
Abstract
Patients with disorders of consciousness (DoC) resulting from severe traumatic brain injury (TBI) may recover consciousness and independence years later. There is a prevailing belief that recovery, when limited to the restoration of independence in activities of daily living, will be accompanied by poor self-reported quality of life (QOL) and psychological health. This perception may influence early clinical decision-making related to the provision of life-sustaining treatment and access to specialized rehabilitation. In this observational study, we utilized data from the multisite TBI Model Systems (TBIMS) to evaluate the outcomes of QOL (Satisfaction With Life Scale [SWLS]), anxiety (Generalized Anxiety Disorder-7 Scale [GAD-7]), and depression (Patient Health Questionnaire-9 [PHQ-9]) in participants who were admitted to inpatient rehabilitation with DoC and recovered the ability to provide self-report on these measures by 1 year post-TBI. Among 887 TBIMS participants admitted to inpatient rehabilitation with DoC (defined as the absence of command-following; 74% male; mean [standard deviation, SD] age = 36.82 [17.87] years; days post-injury on rehabilitation admission = 33.63 [22.51]), 50% regained the capacity to respond to questions on self-report measures at the 1-year follow-up time point. The mean (SD) total scores were as follows: SWLS = 20.38 (7.81), GAD-7 = 4.00 (5.66), and PHQ-9 = 5.22 (5.04). A minority of patients endorsed dissatisfaction (15%) or extreme dissatisfaction (9%) with life, and similarly, only 14% and 16%, respectively, reported anxiety and depression symptoms above the clinical cutoff points. The results were similar at the 2- and 5-year follow-up time points. In summary, at the group level, QOL and psychological health in persons who recover from DoC are similar to those of individuals with less severe brain injuries and to the general population. These findings challenge the assumption that recovery from DoC is associated with poor QOL and psychological health. Clinicians should be aware that patients with a broad range of residual disability after DoC are unlikely to report dissatisfaction with life or have significant anxiety and depression up to 5 years post-TBI.
Keywords
Introduction
Persons who sustain severe traumatic brain injury (TBI) often experience disorders of consciousness (DoC)1–3 characterized by impaired arousal and awareness that persist for days to years. DoC phenotypes include coma (absence of both wakefulness and awareness), vegetative state/unresponsive wakefulness syndrome (evidence of sleep/wake cycles but no evidence of awareness), and minimally conscious state (inconsistent but reproducible signs of conscious awareness). 4 In the intensive care unit setting, patients with DoC are at risk of withdrawal of life-sustaining treatment (WLST) as early as 1 day post-injury, 5 in many cases due to the assumption that meaningful recovery is unlikely. 6 However, in the last decade, evidence from large TBI cohort studies has demonstrated that some patients with DoC recover not only consciousness but also functional independence, with many returning to pre-injury levels of function.7–10 In the Transforming Research and Clinical Knowledge in TBI (TRACK-TBI) study, among participants in a vegetative state at 2 weeks, none remained in a vegetative state, and 25% achieved at least partial independence by 1 year post-injury. 11 Studies leveraging data from a longitudinal cohort of patients with TBI (i.e., TBI Model Systems [TBIMS]) 12 have shown that most patients with DoC (i.e., not following commands) during acute hospitalization recover command-following by inpatient rehabilitation admission. 7 Among participants admitted to inpatient rehabilitation not following commands who regained command-following during rehabilitation, >50% recovered functional independence by 1 year. 10 Furthermore, among those who did not follow commands by rehabilitation discharge, approximately 20% were independent by 1 year. 10 Functional recovery in participants with DoC can continue for at least 10 years after TBI. 8
Despite the potential for patients with DoC to regain independence, WLST is common and results in up to 70% of acute in-hospital TBI-related deaths.13,14 A frequent assumption is that even if patients with DoC survive and show incremental progress in recovery, their quality of life (QOL) will be poor, and they may have higher rates of depression or anxiety than non-DoC TBI cohorts. However, individuals with severe disability and chronic illness tend to report higher levels of QOL than healthy individuals would assume based on their level of functioning, a mismatch in perceptions referred to as the “disability paradox.15,16” Most studies of DoC recovery to date have focused on functional outcomes, which are commonly assessed using measures that can be reliably administered to a caregiver. As a result, we have limited knowledge about patient-reported outcomes in individuals who have emerged from DoC.
To better understand QOL and psychological health in patients with prolonged DoC, we utilized data from the TBIMS to address the following questions: (1) among TBIMS participants admitted to inpatient rehabilitation with DoC (i.e., unable to follow commands), what proportion recovers the ability to complete subjective self-report measures; and (2) among TBIMS participants who recover the ability to self-report, what is their QOL and degree of anxiety and depression at 1, 2, and 5 years post-injury. To facilitate generalization between our study and studies of chronic DoC, we conducted an additional secondary analysis on the subset of patients who were unable to follow commands for ≥28 days post-injury.
Methods
In this observational study, we used data from the TBIMS National Database (NDB), which houses longitudinal demographic, clinical, and outcome data (i.e., at 1 year, 2 years, 5 years, and every 5 years subsequently) prospectively collected at 23 inpatient rehabilitation hospitals.12,17 TBIMS enrolls patients meeting the following inclusion criteria: (1) acute TBI, (2) age of 16 years or older at the time of TBI, and (3) admitted to a TBIMS acute care hospital within 72 h of TBI. Participants in the current study were (1) discharged from a TBIMS inpatient rehabilitation program between January 1989 and June 2023, (2) classified as having DoC at inpatient rehabilitation admission based on the absence of command-following, and (3) followed on measures of QOL, anxiety, or depression at the 1-year time point. Study procedures were approved by the institutional review board of each TBIMS site. All participants, or a surrogate, provided informed consent.
Participants were classified as having DoC if they lacked command-following on admission to inpatient rehabilitation, as the absence of command-following is a key clinical feature of DoC that can be derived from the TBIMS NDB. Consistent with prior TBIMS studies,7–10 we used the following criteria to identify participants with DoC: (1) the date of command-following was after the date of admission to inpatient rehabilitation, and (2) the Disability Rating Scale (DRS) 18 motor subscale score on admission was greater than zero (i.e., not following commands). According to TBIMS standard operating procedures, command-following is recorded on the date a participant accurately follows simple motor commands at least twice within 24 h, as demonstrated on the Glasgow Coma Scale (motor subscale score = 6) or in medical record clinical notes.
At the time of the TBIMS follow-up, trained research staff contacted the participant or surrogate to conduct a telephone-based outcome assessment. If the assessment was completed with the caregiver, the study staff documented the reason that the participant did not complete the assessment themselves (e.g., participant physically or cognitively impaired; unable to contact).
Measures
The primary outcome measures were the Satisfaction With Life Scale (SWLS), 19 Generalized Anxiety Disorder-7 Scale (GAD-7), 20 and the Patient Health Questionnaire-9 (PHQ-9) 21 completed by the participant during the TBIMS interview at 1 year post-injury. Due to concerns with validity, 22 the TBIMS standard operating procedure does not permit subjective self-report measures to be completed by a proxy. Although these measures were developed and normed on typically functioning individuals, multiple studies suggest that they are valid for use in TBI.23–25 In a secondary analysis, we report data on these self-report measures at the 2- and 5-year post-injury follow-up time points.
Satisfaction With Life Scale
The SWLS is a 5-item scale that measures an individual’s judgment of their overall QOL. Items are rated on a 7-point scale (7 = strongly agree; 1 = strongly disagree), with a total score range of 5–35. Total scores between 5 and 9 suggest that the respondent is “extremely dissatisfied” with life, whereas total scores between 31 and 35 suggest that the respondent is “extremely satisfied” with life. An average SWLS score of 26.5 was previously reported in healthy cohorts, 26 and an average score range of 20.3–21.8 was reported in participants with moderate-to-severe TBI.27–29 The SWLS has been collected continuously in the TBIMS NDB since 1998.
Generalized Anxiety Disorder-7 Scale
The GAD-7 is a 7-item self-report measure of anxiety. GAD-7 scores range from 0 to 21, with a score of ≥10 generally considered the cutoff point requiring a formal clinical evaluation referral. 21 In the general population, the mean GAD scores range between 3.0 and 6.1.20,30 In a large study of patients with moderate-to-severe TBI, the average GAD-7 score at 1 year post-injury was 3.1. 31 The GAD-7 measure was added to the TBIMS NDB in 2010. However, data collection for the GAD-7 was paused in 2013, restarted in 2017, and transitioned to a 2-item screener in 2022 (i.e., if the responses to the first two GAD-7 questions are “not at all,” the measure is discontinued, and the total score is not calculated). Therefore, we included GAD-7 data collected between 2010–2013 and 2017–2022.
Patient Health Questionnaire-9
The PHQ-9 is a 9-item self-report measure of depression. PHQ-9 scores range from 0 to 27, with a score of ≥10 serving as the clinical cutoff point for major depressive disorder. 21 A mean score of 3.2 has been reported for individuals without major depressive disorder and a mean score of 17.1 for those with major depressive disorder. 21 In a large study of patients with moderate-to-severe TBI, an average PHQ-9 score of 4.46 was reported at 1 year post-injury. 31 The PHQ-9 measure was added to the TBIMS NDB in 2007, paused in 2013, restarted in 2017, and transitioned to a 2-item screener in 2022 (i.e., if the responses to the first two PHQ-9 questions are “not at all,” the measure is discontinued, and the total score is not calculated). Therefore, we included PHQ-9 data collected between 2007–2013 and 2017–2022.
Disability Rating Scale
The DRS is an 8-domain, 30-point scale used to assess the severity of a participant’s disability.18,32 The scores span from 0 (no disability) to 30 (death), with higher scores reflecting more severe disability, greater dependence on others, and less functional recovery. Although total scores have been used to classify the level of disability, 18 these classification levels have not been validated. For example, scores of 22–29 are considered to be in the range for a vegetative state.33,34
Functional Independence Measure
The Functional Independence Measure (FIM) 35 is an 18-item scale used to quantitatively assess a participant’s functional status across a variety of domains that can be combined into an FIM Cognitive Subscale score (range: 5–35), FIM Motor Subscale score (range: 13–91), and FIM Total score (range: 18–126). Higher FIM scores reflect a higher degree of independence.
Glasgow Outcome Scale–Extended
The Glasgow Outcome Scale–Extended (GOSE) is an 8-item measure used to assess a participant’s global outcome after TBI.36,37 It is administered via a structured interview including questions relating to assistance at home, shopping and travel, work, social and leisure activities, family and friendships, and return to normal life. Scores range from 1 (death) to 8 (upper good recovery), with higher scores reflecting better recovery. Participants assigned a score of 2 are considered to be in a vegetative state.
Statistical analysis
Primary analyses
We reported the descriptive statistics (i.e., n [%], mean, standard deviation [SD], range) for demographic (e.g., age at injury, sex, race) and clinical variables. We compared demographic and clinical characteristics between participants who could self-report at the 1-year follow-up time point versus those who could not self-report due to physical or cognitive reasons using Welch’s two-sample t-tests for continuous variables and Fisher’s exact tests for categorical variables. We also reported the descriptive statistics for functional outcomes (i.e., DRS, FIM, GOSE) and self-reported outcomes (i.e., SWLS, GAD-7, PHQ-9) at the 1-year post-injury follow-up time point. In the absence of a clinical cutoff point for dissatisfaction with life, we reported the number (n) and proportion (%) of participants with scores below “neutral” (i.e., <20) and in each SWLS category (e.g., extremely satisfied, satisfied). We also calculated the number and proportion of participants with GAD-7 and PHQ-9 scores above the clinical cutoff point for anxiety (GAD-7 ≥ 10) and depression (PHQ-9 ≥ 10). We reported the descriptive statistics for other variables (i.e., primary payor source during inpatient rehabilitation and 1-year marital status, residence, living situation, employment, and Participation Assessment with Recombined Tools-Objective 38 ) in Supplementary Data.
Secondary analyses
Prolonged DoC has been defined as impaired arousal and awareness lasting for ≥28 days39,40 and is associated with a worse outcome than a brief period of DoC during the acute phase of recovery. 9 Therefore, we conducted a secondary analysis of a subsample of participants who were unable to follow commands for ≥28 days post-injury but who recovered the ability to self-report at 1 year post-injury (Supplementary Data). We also conducted a secondary analysis to evaluate outcomes at 2 and 5 years post-injury.
Results
Participant characteristics
Between January 1989 and June 2023, 887 participants meeting the TBIMS definition of DoC were enrolled into the TBIMS NDB, and 693 (78.1%) were followed at 1 year post-injury (Fig. 1). The primary reasons the participants did not have outcome data were loss to follow-up (e.g., unable to contact; 85/887 [10%]) and death (61/887 [7%]) at 1 year. Among the 693 participants followed, 349/693 (50%) completed the 1-year follow-up interview independently, and 317/349 (91%) had data on at least one of our primary outcome measures (SWLS, GAD-7, PHQ-9). The primary reason a caregiver proxy rather than the participant completed the follow-up interview was due to the participant's physical and/or cognitive inability to complete the interview (252/344 [73%]). The most common caregiver proxy respondent was a parent (123/252 [49%]), followed by a spouse (58/252 [28%]).
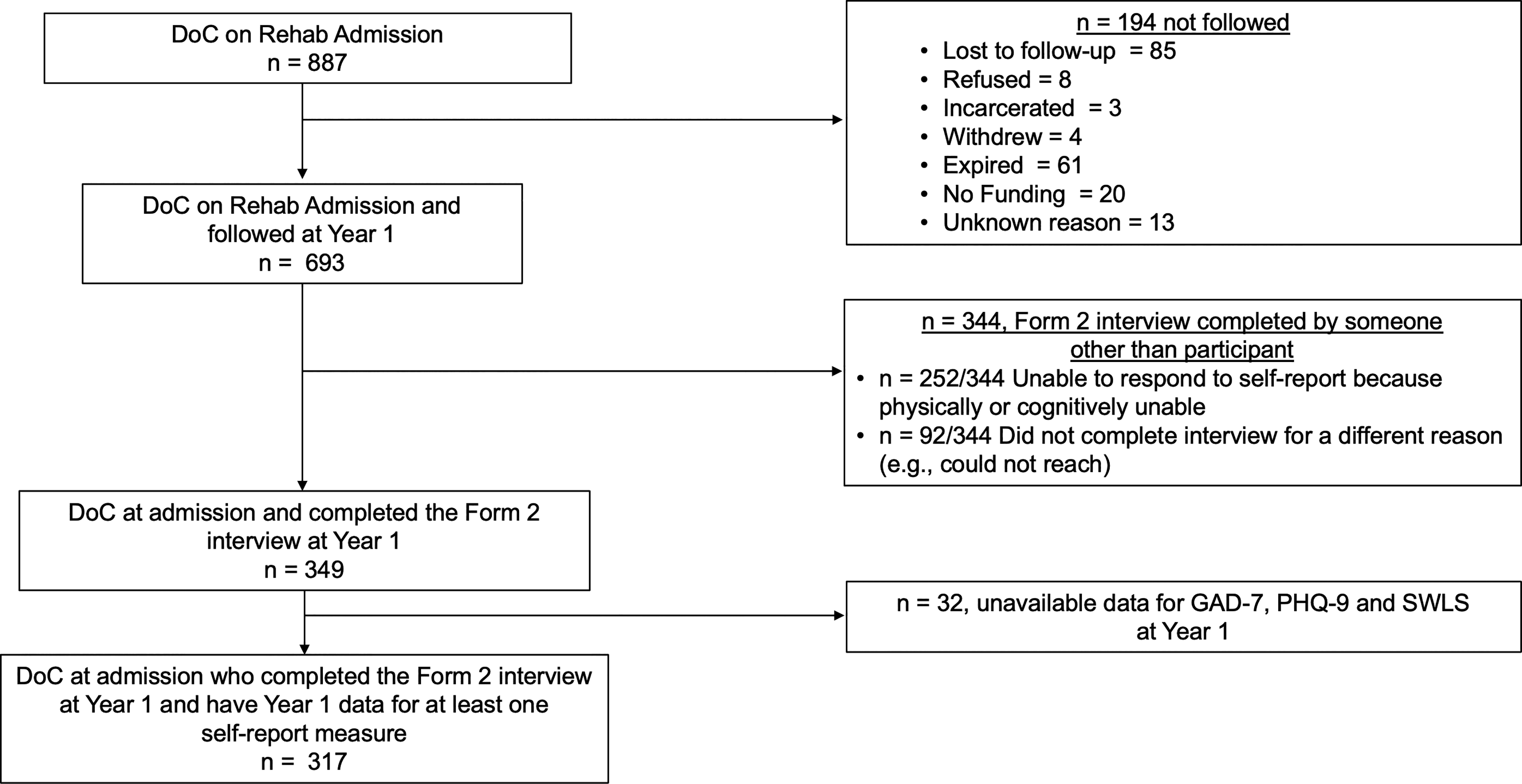
Participant inclusion flowchart. Among 887 participants enrolled into the Traumatic Brain Injury Model Systems (TBIMS) who met our criteria for DoC, 693 were followed at 1 year post-injury, and 317 (50%) provided self-report on at least one of our primary outcome measures. Two-hundred and fifty-two (36%) were unable to provide self-report due physical/cognitive reasons. Ninety-two (13%) were unable to provide self-report for some other reason. Participants met the criteria for DoC if both of the following conditions were met: (1) date of command-following (TBIMS NDB variable name: “FollowComm”) was after the date of admission to inpatient rehabilitation (i.e., TBIMS NDB variable name: “RehabAdm”) and (2) Disability Rating Scale (DRS) 18 motor subscale score on admission (i.e., TBIMS NDB variable name: “DRSMotA”) was greater than zero (i.e., not following commands). DoC, disorders of consciousness; Generalized Anxiety Disorder-7 Scale; PHQ-9, Patient Health Questionnaire-9; SWLS, Satisfaction With Life Scale.
Compared with participants who were unable to self-report at 1 year post-injury due to physical and/or cognitive reasons, participants who were able to self-report were significantly younger (33.14 years vs. 37.70 years; p = 0.002), had shorter acute (27.61 days vs. 42.60 days; p < 0.001) and rehabilitation (50.03 days vs. 80.53 days; p < 0.001) length of stays, and had less disability on the DRS, less dependence on the FIM, and better global outcomes on the GOSE (Table 1 and Supplementary Data). Among participants who were unable to self-report at 1 year post-injury, 12% to 18% were classified as being in a vegetative state based on their DRS and/or GOSE scores (DRS total = 22–29, GOSE = 2). Additional demographics and outcomes for these samples can be found in Supplementary Table S1. Secondary analyses of those with prolonged DoC (i.e., unable to follow commands for ≥28 days) are in Supplementary Tables S2–S4. Supplementary Figures S1 and S2 provide the frequency distributions for the GOSE, DRS, and FIM comparing participants who were unable with those able to provide self-report at 1 year post-injury.
Demographic and Clinical Characteristics of Participants Admitted to TBIMS With DoC
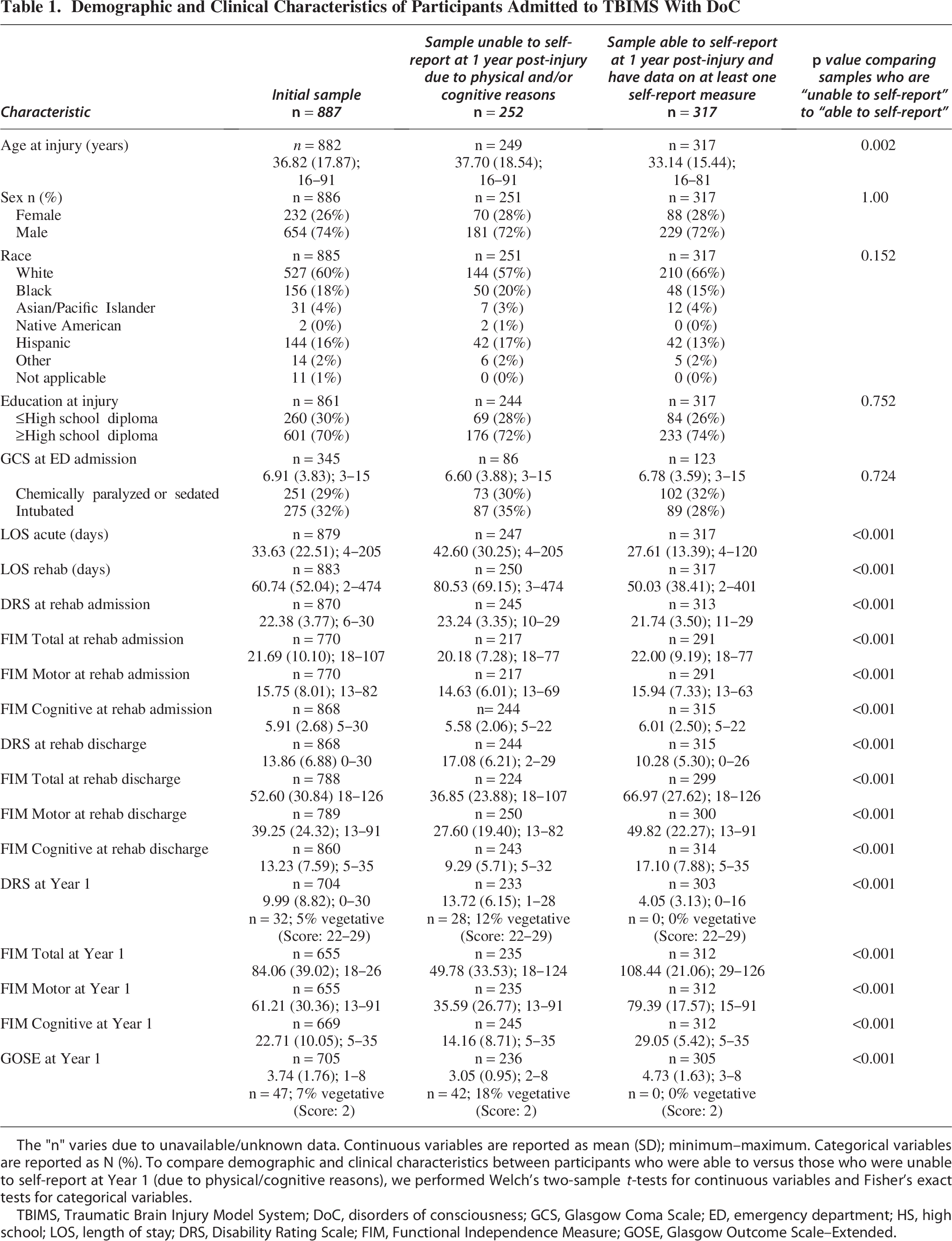
The "n" varies due to unavailable/unknown data. Continuous variables are reported as mean (SD); minimum–maximum. Categorical variables are reported as N (%). To compare demographic and clinical characteristics between participants who were able to versus those who were unable to self-report at Year 1 (due to physical/cognitive reasons), we performed Welch’s two-sample t-tests for continuous variables and Fisher’s exact tests for categorical variables.
TBIMS, Traumatic Brain Injury Model System; DoC, disorders of consciousness; GCS, Glasgow Coma Scale; ED, emergency department; HS, high school; LOS, length of stay; DRS, Disability Rating Scale; FIM, Functional Independence Measure; GOSE, Glasgow Outcome Scale–Extended.
Primary results
Among participants admitted to inpatient rehabilitation with DoC and followed at 1 year, 50% (349/693) regained the capacity to respond to questions on self-report measures; 36% (252/693) did not due to physical/cognitive reasons; and 13% (92/693) did not for some other reason (e.g., unable to reach; Table 1). The mean (SD) total score for the SWLS was 20.38 (7.81), GAD-7 was 4.00 (5.66), and PHQ-9 was 5.22 (5.04; Table 2). Of the 311 participants with SWLS data (Fig. 2a, 2d), 9% reported extreme dissatisfaction, 15% dissatisfaction, 19% satisfaction, and 10% extreme satisfaction with life. Scores on the GAD-7 were above the clinical cutoff point for anxiety in 15 of 105 (14%) participants (Fig. 2b, 2e), and scores on the PHQ-9 were above the clinical cutoff point for depression in 22 of 139 (16%) participants (Fig. 2c, 2f).
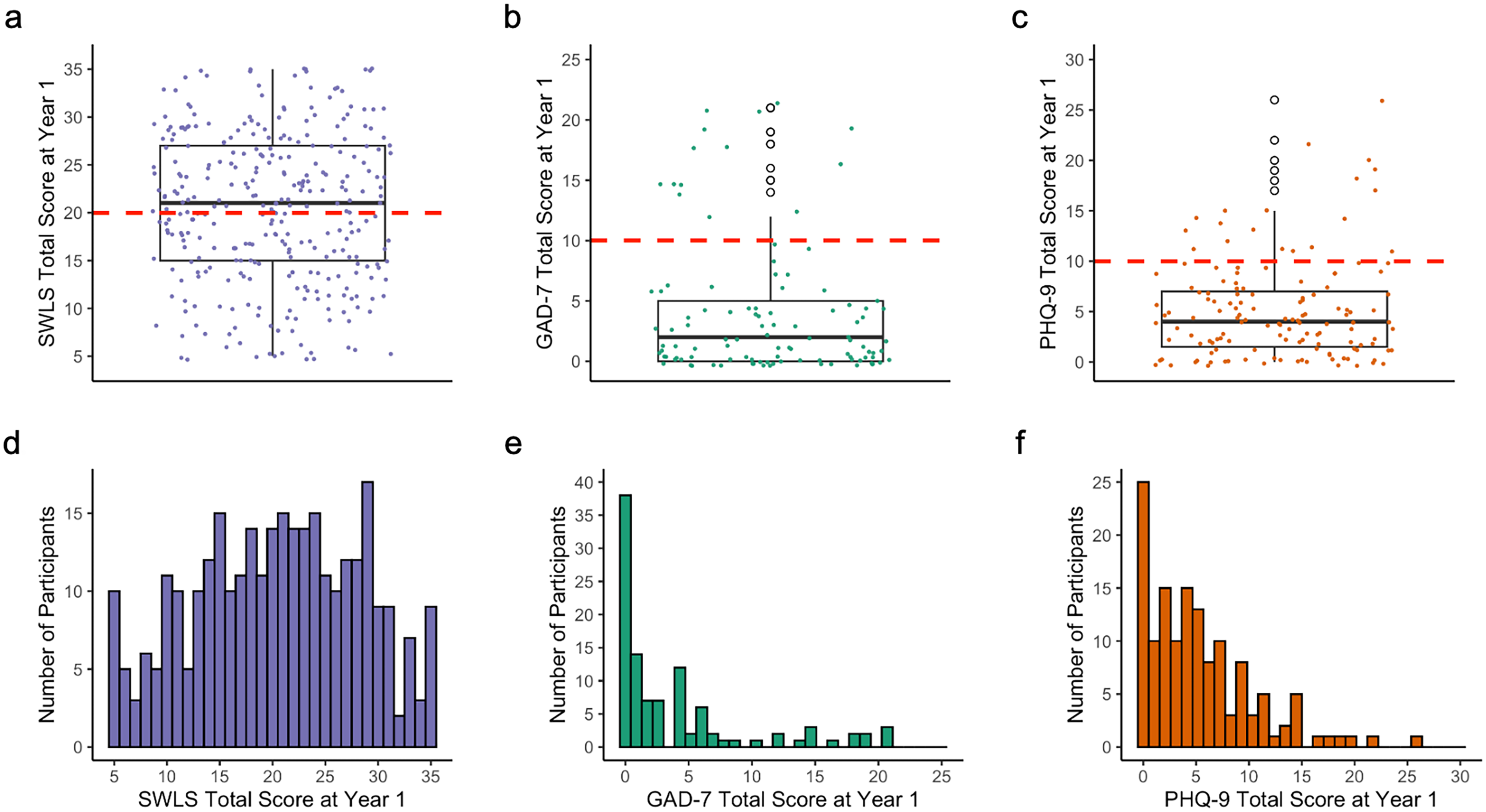
Boxplots and frequency distributions for each outcome measure in patients with DoC who were able to self-report at the 1-year post-injury follow-up assessment. Box plots (top row) indicate the median, interquartile range, and 1.5× the interquartile range values for the SWLS
Outcome Measure Results for Participants Admitted to TBIMS With DoC Who Recovered the Ability to Provide Self-Report by the 1-Year Follow-Up
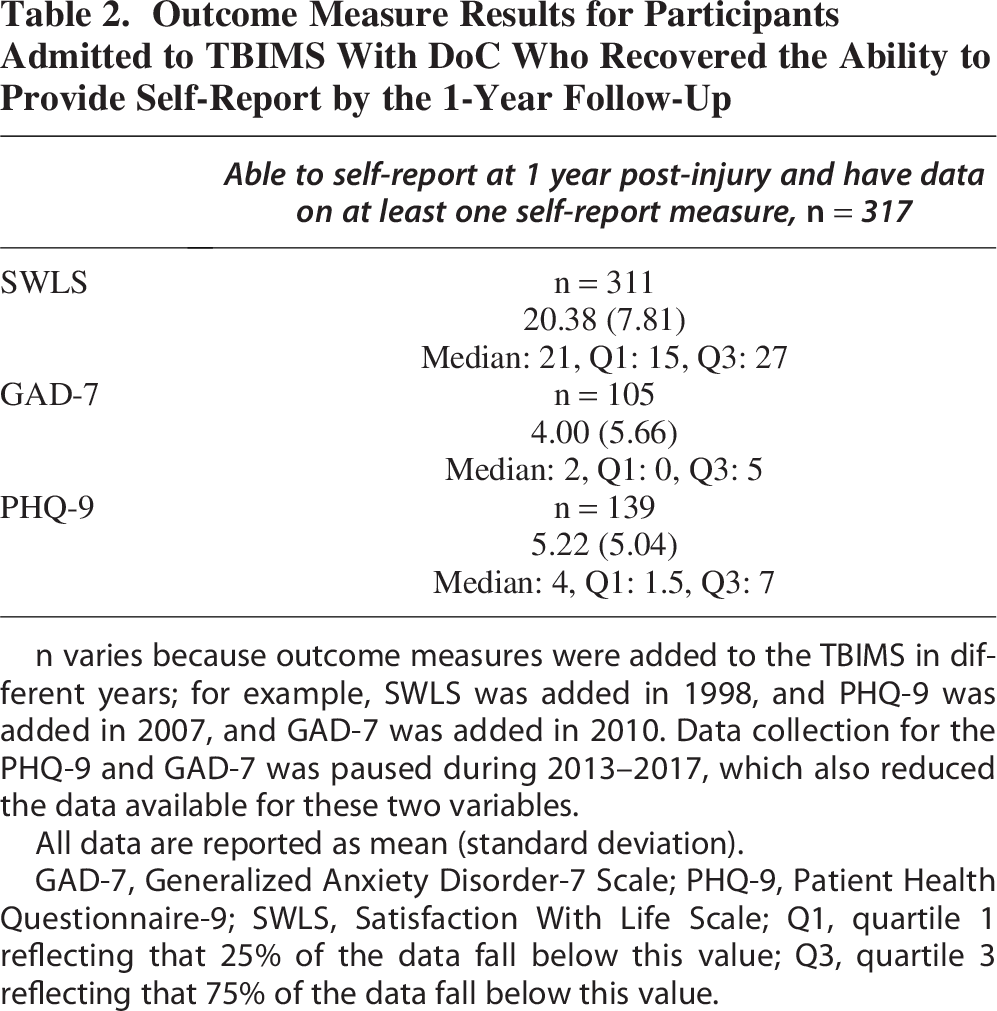
n varies because outcome measures were added to the TBIMS in different years; for example, SWLS was added in 1998, and PHQ-9 was added in 2007, and GAD-7 was added in 2010. Data collection for the PHQ-9 and GAD-7 was paused during 2013–2017, which also reduced the data available for these two variables.
All data are reported as mean (standard deviation).
GAD-7, Generalized Anxiety Disorder-7 Scale; PHQ-9, Patient Health Questionnaire-9; SWLS, Satisfaction With Life Scale; Q1, quartile 1 reflecting that 25% of the data fall below this value; Q3, quartile 3 reflecting that 75% of the data fall below this value.
Secondary results
Participants who had DoC for ≥28 days post-injury (243/317 [77%]) had SWLS, GAD-7, and PHQ-9 scores that were comparable to those of the full sample (n = 317) and the cohort that recovered command-following in <28 days (74/317 [23%], Supplementary Tables S3 and S4). SWLS, GAD-7, and PHQ-9 scores in this subgroup of participants with prolonged DoC were also similar to those of individuals with moderate-to-severe TBI in prior studies.27–29
Among participants in the full cohort who were followed at 2 and 5 years post-injury, 53% and 57%, respectively, recovered the ability to self-report. SWLS, GAD-7, and PHQ-9 total scores were similar at the 2-year and 5-year time points to those reported at the 1-year time point. See Supplementary Table S5 for the basic demographic and clinical characteristics of these cohorts; Supplementary Table S6 for SWLS, GAD-7, and PHQ-9 data; and Supplementary Table S7 for a more detailed characterization of the cohorts at each time point.
Discussion
We found that among TBIMS participants admitted to inpatient rehabilitation with DoC, half recovered the ability to complete self-report outcome measures by 1-year post-injury. On average, these participants reported QOL and levels of anxiety and depression that were similar to those reported by participants with moderate-to-severe TBI at 1 year post-injury27–29,31 and the general population.20,21,26,41 Our results align with the “disability paradox” (i.e., people with severe disability report better QOL than would be predicted for them by able-bodied individuals) 15 and provide support for the continued care and rehabilitation of persons with DoC.7–10 Early WLST occurs, in part, due to the misconception that individuals with severe brain injury will not recover consciousness or independence, and even if they do, they are likely to have poor QOL and/or psychological health. 42 Our findings do not support this premise and, instead, demonstrate that individuals with severe brain injury who emerge from DoC have high rates of self-reported well-being.
It is important to highlight that dissatisfaction with life, anxiety, and depression were reported by some individuals who recovered from DoC. The average SWLS scores in our cohort suggested “neutral” QOL, consistent with prior studies in patients with TBI27–29,43,44 and slightly lower compared with healthy individuals. 26 Nearly a quarter of participants reported some degree of dissatisfaction with life, which is similar to that reported in a 10-year follow-up TBIMS study of moderate-to-severe TBI 44 but substantially higher than the 6% reported in a large United States (U.S.) sample of community-dwelling healthy adults. 45 In persons with TBI, QOL appears to be optimized when (1) basic needs are met, (2) individuals participate in everyday life, (3) there is a trusting circle of care, (4) individuals feel seen and accepted, (5) individuals find meaning in relationships, (6) there are opportunities for giving back and advocating, and (7) individuals achieve purpose and value, 46 providing potential targets for interventions and community support programs. Our results highlight the clear need for the ongoing assessment of QOL and emotional health over the course of recovery. Existing evidence-based mental health interventions may be appropriate for persons with severe TBI experiencing increased levels of anxiety and depression.47,48 Furthermore, it is possible that strong disability supports and resources may improve QOL and psychological health in this population.49,50
One limitation of these results is related to our assessment of consciousness. We relied on the TBIMS definition of DoC, which is based on the absence of command-following. The absence of command-following is just one clinical feature of DoC, and sole reliance on this behavior may exclude participants at the higher end of DoC (e.g., those who can follow commands but cannot functionally communicate). Thus, our sample may overrepresent individuals on the lower end of the DoC spectrum.51,52 Furthermore, the date of command-following in the TBIMS is established via a retrospective chart review by trained data collectors, which prevented us from determining if and when participants recovered from DoC after discharge from inpatient rehabilitation. Nevertheless, we used follow-up GOSE and DRS scores as coarse estimates of DoC diagnosis and, as expected, only observed scores consistent with the vegetative state range in the “unable to self-report” group. Prospective assessment with a comprehensive, standardized, validated behavioral tool such as the Coma Recovery Scale–Revised 53 would allow the more precise selection of participants with DoC.
Several additional limitations should be considered when interpreting our results. The generalizability of TBIMS data has been criticized due to its inclusion criteria (e.g., participants who were treated at acute care hospitals and inpatient rehabilitation facilities participating in TBIMS) and potential bias associated with facilities receiving TBIMS funding (e.g., academic centers in urban areas). However, the TBIMS sample has been shown to be representative of patients receiving inpatient rehabilitation across the U.S. 54 Nevertheless, patients with DoC are more likely to be admitted to inpatient rehabilitation if they have signs of potential recovery of function. 55 Consequently, psychological health and QOL scores reported by participants in this study may be representative of individuals with better overall outcomes. Although the TBIMS follow-up rate is high (>80%), 17 previous work has revealed Hispanic ethnicity, lower education level, and lack of private health insurance to be predictors of loss to follow-up, 3 suggesting that our results may not generalize to persons with those demographic characteristics. Furthermore, intervention data are not collected during TBIMS follow-up assessments, and therefore, its potential impact on participants’ outcomes is unknown. In addition, our follow-up sample likely included both participants who did not regain consciousness and those who regained consciousness but were still unable to provide self-report. The experience of these participants remains unknown, which is an inevitable limitation of studies investigating internal states. Proxy reporting, while suitable for observable constructs such as functional dependence, is not recommended for self-report measures of internal states, 56 which are tied to an individual’s subjective well-being and cannot be assessed in a valid manner via external observation. For example, self-reported QOL is a related, but distinct construct from functional status 57 and remains relatively preserved, even in individuals with severe disability. 58
Another potential concern is that the QOL scores for participants who provided self-report could have been influenced by cognitive impairments that affect insight and awareness of deficits. However, prior evidence suggests these deficits do not result in a positive bias for self-reported QOL in TBI.59–61 In a study comparing how persons with TBI rate their QOL versus how their QOL is rated by a caregiver (n = 74 dyads across the TBI severity spectrum), although QOL was rated higher by persons with TBI relative to their proxies, 59 the subsample of individuals with TBI who had “low” self-awareness of deficits reported lower QOL than those with “adequate” self-awareness. These findings suggest that cognitive impairments resulting in a lack of insight into deficits do not result in the overestimation of QOL. 59 Evidence from studies showing that QOL is related to injury severity and functional independence after TBI also supports this finding.60,61 In a large sample of individuals with TBI, those with the most severe injuries reported the greatest decrease in life satisfaction at 6 months post-injury and the highest life dissatisfaction in most domains of QOL. 61 In a small study of participants who presented to inpatient rehabilitation with prolonged DoC and survived to 5-year follow-up, self-reported health-related QOL was within the normative range and positively associated with functional independence. 60 Taken together, these findings, which span a range of TBI severities and sample sizes, suggest that individuals with DoC who recover the ability to self-report can validly rate their QOL and internal states, such as anxiety and depression. Notably, in our study, the 1-year FIM Cognitive Subscale scores in participants who recovered the ability to self-report were similar to the scores of participants in a separate study of moderate-to-severe TBI. 62 This is a group that is regularly assessed with self-report measures in the TBIMS and other studies.29,63,64 In fact, SWLS and PHQ-9 are two of the most commonly studied TBIMS follow-up outcome measures. 12 Moreover, TBIMS examiners are trained to determine whether participants may be too cognitively impaired to comprehend the questions, which would prompt the completion of the interview with a surrogate. Nevertheless, it is worth considering whether QOL and psychological health reporting, in general, requires validation given that even healthy individuals may have an unrealistic and/or inaccurate perception of themselves.65,66
Our findings should be validated in large prospective datasets that include patients with traumatic and nontraumatic DoC. It will also be valuable to investigate whether other factors, such as social determinants of health, health care policy, and payor source, influence recovery. Future work could consider assessing individual trajectories of QOL and psychological health in this population as well as exploring how they relate to measures of functional outcomes (e.g., DRS, GOSE). 67 These measures generally lack the granularity needed to detect subtle improvement in function; new outcome measures that target the nuances of recovery from severe brain injury and can be administered remotely are needed. 68
Conclusion
Participants admitted to inpatient rehabilitation with DoC are likely to recover the ability to provide self-report of subjective well-being. Among these participants, QOL and psychological health are similar to those of the general population. These observations challenge previous nihilistic prognostic biases. Our findings may provide guidance to families and providers when making decisions about WLST and considering acute inpatient rehabilitation referral in the early phase of TBI recovery.
Transparency, Rigor, and Reproducibility Statement
This study was listed as a part of the TBIMS Notification System, wherein researchers provide background, aims, and methods to TBIMS investigators before conducting the project. All participants were accounted for in the CONSORT diagram (Fig. 1). Data were labeled using codes that were not linked to participant identifying information (e.g., name). Data were collected in accordance with the TBIMS standard operating procedure by trained data collectors. All software programs used to perform acquisition and analysis are widely available through R Studio. The key inclusion criterion (i.e., classified as having disorders of consciousness at inpatient rehabilitation admission based on the absence of command-following) is an accepted standard in the field. Statistical analysis and/or review was performed by N.G. Multiple comparisons were not used, as statistical analysis was conducted to compare the samples on demographic, injury, and clinical variables and not to answer the primary research question. No replication or external validation studies have been performed or are planned/ongoing at this time to our knowledge. Data from this study are available in a public archive: https://www.tbindsc.org/. The corresponding author may provide analytic codes upon request.
Authors’ Contributions
All authors were involved in the conceptualization, methodology, and review and editing of the article. N.G. and Y.G.B. were further responsible for the formal analysis, visualization, and writing of the original draft. B.M. also assisted with the writing of the original draft.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by the following funding sources: Indiana TBI Model System under Award No. 90DPTB0022; Moss TBI Model Systems under Award No. 90DTB0019; Spaulding Rehabilitation Hospital under Grant No. 90DPTB0027-01–01, National Institute of Mental Health under Award No. T32MH019938, and Congressionally Directed Medical Research Program under Awards No. HT94252310621 and No. HT94252310563. This material is the result of work supported with resources and the use of facilities at the James A. Haley Veterans’ Hospital. The Tampa VA Research and Education Foundation was the administering institution for Award No. HT9425-23-1-0621 and No. HT94252310563. Dr. Gilmore is a Research Without Compensation Employee at the James A. Haley Veterans’ Hospital in Tampa, Florida. Dr. Nakase-Richardson is the Associate Chief of Staff for Research at the James A. Haley Veterans’ Hospital in Tampa, Florida.The contents of this publication do not represent the views of the Department of Veterans Affairs or the United States Government.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.