
Abstract
The size of the older foreign-born population has steadily increased from 2.7 million in 1990 to 4.3 million in 2006, making up 8% of the U.S. older adult population (Leach, 2009). The number is expected to reach 16 million by 2050 (Treas & Batalova, 2007). Within the older foreign-born individuals, heterogeneity exists in terms of their motivations for immigration and postimmigrant experience. Whereas nearly two thirds of older foreign-born individuals have lived in the United States for more than 30 years (Brownell & Fenley, 2009), about 4.4% of older immigrants are new to the United States, with less than 5 years of residence in the United States (Choi, 2006). About 50,000 older adults aged 65 or older were legally admitted to the United States as permanent residents in 2005 (Treas, 2009). The literature classifies these late life immigrants as the invited elderly because most come to the United States to reunite with their naturalized children or siblings. This term contrasts with the immigrated elderly, who immigrated to the United States in their young adulthood and lived out their adult lives in the United States (Min, 1998).
With the increase in the number of older foreign-born individuals in the United States, understanding their health status has become important from public health and service provision perspectives. Among older foreign-born individuals in the United States, health status of late life immigrants has begun to draw much attention from scholars and policy makers as a result of the welfare reform of 1996, which set unprecedented limits on the use of federal Medicaid funds for noncitizen immigrants. This ban has mostly affected newly arrived immigrants because they do not qualify for naturalization during their first 5 years of stay in the United States (3 years among refugees; Legomsky, 2005). The ban against noncitizen immigrants from access to federal Medicaid benefits will remain the same under the recent health care reform (National Immigration Law Center, 2010a). The welfare reform of 1996 has been criticized as having been enacted without sufficient studies of both the health care use and needs of these individuals who were affected by the law, including newly arrived older immigrants (Yoo, 2001). One major debate has dealt with uncertainties regarding the cost effectiveness of delays in federal benefits for newly arrived older immigrants until after they have become naturalized citizens (Ku & Matani, 2001). To answer this question, it is essential to understand the relative health status of newly arrived older immigrants, who constitute the target population in the current study.
Theoretical Framework and Hypotheses
The healthy immigrant effect (HIE) suggests that, on initial arrival, immigrants might be better-off in terms of their health than their U.S.-born counterparts due to voluntary positive selection among immigrants, cultural buffering of native culture, and legal barriers against entry by those in poor health (Akresh & Frank, 2008; Antecol & Bedard, 2006; McDonald & Kennedy, 2004). However, health advantages among new immigrants wind down as their length of residence in the United States increases. The longer the period since their migration, the more the patterns of health and disease tend to resemble those of the native-born population (Dunn & Dyck, 2000). The disappearance of initial health advantages over time among new immigrants has been explained by a process of postimmigration acculturation (e.g., changes in lifestyle and dietary practices), exposure to host country’s environmental factors, and poorer access to health care in the host country (Akresh, 2007; Lara, Gamboa, Kahramanian, Morales, & Bautista, 2005; McDonald & Kennedy, 2004). Even though the HIE and the following convergence of health status among immigrants have been tested and well documented among younger adults, little is known about the HIE and postimmigration health changes among late life immigrants (Gee, Kobayashi, & Prus, 2004).
Health consequences of migration among newly arrived older immigrants may also be understood by means of a competing theoretical framework: the stress-illness model (Friis, Yngve, & Persson, 1998). It is well known that stress from the adaptation process is high among new immigrants, especially among late life immigrants. Although aging requires a great deal of adjustment independent of other factors, late life immigrants must also acquire a second language and a new set of sociocultural rules at an old age (MacKinnon, Gien, & Durst, 2001). The stress-illness model hypothesizes that higher levels of stress related to adaptation among immigrants lead to worse health outcomes compared with health outcomes among their U.S.-born counterparts (Lindesay, Jagger, Hibbett, Peet, & Modeldina, 1997).
This study aimed to test the HIE and the convergence of health status over time between older U.S.-born individuals and late life immigrants by comparing (a) the initial health status and (b) the rates of health status changes over time across three groups of older adults who were divided by nativity (foreign-born vs. U.S.-born) and length of stay in the United States (15+ years vs. less than 15 years among the foreign-born) using longitudinal data. Health status is a broad construct that encompasses both physiological conditions and consequences of short- and long-term diseases rooted in daily functioning (Houssien & Carr, 1999). Accordingly, based on a literature review, this study compared self-rated health, chronic condition diagnoses, functional impairments frequency, and mortality across the three groups (Cooper, Kohlmann, Michael, Haffer, & Stevic, 2001; Houssien & Carr, 1999; Osmand, Vranizan, Schillinger, Stewart, & Bindman, 1996).
Health Advantages Among Late Life Immigrants
Previous research studies testing the HIE among younger immigrants compared mortality rates, life expectancy, chronic disease, activity limitations, and self-rated health either between foreign-born and U.S.-born populations or between new immigrants, longer term immigrants, and U.S.-born populations (Anson, 2004; Gee et al., 2004; Newbold, 2006; Singh & Miller, 2004). Overall, these health indicators all supported the HIE and suggested better health status on arrival among recent immigrants. The sole exception to this better health status among new immigrants pertained to self-rated health, a metric about which there have been mixed findings, possibly due to ethnic and cultural variations in the way people evaluate and report their health (Bzostek, Goldman, & Pebley, 2007).
However, differences in motivation for immigration might be found between younger and older immigrants and within the older immigrant population depending on their age at immigration. Specifically, health selectivity might not be applicable to late life immigrants whose major motivation is family reunification rather than employment. New immigrants who were admitted to the United States under the employment preference system reported better health compared with their counterparts who were admitted to the United States under the family preference system (Akresh & Frank, 2008). Similarly, and in contrast to the findings related to younger immigrants, past studies indicate that when compared with their U.S.-born counterparts, newly arrived older immigrants are less likely to rate their health as excellent and are more likely to report restricted activities (Gee et al., 2004).
However, these differences in relative health statuses between new immigrants and the native-born population do not appear to be universal across all health indicators. Despite worse self-rated health and functional status among late life immigrants, this group is associated with lower mortality risks, as explained in the literature by such terms as “epidemiological paradox” and “mortality advantage” (Angel, Angel, Venegas, & Bonazzo, 2010; Markides & Eschbach, 2005; Markides & Gerst, 2011). In addition, for certain chronic conditions including cancer, lung disease, and cardiovascular disease, older foreign-born individuals or late life immigrants fared better with regard to prevalence of disease (Colon-Lopez, Haan, Aiello, & Ghosh, 2009; Swallen, 1997).
Based on previous literature regarding older immigrants, this study hypothesized that late life immigrants were in better health than older U.S.-born individuals in terms of some chronic health conditions and overall mortality rates. However, it was hypothesized that self-rated health and functional status would be worse among newly arrived older immigrants than those of their U.S.-born counterparts.
Changes in Health Status Over Time Among Late Life Immigrants
Longitudinal changes in late life immigrants’ health status after admission have been studied very little. For those who immigrated at younger ages and aged in the United States, downward convergence toward native health has been found in relation to acculturation over time. However, it is especially unclear how or whether acculturation affects changes in health status beyond natural declines among late life immigrants, given that late life immigrants’ levels of acculturation are generally low regardless of their length of stay in the United States (Kim, Hurh, & Kim, 1993; Kim, 1999).
Acculturation seems to negatively affect younger immigrants’ health changes over time, but does so differently depending on the indicator. For example, whereas there is an overall negative relationship between the level of acculturation and major health indicators including birth outcomes and chronic conditions, there is a positive relationship between acculturation and self-rated health, possibly due to obtaining a new definition of health in the host culture (Lara et al., 2005; Lee, Sobal, & Frongillo, 2000).
Accordingly, related to declines in health status with duration of stay among immigrants, it is likely that health status of longer term older immigrants—those who, in this study, were more likely to come to the United States at younger ages and aged in the United States—would be explained by initial health selectivity and the negative effects of acculturation on health over time; thus, this group might be characterized by a convergence toward native health. Therefore, this study hypothesized the following:
Hypothesis 1: Health status of longer-term older immigrants would be similar to that of their U.S.-born counterparts as depicted in the immigrant-related literature on the immigrants with younger ages at immigration.
Hypothesis 2: The rate of health decline over time would not be different by native status or length of residence in the United States because the effects of acculturation would be minimal among late life immigrants. For example, it was hypothesized that the initial discrepancy in the abovementioned self-rated health between the U.S.-born and the recent immigrant groups would remain consistent during the study period.
Similar results were hypothesized across different health indicators irrespective of an initial health advantage among late immigrants. The first hypothesis regarding changes in health status has been tested in other immigrant-related studies using cross-sectional data by comparing newer versus longer term immigrant groups. This study contributes to the literature by following up native-born individuals and immigrants of different lengths of residence in the United States over time to directly test the rates of change among different groups.
Method
Data Sources
This study consists of secondary data analyses of the Second Longitudinal Survey of Aging (LSOA II) and a linked mortality file. The LSOA II is a collaborative effort of the National Center for Health Statistics (NCHS) and the National Institute on Aging (NIA; National Center for Health Statistics, 2003). The Second Supplement on Aging (SOA II), conducted in conjunction with the 1994 National Health Interview Survey (NHIS), served as the baseline for the study. Accordingly, the sample includes all individuals 70 years old or older who were selected for the 1994 NHIS core interview (N = 9,447). Data were collected through personal interviews, which were conducted mainly in English by the U.S. Bureau of the Census. The persons who were interviewed in 1994 were reinterviewed in 1997-1998 and 2000 (i.e., three waves). The 2006 LSOA II-linked mortality file provides mortality status for the LSOA II participants from the initial interview in 1994 through December 31, 2006 (Center for Disease Control and Prevention, 2010). The National Death Index (NDI) was used as the primary source of information for the mortality file.
Study Sample
The LSOA II used a multistage sample design to represent the civilian noninstitutionalized population of the United States who were 70 years or older in 1995 (National Center for Health Statistics, 2003). African Americans were oversampled, making up 10.6% of the sample (n = 1,000), whereas 85.5% were Caucasians (n = 8,077; National Center for Health Statistics, 2006). Respondents with other racial backgrounds included American Indian (n = 51), Chinese (n = 34), Filipino (n = 42), Hawaiian (n = 1), Korean (n = 10), Vietnamese (n = 7), Japanese (n = 32), Asian Indian (n = 10), and Guamanian (n = 2). About 4.8% of the respondents were older adults of Hispanic origin.
Measures
Immigrant status
The sample was divided into three groups depending on place of birth and length of residence in the United States: (a) recent immigrants (n = 133)—older immigrants with fewer than 15 years of residence in the United States, (b) earlier immigrants (n = 672)—older immigrants with 15+ years of residence, and (c) the U.S.-born participants (n = 8,642). Recent immigrants are considered to be late life immigrants who immigrated after age 55 (Angel, Angel, & Markides, 2002). The 15-year cutoff was used because sensitivity analyses using the 10-year mark revealed no major differences in the major results but yielded a smaller sample size for recent immigrants (n = 77). The recent immigrant group was compared with the earlier immigrant and the U.S.-born groups as a reference because recent immigrants are the focus of the current study.
Health status variables
Lifetime diagnosis was asked of study participants for 10 health conditions at baseline (yes/no), including osteoporosis, diabetes, arthritis, bronchitis or emphysema, asthma, hypertension, heart disease, stroke, cancer, and Alzheimer’s disease. Then, the number of chronic health conditions was added to calculate the total number of chronic conditions per individual (0-10). Although chronic health conditions were asked about at all three waves of interviews, only the baseline measure was used in this study because of inconsistent observational periods across waves.
Self-rated health was measured at all three waves. The variable was originally measured on a scale of 1 = excellent to 5 = poor. In this study, the variable was recoded into a dichotomous variable with 1 = excellent/very good/good and 0 = fair/poor. Functional status was assessed at all three waves as the number of functional impairments in six areas of activities of daily living (ADLs) including bathing, dressing, eating, getting in and out of bed/chair, walking, and using the toilet and in seven areas of instrumental activities of daily living (IADLs) including preparing meals, shopping for groceries, managing money, using the telephone, doing heavy housework, doing light housework, and managing medication. The total numbers of ADL limitations (0-6) and IADL limitations (0-7) were calculated as sums of impaired areas per individual.
For all participants who completed the Wave 1 interview, mortality status was followed up through the end of 2006. The crude rate of mortality is regarded as one type of health outcome in the literature (Sudano & Baker, 2006). The duration of survival was calculated from the first interview until death or until the end of follow-up in months. The primary reason for death was assessed based on ICD-10 criteria (Center for Disease Control and Prevention, 2010). The cause of death was available for 5,733 out of 5,806 mortality cases (98.7%).
Covariates
Age at baseline, years of education, gender, marital status (married, divorced/widowed, never married), race (Caucasian, African American, Other), Hispanic origin (yes/no), living alone (yes/no), and family income (less than US$20,000; yes/no) were included as covariates. In addition, Medicare, Medicaid, and private health insurance coverage at Wave 1 (past month; yes/no) were included in the longitudinal models as time-lagged covariates to reduce potential endogenous relationships between health insurance and health status (Freeman, Kadiyala, Bell, & Martin, 2008; Levy & Meltzer, 2008).
Statistical Analysis
Univariate and bivariate analyses were performed to describe and compare the sample by immigrant status (Table 1). To account for the complex survey design of the LSOA II, the STATA SVY procedures were used for all analyses except for the analyses presented in Tables 3 and 4, which were analyzed using the HLM software. The degree of multicollinearity among predicting variables was tested.
Bivariate Comparison of Study Variables by Immigrant Status: Percentage (Standard Error) and Mean (Standard Error)

Note. ADL = activities of daily living; IADL = instrumental activities of daily living. Weighted percentages and means are shown for estimates of the U.S. population. p values were calculated with the STATA SVY procedures using REG, LOGISTIC, and POISSON. Immigrant status was entered as a set of dummy variables (reference = recent immigrants). Thus, statistical significance levels in each column indicate the differences between U.S.-born and recent immigrants (indicated by a superscript “a”) and between earlier immigrants and recent immigrants (indicated by a superscript “b”).
p < .05. **p < .01. ***p < .001.
Ten health conditions were first tested bivariately by immigrant status. Only significant conditions (p < .05) were reported in logistic regression models with control variables (Table 2), whereas all ten conditions were tested in the multivariate models for potential suppressor effects. To test the relationship between the number of chronic conditions and immigrant status, a Poisson regression was conducted to account for the nonnormal distribution of the count variable. Odds ratios (OR) and event-rate ratios (ERR) were reported with 95% confidence intervals.
Multivariate Models for Chronic Conditions and the Number of Conditions by Immigrant Status: Logistic and Poisson Regression Models

Note. Estimates were calculated with the STATA SVY with LOGISTIC and POISSON procedures.
p < .05. **p < .01. ***p < .001.
Unconditional HGLM Models for Self-Rated Health and Functional Impairments (ADL and IADL)

Note. HGLM = hierarchical generalized linear models; ADL = activities of daily living; IADL = instrumental activities of daily living; CI = confidence interval.
Logistic regression was used for Level 1 modeling.
Poisson regression was used for Level 1 modeling.
Random effects were set to zero due to the convergence issue. When included, the model would not converge within 300 macro iterations.
p < .001.
Longitudinal Changes in Self-Rated Health and Functional Impairments: HGLM Models

Note. HGLM = hierarchical generalized linear models; ADL = activities of daily living; IADL = instrumental activities of daily living; CI = confidence interval.
Logistic regression was used for Level 1 modeling.
Poisson regression was used for Level 1 modeling.
Random effect was set to zero due to the convergence issue. When included, the model would not converge within 300 macro iterations. Accordingly, covariates for the linear rate of change were not included in the model except for immigrant status and interview status.
p < .05. **p < .01. ***p < .001.
Longitudinal trajectories of self-rated health and functional status (ADL and IADL limitations) were tested by immigrant status using multilevel modeling to deal with autocorrelation among repeated measures (Tables 3 and 4; Raudenbush, Bryk, Cheong, Congdon, & Toit, 2004; Singer & Willett, 2003). As the three health status variables have nonnormal distributions—functional impairments as count variables and self-rated health as a dichotomous variable—the assumption of normality at Level 1 was not met. Thus, hierarchical generalized linear models (HGLM) were used (Raudenbush, Bryk, Cheong, & Congdon, 2001). With HGLM, the within-person model can be a logistic regression model or a Poisson regression model depending on the characteristics of the Level 1 outcome variables (Herman et al., 2000; Horney, Osgood, & Marchall, 1995). To assess and control for selection bias (Chatfield, Brayne, & Matthews, 2005), interview status (i.e., completed all three waves, attrition due to death, and attrition due to any reason other than death) was added to the conditional models as a Level 2 covariate (Timmon, Stijnen, & Tibben, 2004). Of the 9,447 individuals who were eligible for study participation, 7,060 (74.7%) and 5,559 (58.9%) completed interviews at Waves 2 and 3, respectively.
To describe the survival probabilities and mortality hazards by immigrant status over time, unadjusted survival curves were estimated using the Kaplan-Meyer method (Figure 1). For those who were alive at the end of the study period, right censoring was employed. A Cox proportional hazard regression model was conducted to estimate hazard ratios (HR) and 95% confidence intervals for risk of mortality by immigrant status after controlling for the effects of covariates (Table 5). Whether the hazards of mortality were proportional by immigrant status was tested, and no interaction with time was found. To account for the complex survey design of the LSOA II, the STATA SVY procedures were used for all analyses except for the analyses presented in Tables 3 and 4, which were analyzed using the HLM software. The degree of multicollinearity among predicting variables was tested.
Relative Hazards for All-Cause Mortality: Cox Proportional Hazard Model
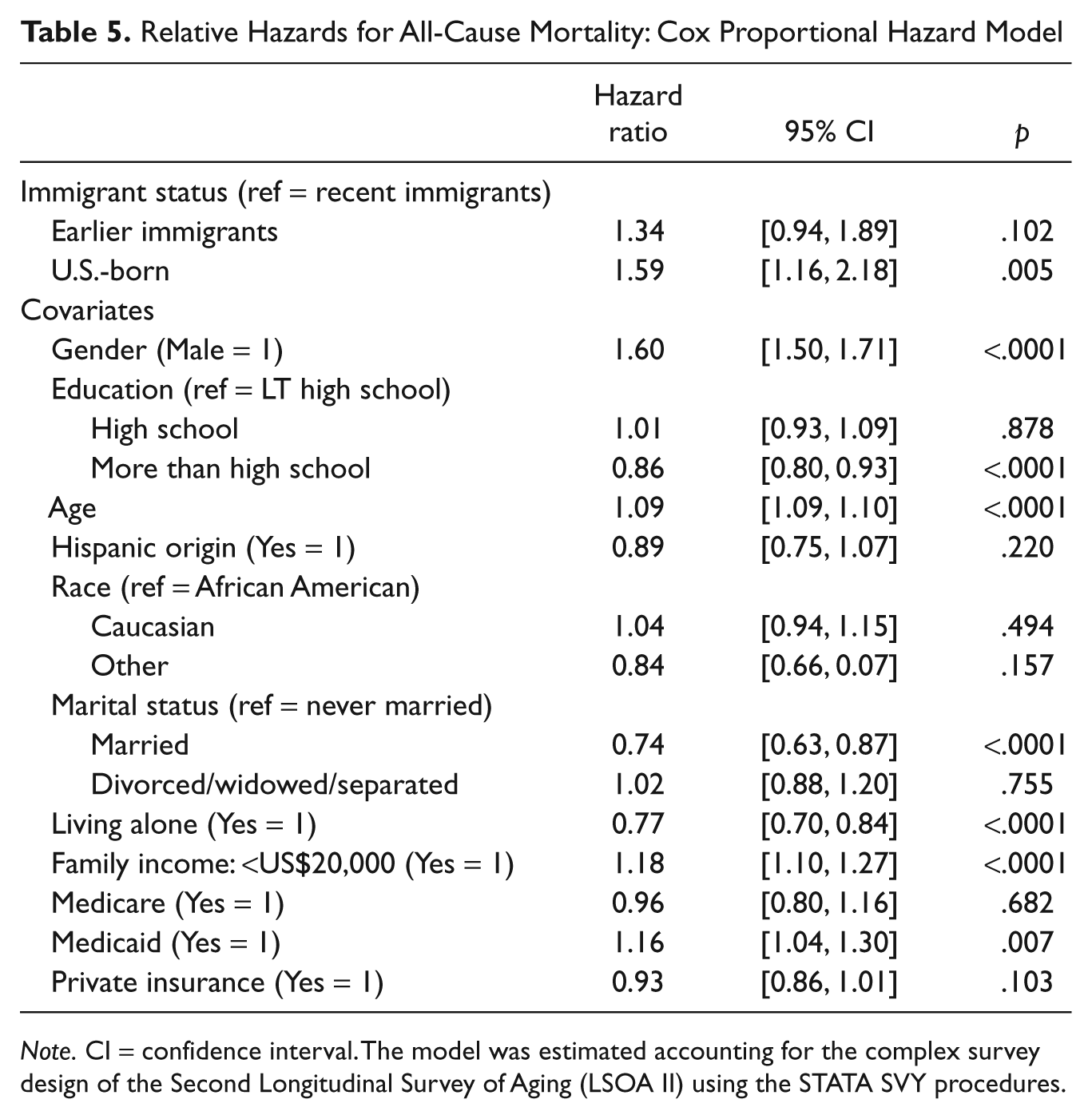
Note. CI = confidence interval. The model was estimated accounting for the complex survey design of the Second Longitudinal Survey of Aging (LSOA II) using the STATA SVY procedures.
Results
Sample Description
Table 1 describes sample characteristics by immigrant status. Compared with U.S.-born older adults and earlier immigrants, recent immigrants were younger, were more likely to live with others, and had lower educational attainment. Recent immigrants were much less likely to have either Medicare or private health insurance coverage and were more likely to rely on Medicaid. In addition, recent immigrants consisted of more diverse ethnic and racial groups than earlier immigrants and their U.S.-born counterparts.
Chronic Health Conditions
Health advantages of late life immigrants
When lifetime diagnoses of listed health conditions at baseline were bivariately compared according to immigrant status, the recent immigrant group did not display any differences compared with their U.S.-born counterparts except in osteoporosis, arthritis, hypertension, and cancer (Table 1). Recent immigrants were less likely to suffer from the aforementioned four conditions than older U.S.-born individuals. The bivariate comparison also revealed that recent immigrants had fewer health conditions at baseline (mean = 1.4) than U.S.-born counterparts (mean = 1.9). However, when tested in the multivariate models (Table 2), only cancer was significantly associated with immigrant status. Compared with recent immigrants, U.S.-born older adults were about 6.5 times as likely to suffer from cancer (OR = 6.45) in terms of odds. Overall, among U.S.-born older adults, the number of chronic health conditions was 20% higher than among recent immigrants at baseline (ERR = 1.20).
Postimmigration health status changes
Although longitudinal data were not available to track respondents’ chronic health conditions over time, the comparison of Wave 1 data indicated that earlier immigrants were associated with higher likelihood of being diagnosed with cancer (OR = 4.08) than recent immigrants, whereas the likelihood was as not as high as in the U.S.-born group (OR = 6.45). In terms of the total number of chronic conditions diagnosed, the same pattern appeared; the ERR of 1.07 among earlier immigrants stood between those of the recent immigrant and the U.S.-born groups, even though the difference between recent and earlier immigrants was not statistically significant.
Self-Rated Health
Health advantages of late life immigrants
As hypothesized, bivariate results indicated that recent immigrants were less likely to report their health as excellent, very good, or good (58.5%) compared with the U.S.-born at Wave 1 (74.5%). The conditional HGLM model in Table 4 also supported this hypothesis, indicating that U.S.-born older adults were more likely to rate their health as excellent, very good, or good at baseline compared with recent immigrants (OR = 3.05).
Postimmigration health status changes
In bivariate analyses, earlier immigrants’ ratings of their health status were better than that of their recent immigrant counterparts across all waves. Their ratings were close to those of the U.S.-born individuals, even though they were not better across all waves. These findings were also supported in the HGLM models. At baseline, earlier immigrants were more likely to rate their health as excellent, very good, or good compared with recent immigrants (OR = 2.99). The OR of 2.99 among earlier immigrants was close to the OR of the U.S.-born group (OR = 3.05).
The significant linear rate of change in the unconditional model (Table 3) indicates that the likelihood of reporting good health among respondents declined each year (OR = 0.94). When growth parameters were tested in the conditional model (Table 4), the linear rate of change did not vary by immigrant status, indicating that the initial difference in self-rated health by immigrant status persisted over the study period.
Functional Status
Health advantages of late life immigrants
Bivariate test results in Table 1 indicate that at baseline, U.S.-born older adults reported better functional status than recent immigrants. On average, the number of ADL and IADL impairments among the U.S.-born was 0.7, whereas these measures were 0.9 and 1.1, respectively, among recent immigrants. As seen in Table 4, after controlling for the covariates, the difference between the U.S.-born and recent immigrants at baseline remained statistically significant. The average number of ADL and IADL impairments at baseline among older U.S.-born adults was 41% that of recent immigrants (ERR = 0.41 for both ADL and IADL impairments).
Postimmigration health status changes
Bivariate and multivariate results indicate that at all three waves, earlier immigrants reported better functional status compared with recent immigrants, even though the differences in the bivariate level were statistically significant only at Wave 3. The conditional models (Table 4) indicate that the average number of earlier immigrants’ IADL functional impairments were 44% that of recent immigrants at baseline. Thus, as with self-rated health, the earlier immigrant group was found to be between the recent immigrant and the U.S.-born groups in terms of their functional status, suggesting the convergence of functional status between earlier immigrants and the U.S.-born individuals over time.
Table 3 displays the coefficients of unconditional growth models for functional status changes. On average at baseline, the expected number of impairments was 0.16 and 0.20 for ADL and IADL (greater than zero), respectively, among all study participants. The significant ERRs greater than 1 for the linear rates of change suggest increases in the number of functional impairments by 28% and 21% for ADL and IADL, respectively, each year. The linear rate of change in IADL did not differ according to immigrant status, indicating that initial differences in the IADL functional status remained constant over the course of the study period.
However, compared with that of recent immigrants, U.S.-born older adults’ ADL statuses deteriorated at a steeper rate (ERR = 1.12). This finding neither supports the hypothesis of this study nor is consistent with related findings from previous literature that suggests the negative effects of acculturation among new immigrants. No difference in the rate of ADL change was found between recent immigrants and longer term immigrants.
Mortality Through 2006
During the 12-year follow-up period, 61.1% of the population died, with a mean survival time from the baseline interview of 93.7 months (approximately 7.8 years) and a median of 108 months (9 years). Unadjusted, bivariate comparison reveals that recent immigrants were more likely to be alive at the end of the 12-year follow-up compared with their U.S.-born and earlier immigrant counterparts (Table 1). Among deceased individuals, there were no differences according to immigrant status in terms of three leading causes of death among older adults in the United States (Kung, Hoyert, Xu, & Murphy, 2008). The Kaplan-Meier survival curve (Figure 1) shows that the probability of survival over the study period was highest among recent immigrants. Figure 1 also displays very similar survival functions between the U.S.-born and the earlier immigrant groups, as was hypothesized for this study. The results from the Cox proportional hazard model (Table 5) indicate that after controlling for other covariates including age at the baseline interview, the hazards of mortality were significantly higher among U.S.-born older adults over time (HR = 1.59) than among recent immigrants. No statistical difference was found between recent and earlier immigrants, even though the HR among earlier immigrants (HR = 1.34) was greater than 1 and in the same direction from the null as that of the U.S.-born population, as was also hypothesized.

Kaplan-Meier survival estimates, by immigrant status
Discussion
This study examined relative health status of recent immigrants, earlier immigrants, and U.S.-born older adults using longitudinal data. The findings support the sparse literature on late life immigrants and their health status. In general, due to lack of initial self-selectivity and convergence into native health among late life immigrants, findings for this recent immigrant group were very different from what was found among those who migrated at younger ages.
HIE Among Late Life Immigrants: Initial Health Advantages
In terms of the initial status at baseline, the results support the HIE only partially, depending on the health status measure in question. Recent immigrants were healthier only when health status was measured using chronic health conditions. The hazard of mortality was also consistently lower among recent immigrants, as has been suggested in previous studies (Markides, Salinas, & Sheffield, 2009). Similar findings to these exist from other studies that compared health status of U.S.-born and foreign-born individuals. For example, older Mexican immigrants reported a lower rate of heart disease than their non-Hispanic, U.S.-born counterparts (Wallace, Gutierrez, & Brown, 2003), whereas recently arrived older immigrants were more likely to report limitations in daily activities and lower levels of self-rated health compared with native-born older adults (Gee et al., 2004).
The reasons for the discrepancies in support of the HIE between younger and older immigrants and between late life and longer term older immigrants may be related to differences in the motivation for immigration between these groups. Considering U.S. immigration policies, younger immigrants are more likely to come to the United States for employment (i.e., employment-based immigration), whereas late life immigrants are more likely to immigrate to reunite with their family members who are already in the United States (i.e., family-based immigration). Thus, the effects of positive selectivity, as well as the tight screening procedures of the U.S. government for prospective immigrants regarding health status, may account for health advantages among younger immigrants on arrival. In addition, further studies are necessary regarding the triggers and motivations of adult children’s decision making to invite their parents from their native countries. If changes in health status of older parents either encourage or discourage the decisions of international migration of late life immigrants, it may account for the systematic differences in health status of late life immigrants on arrival.
In addition, worse self-rated health and functional status among late life immigrants may be better explained by the stress-illness model, given the loss of protective factors inherent in leaving one’s native country in old age (Gushulak, 2007) and the following acculturative stress in the new country (Berry & Sam, 1996). Older foreign-born individuals tend to have poorer mental health compared with their native-born counterparts (Lai, 2004). Underlying stress and mental health status, such as depression, may be presented as worse self-rated health and functional status among late life immigrants because of the close connection between mental health and other such health outcomes (Han, 2002). In addition, low rates of reported health conditions may be related to difficulties in accessing health care among new immigrants because identifying such health conditions requires formal diagnosis made by a health professional (Osmand et al., 1996). The literature suggests that late life immigrants are less likely to see doctors than longer term immigrants or U.S.-born individuals (Choi, 2006).
Further research is necessary to examine whether these inconclusive results stem from the characteristics of different health status measures or from actual differences in health status. Despite the known language barriers experienced by older immigrants, few standardized assessment tools for health status are available in older immigrants’ native languages (Sakauye, 1992) or according to culturally appropriate norms (Livingston et al., 2002). The measurement equivalence of the question asking self-rated health has been brought into question (Bzostek et al., 2007). With culturally insensitive instruments, cultural differences may be misinterpreted as functional impairments when unfamiliar tasks, such as balancing a checkbook, are used to assess an older immigrant’s functioning (Livingston et al., 2002).
Postimmigration Health Status Changes Among Late Life Immigrants
Among those indicators for which recent immigrants had lower status at baseline (i.e., self-rated health, ADL and IADL limitations), there was a steeper rate of deterioration among U.S.-born older adults than among their recent immigrant counterparts, even though statistical significance was found only for ADL limitations. In contrast, the HIE and immigrant health-related literature would hypothesize a better initial health status and a steeper deterioration over time among recent immigrants. In addition, no differences in the rate of changes in self-rated health and functional impairments were found between recent and earlier immigrants, indicating nonsignificant effects of acculturation or duration of stay in the United States on health changes among older foreign-born individuals. Instead of nativity and length of residence in the United States, the rates of health change were significantly associated with other factors including demographic characteristics, living arrangements, and having private insurance.
These results may suggest that the age at immigration is an important factor in understanding initial health status and its changes over time among older immigrants (Angel & Angel, 1992). Even though the LSOA II does not provide information on age at migration—it aggregates all foreign-born individuals with longer than 15 years of residence in the United States in one group—earlier immigrants in this study are more likely to have immigrated to the United States at younger ages than recent immigrants. Among recent immigrants, who are all late life immigrants who migrated to the United States after age 55, health status did not downwardly converge to that of longer term and U.S.-born older adults. Thus, changes in health status over time among late life immigrants did not support previous literature regarding the relationship between health status and length of stay in the United States among younger immigrants. However, among earlier immigrants, health status either stood between that of the recent immigrant and the U.S.-born groups or was very similar to that of U.S.-born individuals. This finding supports the notion of HIE and the effects of negative acculturation on health in that health status of longer term immigrants is expected to become closer to that of native-born individuals over time.
Neither have the causes of mortality advantages among foreign-born older adults (Markides & Eschbach, 2005; Markides et al., 2009) nor have the reasons for the consistent gap in mortality rates between late life immigrants and the U.S.-born been fully explained. As seen in this study, self-selection into migration among healthy individuals does not seem to be true among late life immigrants considering their relatively poor self-rated health and functional status over time. Lower mortality risks were also found for late life immigrants in a 13-year follow-up study of the Hispanic Established Populations for Epidemiologic Studies of the Elderly (H-PESE) sample, where there were no differences found in mortality between U.S.-born older adults and older immigrants from Mexico who migrated to the United States in childhood or midlife (Angel et al., 2010). Lower rates and frequencies of chronic conditions might contribute to lower mortality risks over time among late life immigrants. However, as seen in this study, chronic health conditions were not greatly different by nativity and length of residence in the United States among older adults. For some health outcomes, it may take much longer to see the effects of migration. Chronic health conditions and mortality may take a longer amount of time to bring about the negative impact of stress and environmental changes associated with late life immigration, compared with self-rated health. In addition, it is also possible that mortality among late life immigrants is not accurately recorded in the NDI, resulting in the underestimation of mortality cases among late life immigrants (Markides & Gerst, 2011).
Implications for Late Life Immigrants
The results of this study suggest a paradoxical picture of health status among late life immigrants; even though they live longer lives that are affected by fewer chronic health conditions, their expanded lives are more likely to be affected by a higher number of functional impairments and poorer general health compared with those of their earlier immigrant and U.S.-born counterparts. These findings call for further research regarding late life immigrants’ quality of life in later years. Moreover, late life immigrants experience higher levels of barriers to health insurance coverage and access to formal health care due to lack of work history in the United States and lack of affordable health insurance options for older adults who are not qualified for Medicare and Medicaid (Choi, 2011). The foreign-born individuals in the LSOA II all arrived before the enactment of welfare reform in 1996, and their benefits were therefore not directly affected by the reform. As seen in Table 1, the respondents in the recent immigrant group relied heavily on Medicaid compared with their U.S.-born counterparts (57% vs. 8%, respectively). However, low-income immigrants who entered the United States after the enactment of welfare reform would have been much more vulnerable to being uninsured due to the ban on Medicaid during their first 5 years of stay in the United States.
The Patient Protection and Affordable Care Act is expected to benefit legally admitted older immigrants with moderate incomes. The Act will provide broader nongroup private health insurance options for newly arrived older immigrants without employment history in the United States by prohibiting denial of coverage based on preexisting health conditions and by placing a 3:1 ratio limit in health insurance premium based on age (The Kaiser Family Foundation, 2010; National Immigration Law Center, 2010a). However, the ban on federal Medicaid benefits for individuals with less than 5 years of residence in the United States will remain intact. In addition, during their first 5 years in the United States, late life immigrants cannot buy into Medicare and will be restricted from doing so under the new law. Health care professionals and policy makers should consider late life immigrants’ relative health status and should address their potential unmet health care needs to increase late life immigrants’ long-term quality of life and to provide cost-efficient health services.
Limitations
As the LSOA II data were obtained via self-report, caution should be taken when interpreting the results (McGwin, Melton, May, & Rue, 2000). Moreover, due to the lack of standardization across the three waves of interviews (i.e., inconsistent observational periods), chronic health conditions could not be tracked longitudinally. In addition, the small sample size of the recent immigrant group did not permit examination of diversity within the foreign-born population by their countries of origin.
Moreover, caution should be taken when interpreting nonsignificant statistical differences especially between recent and earlier immigrants due to the small sample size for the recent immigrant group. For many health indicators, earlier immigrants fell between the recent immigrant and the U.S.-born groups (Table 1). Even though retrospective statistical power analyses conducted after data collection have limitations in interpreting nonsignificant results (Nakagawa & Foster, 2004), bivariate-level power analyses conducted using the SAS PROC POWER procedures indicate that the statistical power was below .80, which is recommended in related literature (Cohen & Cohen, 1983), for most bivariate tests between the recent and earlier immigrant groups in Table 1. For example, the statistical power to detect the difference in the percentage of individuals with arthritis between the earlier and recent immigrant groups was only 0.341 and the difference in the percentage was 7.3% between the two groups as seen in Table 1 (55.6% vs. 48.3%).
In terms of language of interview, the LOSA II was conducted mostly in English. Therefore, older immigrants with better English command and higher levels of acculturation may have been overrepresented in the sample. Historically, older immigrants in the United States are underrepresented in health research due to their limited English proficiency, which is often required to participate in research (Gany, Shah, & Changrani, 2006; Livingston et al., 2002).
In addition, even though problems with attrition are not limited to the LSOA II (Chatfield et al., 2005; Mihelic & Crimmins, 1997), the extent and pattern of attrition is another major limitation of this study. Recent immigrants were significantly less likely to complete all three waves of interviews (38.6%) compared with earlier immigrants (46.1%) and the U.S.-born (57.1%). More importantly, a disproportionately high percentage of recent immigrants (8% of those who completed Wave 1) dropped out of the study due to difficulties in conducting a survey in English at Wave 2 (vs. 1% among earlier immigrants). The Health and Retirement Survey (HRS), which oversampled Hispanic older adults, conducted interviews in Spanish for 318 Spanish-speaking Hispanics (Sudano & Baker, 2006). In the HRS, there was no difference in the rate of loss to follow up between Spanish-speaking Hispanics and Caucasians during the 10-year follow-up period (1992-2002; 6 waves; Baker et al., 2006). The LSOA II offered interviews in Spanish for only a limited number of respondents, and interviews were not able to be conducted in any other languages.
Contribution to the Literature
Despite these limitations, this study provides an important insight into the health status of late life immigrants. To gain further knowledge about late life immigrants’ health status, which is necessary for informed policy decisions and adequate provisions of health services for this population, the current study compared relative health status of late life immigrants with that of their longer term immigrant and U.S.-born counterparts using a nationally representative sample of older adults in the United States. Furthermore, a longitudinal design strengthened the study because it permitted extensive testing of the HIE and the following postimmigration changes: comparison of initial health status and the longitudinal trajectory of health across the three study groups. Cross-sectional comparisons between newly arrived older immigrants and more long-term older immigrants may compound the effects of length of residence in the United States and age at immigration. As a longitudinal study, this study examined both the baseline health status and growth characteristics over time. Another contribution of the current article to the literature is that this study tested the HIE using different health status measures.
In addition to the theoretical importance in the context of the HIE, focusing on newly arrived older immigrants also provides important policy implications. As welfare reform in 1996 and Medicare buy-out policies prohibit new immigrants with fewer than 5 years of residence in the United States from getting Medicare and Medicaid coverage (National Immigration Law Center, 2010b), it is important to understand relative health status of recently arrived older immigrants to accurately assess potential impacts of such policies.
Footnotes
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
This study was partially supported by a grant from the John A. Hartford Geriatric Social Work Faculty Scholars program.