
Abstract
Pediatric spinal cord injury (SCI) induces extensive neuroplastic changes in the developing brain; however, the patterns of cortical remodeling associated with complete (CSCI) and incomplete (ICSCI) injuries remain poorly understood. In this study, high-resolution structural magnetic resonance imaging was used to assess cortical morphological alterations in 72 pediatric SCI patients (38 CSCI and 34 ICSCI) and 37 age-matched healthy controls (HCs). Key cortical metrics—including surface area, thickness, volume, and curvature—were analyzed to characterize injury-related reorganization. Significant group differences were identified across multiple cortical regions. Compared with HCs, both CSCI and ICSCI patients exhibited reduced surface area in the left primary somatosensory cortex (S1), with CSCI patients showing significantly greater surface area than ICSCI. In the left posterior cingulate cortex (PCC), surface area was significantly reduced in the CSCI group compared with ICSCI. Cortical thickness analysis revealed that both patient groups showed increased thickness in the bilateral superior and middle temporal regions, but decreased thickness in the left paracentral lobule, inferior insula, and right supramarginal gyrus (SMG). Notably, CSCI patients had significantly lower thickness in the right SMG than ICSCI patients. For cortical volume, both SCI groups exhibited increased volume in the bilateral transverse frontopolar cortex, with the CSCI group showing significantly greater volume in the right hemisphere compared with ICSCI. No significant differences were found in cortical curvature across groups. Correlation analyses showed that surface area in the left PCC was positively associated with sensory scores across all patients. In ICSCI patients, right frontopolar volume positively correlated with both motor and sensory scores. Receiver operating characteristic analysis demonstrated that surface area (left S1, PCC), cortical thickness (right SMG), and cortical volume (right transverse frontopolar cortex) could differentiate CSCI from ICSCI, with a combined classification model achieving an area under the curve of 0.7980. Our findings indicated that CSCI and ICSCI are associated with distinct patterns of cortical reorganization in regions related to sensory processing and affective-cognitive integration. These results highlight the diagnostic potential of multidimensional cortical morphometry and support its relevance in guiding individualized, neuromodulation-based rehabilitation strategies in pediatric SCI.
Introduction
Childhood and adolescence represent pivotal periods for brain development, characterized by continuous transformations in the cerebral cortex. 1 These processes include enhanced white matter myelination and synaptic pruning, which facilitate dynamic remodeling of cortical morphology, including alterations in thickness, volume, and gyrification.1,2 This structural reorganization underlies the maturation of motor and sensory abilities and establishes the neurobiological foundation for higher-order capabilities such as executive control and social cognition.3,4 However, the cerebral cortices of children exhibit greater susceptibility to environmental factors than those of adults. Prior research indicates that exposure to adverse environments during childhood, such as traumatic brain injury, psychological trauma, or malnutrition, can disrupt cortical development and ultimately result in atypical neurofunctional outcomes.5–8 Timely interventions may mitigate or prevent deviations in neural functional development.
Traumatic spinal cord injury (SCI) constitutes a severe form of injury-related exposure, resulting in sensorimotor impairments below the level of the lesion in pediatric patients. Studies have demonstrated that SCI not only causes localized neural damage but also induces adaptive reorganization within the sensorimotor cortex.9,10 Given the immaturity of the motor cortex in children, pediatric SCI patients during a critical neurodevelopmental period may exhibit unique neuroplastic manifestations distinct from adults, potentially hindering the recovery of sensorimotor function.11,12 Moreover, the structural integrity of the sensorimotor cortex serves as a crucial neurobiological foundation for interventions such as repetitive transcranial magnetic stimulation (rTMS) and brain–computer interface (BCI) interventions.13,14 Investigating these changes is essential not only to uncover the neurobiological mechanisms of cortical remodeling following pediatric SCI but also to inform neuromodulation therapies targeting the sensorimotor cortex. In addition, recent evidence indicates that some children with SCI develop psychiatric symptoms post-injury, such as anxiety, depression, executive dysfunction, or social cognitive deficits, with some even exhibiting suicidal tendencies.15–17 These symptoms may be closely associated with adaptive responses in higher cortical regions to spinal afferent disruption. Specifically, studies in murine SCI models have demonstrated that SCI alters the Neuregulin 1 signaling pathway between the prefrontal cortex and hippocampus, potentially mediating cognitive deficits. 18 Furthermore, post-SCI endoplasmic reticulum stress and impaired neurogenesis in the brain are strongly associated with cognitive dysfunction and depression-like behaviors. 19 Therefore, within this research context, investigating cerebral abnormalities in pediatric SCI patients may elucidate the neurobiological mechanisms underlying higher-order dysfunctions and support the development of early interventions to mitigate or delay the onset of these complications.
Previous MRI studies have demonstrated that pediatric SCI can induce structural alterations in brain regions involved in sensorimotor processing and affective cognition.9,10 A recent study in children with CSCI reported alterations in cortical thickness in brain regions associated with sensorimotor, cognitive, and visual functions. 20 However, this study focused solely on cortical thickness. Each morphological metric—thickness, surface area, volume, and curvature—is thought to reflect distinct underlying biological processes. 21 Consequently, reliance on a single metric is insufficient to characterize the cortical alterations following SCI. The cerebral cortex represents a highly complex neural structure, with morphology characterizable via high-resolution structural MRI (sMRI), which provides quantified information on cortical volume, surface area, thickness, and curvature. Specifically, cortical volume constitutes the product of surface area and thickness. Cortical surface area is associated with the differentiation of cortical plate neurons, somatic growth, and the development of surrounding neural fibers (including axons, dendrites, and synapses). 1 In contrast, cortical thickness is primarily influenced by neuronal and glial remodeling, synaptic pruning, and pericortical myelination. 22 Meanwhile, cortical folding patterns (curvature) are linked to the migratory pathways of neurons during development. 23 Therefore, we hypothesize that SCI may differentially impact the development of these cortical morphological features (surface area, thickness, volume, and curvature) in pediatric patients. A systematic quantification of these multidimensional parameters could yield a more precise characterization of cortical alterations following pediatric SCI.
SCI can be classified as CSCI (American Spinal Injury Association [ASIA] Grade A) and incomplete SCI (ICSCI, ASIA Grades B–D) based on the extent of preserved neurological function below the level of injury. These two injury types differ fundamentally in their patterns of afferent disruption: CSCI results in a complete interruption of neural input below the lesion, while residual ascending and descending pathways in ICSCI may provide an anatomical basis for partial signal transmission and compensatory reorganization between the spinal cord and brain. 24 Given these differences, we hypothesize that pediatric patients with CSCI and ICSCI may exhibit distinct patterns of cortical reorganization. Consequently, neuromodulatory interventions such as rTMS should consider these cortical alterations, as the therapeutic targets may differ. Supporting this hypothesis, a previous neuroimaging study in adults has revealed distinct patterns of gray matter volume (GMV) alterations in the primary somatosensory cortex (S1) and primary motor cortex between CSCI and ICSCI patients. 25 In addition, clinical studies have indicated that pediatric patients with CSCI and ICSCI may exhibit differential risk profiles for anxiety and depression—differences potentially attributable to distinct cortical reorganization patterns. 16 This hypothesis is further supported by findings in adult SCI populations. For instance, Kim et al. reported that patients with CSCI exhibited lower fractional amplitude of low-frequency fluctuations values in the superior medial frontal gyrus and middle frontal gyrus compared with those with ICSCI. 26 Despite these findings, the differences in cortical morphological remodeling between pediatric CSCI and ICSCI remain unclear. Moreover, accurate diagnosis and severity classification of SCI in children remain challenging due to limited patient cooperation and the lack of pediatric-specific functional assessment tools. 27 Notably, a study in adult SCI populations has reported that approximately 20%–30% of patients initially diagnosed with CSCI are reclassified as ICSCI within 30 days post-injury. 28 However, treatment strategies and rehabilitation goals differ substantially between CSCI and ICSCI patients. 29 In ICSCI, where corticospinal pathways are partially preserved, interventions such as rTMS may promote functional recovery by enhancing residual neural connectivity. 13 In contrast, CSCI entails a complete disruption of descending pathways, requiring alternative approaches such as BCIs or neuroprosthetic systems to bypass the lesion and restore motor output. 14 These fundamental differences highlight the urgent need for objective neuroimaging biomarkers that can facilitate early and accurate differentiation between CSCI and ICSCI in pediatric populations.
In summary, this study aims to utilize sMRI to investigate differences in cortical morphological reorganization—specifically surface area, thickness, volume, and curvature—between pediatric patients with CSCI and ICSCI. The goals are to elucidate the neurobiological mechanisms underlying cortical remodeling in both CSCI and ICSCI groups and to identify objective neuroimaging biomarkers that may inform diagnosis and neurorehabilitation interventions.
Materials and Methods
Participants
The study protocol adhered to the Declaration of Helsinki and was formally approved by the Medical Research Ethics Committee of XuanWu Hospital. Prior to enrollment, written informed consent was obtained from all pediatric participants and their legal guardians. This prospective cohort included 75 children with SCI and 37 age- and sex-matched healthy controls (HCs), recruited between December 2019 and August 2022. Their demographic and clinical characteristics were systematically gathered through standardized questionnaires. Standardized clinical assessments were performed 1–2 h before MRI acquisition. For SCI participants, neurological assessments encompassed the American Spinal Injury Association (ASIA) Impairment Scales to ascertain ASIA grades, sensory/motor scores, lesion levels, and injury duration (time between SCI occurrence and recruitment), with evaluations carried out by two certified clinicians. After stratification, 39 individuals were categorized into the CSCI group (ASIA A) and 36 into the ICSCI group (ASIA B–D). Neuropathic pain (NP) evaluation, utilizing the Visual Analog Scale, verified the absence of NP symptoms among all SCI participants.
Inclusion criteria for the SCI cohort encompassed: (1) traumatic etiology (e.g., traffic accidents, falls, sports-related injuries); (2) right-hand dominance with a post-injury duration exceeding 2 months; (3) absence of neuropsychiatric comorbidities, genetic disorders, or a history of cranial trauma; (4) no documented substance abuse. HCs met similar criteria, excluding SCI-specific conditions. Exclusion criteria for all participants included: (1) structural brain abnormalities identified via conventional MRI; (2) inadequate image quality for computational analysis. Following an independent quality assessment conducted by two radiologists, one HC subject, one CSCI patient, and two ICSCI patients were excluded due to excessive motion artifacts or geometric distortions in sMRI scans. The comprehensive demographic information of the final SCI cohort is presented in Supplementary Table S1 (these data were collected at the MRI session).
MRI data acquisition
All neuroimaging data were acquired using a 3.0 T Siemens Prisma scanner (Erlangen, Germany) equipped with a 12-channel phased-array head coil. Prior to data acquisition, participants completed standardized preparation procedures, such as wearing noise-reduction earplugs and MRI-compatible visual aids, to enhance compliance and minimize motion artifacts and reduce acoustic interference. An initial neuroanatomical screening, utilizing axial T2-weighted turbo spin echo and fluid-attenuated inversion recovery sequences, was performed to exclude participants with macroscopic cerebral abnormalities. Following this, high-resolution structural imaging was carried out using a three-dimensional magnetization-prepared rapid gradient echo sequence. The imaging parameters were set as follows: repetition time of 1800 msec, echo time of 2.13 msec, inversion time of 1100 msec, flip angle of 9°, field of view of 256 × 256 mm2, matrix size of 256 × 256, slice thickness of 1 mm, isotropic voxel dimensions of 1 mm³, and a total acquisition time of 6 min and 59 sec. This protocol produced 192 continuous sagittal slices, covering the entire brain volume.
Data preprocessing
Neuroimaging data preprocessing was conducted by two radiologists, each with over 5 years of specialized experience. The initial step involved normalizing intensity and correcting bias fields in T1-weighted images, using the unified segmentation module of Statistical Parametric Mapping (SPM, Version 12). This was followed by pediatric-specific skull stripping, aligned to a brain template tailored for children aged 6–12 years (https://www.nitrc.org/projects/chn-pd). The next phase utilized FreeSurfer’s automated “recon-all” pipeline (version 6.0.0), which iteratively refined data through multiple computational stages, including affine registration to MNI152 space, topology-constrained detection of white matter boundaries, deformable pial surface generation, and vertex-wise morphometric calculations. Cortical thickness at each vertex was determined as the shortest distance between the pial and white matter surfaces. Cortical surface area was measured at the pial level to characterize the vertex area on the gray matter surface, while curvature indices reflected the local folding magnitude derived from surface normal vector analysis. Cortical volume was calculated as the product of surface area and thickness across cortical parcels.
Quality control encompassed manual inspection of FreeSurfer-derived surface reconstructions by two authors. The final preprocessing step involved spatial smoothing with a 10-mm full-width-half-maximum Gaussian kernel, followed by cortical surface alignment using high-dimensional spherical registration to establish vertex-wise correspondence across varying folding patterns.
Statistical analysis
Initially, a chi-square analysis was performed to examine gender distribution disparities among the three groups. To evaluate the distribution of continuous variables, the Kolmogorov–Smirnov test was employed. For demographic factors demonstrating normal distribution, group comparisons were carried out using either one-way analysis of variance (ANOVA) or independent sample t tests. Conversely, the Wilcoxon rank-sum test was applied to those variables lacking normal distribution.
Group-wise differences in cortical morphometry—specifically surface area, cortical thickness, and volume—were investigated through FreeSurfer’s QDEC module. A vertex-wise one-way ANOVA, grounded in a general linear modeling framework, was used to detect cortical variations across groups. This model incorporated age, sex, and global cortical measures (average cortical thickness or total cortical surface area/volume/curvature) as covariates. Analyses were conducted separately for the left and right hemispheres. Correction for multiple comparisons was performed using Monte Carlo simulation (5000 permutations), with clusters showing a corrected cluster-wise padj below 0.05 (uncorrected vertex-wise p < 0.01) deemed statistically significant.
Regions exhibiting significant morphometric alterations were delineated as regions of interest (ROIs). Corresponding ROI values were extracted for statistical analysis using a general linear model, with age, sex, and global cortical measures as covariates, followed by post hoc tests with false discovery rate correction (Benjamini–Hochberg method) for multiple comparisons (padj < 0.05). In addition, partial correlation analyses were performed to explore relationships between ROI-derived morphometric indicators and clinical variables—including motor and sensory function scores, age at injury, and injury duration—while adjusting for age and gender (p < 0.05). Finally, diagnostic utility of the morphometric markers in distinguishing pediatric CSCI from ICSCI was evaluated using receiver operating characteristic (ROC) analysis. This ROC was conducted as a binary classification task between pediatric ICSCI and CSCI cases, producing sensitivity and specificity estimates.
Results
Demographic data
The demographic characteristics of CSCI patients, ICSCI patients, and HCs are presented in Supplementary Table S1 and Table 1. We observed no significant difference in age (p = 0.817) and sex (p = 0.914) among three groups. In SCI patients, there was no significant between-group difference in injury duration between CSCI and ICSCI patients (p = 0.410). However, the motor (p < 0.001) and sensory scores (p < 0.001) were significantly higher in ICSCI patients when compared with CSCI patients.
Demographic and Clinical Characteristics of CSCI and ICSCI Patients and HCs
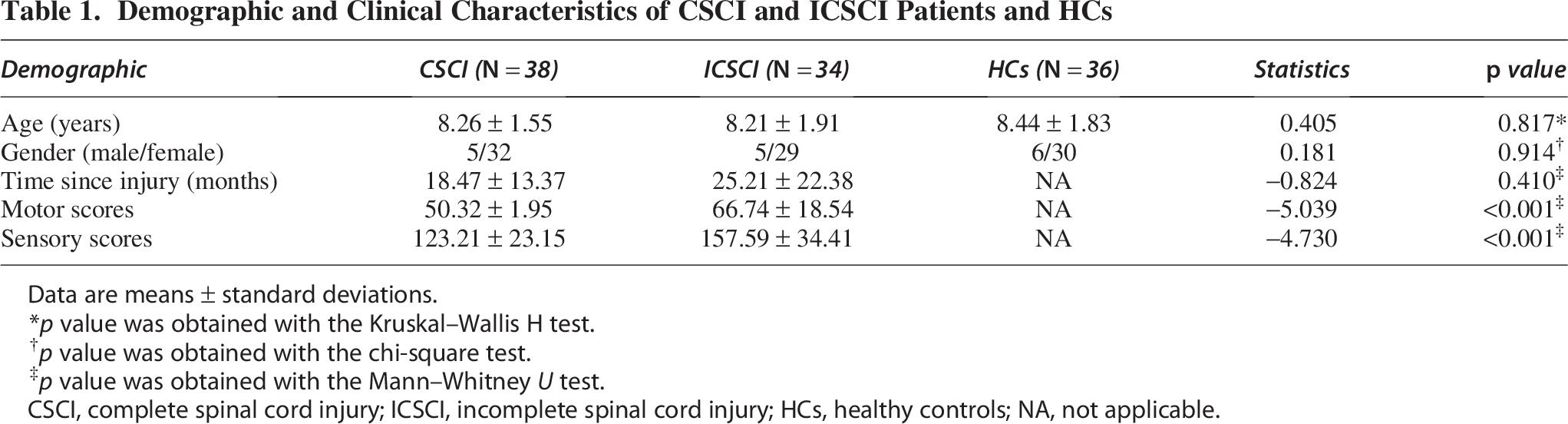
Data are means ± standard deviations.
p value was obtained with the Kruskal–Wallis H test.
p value was obtained with the chi‐square test.
p value was obtained with the Mann–Whitney U test.
CSCI, complete spinal cord injury; ICSCI, incomplete spinal cord injury; HCs, healthy controls; NA, not applicable.
Group differences in cortical metrics
Significant group differences in cortical surface area were observed among the CSCI, ICSCI, and HCs groups in the left S1 and posterior cingulate cortex (PCC; Fig. 1 and Table 2). Specifically, compared with HCs, both CSCI (padj = 0.0162, t = −2.620, Cohen’s d = −0.631) and ICSCI (padj = 0.0001, t = −4.426, Cohen’s d = −1.098) patients exhibited significantly reduced surface area in the left S1 (Fig. 1A). Furthermore, the CSCI group showed significantly greater surface area in the left S1 compared with the ICSCI group (padj = 0.0353, t = 2.286, Cohen’s d = 0.558; Fig. 1A). In the left PCC, cortical surface area was significantly lower in the CSCI group compared with the ICSCI group (padj = 0.0003, t = −4.094, Cohen’s d = −1.000) and significantly higher in the ICSCI group compared with the HCs group (padj = 0.0015, t = 3.529, Cohen’s d = 0.875; Fig. 1B). However, no significant differences were found between the CSCI and HCs groups in this region (padj = 0.335, t = −1.041, Cohen’s d = −0.251; Fig. 1B).

Comparison of cortical surface area among the HCs group, ICSCI group, and CSCI group.
Differences in Cortical Metrics of the Left and Right Hemisphere Between CSCI, ICSCI, and HCs
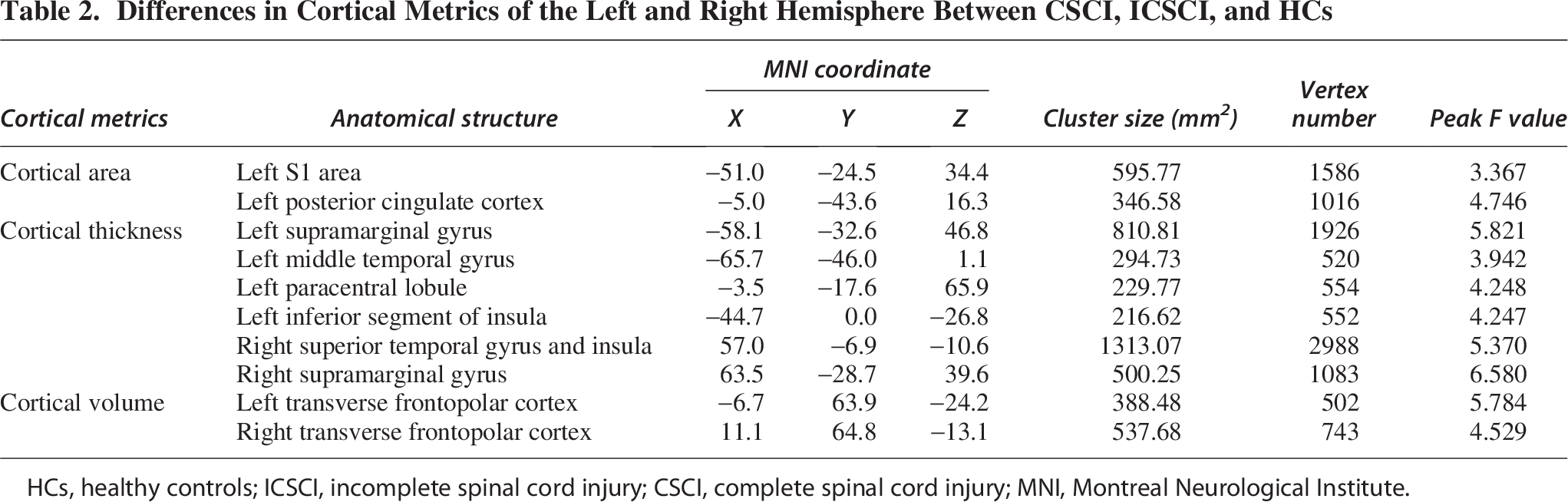
HCs, healthy controls; ICSCI, incomplete spinal cord injury; CSCI, complete spinal cord injury; MNI, Montreal Neurological Institute.
Significant group differences in cortical thickness were observed in the left supramarginal gyrus (SMG), middle temporal gyrus (MTG), paracentral lobule (PAL), and inferior segment of insula, as well as in the right SMG, superior temporal gyrus (STG), and insula (Fig. 2 and Table 2). Compared with HCs, the CSCI (padj < 0.0001, t = 4.708, Cohen’s d = 1.134) and ICSCI (padj < 0.0001, t = 5.764, Cohen’s d = 1.430) groups had significantly increased cortical thickness in the left SMG (Fig. 2A). Similarly, both patient groups showed increased cortical thickness in the left MTG (CSCI: padj = 0.0024, t = 3.344, Cohen’s d = 0.805; ICSCI: padj = 0.0006, t = 3.900, Cohen’s d = 0.967; Fig. 2B). In contrast, both CSCI and ICSCI groups exhibited reduced thickness in the left PAL (CSCI: padj = 0.0002, t = −4.241, Cohen’s d = −1.021; ICSCI: padj = 0.0010, t = −3.697, Cohen’s d = −0.917; Fig. 2C) and in the left inferior segment of insula (CSCI: padj = 0.0016, t = −3.494, Cohen’s d = −0.841; ICSCI: padj < 0.0001, t = −5.466, Cohen’s d = −1.356; Fig. 2D). In the right STG and insula, cortical thickness was also significantly lower in both CSCI (padj < 0.0001, t = −6.791, Cohen’s d = −1.635) and ICSCI (padj < 0.0001, t = −6.505, Cohen’s d = −1.614) groups (Fig. 2E), while in the right SMG, both groups showed significantly increased cortical thickness (CSCI: padj = 0.0012, t = 3.607, Cohen’s d = 0.868; ICSCI: padj < 0.0001, t = 4.818, Cohen’s d = 1.195; Fig. 2F). In addition, the CSCI group had significantly reduced cortical thickness in the right SMG compared with the ICSCI group (padj = 0.0489, t = −2.122, Cohen’s d = −0.519; Fig. 2F). No significant differences in cortical thickness were detected between the CSCI and ICSCI groups in the left SMG (padj = 0.191, t = −1.401, Cohen’s d = −0.342; Fig. 2A), MTG (padj = 0.365, t = −0.960, Cohen’s d = −0.235; Fig. 2B), PAL (padj = 0.869, t = −0.165, Cohen’s d = 0.020; Fig. 2C), left inferior segment of insula (padj = 0.059, t = 2.022, Cohen’s d = 0.494; Fig. 2D), and right STG and insula (padj = 0.660, t = 0.473, Cohen’s d = 0.116; Fig. 2E).
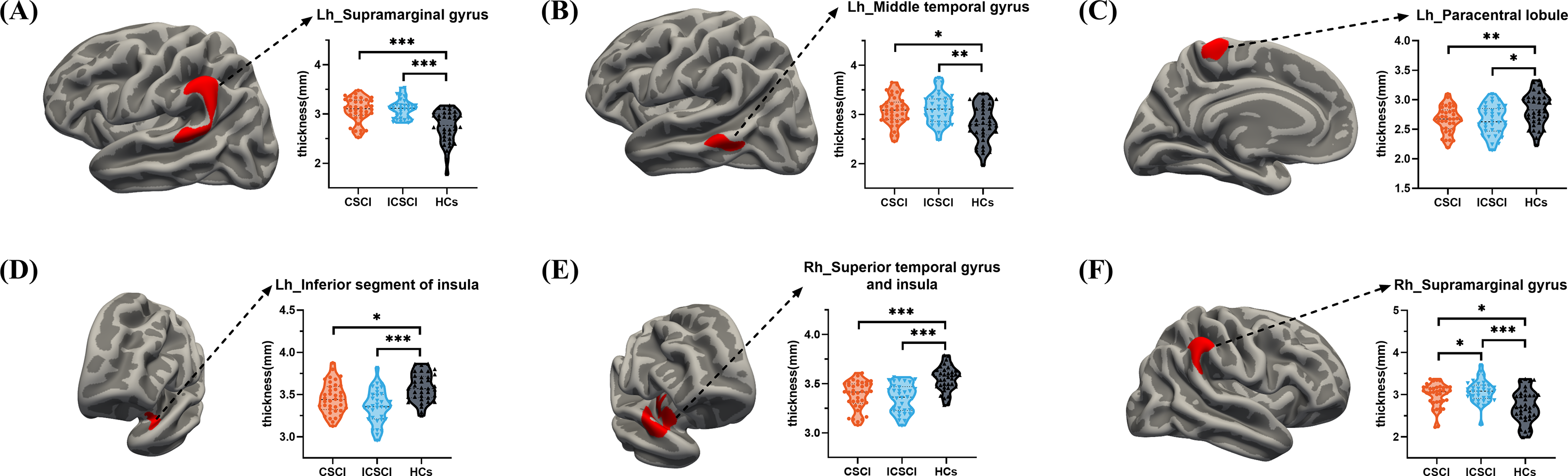
Comparison of cortical thickness among the HCs group, ICSCI group, and CSCI group.
Group differences in cortical volume were primarily observed in the bilateral transverse frontopolar cortices (Fig. 3 and Table 2). Compared with HCs, both CSCI (padj < 0.0001, t = 5.813, Cohen’s d = 1.399) and ICSCI (padj = 0.0057, t = 3.042, Cohen’s d = 0.755) patients demonstrated significantly increased volume in the left transverse frontopolar cortex (Fig. 3A). A similar pattern was observed in the right transverse frontopolar cortex (CSCI: padj < 0.0001, t = 5.188, Cohen’s d = 1.249; ICSCI: padj = 0.007, t = 2.971, Cohen’s d = 0.737; Fig. 3B). In addition, the CSCI group had significantly greater right transverse frontopolar cortex volume compared with the ICSCI group (padj = 0.035, t = 2.279, Cohen’s d = 0.557; Fig. 3B), although no significant differences were found between them in the left hemisphere (padj = 0.077, t = 1.883, Cohen’s d = 0.460; Fig. 3A). Detailed post hoc pairwise comparisons of cortical metrics between the CSCI, ICSCI, and HCs group are presented in Table 3.
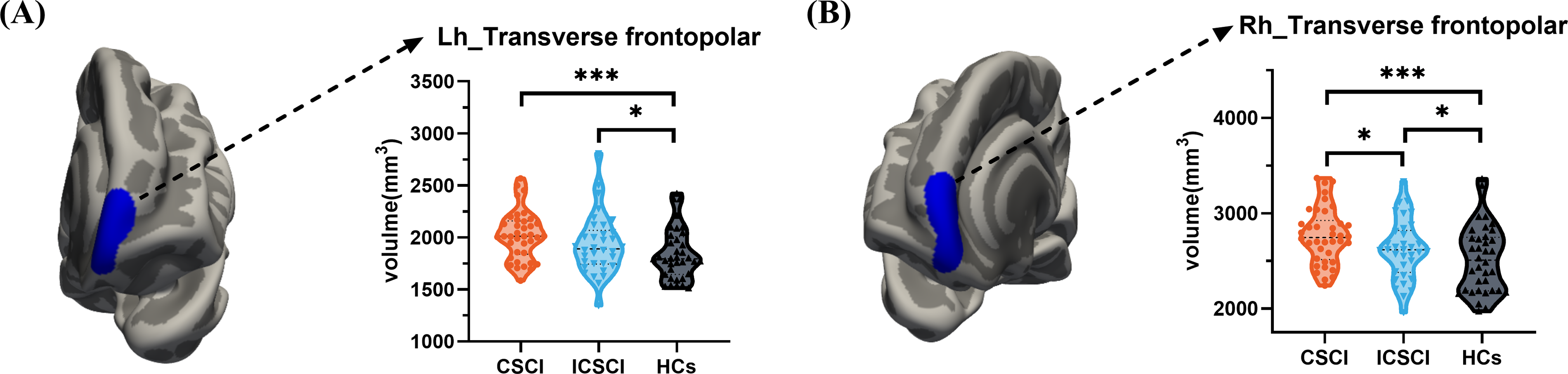
Comparison of cortical volume among the HCs group, ICSCI group, and CSCI group.
Post Hoc Pairwise Comparisons for Cortical Metrics Between CSCI, ICSCI, and HCs
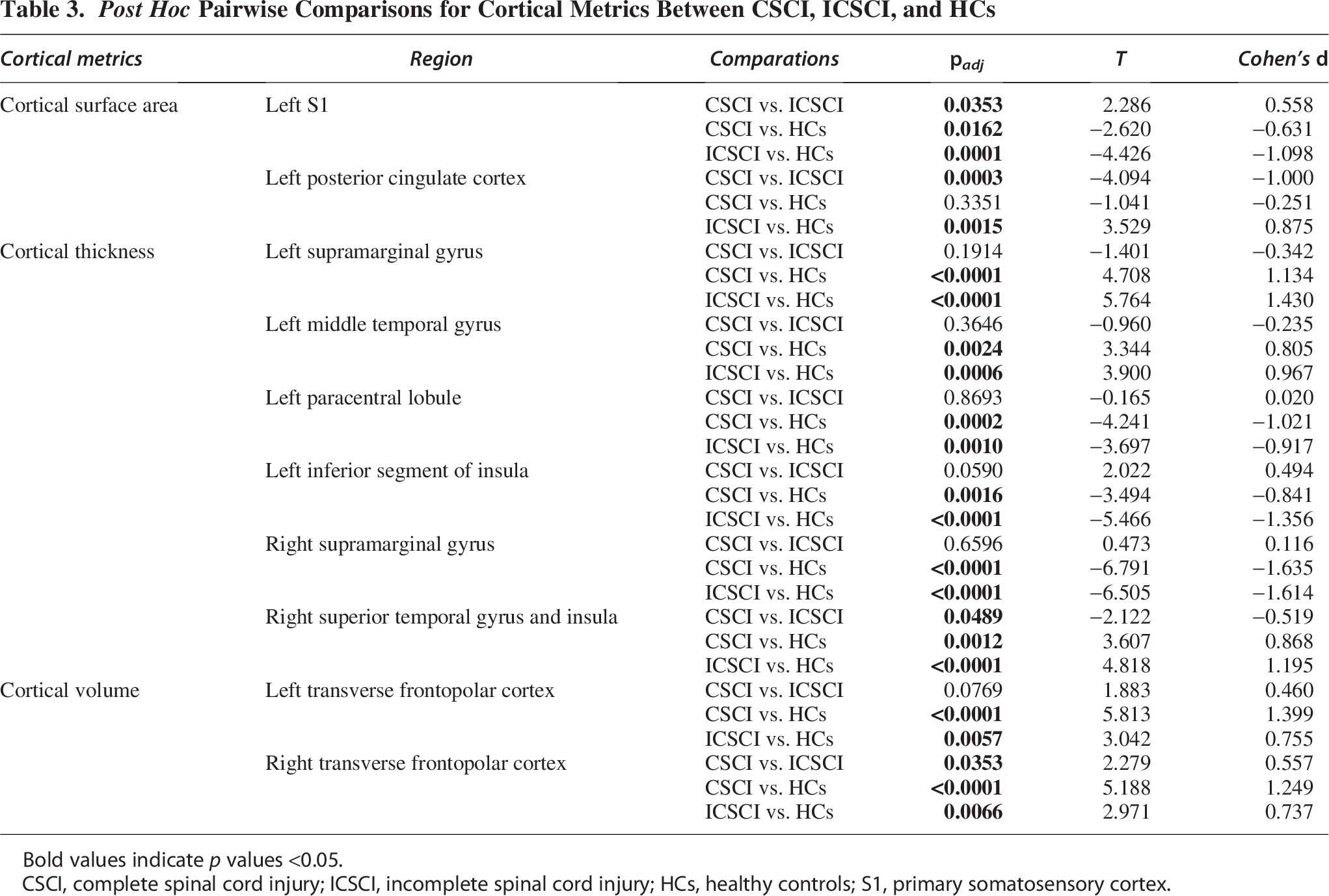
Bold values indicate p values <0.05.
CSCI, complete spinal cord injury; ICSCI, incomplete spinal cord injury; HCs, healthy controls; S1, primary somatosensory cortex.
No significant differences in cortical curvature metrics were observed among the CSCI, ICSCI, and HCs groups.
Correlation analysis between cortical metrics and clinical performance
Among all pediatric SCI patients, cortical surface area in the left PCC was positively correlated with sensory scores (p = 0.036, r = 0.254; Fig. 4A). In the ICSCI subgroup, cortical volume in the right transverse frontopolar cortex was positively correlated with both motor (p = 0.013, r = 0.434; Fig. 4B) and sensory scores (p = 0.030, r = 0.385; Fig. 4C). No other significant associations between cortical metrics and clinical performance were identified.
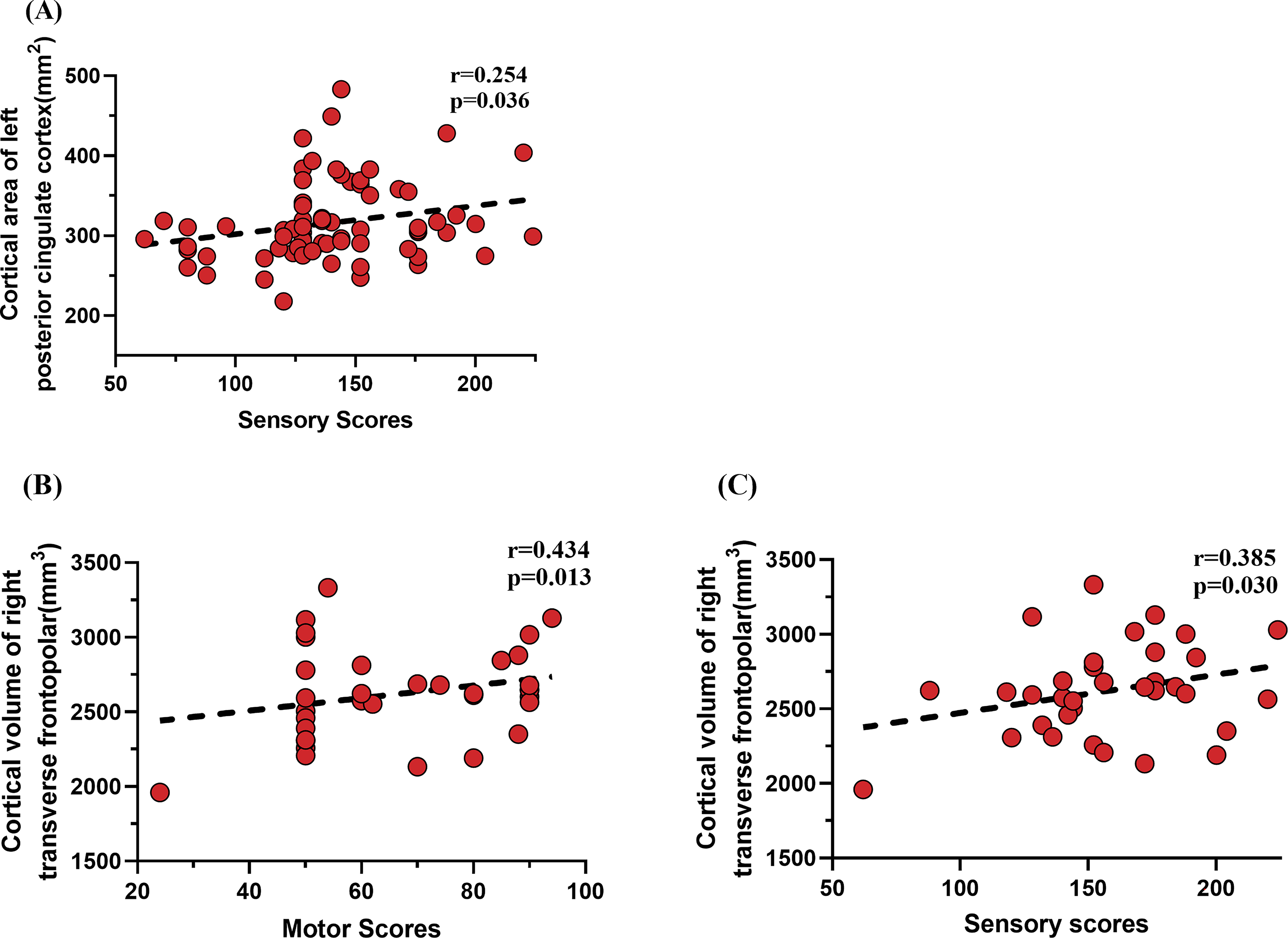
Correlations between cortical morphology metrics and sensory or motor scores in CSCI and ICSCI patients.
ROC analysis between CSCI and ICSCI patients
As shown in Figure 5 and Table 4, cortical surface area in the left S1 and PCC, cortical thickness in the right SMG, and cortical volume in the right transverse frontopolar cortex demonstrated diagnostic value for distinguishing pediatric CSCI from ICSCI patients. When combining all four metrics, the classification model yielded a sensitivity of 61.8%, specificity of 89.5%, and an area under the curve (AUC) of 0.7980 (p < 0.0001, 95% confidence interval [CI]: 0.695–0.901). Using the surface area of the left S1 alone, the model achieved a sensitivity of 58.8%, specificity of 78.9%, and AUC of 0.6223 (p = 0.0747, 95% CI: 0.490–0.755). With the surface area of the left PCC, sensitivity was 41.2%, specificity was 92.1%, and AUC was 0.6935 (p = 0.0048, 95% CI: 0.571–0.816). The cortical thickness of the right SMG yielded a sensitivity of 29.4%, specificity of 86.8%, and AUC of 0.5635 (p = 0.3550, 95% CI: 0.430–0.697). For the cortical volume of the right transverse frontopolar cortex, sensitivity was 70.6%, specificity was 68.4%, and AUC was 0.6447.
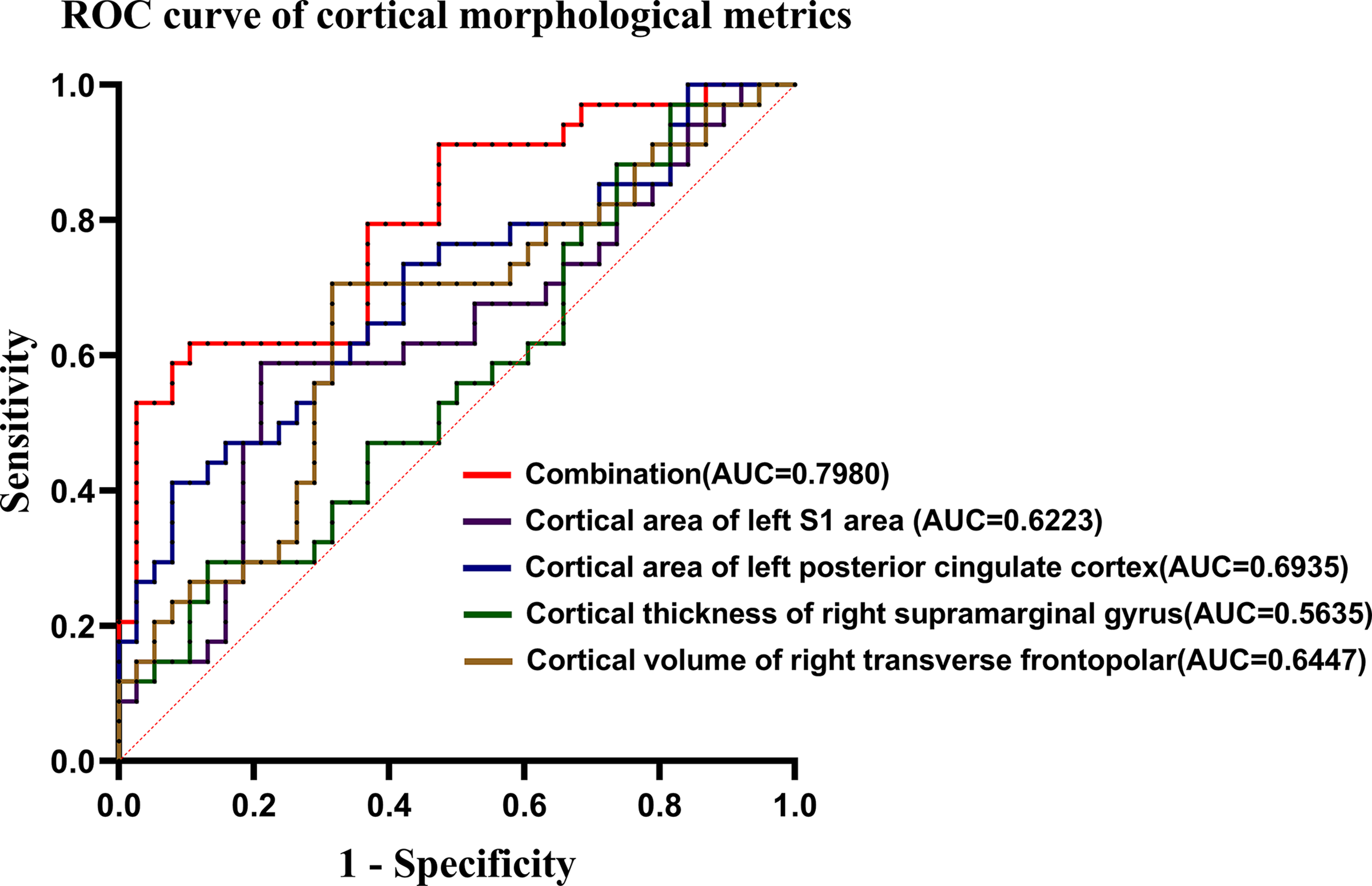
ROC curve analysis between CSCI and ICSCI patients of the cortical morphological metrics. ROC, receiver operating characteristic; CSCI, complete spinal cord injury; ICSCI, incomplete spinal cord injury; AUC, area under the curve; S1, primary somatosensory cortex.
ROC Analysis Between CSCI and ICSCI Patient
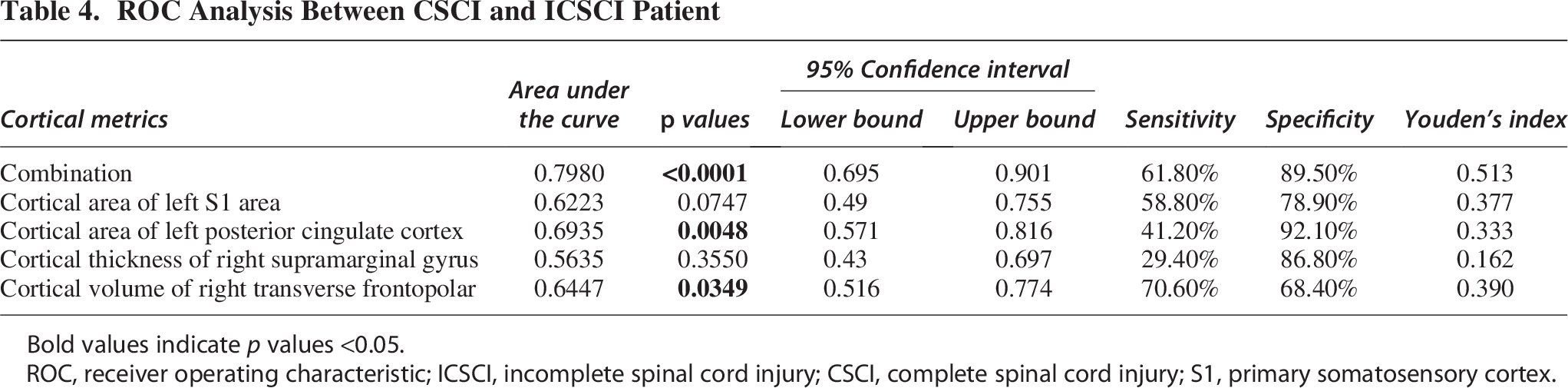
Bold values indicate p values <0.05.
ROC, receiver operating characteristic; ICSCI, incomplete spinal cord injury; CSCI, complete spinal cord injury; S1, primary somatosensory cortex.
Discussion
This study identified both shared and distinct patterns of cortical reorganization. Compared with HCs, CSCI patients showed reduced surface area in the left S1, while ICSCI patients exhibited reductions in S1 and increases in the left PCC. In addition, ICSCI patients had lower surface area in the left S1 and higher surface area in the left PCC than CSCI patients. Both groups demonstrated increased cortical thickness in the bilateral SMG and left MTG, along with decreased thickness in the left PAL, left inferior insular segment, and right STG. ICSCI patients also showed greater thickness in the right SMG compared with CSCI patients. In terms of cortical volume, both groups exhibited increases in the bilateral transverse frontopolar cortices, although the right side was smaller in ICSCI than in CSCI. These findings provide insights into cortical reorganization mechanisms and offer important targets for rehabilitation strategies and therapeutic interventions.
Group differences in cortical morphometric metrics
During typical childhood and adolescent development, cortical surface area expands initially and then stabilizes, a process driven by subcortical myelination, synaptic pruning, and dendritic remodeling.1,30 This trajectory reflects the progressive maturation of cortical structure and function. In our study, both CSCI and ICSCI patients exhibited significant reductions in the surface area of the left S1, suggesting developmental arrest or premature atrophy in this region due to impaired sensory input. Such alterations may reflect reduced synaptic activity and compromised cortical plasticity, deviating from the typical trajectory of organized cortical remodeling. 31 Notably, compared with CSCI patients, ICSCI patients exhibited a more pronounced reduction in S1 surface area, indicating that residual but unstable sensory input may not provide adequate stimulation, potentially leading to maladaptive cortical reorganization. Specifically, we speculate that such irregular sensory inputs may disrupt effective synaptic integration and promote maladaptive remodeling, thereby accelerating structural degeneration. This pathological pattern diverges from normative pruning processes, suggesting that ICSCI may induce a chaotic form of cortical restructuring. 32 Therefore, in clinical rehabilitation, emphasis should be placed on providing ICSCI patients with consistent and high-quality sensory input to support functional reactivation and prevent further structural deterioration in the S1 region.
In addition, our findings revealed significantly increased surface area in the left PCC in ICSCI patients. As a key hub for higher-order cognitive functions such as executive control, memory, and spatial processing, the PCC undergoes substantial structural remodeling during adolescence. 33 The observed expansion in ICSCI patients may reflect compensatory adaptations to partial disruption of somatosensory pathways. In contrast, complete deafferentation in CSCI patients likely prevents effective PCC engagement, whereas persistent activation of residual pathways in ICSCI may drive PCC involvement in sensory-cognitive integration, resulting in its structural reorganization. Given prior evidence of attention and executive function impairments in adult SCI patients, PCC expansion in ICSCI patients may represent a neurodevelopmental risk for long-term cognitive impairment, necessitating longitudinal investigation. 34
In terms of cortical thickness, typically developing children are characterized by progressive thinning, particularly along a temporal gradient from primary sensory to higher-order association cortices, paralleling reorganization of dendritic arbor and pericortical myelination.3,4 However, both CSCI and ICSCI patients in our cohort exhibited increased cortical thickness in the bilateral SMG and the left MTG. As part of the secondary sensory cortex, the SMG is involved not only in processing tactile and painful stimuli but also in higher cognitive functions like working memory and language processing.35,36 In contrast, the MTG is implicated in semantic comprehension and socioemotional processing.37,38 In the context of diminished sensorimotor input, these areas may undergo compensatory engagement, reflected in structural thickening. Supporting this, previous voxel-based morphometry studies in pediatric SCI patients have reported increased GMV in the SMG, suggesting compensatory neuroplasticity. 39 Moreover, our data showed that ICSCI patients demonstrated greater thickening in the right SMG than CSCI patients, potentially reflecting enhanced plastic activation afforded by partially preserved sensorimotor pathways.
Conversely, some regions exhibited cortical thinning, including the left PAL, right STG, and bilateral insula. The PAL plays a critical role in lower limb motor control and bladder function. 40 Its atrophy may reflect disuse-related degeneration secondary to prolonged motor and sensory deafferentation. However, a prior functional MRI study has demonstrated significantly enhanced activation of this region during motor imagery tasks in children with CSCI, suggesting retained plastic potential. 41 Based on these findings, this dissociation between structural atrophy and functional preservation of PAL highlights its potential as a therapeutic target for rTMS to promote functional recovery. Cortical thinning in the STG was also observed in our study and aligns with previous surface-based morphometry findings in pediatric CSCI. 20 Given its role in semantic processing and social cognition, this change may be the neural basis for difficulties in language, interpersonal communication, and emotion regulation.42,43 Atrophy in the bilateral insular cortices may further indicate compromised interoceptive awareness and autonomic integration, impairing children’s ability to process internal bodily states and emotional cues. 44 These structural alterations carry meaningful implications for rehabilitation: regions with cortical thickening likely reflect compensatory potential and may benefit from targeted cognitive training (e.g., language comprehension, social inference), while thinning regions indicate potential functional vulnerability and should be addressed with early interventions.
Regarding cortical volume, both CSCI and ICSCI patients exhibited significantly increased cortical volume in the bilateral transverse frontopolar cortex, with a more pronounced right-sided increase in the CSCI group. This region is a critical node within the prefrontal cortex, supporting high-level cognitive functions such as decision-making, social reasoning, and executive control.45,46 In normative development, cortical volume tends to decrease nonlinearly with age during childhood, reflecting refinement of neural circuitry.2,5 Thus, increased cortical volume in pediatric SCI may represent an aberrant remodeling process triggered by injury-related functional demands. Specifically, compared with ICSCI, the complete loss of sensory input in CSCI patients may lead to greater reliance on the frontopolar cortex for environmental monitoring and cognitive regulation, driving more extensive compensatory hypertrophy. Notably, prior animal research has shown that SCI activates astrocytes and microglia in the prefrontal cortex, suggesting a potential link between volume expansion and neuroinflammatory responses. 18 Therefore, the volumetric increase observed in this region may reflect a combination of compensatory and pathological mechanisms. In this context, rehabilitation strategies should closely monitor frontopolar cortical development. Future studies combining multimodal imaging and longitudinal data are needed to elucidate the long-term developmental trajectory of this region and its impact on cognitive outcomes in pediatric SCI.
Correlation analysis between cortical metrics and clinical performance
This study further revealed that specific cortical morphological alterations were significantly associated with clinical sensory and motor function scores, suggesting their potential role in functional compensation following pediatric SCI. First, across all SCI patients, the surface area of the left PCC was positively correlated with sensory scores. This finding indicates that the degree of structural remodeling in this region may reflect the extent of preserved sensory function. However, given the relatively weak correlation observed, this finding should be interpreted with caution, and further studies with larger cohorts are warranted to validate this association. Furthermore, within the ICSCI subgroup, the cortical volume of the right transverse frontopolar cortex showed significant positive correlations with both sensory and motor scores, implying a broader involvement in sensorimotor integration. While this region is primarily associated with advanced cognitive functions—including decision-making, executive regulation, and social cognition—its correlation with functional outcomes suggests a compensatory recruitment of this region in response to partially preserved sensorimotor pathways.45,46 The enhanced structural development may reflect increased demands placed on this region to support remaining sensory and motor functions. By contrast, in CSCI patients, although similar structural alterations were observed in these regions, no significant correlations with sensory or motor scores were found. This may be due to the complete disruption of ascending sensory pathways, limiting the potential for effective central compensatory mechanisms. Consequently, the observed structural changes in CSCI may be more reflective of passive, non-functional degenerative processes rather than active functional reorganization. Taken together, these structure–function correlations highlight the potential utility of specific cortical metrics as objective neuroimaging indicators of recovery potential in pediatric SCI. In future clinical practice, such biomarkers may assist in prognosis evaluation and guide the development of rehabilitation strategies.
Cortical metrics as potential biomarkers for pediatric CSCI and ICSCI patients
Previous studies have demonstrated that structural and functional alterations in the brain and spinal cord can serve as objective biomarkers for pediatric SCI.39,47,48 Building upon this foundation, our study identified cortical morphological metrics with potential diagnostic value in distinguishing pediatric CSCI and ICSCI patients. Specifically, a classification model incorporating four cortical features—the cortical surface area of the left S1 and left PCC, the cortical thickness of the right SMG, and the cortical volume of the right transverse frontopolar cortex—achieved a sensitivity of 61.8%, specificity of 89.5%, and an AUC of 0.7980, indicating good overall diagnostic performance. Notably, evidence suggests that a subset of clinically diagnosed CSCI patients may retain residual somatosensory pathways, indicating the possibility of misclassified ICSCI cases within the chronic CSCI population.49,50 The cortical markers identified in our study may offer a promising avenue for detecting such cases. Early identification of residual sensorimotor function is essential for tailoring individualized rehabilitation strategies and optimizing therapeutic outcomes in pediatric SCI. Nevertheless, large-scale longitudinal studies are warranted to further validate the clinical utility and generalizability of these neuroimaging biomarkers.
Limitations
First, the relatively limited sample size, broad variability in injury duration, and the overrepresentation of female participants—mainly resulting from backbend-related injuries—may have introduced sampling bias and affected the generalizability of our findings. This gender imbalance reflects the epidemiological pattern of backbend-related SCI, where such injuries predominantly affect school-aged girls. Future research should aim for larger, gender-balanced cohorts and more uniform injury durations to enhance reproducibility and external validity. Second, due to the cross-sectional design of this study, we were unable to capture developmental or disease-related changes in brain structure over time. To address this, future studies should adopt longitudinal approaches. Lastly, the absence of cognitive and psychological evaluations is another limitation. In upcoming research, we plan to incorporate assessments such as mini-mental state examination, montreal cognitive assessment, hamilton anxiety scale, and hamilton depression scale to more thoroughly explore the neurobiological mechanisms related to the observed alterations in brain regions.
Conclusion
In conclusion, pediatric CSCI and ICSCI patients exhibit distinct patterns of cortical reorganization in regions involved in sensory, emotional, and cognitive processing. These findings not only deepen our understanding of the neuroplastic mechanisms underlying pediatric SCI but also provide a theoretical foundation for the development of targeted rehabilitation strategies. Several cortical structural features correlated with clinical function underscore biomarker potential, while differential cortical metrics show diagnostic value for classification and treatment planning.
Transparency, Rigor, and Reproducibility Summary
The study received ethical approval from the Ethics Committee of Xuanwu Hospital, Capital Medical University (Ethics No: [2021] 241). The analysis plan was preregistered prior to the commencement of data collection. To achieve a statistical power of 90% with an alpha level of 0.05, a target sample size of 84 participants was determined. A total of 112 potential participants were screened, of whom imaging data were successfully obtained and analyzed for 108 individuals. Participants were informed of their imaging results after the completion of all clinical assessments. MRI scans were performed using a 3.0-T Siemens system (Erlangen, Germany) equipped with a 12-channel phased-array head coil. High-resolution structural imaging was conducted using a three-dimensional magnetization-prepared rapid gradient echo (3D-MPRAGE) sequence. Both image acquisition and analysis were conducted by research staff blinded to participants’ clinical characteristics, while clinical outcomes were assessed by team members blinded to imaging results. All imaging hardware and preprocessing software utilized in this study are commercially available. The primary inclusion criteria and outcome measures followed established standards. Replication efforts by the research group are currently ongoing.
Authors’ Contributions
Conceptualization: B.Y., L.W., and N.C. Data collection: B.Y., L.W., Y.W., H.X., X.G., J.D., Y.H., and L.W. Formal analysis: B.Y. Funding acquisition: N.C. Investigation: B.Y., C.S., and X.C. Methodology: B.Y. Project administration: N.C. Resources: J.L. Software: B.Y. Supervision: J.L. Validation: Q.Q., Y.J., and W.Z. Visualization: B.Y. Writing—original draft: B.Y. Writing—review and editing: N.C.
Footnotes
Acknowledgment
The authors thank all the SCI and healthy volunteers who participated in this study.
Author Disclosure Statement
The authors have no conflict of interest to disclose.
Funding Information
This study was supported by the National Key Research and Development Program of China (2023YFF1204104) and the National Natural Science Foundation of China (Nos. 81871339 and 81271556).
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.