
Abstract
Keywords
Introduction
Despite a worldwide increase in life expectancy, the negative impact of the natural aging process may directly or indirectly affect the individual perception of the quality of additional years of life due to increased longevity. Within this scenario, in addition to traditional data such as morbidity and mortality rates, the monitoring of subjective indicators related to quality of life in older adults has received much attention in public health (Alexandre, Cordeiro, & Ramos, 2009; Chachamovich, Fleck, Laidlaw, & Power, 2008; Hawthorne et al., 2006; Torres, Quezada, Risoseco, & Ducci, 2008). This fact is mainly associated with the notion that a favorable perception of one’s own quality of life may minimize the limitations that accompany the process of aging (Elavsky et al., 2005). Maintaining a high level of quality of life into advanced age is a growing public health concern as the older adult population continues to increase. In fact, nowadays one of the primary goals is to improve both the quality and the number of years of healthy life (Acree et al., 2006).
Literature data suggest that regular physical activity preserve the general health, the vitality, and the social functioning (Blacklock, Rhodes, & Brown, 2007), reduces the risk of the occurrence and development of chronic-degenerative disorders (Bassuk & Manson, 2005), increases the capacity to perform physical work (Puggaard, Larsen, Stovring, & Jeune, 2000), improves the sensation of well-being (McAuley, Elavsky, Jerone, Konapack, & Marques, 2005), and postpones eventual functional and motor disabilities (Vita, Terry, Hubert, & Fries, 1998). Many of these studies were conducted in highly industrialized countries and whether these findings apply to other less developed societies remains to be determined. In addition, due to specific sociocultural and environmental determinants and consequently living in different circumstances, it is questionable whether the magnitude of the association between regular physical activity and a better health status is similar in developing countries such as Brazil. In view of this perspective, public health policies have tried to encourage intervention programs designed to promote a physically active lifestyle to minimize possible outcomes that may compromise quality of life at any age, notably in adults of older age when the risks of insufficient and inadequate physical activity are elevated, thus compromising the years of useful life.
However, data supporting the positive association between a physically active lifestyle and indicators related to quality of life may be hindered by differences in the nature and specifications of the instruments used for data collection (Acree et al., 2006; Aoyagi, Park, Park, & Shephard, 2010; Tessier et al., 2007). As a consequence, specialist groups under the auspices of the World Health Organization have worked since the end of the 1990s on the proposal and dissemination of internationally validated and standardized instruments for the monitoring of physical activity and quality of life. As a result of this effort, the International Physical Activity Questionnaire—IPAQ (Marshall & Baumann, 2001) and the World Health Organization Quality of Life—WHOQol questionnaire (WHOQol, 1998) were intended as common instruments to monitor physical activity and quality of life, respectively, in subjects from different regions of the world. The main characteristic of the two questionnaires is the expectation of cultural and linguistic equivalence in international comparative studies within and between populations.
The purpose of this study was to investigate the association between physical activity and perception of quality of life in a sample of Brazilian older adults using data collected with two internationally recognized and validated instruments (IPAQ and WHOQol-Old). The key research question addressed was “Is the different quality of life perception of older adults associated with the level of physical activity?” It was hypothesized that physically more active older adults would present better quality of life perception than their sedentary peers and that the favorable influence of physical activity on quality of life independent of the impact of sociodemographic variables, such as gender, age, marital status, educational level, and family socioeconomic status.
Method
A descriptive, cross-sectional, population-based study was conducted. Data were collected from September to November 2009. The study protocol was approved by the Ethics Committee of Centro Universitário de União da Vitória and the study was conducted according to guidelines on research involving humans.
Sample and Subject Selection
The reference population for the study included older adults registered at the family health center of the town of União da Vitória, southwestern region of the State of Paraná, Brazil. Older adults who volunteered to participate in the study were selected according to the following criteria: (a) age ≥ 60 years; (b) living with the family in the urban area of the town; (c) independence in activities of daily living; and (d) cognitive ability to respond to the questionnaires, determined by the version translated to Portuguese of the Short-Care (Veras, Coutinho, & Ney Júnior, 1990). For this purpose, all older adults registered at the health center were contacted at home, informed regarding the nature, objectives, and procedures of the study, and invited to participate in the study. A total of 1,204 older adults (645 women and 559 men) agreed to participate in the study by signing the free informed consent form.
Data Collection
Data were collected with an instrument consisting of three sections. The first section comprised sociodemographic data (gender, age, marital status, educational level, and family socioeconomic status). The second section corresponded to the specific module of the WHOQol assessment instrument translated and adapted to Portuguese (Fleck, Chachamovich, & Treintini, 2006), which measures the quality of life perception of older adults (WHOQol-Old). The questionnaire consisted of 24 items divided into six domains, with a 5-point Likert-type response scale: sensory abilities, autonomy, past/present/future activities, social participation, death/dying, and intimacy. In addition to the six specific domains, the WHOQol-Old also includes an additional domain that results from the responses to the set of 24 items (overall quality of life). Originally the WHOQol-Old module translated and adapted to Portuguese showed adequate internal consistency (Cronbach’s coefficients ranging from .71 to .88), discriminate and concurrent validity (correlation coefficients ranging from .50 to .61) and test-retest reliability (correlation coefficients ranging from .58 to .82). The scores of each domain were calculated by a syntax that considers the responses to the group of items of the domain. The final scores obtained for each domain were transformed to a scale ranging from 0 to 100, with zero corresponding to a low perception and 100 to a high perception of the quality of life indicator in each domain (Power, Quinn, Schmidt, & WHOQol-Old, 2005).
The third section consisted of the short version of the IPAQ translated to Portuguese, with the last 7 days as reference period (International Physical Activity Questionnaire [IPAQ], 2005). The four questions of the questionnaire are aimed at obtaining information about the frequency (days/week) and duration (minutes/day) of walks and daily activities that require physical effort of moderate to vigorous intensity, in addition to the time (minutes/day) spent on activities in the sitting position on week days and on the weekend. Physical activity defined as “any bodily movement produced by skeletal muscles that results in energy expenditure above a basal level” (Caspersen, Powell, & Christenson, 1985) was classified into three categories according to the IPAQ consensus group: sedentary (< 600 Met-minutes/week), active (≥ 600 Met-minutes/week), and very active (≥ 3,000 Met-minutes/week).
Two researches administered the instruments individually to the subjects during a home visit. The participants were given instructions and recommendations for completion of the instrument; there were no time limits for completion of the instrument. The researchers clarified any doubt raised by the respondents during data collection. Although the instrument was self-reported, for those subjects with low literacy who could not read (18% of the total sample), the researchers administered the instrument in face-to-face interviews.
Data Analysis
All data were analyzed and reported as group data to maintain the participants’ confidentiality. The data were analyzed statistically using the Statistical Package for the Social Sciences (SPSS), version 17.0. Descriptive statistics was used for sociodemographic characterization by calculating the proportion of distribution in each stratum. Contingency tables were constructed to analyze the proportions of subjects in the three categories of physical activity proposed by the IPAQ (sedentary, active, and very active) and the chi-square (χ2) test was applied to identify significant differences between genders and ages. The results regarding quality of life perception were first compared to a normal distribution by the Kolmogorov–Smirnov distance test. Since the data showed a normal distribution, parametric tests were used and the mean and standard deviation were calculated. Differences between the three categories of physical activity were determined by analysis of covariance (ANCOVA) controlling for age, marital status, educational level, and family socioeconomic status. The Scheffe post hoc multiple comparisons test was used to identify specific differences in the quality of life dimensions. A p ≤ .05 was considered as indicating statistical significance.
Results
This study investigated the association between physical activity and perception of quality of life in a sample of Brazilian older adults using data collected with two internationally recognized and validated instruments (IPAQ and WHOQol-Old). The Table 1 shows the sociodemographic characteristics of the sample studied. Among the 1,204 older adults participating in the study, 53.6% were women, 45.3% ranged in age from 60 to 69 years, and 18.1% were older than 80 years. With respect to marital status, 38.4% of the subjects were married or lived with a partner and 59.1% were widowed or separated. About one third of the subjects (30.9%) went to school for ≤ 4 years, whereas 20.4% had ≥ 9 years of schooling. Regarding family socioeconomic status, 10.4% of the subjects belonged to classes A and B (high socioeconomic level) and 23.5% to classes D and E (low socioeconomic level).
Sociodemographic Characteristics of the Sample Studied

Note: Statistically significant differences between sexes: *p < .05. **p < 0.01.
Analysis of the proportions of subjects classified into the categories of physical activity recommended by IPAQ (Table 2) showed a similar distribution in the two genders although borderline significance indicating a lower proportion of sedentary subjects among men was observed (χ2 = 3.749, p = .0541). In addition, no significant differences were observed between the age classes studied here. However, there was a clear tendency toward an increase in the proportions of sedentary older adults and a concomitant reduction in the proportions of active and very active subjects with age.
Categories of Physical Activity According to Gender and Age in the Sample Studied

Table 3 illustrates the statistical results regarding the perception of quality of life in the sample of older adults according to gender. Although the questionnaire used (WHOQol-Old) has been validated in Brazil, its reliability was evaluated by the analysis of internal consistency of the questions and domains using Cronbach’s alpha coefficient. A coefficient of .846 for questions and of .803 for domains was obtained, suggesting that the instrument showed very good reliability for the identification of quality of life perception in the sample of older adults studied here.
Mean and Standard Deviation of Domain Scores and F Statistics Regarding the Perception of Quality of Life in Brazilian Older Adults Assessed Using the WHOQol-Old Questionnaire
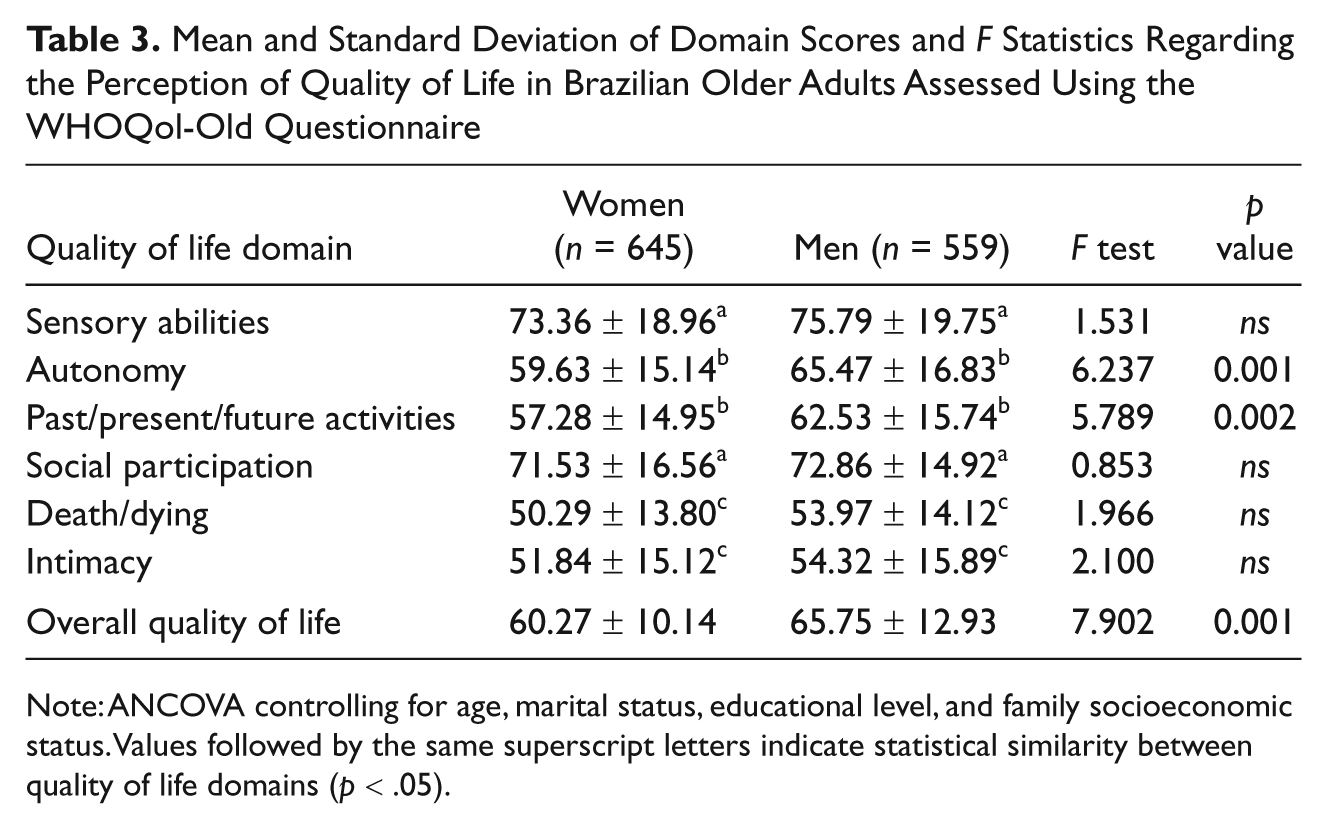
Note: ANCOVA controlling for age, marital status, educational level, and family socioeconomic status. Values followed by the same superscript letters indicate statistical similarity between quality of life domains (p < .05).
Comparison of the two genders showed significant differences in the mean scores for autonomy (F = 6.237, p < .001) and past/present/future activities (F = 5.789, p = .002) in favor of men. With respect to overall quality of life, significant differences were also observed between women and men (F = 7.902, p < .001). The hierarchical organization demonstrated by the magnitude of mean scores obtained for each quality of life domain was similar in the two genders. However, three statistically significant domains could be defined. In this case, the sensory abilities and social participation domains formed a group in which the subjects presented the best aspects related to quality of life perception. The next group consisted of the autonomy and past/present/future activities domains with intermediate scores. The death/dying and intimacy domains received the lowest scores.
Table 4 shows the results of covariance analysis controlling for age, marital status, educational level, and family socioeconomic status, comparing the quality of life domain scores obtained for the older adults studied according to the strata of physical activity. Older adults of both genders who reported to be more physically active attributed higher scores to the sensory ability (women: F = 3.796, p = .028; men: F = 9.486, p < .001), autonomy (women: F = 4.227, p = .017; men: F = 8.237, p < .001), and intimacy domains (women: F = 3.549, p = .020; men: F = 10.114, p < .001), in addition to presenting significantly higher overall quality of life scores (women: F = 4.153, p = .016; men: F = 8.69, p = .001). Specifically in women, the scores obtained for the social participation domain were significantly higher in the strata of active and very active subjects when compared to sedentary subjects (F = 4.535, p = .014). The variation in scores also differed between genders. In men, more marked differences were observed between the very active and sedentary strata, whereas in women larger differences were found between the active and sedentary strata.
Mean and Standard Deviation of Domain Scores and F Statistics Regarding the Perception of Quality of Life in Brazilian Older Adults According to Level of Physical Activity
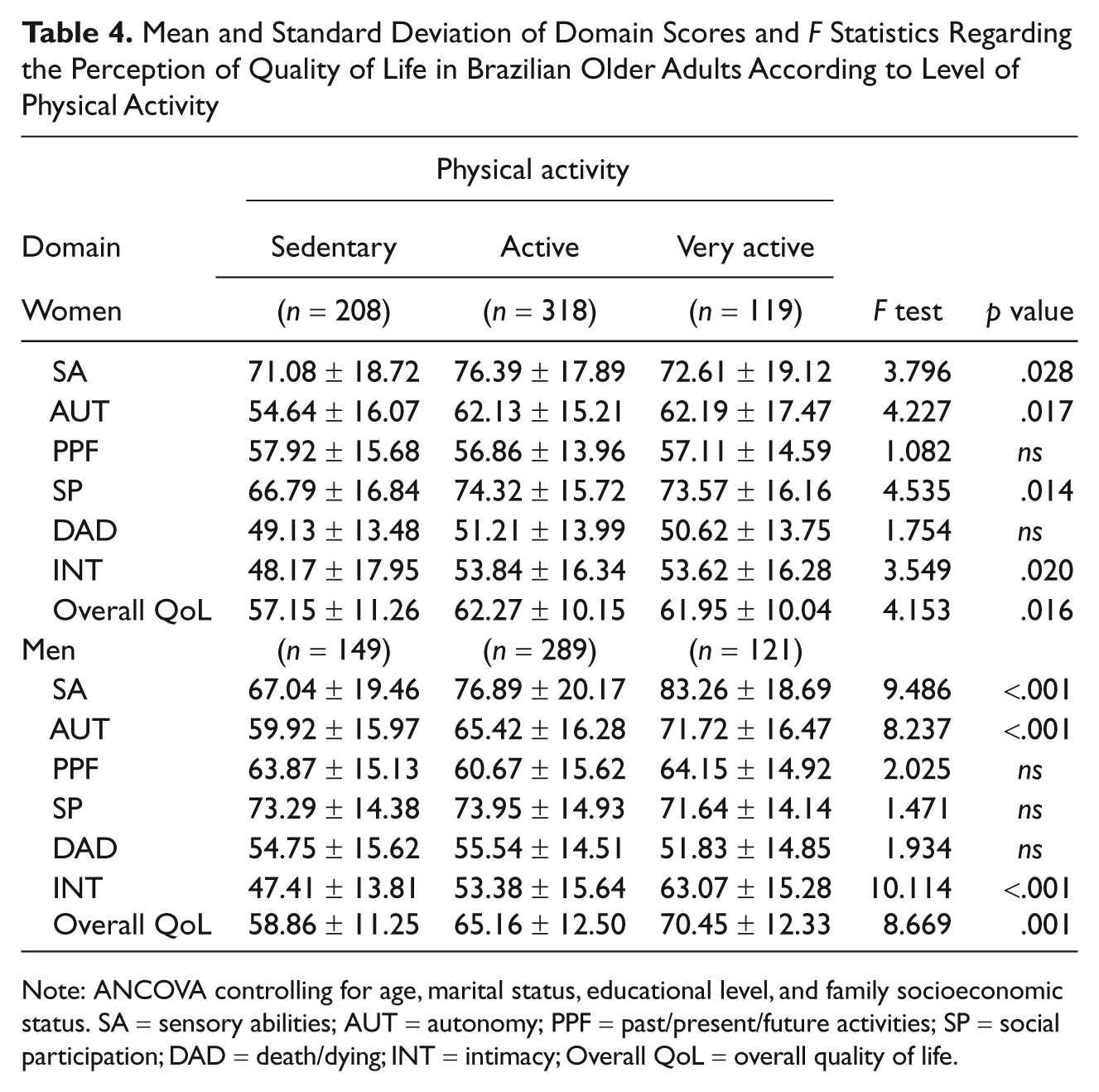
Note: ANCOVA controlling for age, marital status, educational level, and family socioeconomic status. SA = sensory abilities; AUT = autonomy; PPF = past/present/future activities; SP = social participation; DAD = death/dying; INT = intimacy; Overall QoL = overall quality of life.
Discussion
Physical activity (Ainsworth et al., 2006; Bauman et al., 2009; Florindo, Hallal, Moura, & Malta, 2009; Hallal, Victora, Wells, & Lima, 2003; Rütten & Abu-Omar, 2004; Guthold, Ono, Strong, Chatterji, & Morabia, 2008; Siqueira et al., 2008; Varo et al., 2003) and quality of life perception (Alexandre et al., 2009; Chachamovich et al., 2008; Hawthorne et al., 2006; Torres et al., 2008) has been the subject of numerous studies. This marked interest is probably due to the close association of these aspects with the occurrence and development of outcomes that compromise a good health status (Abbott et al., 2004; Florindo et al., 2009; Lee & Paffenbarger, 2000; Nelson et al, 2004; Rabin, Heldt, Hirakata, & Fleck, 2008; Weuve et al., 2004). However, none of these studies has simultaneously employed internationally recognized instruments for the assessment of physical activity and quality of life, a fact impairing generalization of the results due to the specificities of the instruments applied. In addition, studies involving older adults are scarce. To our knowledge, this is the first study conducted on older adults in which two international instruments (IPAQ and WHOQol) were applied simultaneously, a fact permitting more reliable conclusions regarding physical activity and quality of life perception.
Consistent with the findings reported in other studies using the IPAQ and identical criteria for interpretation of the data collected (Ainsworth et al., 2006; Bauman et al., 2009; Florindo et al., 2009; Guthold et al., 2008; Hallal et al., 2003; Rütten & Abu-Omar, 2004; Siqueira et al., 2008; Varo et al., 2003), the present results indicate a similar physical activity behavior in both genders for subjects ≥ 60 years despite a discretely higher proportion of sedentary women. However, in the present sample of older adults the proportion of physical inactivity was lower than that reported in other Brazilian (Florindo et al., 2009; Hallal et al., 2003; Siqueira et al., 2008), North American (Ainsworth et al., 2006) and European (Guthold et al., 2008; Rütten & Abu-Omar, 2004) studies but higher than the proportion found in studies on older adults from different developing countries (Guthold et al., 2008). The reasons for these differences are not completely understood. Methodological differences between studies in terms of sample selection and of the stratification of older adults according to age may explain, in part, the differences identified. In addition, sociocultural, structural, and environmental factors may contribute to the identification of differences in physical activity levels between older adults from different regions of the world.
In the present study, analysis of quality of life perception revealed significant differences between mean scores obtained for the domains of the WHOQol-Old module, a finding demonstrating the multidimensional concept of quality of life and suggesting the separate analysis of each. This tendency agrees with data reported in the multicenter study originally conducted for the development of the WHOQol-Old module domain (Bowling, Banister, Sutton, Evans, & Windsor, 2002) and with other studies investigating quality of life in older adults (Chachamovich et al., 2008; Fleck et al., 2006; Halvorsrud, Kalfoss, & Diseth, 2008).
In contrast, the mean scores obtained for the six quality of life domains in the present study are higher than those reported for a sample of older adults from the northeastern region of Brazil (Torres, Reis, & Fernandes, 2009) but similar to data found for a sample of older adults also from the south region of Brazil (Fleck et al., 2006). In this particular case, evidence suggests that the perception of quality of life is affected by physiological, social, cognitive, and emotional attributes, with aging affecting one or more of these attributes to a greater or lesser extent depending on the context in which the older individual is inserted (Rejeski, Brawley, & Shumaker, 1996). In the case of the present sample, the more advanced regional development observed in the south region of Brazil may have led to a better quality of life of older adults compared to those from the northeastern region of Brazil.
An important finding of the present study was that higher levels of physical activity were associated with higher quality of life scores. However, one may speculate that the favorable influence of physical activity on quality of life might be confused with the concomitant impact of other sociodemographic variables, such as age, marital status, educational level, and family socioeconomic status. Thus, in the present study analysis of covariance was used to control for the impact of these variables. After ruling out the participation of these variables, the present results showed that older adults belonging to more physically active strata presented higher quality of life scores. This finding is consistent with previous studies using other assessment instruments to monitor physical activity and quality of life (Rejeski et al., 1996).
Another finding that deserves discussion is that the gradient of physical activity and quality of life scores followed a specific trend in each gender. In men, marked differences were observed between the very active and sedentary strata, whereas in women this phenomenon was observed between active and sedentary strata. The differences in quality of life scores between physically active and very active women were not analyzed statistically.
The present results also demonstrated that higher levels of physical activity did not equally influence the six quality of life domains proposed in the WHOQol-Old module. If, on one hand, the mean scores obtained for the sensory abilities, autonomy, social participation and intimacy domains were significantly higher among physically active older adults compared to sedentary subjects, on the other, mean scores for the past/present/future activities and death/dying domains did not differ significantly between the three physical activity strata. These findings agree with the results of intervention studies, which demonstrated improvement in the perception of quality of life in domains related to functional capacity, independence, and interpersonal relations when increasing the level of physical activity of older adults by submitting them to systematic physical exercise programs (Carter et al., 2002; King et al., 2000; Mota, Ribeiro, Carvalho, & Matos, 2006; Rocha, Paixão, Tucher, Botaro, & Bruno, 2009).
The results of the present study should be interpreted in view of some limitations. First, the IPAQ is a retrospective instrument of self-recall of daily activities performed in the week preceding its application. Although the psychometric indications of the questionnaire are available and meet the acceptance criteria proposed (Craig et al., 2003), there is the possibility of seasonal influences that may interfere with the identification of physical activity. Second, the reports provided by the older adults of the present sample indicate that self-perception of quality of life reflects individual responses that exclusively depend on attitudes toward different surrounding situations. Thus, since the sample consisted of older adults with a wide diversity of life experiences, the possibility of eventual bias in the interpretation of the questions of the WHOQOL-Old cannot be ruled out. Furthermore, the selected sample comprising only older adults from a specific town in the southwestern region of the State of Paraná, Brazil, which is located in a region with specific social, economic, and cultural characteristics, may weaken the external validity of the study and impair generalization of the results.
In conclusion, the significant finding of the present study was the different quality of life perception of older adults according to the level of physical activity. Physically more active subjects presented better quality of life perception than their sedentary peers, a finding confirming the hypothesis that perception of quality of life is associated with physical activity. Despite methodological difficulties in designing studies with this purpose, a better understanding of the complex dose-response relationship between physical activity and quality of life is important to propose recommendations addressing lifestyle changes in older adults, especially those who are still not affected by debilitating diseases and are physically independent.
Footnotes
Acknowledgements
The authors extend special thanks to staff of the family health center of the town of União da Vitória, Paraná, Brazil, for valuable help in conducting this study, and all study participants for their cooperation.
The authors declared no conflicts of interest with respect to the research, authorship, and/or publication of this article.
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The primary author is supported by Brazilian National Board for Scientific and Technological Development—CNPq (Protocol no. 306361/2007-8).