
Abstract
Prescribed aerobic exercise is the recommended treatment for athletes with sport-related concussion (SRC) who present with exercise intolerance. A recent randomized controlled trial (RCT) found that higher volumes of aerobic exercise, compared with lower volumes, may not be as efficacious in adolescent females with SRC compared with adolescent males. We reanalyzed data from our previously published randomized controlled trials (RCT) and hypothesized that prescribed aerobic exercise, and not stretching, within 10 days of injury would result in faster recovery after SRC in males compared with females. The first RCT (n = 103) recruited from 2015 to 2018 and the second RCT (n = 115) recruited from 2018 to 2020. Sexes were compared in each RCT, then samples were stratified by sex, and intervention groups were compared using a Log-rank test. There were no significant differences in recovery times between males and females in either RCT, regardless of intervention. When stratified by sex and comparing intervention groups, males in RCT1 who were prescribed aerobic exercise (n = 28) recovered 6 days faster than males prescribed stretching (n = 27, p = 0.004) but there was no significant difference for females (aerobic exercise [n = 24] vs. stretching [n = 24, 3-day difference, p = 0.564]). In RCT2, males prescribed aerobic exercise (n = 39) recovered 8 days faster than the stretching group (n = 34, p = 0.020), whereas there was no significant difference for females (aerobic exercise [n = 22] vs. stretching [n = 20, 3-day difference, p = 0.587]). This reanalysis of prior RCT data revealed that male adolescents after SRC recovered significantly faster by 7–8 days when prescribed aerobic exercise within 10 days of injury, whereas female adolescents had a nonsignificant improvement of 3 days. Future adequately powered studies should account for variability between sexes.
Introduction
Concussions are caused by acceleration, deceleration, and rotational forces to the brain, leading to a broad range of symptoms and limitations in cognitive and physical function. 1 The typical recovery time is within 4 weeks of injury 2 ; however, symptoms can be present for months or years in some patients, referred to as Persisting Symptoms after Concussion (PSaC).3–8 Sport-related concussions (SRC), 9 common among athletic adolescents and young adults, 2 are a public health concern due to their effect on sport, school, and work participation,10,11 and their potential to cause long-term neurological problems. 12
A pathognomonic sign and symptom of SRC in athletes is exercise intolerance, 11 which is defined as the inability to perform exercise to the level expected for an athlete due to worsening of concussion symptoms or excessive fatigue. 13 The recommended treatment for exercise intolerance in athletes after SRC is subsymptom threshold aerobic physical activity/exercise initiated 2–10 days after injury. 14 The strength of this recommendation, based on a comprehensive systematic review by the Concussion In Sport Group (CISG), 14 was rated high according to the Grading of Recommendations, Assessment, Development, and Evaluations criteria. There are multiple methods of prescribing physical activity in patients with SRC, ranging from structured and individualized to more cost-effective and generalizable. 15 Prescribed targeted heart rate (HR) aerobic exercise typically includes identification of the HR threshold (HRt) at the more-than-mild symptom exacerbation point (defined as an increase of ≥3 points from the resting value on a 0–10 point scale) 13 on a graded exertion test. Prescriptions typically recommend at least 20 min of daily aerobic exercise at 80–90% of the HRt. Exercise intensity (HRt) is progressed as tolerated until the patient can exercise at 80% or more of age-appropriate maximum HR without exacerbation of concussion symptoms. 16 This specific method is associated with a mean reduction in recovery time by 4.64 (95% confidence intervals [CI]: 2.59, 6.69) days compared with stretching exercise or strict rest. 14
In a recent trial, Chizuk et al. 17 found that females did not respond as well as males to prescribed high volumes of individualized aerobic exercise. This was unexpected since in our previously published randomized controlled trials (RCTs), which are reanalyzed in the present article, we found that sex was not a significant modifier of treatment effect.18,19 These RCTs were used to develop the international guidelines that recommend prescribed early aerobic exercise for facilitating recovery from SRC. 14 The first RCT 19 assessed the effectiveness of prescribed aerobic exercise versus stretching exercise for adolescent recovery from SRC. The second RCT 18 was a replication of the first RCT, where the efficacy, safety, generalizability, and objective adherence to prescribed aerobic exercise in adolescents with SRC were validated. Since these RCTs evaluated aerobic exercise as a novel treatment for SRC, they were not powered for potential sex differences in treatment response. Hence, the purpose of this study was to reanalyze our prior data, stratify by sex, and determine whether recovery times and incidence of PSaC differed for adolescent males and females prescribed aerobic or stretching exercise after SRC. We hypothesized that there would be significant improvement in recovery time and incidence of PSaC in males and females prescribed aerobic exercise when compared with stretching.
Methods
This reanalysis was considered nonhuman subjects research and was approved by the authors’ Institutional Review Board. Deidentified data from both our previous trials (RCT1 19 and RCT2 18 ) were available to the senior author (M.N.H.). RCT1 was recruited from 2015 to 2018 and included 103 participants (48 [46.6%] females), all of which were included in the reanalysis. RCT2 recruited 118 participants (44 [38.3%] females) from 2018 to 2020; 115 participants were included in the reanalysis due to withdrawn consent (n = 2) and a second head injury during the trial (n = 1). In both trials, adolescent athletes (aged 13–18) within 10 days of physician-diagnosed SRC were recruited and randomized to prescribed aerobic exercise or to placebo-like stretching exercise. Recruitment occurred at four university-based outpatient sports medicine practices in RCT1 and at three community- and hospital-affiliated concussion centers in RCT2. Diagnosis of SRC was based on criteria from the 5th Concussion in Sport Group. 3 In both trials, participants were excluded if: the current injury was more severe than a mild traumatic brain injury, they had a history of three or more diagnosed SRC, were still experiencing self-reported impairments from a prior SRC, had a history of moderate-to-severe brain injury, or they were taking medications that affected cardiac autonomic function, such as stimulants or beta-blockers. Participants reported their symptoms daily for up to 4 weeks since injury and were seen weekly by a study physician.
Summary of RCT1 and RCT2 methodology (previously published)18,19
The Buffalo Concussion Treadmill Test (BCTT) was used to identify the HRt in both trials. Aerobic exercise group participants were instructed to perform aerobic exercise (walking, jogging, stationary cycling) at 80% of their HRt for 20 min/day in RCT1 and at 90% of their HRt for at least 20 min/day in RCT2. Participants randomized to the placebo arm in both trials were instructed to perform a progressively increasing stretching program designed to not to elevate the HR. Completion of at-home exercise sessions was recorded, but no information about symptom changes due to exercise was collected. Details of trial procedures and methods are in the RCT’s published manuscripts.18,19
Outcome measures
The main outcome measures from the previously published RCTs reanalyzed here are recovery times and incidence of PSaC. Recovery, determined by blinded study physicians in both RCTs, was defined as normal exercise tolerance on the BCTT, a return to a preinjury symptom level, and a normal physical examination.18,19 Recovery time was the number of days from injury to recovery. RCT1 participants were classified as having delayed recovery, PSaC, if they took 30 days or more to recover, whereas RCT2 defined PSaC as 28 days or more since injury.18,19 The difference is because the 4th CISG guidelines defined PSaC as > 1 month whereas the 5th guidelines defined PSaC as >4 weeks in children and adolescents. 3 To perform the reanalysis, the definition of PSaC needed to be consistent, so the senior author (M.N.H.) aligned the definition of PSaC in RCT1 to be consistent with RCT2.
Re-analysis for current study
First, Kaplan Meier survival curves were created up to 28 days for each RCT, and males and females were then compared using a Log-rank test. Data from the RCTs were then separately analyzed. Each RCT was stratified by participant sex to compare aerobic exercise and stretching. Kaplan Meier survival curves were compared using a Log-rank test. Chi-squared tests were used to compare proportions of PSaC in males versus females within and between intervention groups (Fisher’s Exact test for sample sizes <5). Post-hoc power calculations were performed for the Log-rank test comparing males and females without stratification. 20 A p value of <0.05 was considered statistically significant and all analyses were performed using SPSS (Version 29, Armonk, NY).
Results
Table 1 presents the sample characteristics for each RCT stratified by sex. All participants from the RCTs were included in the reanalysis (RCT1 = 103, RCT2 = 115). In RCT1, males prescribed stretching had significantly more abnormal smooth pursuit signs and symptoms compared to males prescribed aerobic exercise. There were no other significant differences. In RCT2, males in the stretching group took on average 1 day longer to come to the clinic compared to males in the aerobic exercise group. Females prescribed stretching also presented with significantly more signs and symptoms on the vestibulo-ocular reflex compared with those prescribed aerobic exercise. No other demographic or sample differences were present in RCT2.
Sample Demographics by RCT and Sex
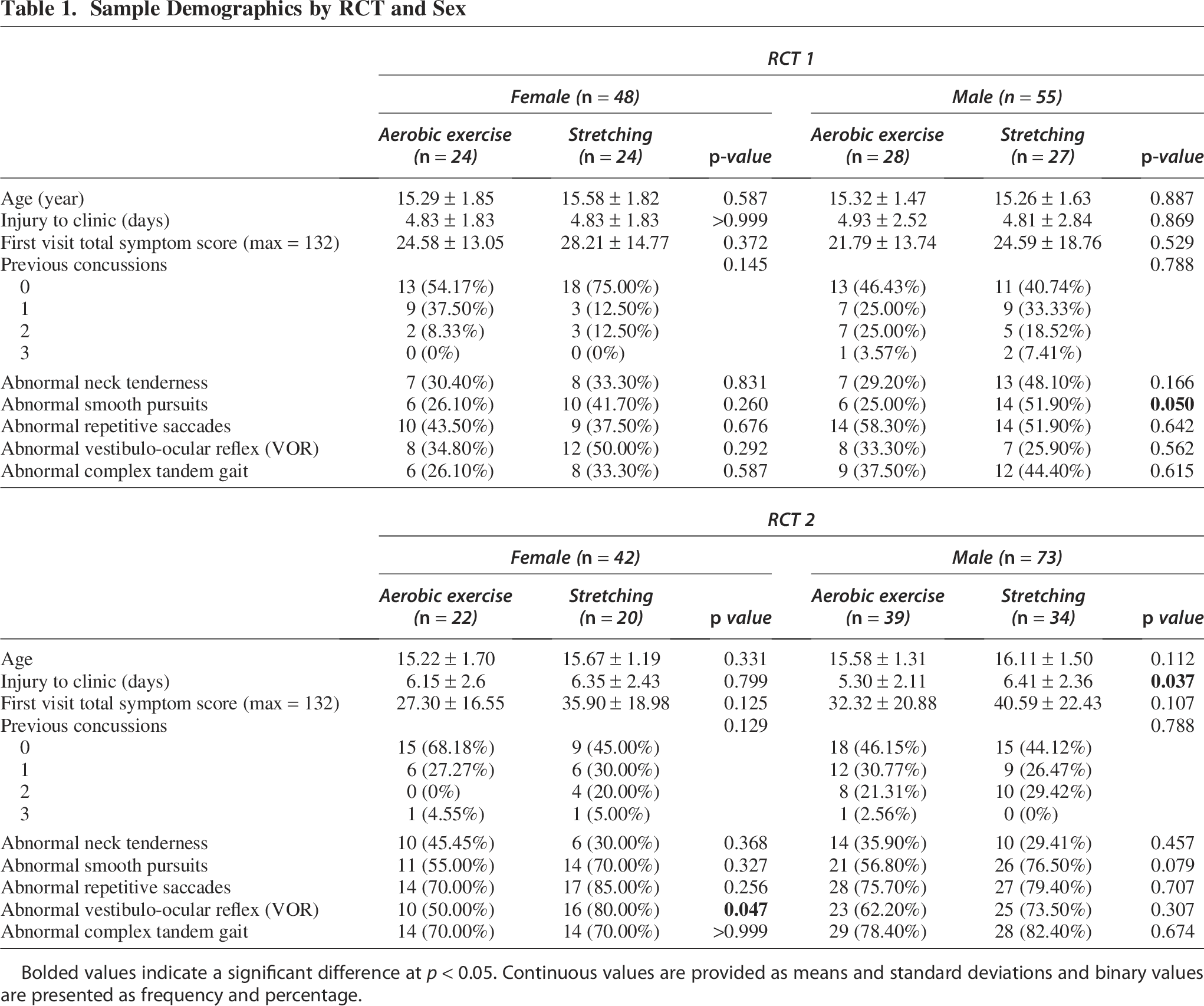
Bolded values indicate a significant difference at p < 0.05. Continuous values are provided as means and standard deviations and binary values are presented as frequency and percentage.
Figure 1 compares the sexes in each RCT regardless of intervention. In RCT1, there was no significant difference in time to recovery between males (14 days) and females (15 days) (p = 0.950, post-hoc power <1%). In RCT2, there was also no significant difference in time to recovery between males (18 days) and females (19 days) (p = 0.948, post-hoc power <1%).
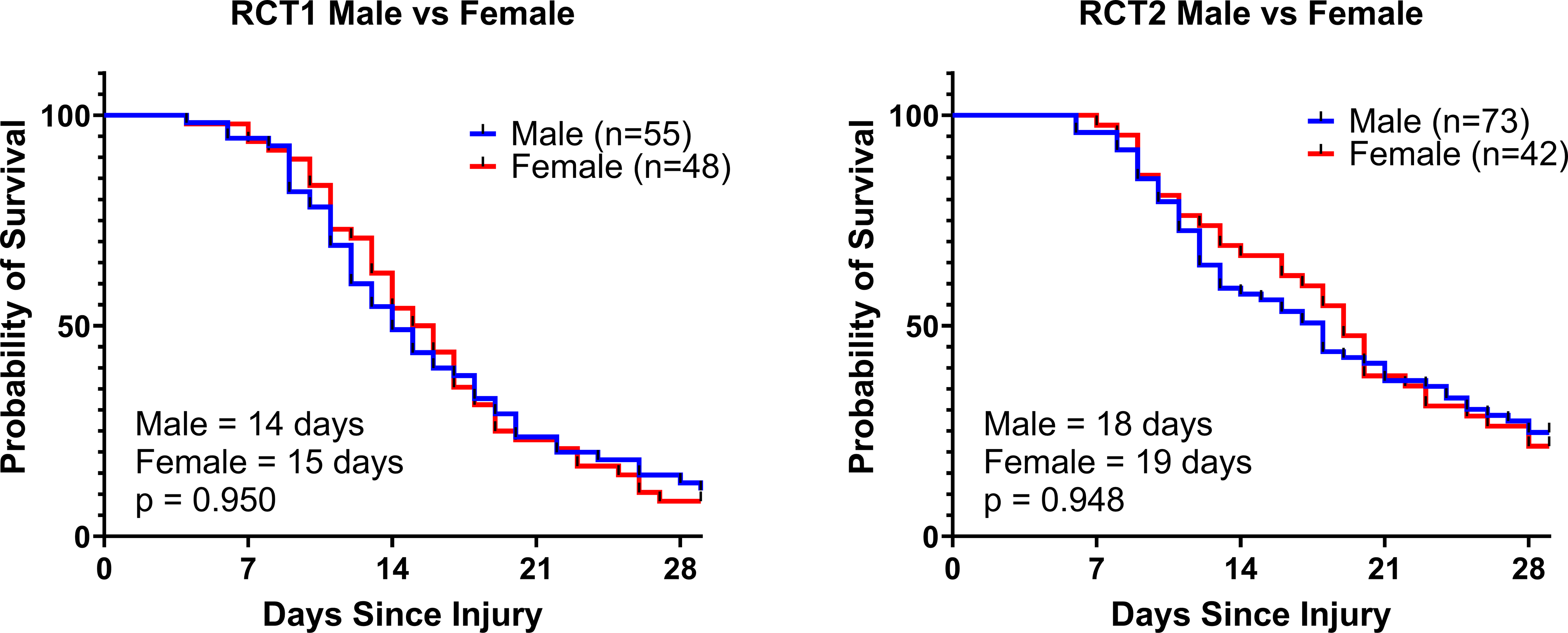
Survival curves comparing recovery times (days) between the sexes, regardless of intervention, for RCT1 and RCT2, respectively. RCT, randomized controlled trial.
Figure 2 presents results stratified by sex for RCT1 only. Previous RCT1 19 results reported a median recovery time of 13 days for aerobic exercise versus 17 days for stretching (Log-rank = 0.010). The reanalysis showed that males prescribed aerobic exercise recovered significantly faster than males prescribed stretching (6-day difference, p = 0.004), but there was no significant difference in recovery for females (3-day difference, p = 0.564, post-hoc power <1%).

Survival curves comparing recovery times (days) for RCT1. Intervention groups are compared within females and males, respectively.
Figure 3 presents results stratified by sex for RCT2 only. Previous RCT2 18 results reported a median recovery time of 14 days for the aerobic exercise group versus 19 days for the stretching group (p = 0.039) on a Cox Proportional Hazard model after controlling for site (p < 0.001) and sex (p = 0.854). The reanalysis showed that males prescribed aerobic exercise recovered 7 days faster relative to the placebo stretching group (p = 0.020), whereas females did not have a significant difference in recovery time (3-day difference, p = 0.587, post-hoc power < 1%).
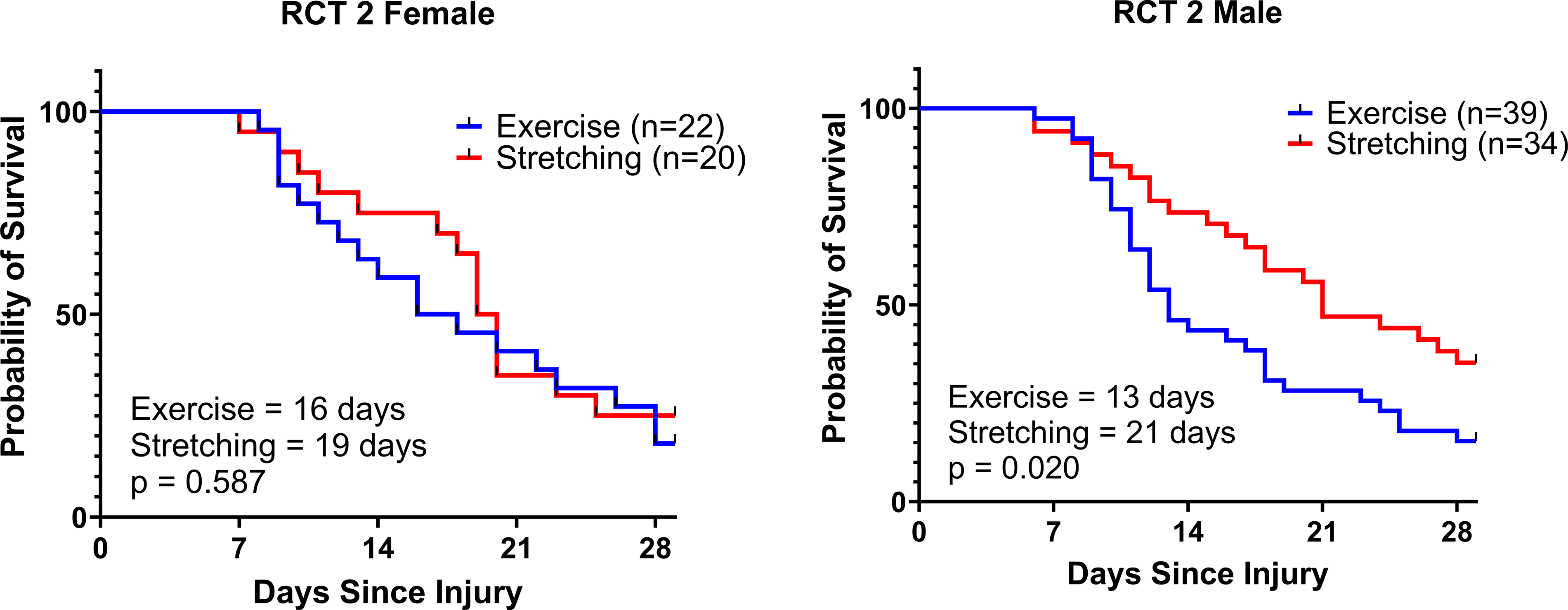
Survival curves comparing recovery times (days) for RCT2. Intervention groups are compared within females and males, respectively.
Table 2 shows the proportions of PSaC for each RCT stratified by sex and intervention group. For RCT1, when comparing between the sexes for each intervention group, males had a significant difference in PSaC proportion between the exercise and stretching groups (0/28 vs. 6/27, p = 0.010). Females in RCT1 did not have a significant difference in PSaC proportion between intervention groups (p ≥ 0.999). In RCT1, when comparing between intervention groups within the sexes, there was no significant difference in PSaC proportions between the sexes for the exercise or stretching interventions (p = 0.208, 0.255, respectively). For RCT2, when comparing between the sexes for each intervention group, males showed a significant difference in PSaC proportions between intervention groups (6/39 vs. 12/34, p = 0.049). Females showed no significant difference (p = 0.714). When comparing between intervention groups within the sexes for RCT2, there was no significant difference in PSaC proportions between the sexes for either intervention group (p ≥ 0.999, 0.549, respectively).
Proportion of PSaC by RCT and Sex
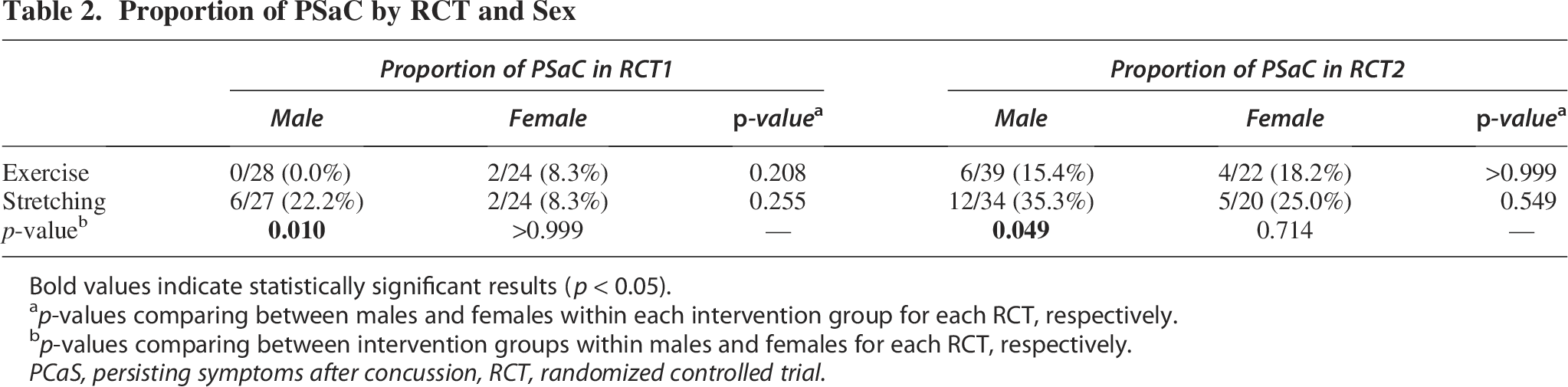
Bold values indicate statistically significant results (p < 0.05).
ap-values comparing between males and females within each intervention group for each RCT, respectively.
bp-values comparing between intervention groups within males and females for each RCT, respectively.
PCaS, persisting symptoms after concussion, RCT, randomized controlled trial.
Discussion
This reanalysis of two RCTs showed that while the current standard of care for SRC, prescribed early aerobic exercise, is very effective for adolescent males, it may not be as effective for females. In RCT1, males who performed early aerobic exercise recovered significantly faster (6 days) when compared with those who did stretching exercise. Similarly, males in the aerobic exercise group in RCT2 recovered 8 days faster than those in the stretching group. Females in both RCTs, however, showed no significant differences between the exercise and stretching groups, despite an average improvement of 3 days for the exercise group. This suggests that aerobic exercise is effective for females, but to a lesser degree as for males. Proportions of PSaC were significantly higher in the male stretching group compared with the exercise group, whereas there were no between-group differences for the females. Participants in RCT2 had higher rates of PSaC compared with RCT1. RCT2 recruited from three community- and hospital-affiliated concussion centers to validate the generalizability of aerobic exercise as a treatment for SRC, whereas RCT1 recruited from 4 university-based outpatient sports medicine practices. 18 The difference in PSaC incidence was likely due to the varying injury severities in RCT2. Participants in RCT2 who were treated at hospital-affiliated sites had longer recovery times and a higher incidence of PSaC compared with those treated at community concussion centers. 18
Our reanalysis suggests that prescribed early aerobic exercise is more effective for males after SRC, in accordance with current CISG guidelines. This finding was consistent across both RCTs. Furthermore, males in the stretching group of both RCTs had significantly higher rates of PSaC compared with males in the exercise groups. The data suggest that stretching or relative rest for males after SRC is detrimental to optimal recovery, and that prescribed early aerobic exercise treatment is effective for facilitating recovery and, importantly, for preventing PSaC. Reducing PSaC incidence is critical since it is associated with impaired school and athletic performance and reduced quality of life in adolescents.21,22 Conversely, females did not show any statistically significant difference in recovery duration when prescribed aerobic versus stretching exercise. Nevertheless, females in the exercise groups recovered on average 3 days faster than those who performed stretching. Prior work has shown that timely intervention (e.g., early access to specialty care) improves recovery in a range from 3 to 6 days. 23 Thus, a 3-day improvement in recovery may be clinically important even though it did not reach statistical significance. 2
A possible explanation for our results may be the structure of the exercise prescription. We have shown that females have higher resting HRs (5 beats per minute [bpm]) and higher exercise test HRts (7 bpm) when compared with males. 24 The exercise prescription methodology in both RCTs used a standardized percentage of HRt. Since females have higher HRts on exertion testing compared to males, they are therefore prescribed higher absolute training intensities. The effect of the greater absolute training intensity on female recovery after SRC was corroborated by data from Chizuk et al. 17 Their study used a prescription intensity of 90% of the individual’s HRt. 88% of exercise-intolerant females with SRC had to stop an at-home exercise session on 1 or more days due to more-than-mild symptom exacerbation versus only 17% of males. Symptom exacerbation that stopped aerobic exercise treatment in females may be from increased intensity, which would reduce the efficacy of prescribed early exercise treatment. Current evidence is insufficient to recommend a modified exercise prescription for females in clinical practice. Nonetheless, future trials should consider exploring alternative exercise prescriptions such as lower intensity and/or longer duration for females within 10 days of SRC.
To better understand why the sex effect of aerobic exercise response after SRC has not been reported before, we reviewed studies used in the CISG position statement that prescribed exercise for SRC. The studies that examined aerobic exercise for SRC did not identify sex differences either because their sample sizes were too small, 25 there was an unequal sex distribution,25–28 or the study did not include females.29,30 Apart from the studies used to generate the 2023 CISG guidelines, two other studies31,32 that assessed the effect of physical activity on recovery from SRC also found no sex differences. Lawrence et al, 31 found no differences in recovery time between sexes and provided hazard ratios with 95% CI (return to sport = 0.83 [0.59, 1.17], p = 0.283, return to school/work = 1.20 [0.68, 2.11], p = 0.639) indicating no directional trend. Stumph et al. 32 found aerobic exercise was associated with longer recovery times in males from initial visit to symptom resolution compared with males who were prescribed rest; however, there was no difference in recovery time for females. It is important to note that both studies were retrospective, which may be limited by missing data, confounders, selection bias, and recall bias.33,34 Ultimately, our data suggest that it will be critical for future research to carefully address sex as a biological variable in studies that assess aerobic exercise as treatment for concussion.
Despite its strengths, this study has limitations. This re-analysis may not apply to other populations. Sample sizes for direct male versus female comparisons were limited, resulting in reduced statistical power to detect sex effects. Post-hoc power calculations indicated that these sex-based log-rank comparisons were underpowered (<1% power). Specifically, this implies a high risk of Type II error; therefore, null findings should be interpreted with caution and larger sample sizes will be required to find statistically significant differences. The original trials did not collect menstrual cycle data; therefore, these sex differences cannot be studied in association to hormonal changes. Finally, this re-analysis is exploratory and motivated by other recent data; future randomized controlled and adequately powered trials are needed to validate these results. Future studies should also investigate sex-specific exercise prescriptions for females to determine if indeed it is exercise intensity or some other variable that moderates the effectiveness of the intervention.
Conclusion
When stratified by sex, this re-analysis of prior RCT data revealed that male adolescents recovered significantly faster by 7–8 days when prescribed aerobic exercise treatment within 2–10 days of SRC relative to stretching exercise. Female adolescents prescribed aerobic exercise treatment, although they recovered as quickly as males, recovered only 3-days faster when compared with females who performed stretching exercise, which did not reach statistical significance. Males prescribed stretching exercise had higher rates of PSaC compared with aerobic exercise, indicating that controlled early aerobic exercise treatment is extremely important for preventing the prolonged recovery that is so detrimental to adolescent health and function. Females prescribed controlled early aerobic exercise treatment had a clinically, although not statistically significant, beneficial effect on recovery but did not have a significant difference in PSaC rates versus stretching exercise. Our findings suggest that early aerobic exercise is a very effective treatment for males after SRC, but while useful, may be less efficacious for females. Future adequately powered studies should be performed to identify optimal exercise prescriptions for females after SRC.
Transparency, Rigor, and Reproducibility
The first RCT was published in 2019 and the second was published in 2021, and the analysis plan and sample size estimation for both were formally preregistered (RCT1: NCT02710123; RCT 2: NCT02959216). The analysis plan for the current reanalysis was not preregistered, but the lead statistician (MNH) confirms that the proposed statistical analysis plan was prespecified. The decision to perform the present study was influenced by the knowledge that males were recovering more quickly with a prescription of aerobic exercise than females, which may be a source of positive results bias.
Authors’ Contributions
E.V.C.: Conceptualization, methodology, formal analysis, writing—original draft, writing—review and editing, and visualization. H.M.C.: Writing—review and editing. E.M.V.: Writing—review and editing. N.A.: Methodology and writing—review and editing. J.J.L.: Conceptualization and writing—review and editing. M.N.H.: Conceptualization, methodology, formal analysis, resources, and writing—original draft.
Footnotes
Author Disclosure Statement
The author(s) have no competing interest to disclose.
Funding Information
Research reported in this publication was supported by the Department of Defense Congressionally Directed Medical Research Program award number TP210003 (J.J.L.). The content is solely the responsibility of the authors and does not necessarily represent the official views of the Department of Defense.