PBS. Other antibodies were diluted in serum block (2% or 5% goat serum, Gibco 16210-064, Fisher Scientific) and 0.3% Triton in 1× PBS based on optimization protocols. Primary antibodies were incubated overnight at 4°C. Secondary antibodies were incubated for 1–2 h at room temperature. Sudan Black B (SUD535.25, BioShop; 0.05% in 70% ethanol) was used as a quenching agent for select antibodies to reduce background noise. TUNEL was conducted based on the instructions provided in the kit. The cords sectioned were stained with these markers and counterstained with 4ʹ,6-diamidino-2-phenylindole, dilactate (DAPI; D3571, Fisher Scientific) at a concentration of 1:500 to examine the effect of NX210c on the cell distribution and tissue surrounding the injury along with a comparison of the two initial injection time points. Antibodies and concentrations are shown in Table 2. Full cord axial sections were imaged with Nikon Eclipse Ti (Nikon Instruments, Melville, NY, USA) using epifluorescence (QImaging driver; Retiga 2000R Mono camera) at 20× objective, with the quantification conducted using a custom ImageJ script employing cell counting counterstaining with DAPI or % area/intensity depending on the nature of the cell marker. All fluorescent markers were normalized to the uninjured controls, allowing for comparisons between the NX210c and corresponding vehicle groups at each distance from the injury epicenter.
Primary and Secondary Antibody Concentrations for Fluorescent Immunohistochemistry
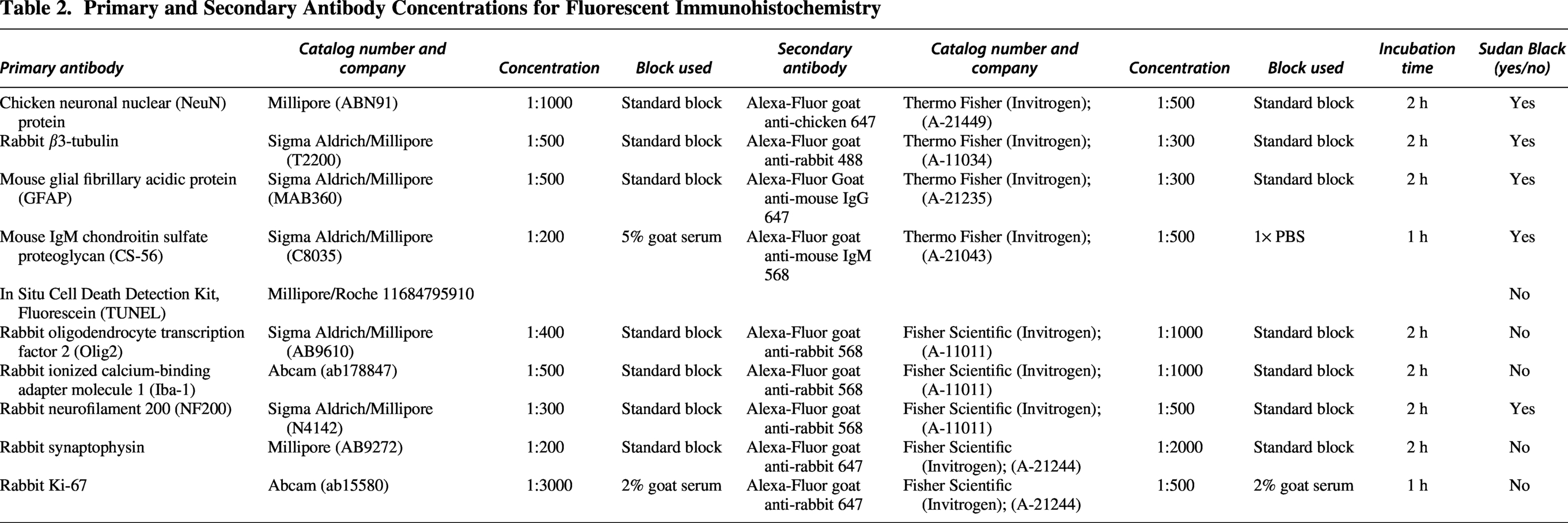
Image processing
Fluorescence of the full tissue sections was analyzed. Depending on the marker, counts or percentage positive fluorescent areas (of the total tissue area) were assessed. Images were converted from their native Nikon format (.nd2) to 8-bit multichannel .tiffs using the Bio-Formats reading plugin in Fiji. The images were then converted to 8-bit using the native 8-bit function and split using the Split Channels function into their respective channels. For all counts, noisier images (Iba1) were taken through a background removal procedure, where the images were processed using the Gaussian Blur function (s = 2) and then multiplied unto their respective originals using the native Image Calculator function. For cell counting, the Median Blur function (radius = 2) was used to smoothen multifoci cells, and the Find Maxima function (prominence = 40–60, output = count) was used to count cells. For the percent positive area, images were first thresholded (greyscale value = 70–90) and the area fraction measured with the measure function.
Statistical analyses
Statistical analyses were performed with GraphPad Prism software package 10.1.1 (GraphPad Software, La Jolla, CA, USA). For CatWalk gait analysis, a mixed effects model was used, as some animals had missing values (at one or both times) depending on their ability to sustain at least three consecutive steps. For all other neurobehavioral tests, a repeated measures two-way analysis of variance (ANOVA) followed by post hoc uncorrected Fisher’s least significant difference (LSD) was used. For colorimetric histology and immunofluorescence, a two-way ANOVA was used, followed by post hoc uncorrected Fisher’s LSD. Post hoc Fisher’s LSD was used for comparison of no more than three groups (NX210c, corresponding vehicle, and uninjured control), as used in the study by Mironets et al. (2018). 31 Bladder recovery was analyzed using Student’s t-test. Comparison of mortality between the groups was assessed using the Fisher’s exact test. A p value of < 0.05 was considered significant in all statistical tests. All values are depicted as mean ± standard error of the mean (SEM).
Results
Neurobehavioral tests and functional measures
Baseline (pre-injury)
To ensure no bias in baseline randomization between the experimental groups, we measured baseline grip strength and inclined plane. Grip strength (Supplementary Fig. S1A [left panel]: F(4,74) = 0.09755; p = 0.98) and inclined plane (Supplementary Fig. S1A [right panel]: F(4,72) = 1.136; p = 0.35) showed no significant differences between the experimental groups.
Qualitative observations and survival post-injury
Thirty-one rats died or were euthanized during the course of the study, with 20 rats dying over the course of the study post-surgery, three rats being euthanized due to surgical complications, two due to injection complications, and six due to a humane end-point (i.e., labored breathing and weight loss). Finally, 77 rats were alive at the completion of the study, with n = 16/17 rats per treatment/vehicle group and n = 12 for uninjured control animals. This is illustrated in Figure 2, along with a further breakdown of mortality per group. Fisher’s exact test comparing mortality between the SCI treatment and vehicle groups without human error (i.e., death post-surgery and death due to a humane end-point) and survival (n = 16–17 per group) found no significant difference between the groups (p = 0.8).
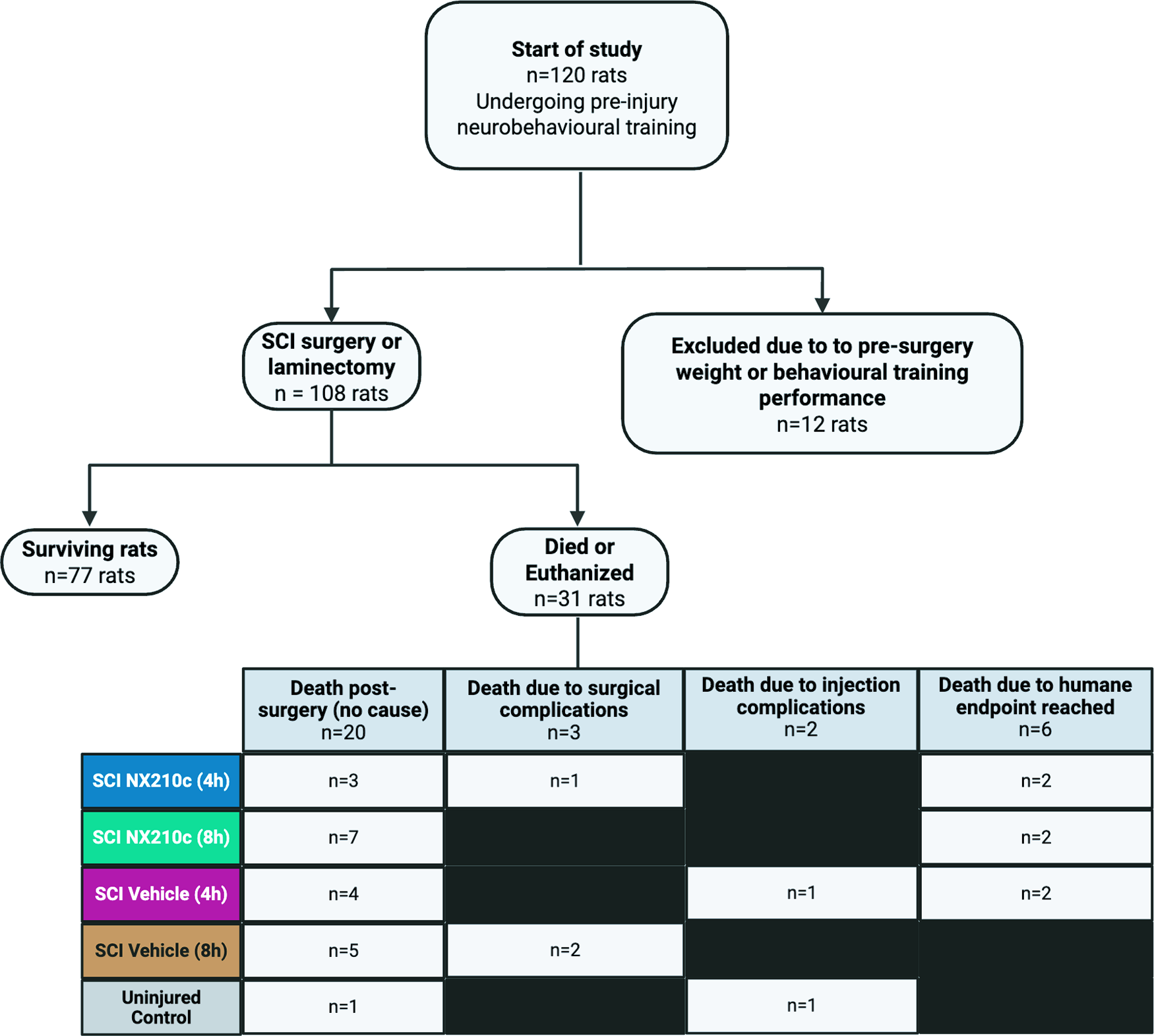
Flowchart of survival numbers. A total of 120 rats began initial pre-injury behavioral training in the study, with 108 rats undergoing surgery. Thirty-one rats died or were euthanized post-surgery, with select rats dying due to surgical complications, injection complications, or reaching the humane end-point. The mortality per treatment and vehicle group has been illustrated. Seventy-seven rats survived until the end of the study. Created in https://BioRender.com.
Directly following the C6/C7 level injury, rats had markedly limited mobility and minimal hindlimb weight support. Range of motion and grip strength of the forelimbs were lower, with some animals having unilateral or bilateral clubbed fists.
Neurobehavioral tests
Four-hour post-injury groups
The NX210c group with initial administration at 4 h post-injury had significantly increased forelimb grip strength at 3, 4, 7, and 8 weeks post-injury (Fig. 3A [left panel]: F(16,336) = 22.16; p = 0.04, 0.02, 0.03, and 0.01, respectively) and improved several static and dynamic aspects of locomotion as measured using Catwalk, including regularity index at 8 weeks post-injury (Fig. 3D [left panel]: F(4,70) = 20.84; p = 0.03) when compared with the corresponding vehicle group. Supplementary Figure S2 illustrates the additional significant CatWalk parameters, with the graphical depiction of important parameters.
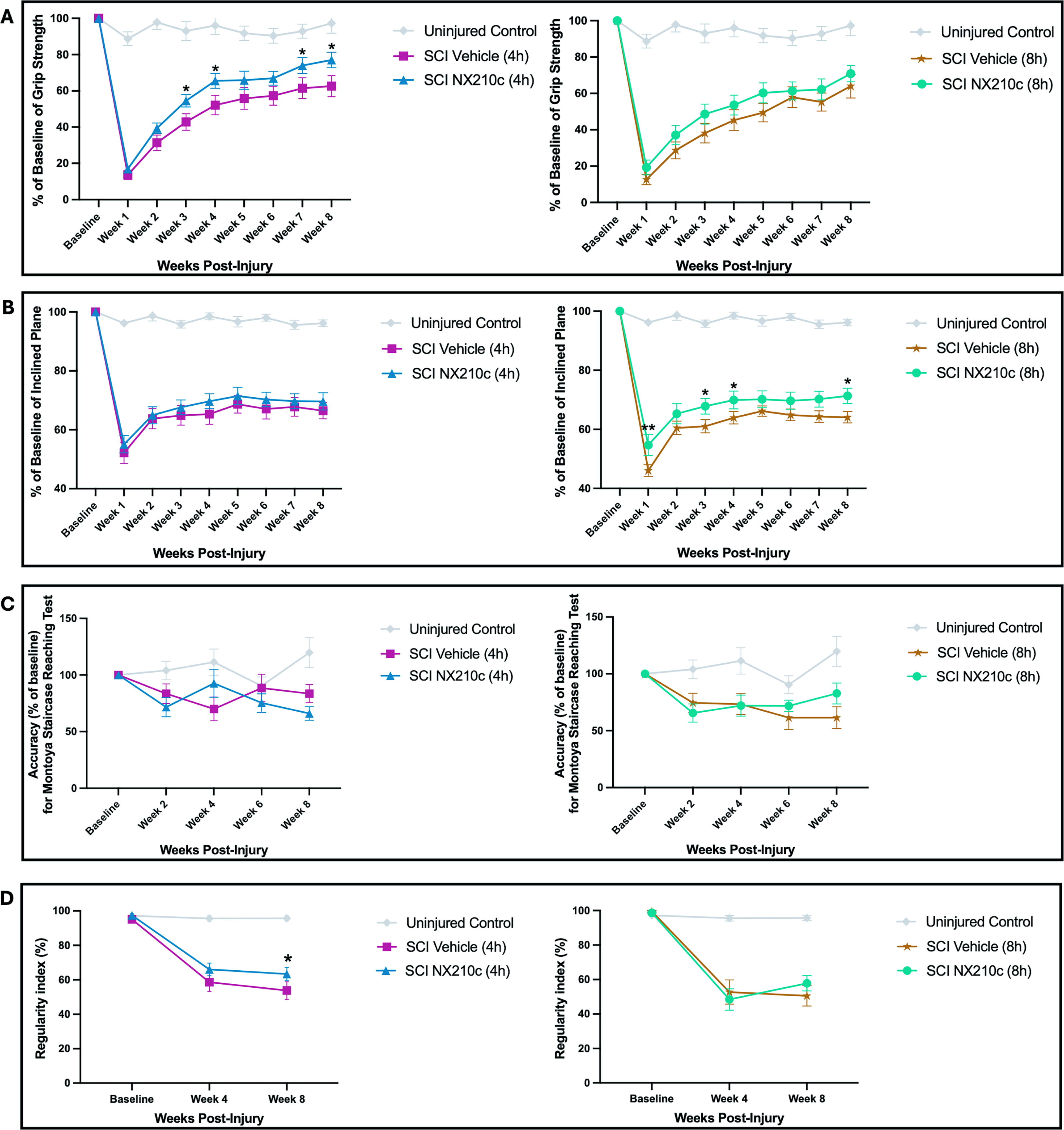
Early and delayed initial administration followed by daily systemic administration of NX210c promotes locomotor recovery, trunk balance, and forelimb function after cervical SCI in rats. Neurobehaviour tests of grip strength
Eight-hour post-injury groups
When compared with the vehicle, the initial administration of NX210c beginning at 8 h post-injury resulted in significant improvements in trunk balance (inclined plane) at 1, 3, 4, and 8 weeks post-injury (Fig. 3B [right panel]: F(16,328) = 31.63; p = 0.005, 0.03, 0.05, and 0.02, respectively). When examining skilled forelimb reaching with the Montoya Staircase Reaching Test (successfully grasped and ate pellets compared with baseline), this approached significance at 8 weeks post-injury (Fig. 3C [right panel]: F(8,148) = 2.926; p = 0.058). Animals overall were healthy, with significantly improved weight gain maintained for weeks 2–8 post-injury (Fig. 4A [right panel]: F(16,328) = 19.61; p = 0.04, 0.007, 0.03, 0.006, 0.001, 0.03, and 0.03, respectively).
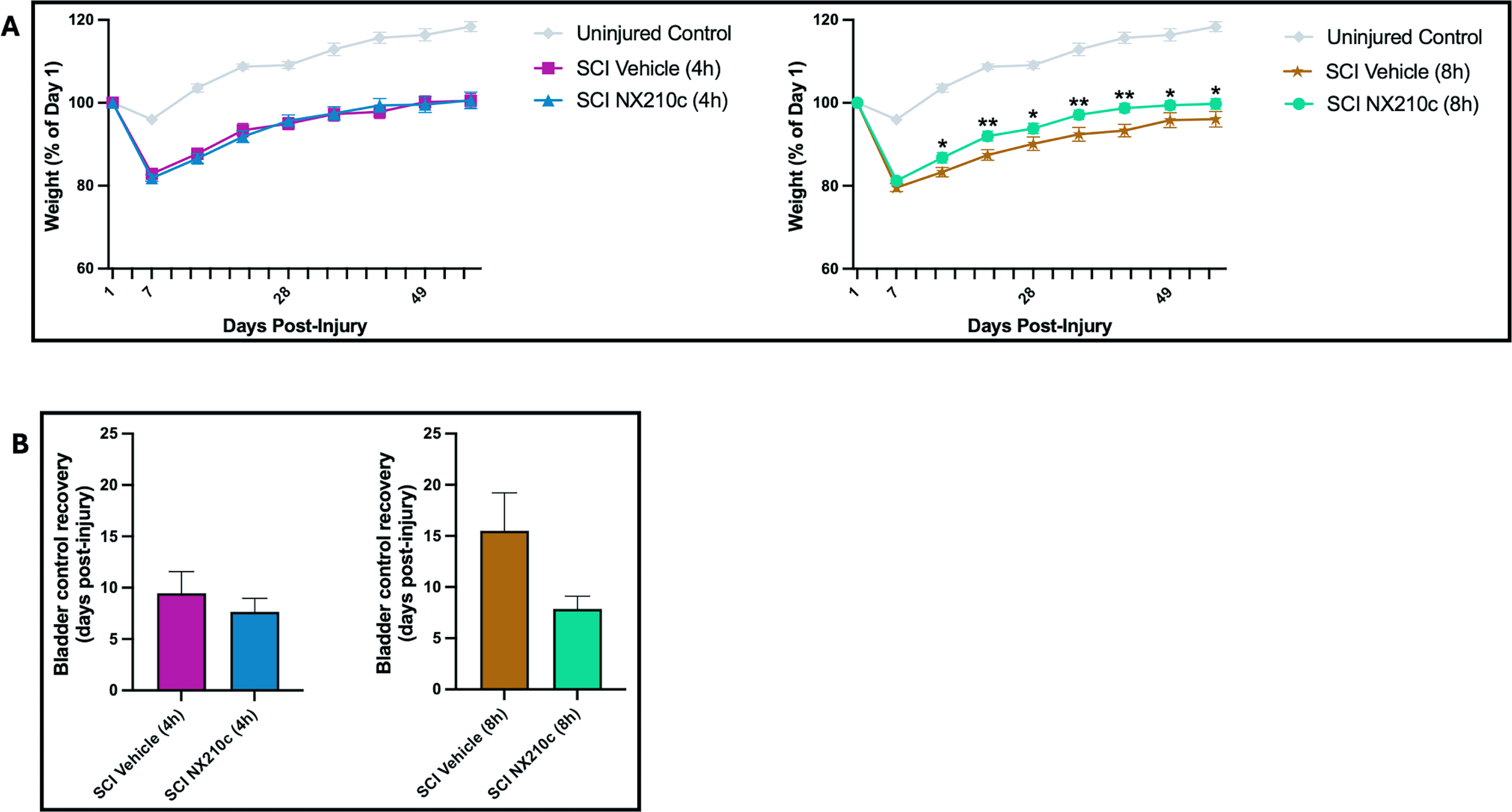
Early and delayed initial administration followed by daily systemic administration of NX210c promotes weight gain and trends toward bladder recovery after cervical SCI in rats. NX210c-treated groups with administration beginning at 4 h (left panels) and 8 h post-injury (right panels), and their corresponding vehicle, are shown. Statistically significant differences were observed between NX210c administered starting at 8 h and vehicle for weight gain
Recovery of spontaneous bladder voiding
Comparison of spontaneous bladder recovery between NX210c administered beginning at 4 h or 8 h post-injury did not show statistical significance when compared with the corresponding vehicle groups. However, restoration of bladder function trended toward quicker recovery in the group receiving injections beginning 8 h post-injury, with an improvement of 49% in the NX210c group relative to the vehicle group (Fig. 4B [right panel]: p = 0.07). This compares to a 20% quicker restoration of bladder function in the 4 h initial administration of NX210c group compared with the vehicle group, although not statistically significant (Fig. 4B [left panel]: p = 0.4). There was also no statistically significant difference observed between the two vehicle groups (p = 0.2).
Neuropathic pain
No statistically significant differences in tail flick (thermal allodynia; Supplementary Fig. S1B) were observed when comparing NX210c initial administration at 4 h post-injury (F(4,84) = 1.889; p = 0.3 at 4 weeks and p = 0.9 at 8 weeks) and 8 h post-injury (F(4,82) = 0.5163; p = 0.1 at 4 weeks and p = 0.8 at 8 weeks) with their corresponding vehicle groups at all time points post-injury.
No statistically significant differences were observed in von Frey (mechanical allodynia; Supplementary Fig. S1C) when comparing NX210c first administration at 4 h post-injury (F(2,42) = 3.011; p = 0.6 at 4 weeks and p = 0.2 at 8 weeks) and 8 h post-injury (F(2,41) = 3.398; p = 0.7 at 4 weeks and p > 0.9 at 8 weeks) with their corresponding vehicle groups at all time points post-injury.
Histology
LFB/H&E was used to assess tissue preservation (gray and white matter), lesion tissue area, and cavity size as a proportion of the total tissue area. This can be observed visually using the representative tissue samples in Figure 5D.
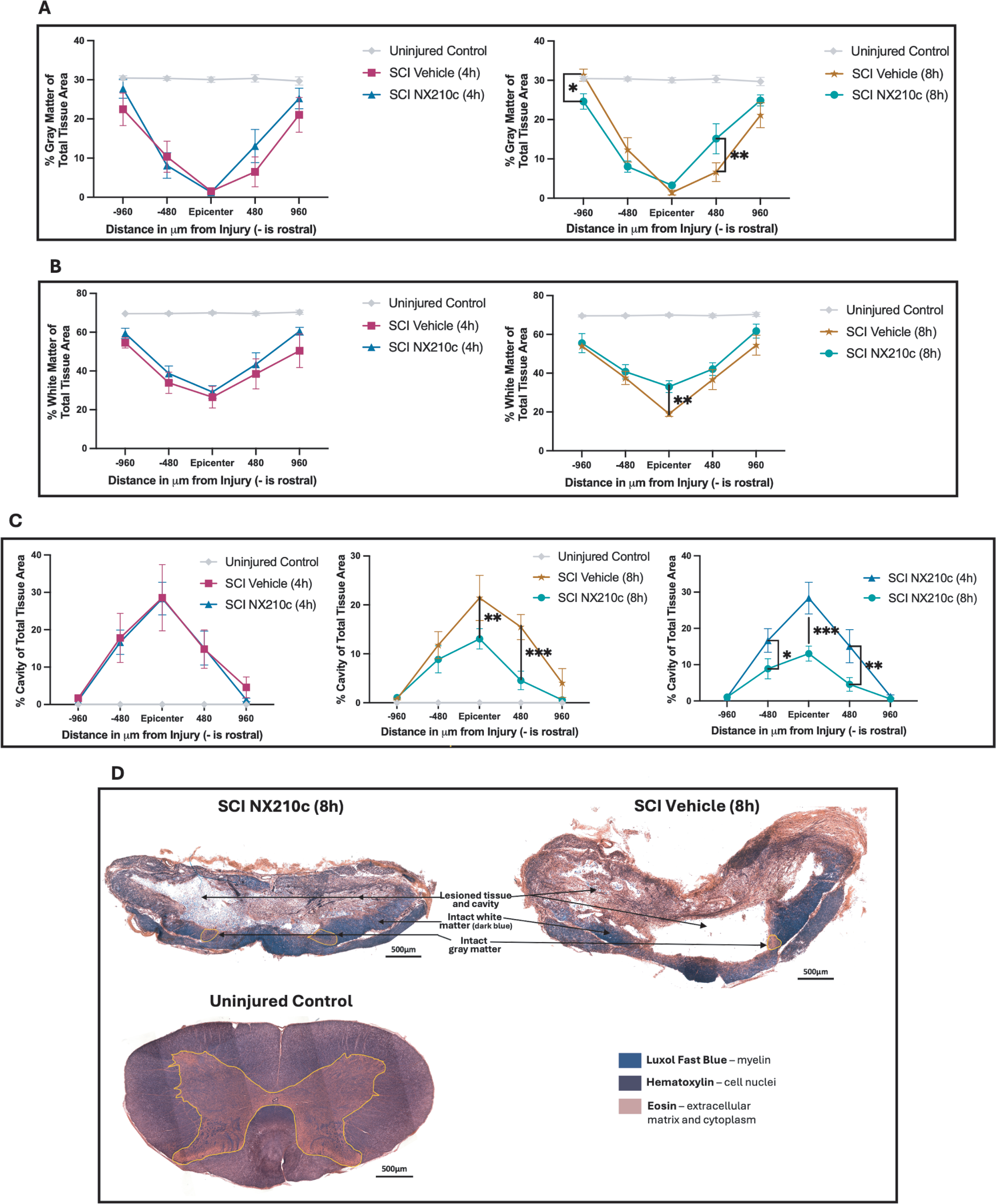
Delayed initial administration followed by daily systemic administration of NX210c promotes tissue preservation after cervical SCI in rats. No significant differences were observed between NX210c and vehicle for administration beginning at 4 h post-injury in terms of gray matter preservation (
Four-hour post-injury groups
For the 4 h initial injection group, no statistical significance was observed when comparing the NX210c and vehicle groups at all measured distances from the injury epicenter for white matter preservation (Fig. 5B
Eight-hour post-injury groups
Greater white matter preservation was observed in the NX210c treatment group compared with vehicle group, with statistical significance observed at the injury epicenter (Fig. 5B
Comparing 4- and 8-hour post-injury groups
Rats with NX210c initial administration beginning at 4 h had a larger cavity size compared with rats in the 8 h initial administration group. This was statistically significant at the injury epicenter (Fig. 5C
Fluorescent histology markers
Both groups
No statistically significant differences (p > 0.05) were observed in either the 4 h or 8 h NX210c group compared with their corresponding vehicle groups with tissue extracted at 8 weeks post-injury at all measured distances from the injury epicenter for CS-56 (4 h: F(2,30) = 0.8559; 8 h: F(2,30) = 0.2408), Iba-1 (4 h: F(2,30) = 0.01367; 8 h: F(2,30) = 0.1298), Olig2 (4 h: F(2,30) = 0.06678; 8 h: F(2,30) = 0.3741), GFAP (4 h: F(2,30) = 1,475; 8 h: F(2,30) = 0.1793), NF200 (4 h: F(2,30) = 0.1123; 8 h: F(2,30) = 0.4668), and Ki-67 (4 h: F(2,30) = 0.1467; 8 h: F (2,30) = 1.653). Graphs are illustrated in Supplementary Figure S3D. As tissue was solely extracted at the chronic injury time point (8 weeks post-injury) when the injury microenvironment would have achieved homeostasis, discernable differences in glial cells, apoptosis, and cell proliferation would need to be examined earlier in the acute/subacute phase.
Four-hour post-injury groups
For the 4 h post-injury initial injection group, no statistically significant differences were observed when comparing the NX210c and vehicle groups at all measured distances from the epicenter for all markers, except for TUNEL, whereby a statistically significant decrease was observed in the NX210c group compared with the corresponding vehicle group 1920 µm rostral to the injury epicenter (Supplementary Fig. S3D; F(2,30) = 4.050; p = 0.002).
Eight-hour post-injury groups
NeuN counts, β3-tubulin % area, and synaptophysin counts were upregulated across all measured distances from the injury epicenter when comparing the NX210c and vehicle groups with initial injection at 8 h post-injury. Normalized NeuN counts were statistically significant 1920 µm caudal to the injury site (Fig. 6A: F(2,30) = 0.9429; p = 0.02) when comparing the NX210c and corresponding vehicle groups (Fig. 6D). The normalized β3-tubulin % area threshold was statistically significant caudal to the injury site (Fig. 6B: F(2,30) = 1.737; p = 0.02) for the NX210c-treated group compared with the vehicle group (Fig. 6E). Lastly, normalized synaptophysin counts were increased at the injury epicenter (Fig. 6C: F(2,30) = 0.1213; p = 0.052) when comparing the NX210c and corresponding vehicle groups (Fig. 6F).
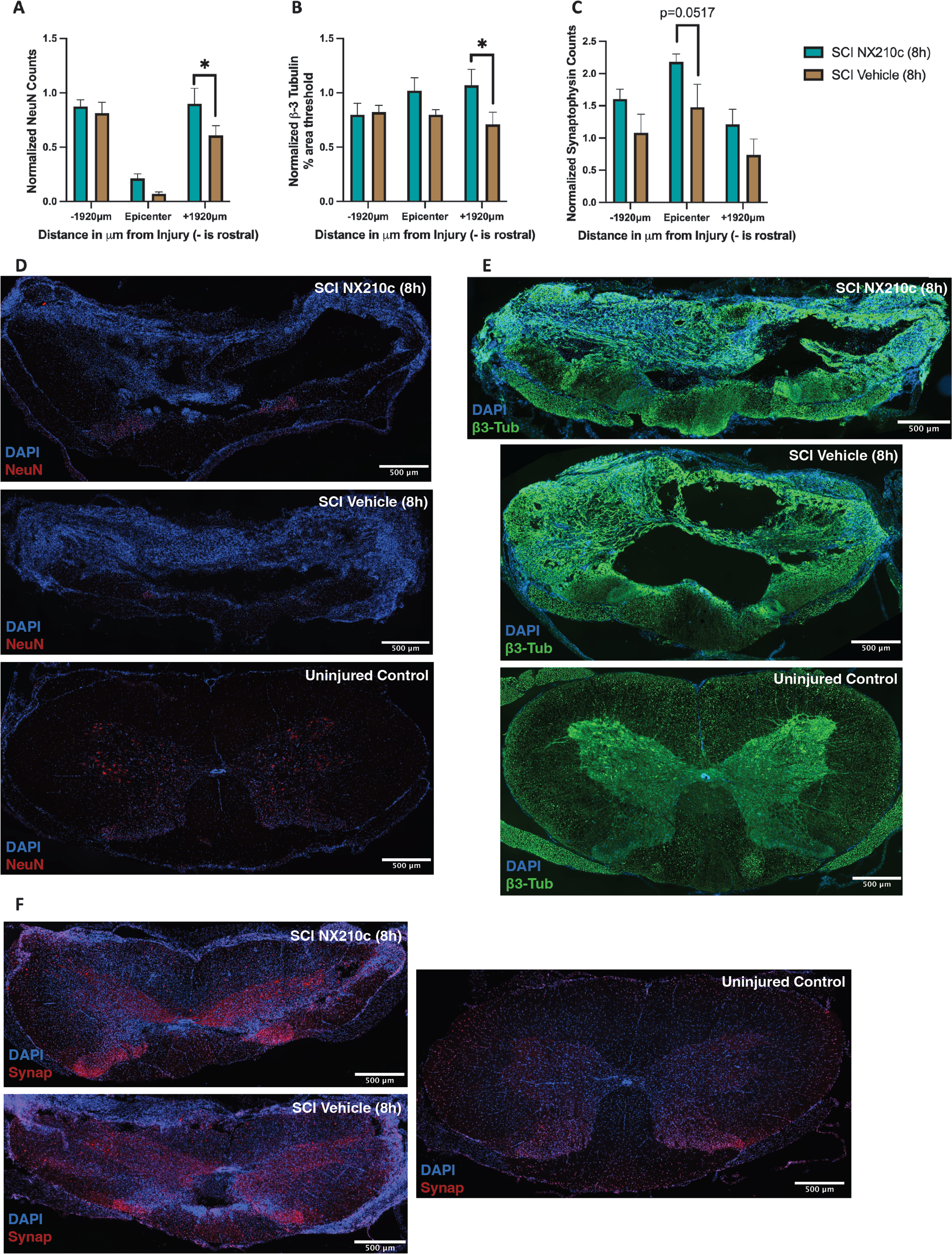
Delayed initial administration followed by daily systemic administration of NX210c is neuroprotective after cervical SCI in rats. Graphical depiction of NeuN
Discussion
Overall, NX210c appears to be neuroprotective in nature—resulting in improvements in gray and white matter tissue preservation, reduced cavity size, upregulation of neuronal markers, enhancements in motor function, and trended toward faster spontaneous bladder control, with preferential results being obtained with the 8 h initial administration of NX210c.
When combining histology with behavioral data, we observed modest improvements in functional recovery at both injection time points. However, at the 8 h initial injection time point, there was enhanced anatomical preservation and improvements that were not observed in the 4 h initial injection group, which also presented with a larger mean cavity size in comparison with the 8 h initial administration group. This suggests that delaying the initial injection of NX210c may provide the same benefit, if not better for certain parameters. Animals were also healthier considering functional measures that are important for clinical translation, such as weight gain.
Although no significant changes were observed in other cell types, such as microglia (Iba-1), astrocytes (GFAP), and oligodendrocytes (Olig2), this may be a result of the tissue having been extracted in the chronic phrase, whereby with consolidation of the perilesional scar, the injury microenvironment is devoid of immune cells. 3
There are currently no approved pharmacological therapeutics for SCI, 4 with the only available option being MPSS, which provides moderate benefits if administered within a narrow window of 8 h post-injury in humans but is linked to risks associated with the drug being a systemic immunosuppressant. 5 The current clinical guidelines generated by AO Spine recommend surgical decompression within 24 h of injury, preferentially at specialist trauma centers. 32 Despite this recommendation, less than 50% of cervical SCI cases meet this clinical recommendation.33,34 Treatment with NX210c would enable the administration of a neuroprotective drug within the critical first 24 h post-injury to attenuate the secondary injury response and potentially extend the window for decompressive surgery.
The current study demonstrates a neuroprotective role for NX210c, which results in improved locomotion, white matter and gray matter preservation, neuronal survival, and weight gain. The neuroprotective effect of NX210c may be mediated through several molecular pathways and mechanisms, and further work is required to determine the mechanism of action of this peptide in the acute phase of SCI.
PI3K-Akt-mediated neuroprotection
NX210c has also been previously shown to trigger its effect through β1-integrin receptors, 15 which are present in various cells in the CNS. The PI3K/Akt pathway is involved in the transcription of genes regulating cell survival and neuronal growth. Following SCI, the expression of PI3K and Akt gradually decreases. 35 Activation of this pathway may reduce apoptosis and promote cell regeneration and survival.15,35,36 In rat and human cortical primary neuronal cultures, treatment with NX210c helped enhance neuronal survival under excitotoxic conditions, reducing cell death and the expression of pro-apoptotic factors. 15 Administration of an anti-β1 integrin antibody also prevented NX210c-mediated neuronal survival. Furthermore, inhibitors of γ-secretase, PI3K, and p7056K, key factors in the PI3K/Akt pathway, made cells unresponsive to NX210c, blocking the corresponding neuroprotective benefits. 15 Examining this potential mechanistic pathway in vivo in the context of the acute excitotoxic SCI post-injury environment will be important for understanding the neuroprotective properties of NX210c.
Astrocyte-mediated synaptogenesis
With tissue extracted in the chronic phase post-SCI, NX210c administration resulted in the upregulation of the synaptophysin marker. TSP1 specifically has been implicated in astrocyte-mediated synaptogenesis. During development, TSP1, as secreted by astrocytes, promotes the formation of excitatory synapses and axonal sprouting through interacting with neuronal calcium receptors and activating transforming growth factor-β1.13,37 STAT3 activation has also been shown to mediate the upregulation of astrocytic TSP1 to promote excitatory synaptogenesis following an axonal injury. 38 In the acute phase, following the administration of NX210c, it will be essential to determine its impact on reactive astrocyte mobilization, axon formation, and STAT3 levels.
Matrix metalloproteinases and BSCB permeability
Matrix metalloproteinase-9 (MMP-9) and MMP-12 are upregulated following SCI.39–41 Within the first 24 h post-injury, the reduced integrity of the BSCB is associated with peripheral neutrophil infiltration. 40 MMP-9 is released by these infiltrating neutrophils and further disrupts BSCB integrity by targeting tight junction protein expression. 40 MMP-12 has also been associated with reduced BSCB integrity. 39 Studies have shown that TSP1 knockout and inhibitors result in reduced MMP-9 activation, thereby enhancing BSCB integrity and decreasing vascular endothelial growth factor expression, thus inhibiting angiogenesis.13,40 With the derivation of NX210c from TSP1, it is expected that NX210c reduces the levels of MMP-9, improving BSCB integrity and reducing aberrant angiogenesis and the associated hemorrhagic ischemia common in cervical-level traumatic SCI. This would be in line with recent work showing that NX210c stabilized mouse and human blood–brain barriers in several settings in vitro and in in vivo mouse models of aging. 22
Microglial activation
In injury microenvironments, knockout of TSP1 has been shown to increase the migration of microglia with a proinflammatory phenotype, as demonstrated by the increased expression of tumor necrosis factor alpha and nitric oxide. 42 TSP1 has also been involved in the modulation of monocyte aggregation mediated by CD36 and CD47. 13 It will be important to examine the role of NX210c in modulating microglial activity, as well as the levels of pro-inflammatory and anti-inflammatory chemokines and cytokines in an acute injury. It is expected that administering NX210c will help to shift the inflammatory profile of microglia toward a more anti-inflammatory phenotype and reduce the levels of circulating pro-inflammatory cytokines within the acute phase of an injury.
Clinical relevance and translation
This study has been undertaken in a translationally relevant model of moderate–severe cervical traumatic SCI, strengthening the results obtained in this preclinical dataset. Supplementary Figure S4 illustrates representative statistically significant behavioral and histological data with 95% confidence intervals when comparing NX210c initial administration at 8 h post-injury with its corresponding vehicle. Significant changes in behavior at 8 weeks post-injury (Supplementary Fig. S4A
At present, the only pharmacological therapeutic available for SCI is MPSS, which remains controversial. 5 Thus, NX210c administered in the acute phase of injury shows promise as an alternate neuroprotective pharmacotherapy for cervical traumatic SCI.
The hope for this drug is to move it toward being an Investigational New Drug with the Food and Drug Administration. This would be followed by confirmation of the mechanism of NX210c in subsequent studies, in the context of acute cervical SCI, as mentioned in earlier sections of the discussion. Finally, the locomotor and neuroprotective potential of NX210c would need to be validated in early-stage clinical trials for acute cervical traumatic SCI.
Conclusions
Overall, we report that NX210c provides preferential neuroprotective effects when administered beginning at 8 h post-injury, a time point that can attenuate the secondary injury response of SCI. 43 The current study demonstrates that the neuroprotective effect of NX210c results in enhanced motor function, white matter preservation, and correlates with the upregulation of neuronal markers. Elucidating the neuroprotective mechanisms of NX210c will determine how the secondary injury response is attenuated and indicate the optimal time for the administration of the peptide within the critical 24 h time window following injury that can extend the time frame for decompressive surgery. We anticipate that this study will provide a strong proof of concept for the use of NX210c as a treatment for acute cervical SCI patients.
Transparency, Rigor, and Reproducibility Summary
All statistical analyses were performed using GraphPad Software Prism 10.1.1, and differences were considered significant with a p value of < 0.05. Two-way ANOVA followed by uncorrected Fisher’s LSD test was conducted for neurobehavioral tests, colorimetric histology, and immunofluorescence. Bladder recovery was analyzed using Student’s t-test. Sample sizes were determined based on power analyses conducted using R Studio version 4.1, desiring at least 80% power. In total, 108 of 120 rats were operated on, with 12 rats excluded prior to surgery due to low performance during behavioral training or not achieving the minimum weight of 200 g for surgery. Thirty-one rats died or were euthanized during the study, due to surgical and injection complications or humane endpoints. Rats were randomly assigned using a random number generator to receive sham laminectomy (n = 12) or C6/C7 clip compression-contusion SCI (n = 16–17 per group) surgery. SCI rats were randomly assigned to receive NX210c or vehicle beginning 4 h or 8 h post-injury and continued daily for 8 weeks. NX210c was obtained as an acetate salt lyophilizate, whose purity was assessed as 96% using high-performance liquid chromatography. NX210c was dissolved in sterile water for injection and stored at −80°C for 3 weeks at a time and thawed prior to use. All animals treated with the drug received NX210c prepared from the same batch. Sham rats received vehicle treatment beginning at 4 h post-injury. This study was double blinded and randomized for group allocation and drug administration. The drug was prepared and the tubes for drug and vehicle were assigned letter codes blinded to those conducting surgeries, administering drug, and performing the neurobehavioral tests. Perfused spinal cord tissue was held at −80°C until being used for histological analysis. Animals were assessed over two behavioral cohorts, with tissue examined in one batch. Additional details of n, statistical tests, and results of statistical comparisons can be found in the results and figure legends. The surgical procedure and functional neurobehavioral outcome measures are standard in the field.
Authors’ Contributions
N.P.: Writing—original draft (lead); running experiments (lead); formal analysis (lead); writing—review and editing (lead); conceptualization (supporting). S.L.: Writing—review and editing (supporting); conceptualization (equal); formal analysis (supporting). S.A.: Running experiments (supporting). J.C.T.C.: Running experiments (supporting); conceptualization (supporting). J.H.: Formal analysis (supporting). J.W.: Running experiments (supporting). Y.G.: Conceptualization (equal); writing—review and editing (supporting). M.G.F.: Conceptualization (equal); writing—review and editing (supporting).
Footnotes
Author Disclosure Statement
S.L. is employed by Axoltis Pharma and is Chief Scientific Officer of the company. Y.G. is the President of Godfrin Life-Sciences, giving advice to Axoltis Pharma, and is also the Chief Executive Officer and a shareholder of Axoltis Pharma.
Funding Information
This study was fully funded by Axoltis Pharma to Michael Fehlings’ laboratory, under a master service agreement.
Data Availability
The data that support the findings of this study are available from the corresponding author, M.G.F. (michael.fehlings@uhn.ca), upon reasonable request.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.