
Abstract
Delirium is a common complication among survivors of traumatic brain injury (TBI). Although prior studies have predominantly focused on delirium onset following moderate to severe TBI, mild TBI accounts for the majority of TBI cases in hospital settings. However, key risk factors for delirium in this population remain unclear. In this prospective observational study, we analyzed changes in sleep parameters and circadian rhythm during the first 7 days following mild TBI among patients in a neurosurgical ward. We further identified the key factors associated with post-TBI delirium. This study included 100 patients with mild TBI. Delirium was evaluated using the traditional Chinese version of the 4 A’s Test (4AT). Sleep parameters and circadian rhythms were monitored through actigraphy for up to 7 consecutive days following admission. Risk factors for post-TBI delirium were identified through univariate and multivariate regression analyses. A total of 12 patients developed delirium, three of whom exhibited delirium onset immediately before their first nighttime sleep. Therefore, the actigraphic data of these individuals were exclusively classified as post-delirium. The remaining 97 patients were categorized into delirium and nondelirium groups. Interdaily stability was significantly lower in the delirium group than in the nondelirium group (0.27 vs. 0.48, p = 0.007). Risk factor analysis revealed that each one-unit increase in interdaily stability was associated with an 84% reduction in delirium risk (adjusted hazard ratio: 0.16, 95% confidence interval [CI]: 0.03–0.78). In summary, circadian rhythm disruptions are associated with an increased risk of delirium following mild TBI. This study underscores the importance of circadian rhythm stability and may inform targeted interventions aimed at preventing delirium in this patient population.
Introduction
Delirium, a common complication following traumatic brain injury (TBI), is characterized by fluctuating attention and disorganized thinking. These symptoms are often overlooked during hospitalization. More than 50% of all patients with acute-phase moderate to severe TBI develop delirium during intensive care unit (ICU) stay.1,2 Patients who develop delirium following brain injury are at an increased risk of prolonged hospitalization, long-term cognitive impairment, and mortality. 3 Although most studies have focused on delirium following moderate to severe TBI, mild TBI accounts for the majority of TBI cases in hospital settings. 4 Furthermore, acute cognitive impairment in patients with mild TBI may lead to long-term cognitive decline. 5 These findings underscore the need for further research regarding the development of delirium in patients with mild TBI.
Sleep–wake disruption predisposes patients to delirium during hospitalization. 6 Delirium and sleep–wake rhythm disturbances may share underlying mechanisms. 7 A systematic review revealed that delirium is associated with several sleep-related parameters, such as reduced total sleep time (TST), sleep efficiency (SE), nighttime minutes of rest, and minutes of rest over 24 h, as measured using an accelerometer. 8 However, this association has not been explored in patients with TBI. TBI can directly impair sleep regulation and is thus considered a potential risk factor for disturbances in the sleep–wake cycle and circadian rhythm. 9
In this study, we analyzed changes in the sleep–wake cycle and circadian rhythm during the first 7 days after TBI among patients in a neurosurgical ward. In patients who developed delirium, we further investigated whether the aforementioned changes were associated with the onset of post-TBI delirium.
Methods
Study design and setting
This prospective observational study included patients from the neurosurgical ward of a medical center in northern Taiwan between October 2022 and October 2023. The study protocol was approved by the Joint Institutional Review Board of Taipei Medical University (approval number: N202205062).
Study cohort
Eligible patients were adults aged ≥20 years who received a diagnosis of TBI and had a Glasgow Coma Scale (GCS) score of 13–15 upon admission to the neurosurgical ward. Patients with a pre-existing psychiatric or cognitive disorder (e.g., dementia), a history of drug or alcohol use, or any other neurological condition (e.g., stroke or brain tumor) before the study were excluded from this study.
Measurement
Information sheet
A structured information sheet was used to collect data on clinicodemographic variables potentially associated with delirium, for example, age, sex, GCS score, medical and medication history, and alcohol consumption.10,11
Pittsburgh Sleep Quality Index
The Pittsburgh Sleep Quality Index is a self-report questionnaire designed to measure sleep quality over 1 month across the following seven components: subjective sleep quality, sleep latency, sleep duration, habitual SE, sleep disturbances, sleep medication use, and daytime dysfunction. The total score ranges from 0 to 21, with scores greater than 5 indicating poor sleep quality. 12 During validation, the Chinese version of the Pittsburgh Sleep Quality Index exhibited strong validity and reliability. 13
Actigraphy
Objective sleep parameters were evaluated using a Mini Motionlogger Actigraph, a wrist-worn accelerometer capable of distinguishing between sleep and wake states depending on the amount of movement. Data were recorded in 60 s epochs and analyzed using the Cole–Kripke algorithm 14 to determine minute-by-minute sleep–wake status. Sleep data obtained through actigraphy are comparable to those obtained through polysomnography 15 and have been widely used in research exploring sleep patterns in patients with TBI. 16 In accordance with standard ward routines, wherein nurses encourage rest and dim ward lights between 10 pm and 6 am, the nighttime and daytime periods were defined as the interval between 10 pm and 6 am and that between 6 am and 10 pm, respectively, to standardize sleep analyses. The following nighttime sleep parameters were assessed: TST, sleep onset latency (SOL), SE, wake after sleep onset (WASO), sleep fragmentation index (SFI), and activity index. Nighttime TST refers to the cumulative duration of sleep during the nighttime period. SOL is the interval between bedtime and the first sustained sleep period of at least 20 consecutive minutes. WASO is the total time spent awake after the onset of a continuous sleep state. SE is the ratio of TST to the total time spent in bed. The SFI is the ratio of the number of awakenings to TST in minutes. The activity index is the percentage of epochs with an activity score greater than zero. The following daytime parameters were assessed: TST and activity index.
The following circadian rhythm indicators were measured: intradaily variability (IV), interdaily stability (IS), and relative amplitude (RA).17,18 IV quantifies the fragmentation of rest–activity cycles. Values range from 0 to 2, with higher IV indicating greater fragmentation. IS quantifies the multiday stability of rest–activity rhythms. Values range from 0 to 1, with higher IS indicating a more stable rhythm. RA can be calculated using the formula (M10 − L5)/(M10 + L5), where L5 represents the average activity level during the 5 least active consecutive hours of the day and M10 represents the average activity level during the 10 most active consecutive hours. RA values range from 0 to 1; higher values indicate a greater circadian amplitude, reflecting more regular rest–activity rhythms.
All patients were instructed to continuously wear the actigraphy device on their nondominant wrist for up to 7 days following enrollment. The device was removed only for bathing or medical procedures, and patients were advised to reattach it immediately afterward.
Delirium assessment
The traditional Chinese version of the 4 A’s Test was used to identify delirium. This rapid bedside screening tool enables delirium assessment in less than 2 min during daily clinical practice. The test encompasses four key domains: alertness, Abbreviated Mental Test 4, attention, and acute onset or fluctuating course. The total 4AT score ranges from 0 to 12, with a score of ≥4 indicating delirium, whereas a score above 0 but lower than 4 indicates cognitive impairment without delirium. 19 The traditional Chinese version of 4AT exhibited high diagnostic accuracy, with a sensitivity of 0.90 and a specificity of 0.94. 20
Statistical analysis
All statistical analyses were conducted using Statistical Package for the Social Sciences (SPSS) (version 25; IBM, Armonk, NY, USA). A p value of <0.05 was considered statistically significant. The chi-square and Mann–Whitney U tests were used to compare demographic characteristics, sleep parameters, and circadian rhythms between patients. Fisher’s exact test was performed when any cell in the contingency table had an expected frequency of <5. For patients who developed delirium after the first nighttime sleep, actigraphic data were categorized into pre-delirium and post-delirium periods on the basis of the recorded time of delirium onset. For instance, if the onset time was 11:00 am, the pre-delirium period included data collected up to 10:59 am and the post-delirium period included data collected 11:01 am onward. If delirium developed before the first nighttime sleep, only actigraphic data from the post-delirium period were analyzed (Supplementary Figs. S1 and Figs. S2). The Bonferroni method was used for multiple comparison correction. 21 Wilcoxon’s signed-rank test was used to compare sleep parameters and circadian rhythms between the pre-delirium and post-delirium periods. Cox proportional-hazards regression models were used to investigate the correlation between sleep disturbances and post-TBI delirium. The models were adjusted for covariates that have previously been associated with delirium onset (i.e., age, sex, sedative–hypnotic use, body mass index).11,22,23 If any variables violated the proportional-hazards assumption (Schoenfeld residuals test), stratified Cox regression models were used.24,25 Circadian rhythm data were standardized using Z scores. Results are presented as crude and adjusted hazard ratios with corresponding 95% CIs. Post hoc power analysis was performed using G*Power, 26 incorporating the observed sample size, the number of incident post-TBI delirium events, a two-sided α of 0.05, and the hazard ratios for circadian rhythm indicators.
Results
Patient demographics
This study included 100 patients, of whom 12 developed delirium during the acute phase of TBI. Actigraphic data were categorized into two periods: pre-delirium and post-delirium. Three patients had no pre-delirium actigraphy data because they developed delirium immediately upon their admission to the ward (within 1 h of their enrollment in this study) and were therefore excluded. Finally, 97 patients with TBI were included in the analysis. No patient exhibited changes in neurological symptoms, assessed on the basis of pupil size and the GCS score, suggesting no worsening of brain injury.
Nine patients (9.2%) in the final sample developed delirium during hospitalization. The characteristics of these patients were similar to those of patients excluded from the analysis because of the lack of relevant data (n = 3; Supplementary Tables S1 and S2). The patients’ median age was 69 years, and 49% of them were men. Clinicodemographic characteristics were similar between patients with delirium and those without it (Table 1).
Characteristic of Participants
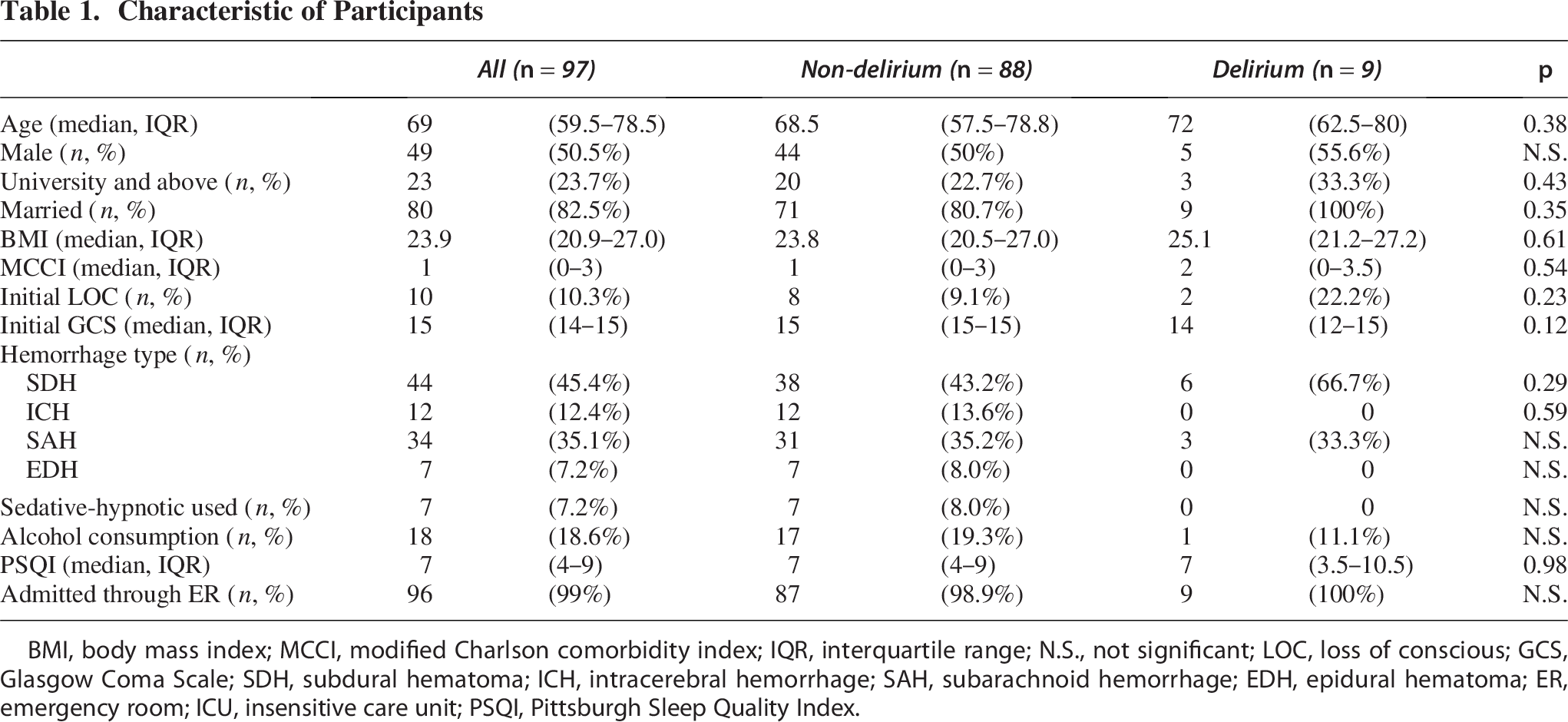
BMI, body mass index; MCCI, modified Charlson comorbidity index; IQR, interquartile range; N.S., not significant; LOC, loss of conscious; GCS, Glasgow Coma Scale; SDH, subdural hematoma; ICH, intracerebral hemorrhage; SAH, subarachnoid hemorrhage; EDH, epidural hematoma; ER, emergency room; ICU, insensitive care unit; PSQI, Pittsburgh Sleep Quality Index.
Actigraphic data
The sleep parameters measured before delirium onset, except IS, were generally similar between the delirium and nondelirium groups (Table 2). The delirium group exhibited longer TST during both the nighttime and daytime periods before delirium onset than did the nondelirium group, but this difference was nonsignificant. IS was significantly lower in the delirium group than in the nondelirium group (0.27 vs. 0.48, p = 0.007).
Comparing Sleep Parameters Before Developing Delirium Between Nondelirium and Delirium Groups
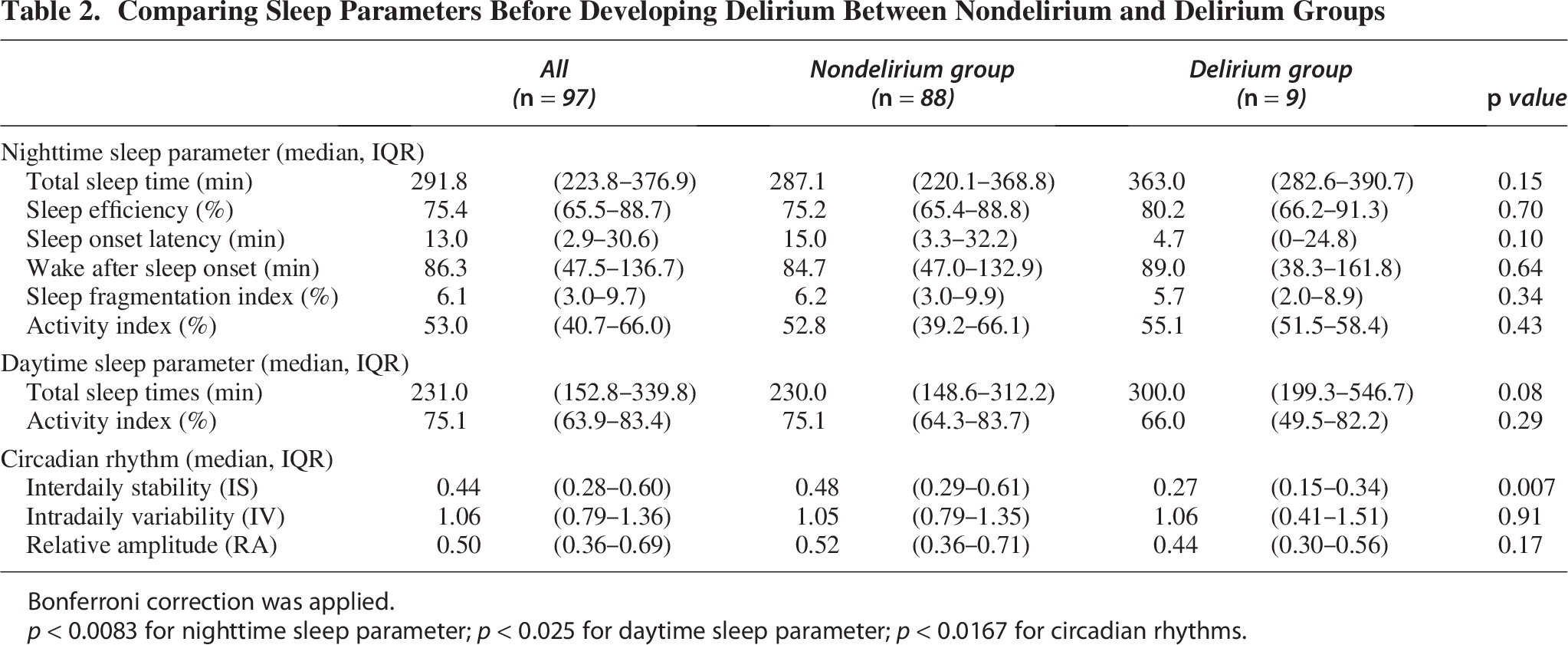
Bonferroni correction was applied.
p < 0.0083 for nighttime sleep parameter; p < 0.025 for daytime sleep parameter; p < 0.0167 for circadian rhythms.
Effect of circadian rhythm on post-TBI delirium risk
IS emerged as a potential risk factor for delirium in the univariate Cox regression analysis (Table 3). Because sex-related data violated the proportional-hazards assumption, stratified Cox regression was performed. In the multivariate Cox regression analysis, IS remained significantly associated with the risk of post-TBI delirium (adjusted hazard ratio: 0.16, 95% CI: 0.03–0.78). These findings indicate that for each one-unit increase in IS (reflecting greater multiday stability in rest–activity rhythms), the risk of post-TBI delirium decreased by 82%.
Risk of Developing Post-TBI Delirium
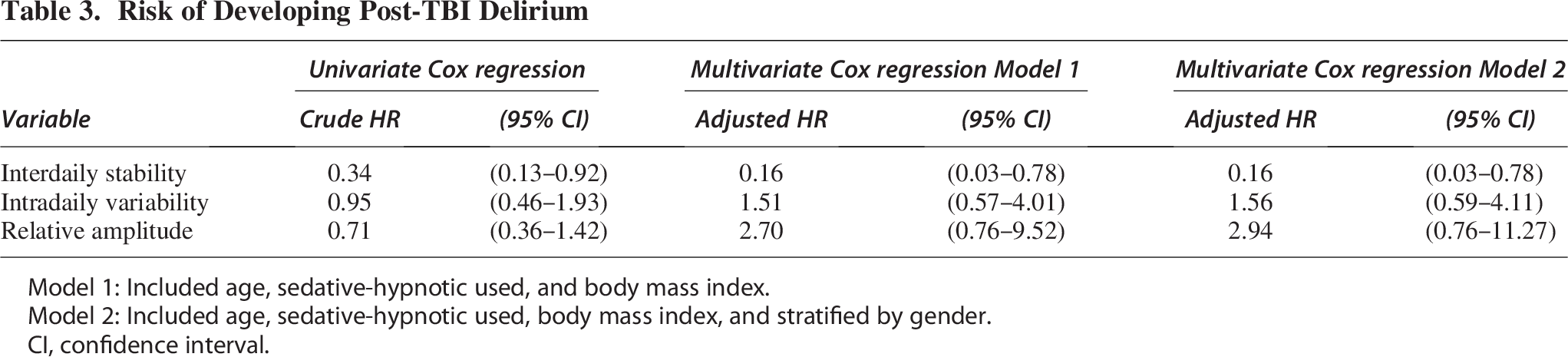
Model 1: Included age, sedative-hypnotic used, and body mass index.
Model 2: Included age, sedative-hypnotic used, body mass index, and stratified by gender.
CI, confidence interval.
Results of power analysis
Power analysis included 97 patients, among whom 9 had incident delirium. Post hoc power analysis indicated that, given the observed sample size and event count, our study had 7% power to detect a hazard ratio of 0.16 for IS at a two-sided α of 0.05.
Discussion
To the best of our knowledge, this is the first study to explore the association of delirium onset during the first 7 days following mild TBI with the sleep–wake cycle. Our findings associated a disrupted circadian rhythm in TBI survivors with delirium. Specifically, IS influences the risk of post-TBI delirium.
Our findings are consistent with those of a study reporting lower IS in patients with delirium than in those without it. 27 IS measures the consistency of circadian rhythms over multiple days, reflecting the degree of similarity in day–night patterns over time. 28 In the present study, patients who developed delirium exhibited increasingly irregular 24 h circadian rhythms. In most cases of delirium, symptoms developed between 48 h and 72 h after hospitalization, indicating that hospitalization-related factors contributed to the disruptions in stable sleep–wake patterns. Certain aspects of routine care for patients with TBI—for example, frequent neurological examinations, may affect the stability of their sleep–wake cycle. For instance, in one study, a higher frequency of neurochecks in the ICU was associated with a higher risk of delirium in patients with TBI. 29 Further research is required to clarify key factors influencing the regularity of sleep–wake patterns in general ward settings.
Our study suggests that IS, a circadian rhythm parameter, can serve as a predictor of delirium following mild TBI. This finding is consistent with that of a study linking variations in circadian rhythm performance to an increased risk of delirium in other populations. 30 Circadian dysregulation may contribute to the onset of delirium by disrupting the synchronization of patients’ internal clocks with external environmental cues. 31 Circadian rhythms are natural biological cycles that typically follow a 24 h pattern in humans. 32 Light plays a key role in aligning and regulating these rhythms. 33 In hospitalized patients with TBI, sleep disruption has been attributed to both internal and external factors, including environmental lighting. 34 Controlling environmental factors, including light, has proven effective in reducing stressors and preventing delirium in ICU settings. 35 Given that the establishment of causal relationships between circadian rhythm indicators and delirium is challenging, 36 our findings should be interpreted with caution, and further research is required to confirm the results.
Post-traumatic hyposomnia (PTH) is a common condition among patients with acute-stage or chronic TBI, with a reported prevalence of 20% to 55%.37,38 PTH is defined as an increase in TST by more than 2 h within a 24 h period compared with the baseline value, operationally defined as an average TST exceeding 570 min.16,39 In our study, patients who developed delirium exhibited a PTH sleep pattern before its onset, suggesting an association between PTH and delirium risk. The underlying pathology of PTH likely involves the downregulation of hypocretin-1 (also known as orexin-A) in the cerebrospinal fluid of patients with TBI.40,41 However, a study revealed higher plasma orexin-A levels in older adults with delirium than in those without it, but this difference was nonsignificant. 42 This discrepancy may be attributable to the different types of samples analyzed, given that the level of orexin-A in plasma may not accurately reflect its level in the cerebrospinal fluid. Overall, the precise role of orexin-A in the pathophysiology of delirium remains unclear. Future studies should explore the variations in the sleep–wake cycle and its mediators, such as orexin-A, across various populations with delirium. Further research is required to elucidate the correlation between PTH and delirium in TBI survivors.
Limitations
This study has several limitations. First, the small number of patients with mild TBI and the low rate of delirium development might have reduced statistical power and led to a lower incidence than that in other studies. Consequently, our findings are not generalizable to the broader TBI population. Second, the absence of hormonal, cerebrospinal fluid, and plasma biomarkers limited our ability to investigate the biological mechanisms underlying the association between circadian rhythm and delirium. Finally, our analysis did not account for comorbidities that contribute to circadian disruption—for example, sleep apnea, potentially hindering a comprehensive understanding of the observed associations. Therefore, our findings should be interpreted with caution.
Conclusion
Our findings suggest that sleep pattern alterations and circadian rhythm disruption following mild TBI, particularly as measured using IS, are associated with delirium. This finding offers valuable insights into the relationship between sleep disturbances and delirium, highlighting the need for health care providers to incorporate circadian rhythm management into delirium prevention strategies. Additional studies are warranted to validate these findings in patients with varying degrees of TBI severity and to elucidate potential causal pathways linking circadian rhythm and delirium.
Transparency, Rigor, and Reproducibility
This prospective observational study included 100 patients. Primary outcomes were evaluated in 97 patients after the exclusion of 3 patients because of the lack of actigraphic data before delirium onset. Our findings have not yet been replicated or externally validated. The data generated during this study are available from the corresponding author, H.-Y.C., upon reasonable request.
Authors’ Contributions
C.-J.L.: Conceptualization, methodology, formal analysis, and writing (original draft). Y.-S.L.: Conceptualization and data collection. D.M.F.: Conceptualization. L.-P.C.: Conceptualization. H.-H.C.: Conceptualization. H.-C.L.: Conceptualization. H.-Y.C.: Methodology, formal analysis, writing (review and editing), and supervision.
Footnotes
Author Disclosure Statement
The authors have no potential conflicts of interest to declare.
Funding Information
This work was supported by the National Science and Technology Council of Taiwan (grant numbers: NSTC 111-2314-B-038-033-MY3 and NSTC 113-2628-B-038-003-MY3).
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.