
Abstract
Keywords
Introduction
To maintain good oral health in later life, regular utilization of dental care services has been strongly recommended. Dental care is identified by the older population as the most common health care service they need for which they do not have access (Dolan, Atchison, & Huynh, 2005; see also Lau & Kirby, 2009). Among adults of all ages, persons aged 65 years and older are the least likely to see a dental health care professional on a regular basis (Dye et al., 2007). One of the objectives of HealthyPeople 2020 is to reduce age disparities in access to dental services (U.S. Department of Health and Human Services [USDHHS], 2011). Understanding the factors associated with dental care service utilization among older persons is essential for health care providers and health care policy makers, as well as for the design of interventions to promote oral health and regular dental care service utilization.
Maintaining oral health in later life is important for many reasons. Poor oral health is marked by tooth loss, dental caries, periodontal disease, oral dysfunction, poor nutrition, and pain (Brennan, Spencer, & Roberts-Thomson, 2008; Dolan et al., 2005; Ettinger, 2007; Naito et al., 2006; Randolph, Ostir, & Markides, 2001; Wu, Plassman, Liang, & Wei, 2007). In addition, poor oral health is associated with other health conditions, including cardiovascular disease (Buhlin, Gustafsson, Andersson, Håkansson, & Klinge, 2002; Cotti, Dessi, Piras, & Mercuro, 2011; Meurman, Sanz, & Janket, 2004), diabetes (Lamster, Lalla, Borgnakke, & Taylor, 2008; Santacroce, Carlaio, & Bottalico, 2010), cognitive impairment (Noble, 2009; Yu & Kuo, 2008), and Alzheimer’s disease (Kamer et al., 2008). Good oral health is related to higher levels of overall quality of life. To ensure and maintain oral health, it is important to receive routine dental checkups and preventive care and to have dental problems diagnosed and addressed in a timely manner. Visits to dental professionals for preventive and restorative care can save money and trauma, especially when more expensive and intrusive dental procedures are forestalled (Moeller, Chen, & Manski, 2010).
This study focuses on an understudied topic in this field: the relationship between social relationships and dental care service utilization. The importance of social relationships for general health is well documented (Berkman, Glass, Brissettte, & Seeman, 2000; Holt-Lunstad, Smith, & Layton, 2010; House, Landis, & Umberson, 1988; Uchino, Cacioppo, & Kiecolt-Glaser, 1996), as is the linkage between social relationships and certain health behaviors (Broman, 1993; Umberson, Crosnoe, & Reczek, 2010). Although the scientific evaluation of the association between social relationships and oral health is limited, this body of research is growing (Avlund, Holm-Pedersen, Morse, Viitanen, & Winblad, 2003; Hanson, Liedberg, & Owall, 1994; McGrath & Bedi, 2002; Merchant, Pitiphat, Ahmed, Kawachi, & Joshipura, 2003). Within this field, relatively little research has been reported that examines the relationships among multiple dimensions of social relationships and dental care service utilization. Much of the extant research on this topic employs data from Europe, especially Scandinavia, where governments routinely provide financial support for dental care for their populations (Lundgren, Osterberg, Emilson, & Stern, 1995; Petersen & Nørtov, 1989; Rickardsson & Hanson, 1989). It is necessary to increase our knowledge of the relationships among social relationships and dental care service utilization among older persons in the United States because the financing of dental care primarily rests with older individuals and their families and because of potential cultural differences related to values and norms of oral health and dental care service utilization across countries.
The purpose of this study is to examine the relationships among two domains of social relationships and dental care service utilization among older persons in the United States. These domains are social integration (structural) and social support (functional; Cohen & Wills, 1985; Uchino, 2004). Previous studies of this topic are based on small, nonprobability samples, single communities, or a single age group. The current study relies on a large, nationally representative survey, the Health and Retirement Study (HRS), which helps overcome some of the limitations of earlier studies.
Literature Review and Conceptual Model
Seeking health care is considered to be one of the pathways through which the social environment is related to health (Berkman et al., 2000; Rosenstock, 1966). More specific to this study, seeking dental care, whether preventative or restorative, is a pathway to overall oral health. Understanding how social relationships are associated with dental care service utilization among older persons, the central objective of this study, provides a partial representation of an overall model of oral health.
Theory regarding the potential linkages between social relationships and dental care service utilization is not well developed and the causal mechanisms are complex. However, it is possible to construct a conceptual model by applying theoretical advances surrounding social relationships and physical and mental health. It is also informative to review the literature on social relationships and health care utilization, broadly defined, as well as the limited literature on dental care utilization and social relationships.
There are two well-known models of social relationships and health (Cohen, 2004; Umberson & Karas Montez, 2010). On one hand, the direct effects model (or main effects model) of social relationships and health focuses on the concepts of social integration and social ties (Uchino, 2004). This model allows for the likelihood that social relationships are associated with health through cognitive, behavioral, emotional, and biological pathways (Holt-Lunstad et al., 2010). In this model, individuals tap into “more general social resources” based on the structural characteristics of their social network relationships, which often are not explicitly meant to provide help for a given problem (Uchino, 2004, p. 45). As discussed below, we expect structural relationships to be associated with more active participation in maintaining one’s oral health through the use of dental care services.
On the other hand, the stress-related model of social relationships and health focuses on functional characteristics of social networks. One version of this model hypothesizes that the impact of stress on health is moderated by social support systems (the buffering hypothesis). Another version suggests that social support can enhance meaning and give purpose to life and promote less risky lifestyles, yielding positive associations with health irrespective of the stress component (Umberson & Karas Montez, 2010). The functional support provided by network members is hypothesized to more directly attend to the needs of the individual. Functional support includes providing emotional, tangible, and informational assistance. This type of support can be the actual support provided (such as giving money or reassurance), or it can be perceived support, based on expectations about assistance that would be available if the need arises. We expect that persons who receive functional support, or perceive that such support is available, when needed, will be more likely to utilize dental services. Before we discuss how each of the domains of social relationships may be related to dental care service utilization, we briefly describe the more general literature on social relationships and health care service utilization.
Social relationships and health care service utilization
The research literature on social relationships and physical and mental health care utilization is far more developed than that for dental care utilization (Andersen & Newman, 1973; Gourash, 1978; Maulik, Eaton, & Bradshaw, 2011; McKinlay, 1973; Wolinsky & Johnson, 1991, 1992). However, results from research investigating the association between health care utilization and social relationships are mixed. The research literature is complicated by conceptual ambiguity regarding the domains of social relationships (not distinguishing between the two types of social relationships identified above), variability in measurement strategies (often using only one or two indicators of social relationships), and the use of nonrepresentative community samples (although this has changed over time).
Andersen and his colleagues (Andersen, 1995; Andersen & Davidson, 1997; Andersen & Newman, 1973) provided an early, well-known conceptual framework for health care–seeking behavior that included both individual- and societal-level characteristics. At the individual level, three groups of variables are included; these are predisposing, enabling, and need characteristics. The model has been refined many times (Andersen, 1995), used as a conceptual framework in thousands of studies, and has been reviewed and criticized routinely (Andersen, 2008; Wolinsky, 1994).
One set of individual characteristics that did not receive as much attention in the Andersen model is the role of social relationships. Following the early work of Andersen and Newman (1973), Gourash reviewed the state-of-the-science regarding social relationships and health care utilization. In her review article (Gourash, 1978, p. 416), she stipulates that social relationships play four possible roles in help seeking: (a) moderate the impact of stress leading to less need for help, (b) reduce the need for professional help by providing tangible and emotional support, (c) act as referral agent to professional help, and (d) provide support for norms, attitudes, and values regarding pursuing professional help when needed. Gourash did not make a distinction between the social integration and social support domains of the social relationships model.
Rundall and Evashwick (1982) added to the literature by alerting researchers to the fact that not all social relationships were necessarily positive with respect to promoting health care utilization. They found that older persons who were disengaged from or abandoned by their social network members were less likely to visit a doctor. Expanding on this idea, Maulik et al. (2011) noted that sometimes social network members discourage persons from using health care services. They argue this may be especially relevant with regard to seeking mental health services because of the stigmatization associated with seeking such care.
Schmitz, Russell, and Cutrona (1997) developed the field further by showing that dense social networks promote less use of formal health care services and that perceived social support promotes greater utilization. Wolinsky and Johnson (1991) demonstrated that the role of social relationships in promoting health care utilization may depend on the type of health care examined and whether the social relationships are kin or non-kin based. They find non-kin and kin connections are related to more physician visits, and non-kin connections are related to fewer hospital stays and a lower likelihood of entry into nursing homes. Kin social relationships were not related to any other form of health care service in their study.
Other researchers demonstrate that it may be the level (or amount) of social interaction that is most predictive of using medical care services (Counte & Glandon, 1991); this same research did not find a stress-moderating effect for social relationships. In that study, social support was operationalized by social integration characteristics and not the functional characteristics now more generally recognized as indicating social support. Using a fine-grained approach to identifying types of social support, Krause (1988) finds that informational and tangible social support are positively related to physician visits among older people and that level of support is also important but other forms of support were not statistically significant.
Social integration and dental care utilization
Marital status is one of the most important structural dimensions of social relationships. Married persons are believed to have a greater sense of purpose, commitment, and responsibility toward their spouses and thus should be more likely to take care of themselves in order to achieve these goals (Umberson et al., 2010, p. 148). Spouses also provide social control, which might include insisting on positive health behaviors such as seeing a dentist for routine or restorative care. Studies show that being married is positively related to greater use of dental services. Evidence from the 2002-2005 U.S. Medical Expenditure Panel Surveys shows older persons living alone are at higher risk than married couples living alone of not having routine dental checkups (Lau & Kirby, 2009); similar results were found among a sample of older Japanese (Takehara & Shimoyama, 2008).
However, Wu et al. (Wu, Tran, & Khatutsky, 2005) do not find support for an association between marital status and dental care service utilization among older Russian and Chinese immigrants in a large New England city. Other research shows that marital status is associated with visiting a dentist when considered within the context of the living arrangements of the married couple. Lau and Kirby (2009) find that married persons living with others are less likely than married persons living alone to visit a dentist. We expect married persons will be more likely than nonmarried persons to use dental care services.
Structural aspects of social relationships also include social interactions with family, friends, and neighbors. Social interaction leads to a higher compliance with positive health norms and health behaviors, including accessing dental care services (Cacioppo & Hawkley, 2003; Gourash, 1978). Persons who are actively engaged with others in their social network may develop a higher sense of self-esteem and a greater sense of meaning and control over their personal lives. These contacts may also provide referrals to appropriate dental care providers. Thus, more social integration through contacts with friends, family, and other relatives should be positively related to the likelihood of using dental care services.
Social participation (sometimes labeled social engagement) is another dimension of social integration, but the interactions are more formal and structured than interactions with friends and family. Social participation is conceptualized as belonging to and spending time engaging with community-based groups such as social clubs and religious organizations. Engaging with others in the community through formal volunteering (e.g., schools, hospitals) is another form of social participation shown to be related to positive health outcomes (Fried et al., 2004). Engagement with other persons in the community promotes the development of social skills and helps increase positive psychological health, such as self-efficacy, self-esteem, and self-confidence. Furthermore, interacting with community members may reinforce positive health behaviors, like seeing a dentist regularly, through the referral process identified above. Survey evidence from Sweden shows that higher levels of social participation are related to an increased likelihood of engaging in regular dental care (Rickardsson & Hanson, 1989). We expect that engaging in community activity is related to a higher likelihood of dental care service utilization.
Being embedded in neighborhoods or communities where relationships with others are supportive and affirming is another aspect of the social integration domain of social relationships considered here. Living in neighborhoods where people know each other and have positive contacts likely generates social capital that translates into support for taking care of oneself and provides meaning to life (Aida et al., 2010). Although studies show that neighborhood-based social capital is related to indicators of oral health, we are not aware of any studies that link neighborhood social relationships to dental care service utilization. Nevertheless, it is reasonable to expect that the trust and reciprocity associated with social capital would be helpful to older persons who might otherwise not seek dental care (Aida et al., 2010).
Loneliness represents an indicator of social isolation, in other words, a lack of social connectedness or integration (Cacioppo & Hawkley, 2003). Research indicates that loneliness is related to health outcomes, broadly defined, in that those who are most lonely suffer more negative health consequences; however, the evidence regarding health behaviors is mixed (Cacioppo & Hawkley, 2003). Examining a cohort of 88-year-olds in Sweden, Lundgren et al. (1995) find that net of dental status and other controls persons who reported feelings of loneliness were less likely to use dental care services. We expect that persons who report being lonely will be less likely to engage with the dental care service profession.
Social support and dental care utilization
Levels of social support are conditioned by social network integration and are related to health and health behaviors, including seeking dental care for preventive and restorative purposes (Ertel, Glymour, & Berkman, 2009). Social support is most often provided informally by family members and friends and contains actual and perceived components. Functional social support takes many forms, including exchange of information as well as the exchange of emotional and material (or instrumental/tangible) aid. Some forms of functional social support require geographic proximity to social network members, and other forms may be provided from a distance. For older persons, living close to adult children represents a form of potential social support. Support from network members may include the provision of information about and assistance with navigating the dental health care system, including helping to make and keep appointments with dental care providers (McGrath & Bedi, 2002). Furthermore, functional support may include the provision of financial resources to help pay for care or it may include providing transportation to dental clinics. Family and friends may also help to overcome negative attitudes and misperceptions about dentistry (Andersen & Davidson, 1997; Wu et al., 2005).
In general, a small number of studies show support for a positive relationship between social support and use of oral health services (Lai & Hui, 2007; Marino, Browning, & Kendig, 2007; McGrath & Bedi, 2002; Rickardsson & Hanson, 1989; Wu et al., 2005). Lai and Hui find that dental care service utilization was higher among older Chinese immigrants in Canada when levels of social support were higher. Other research with a small sample of orofacial injury patients at a clinic in Los Angeles who were age 18 years and older shows that postsurgical appointments are more likely to be missed by persons with low perceived social support (Brown, Shetty, Delrahim, Belin, & Leathers, 1999). Using Swedish data from the 1980s, another study found that a cohort of 68-year-old men are more likely to see a dentist at least once every 2 years if their emotional, material, and informational support is high (Rickardsson & Hanson, 1989). We anticipate that actual and perceived social support will be associated with a greater likelihood of engaging with the dental care profession.
On the basis of our review of the research literature about social relationships, health, health care service utilization, and dental care service utilization, we pose two research questions.
Research Question 1: Are the two domains of social relationships (social integration and social support) related to dental care service utilization among a nationally representative sample of older persons in the United States?
Research Question 2: Do these relationships remain statistically significant after adjusting for a set of covariates known to be barriers to and facilitators of dental care service utilization?
Research Design
Data Source and Study Sample
We analyzed survey data from the 2008 wave of the HRS. The HRS survey was based on a stratified, multistage area probability sample that was nationally representative of persons aged 51 and older residing in the contiguous United States (Servais, 2011). African Americans and Hispanics were oversampled. We combined data from the core questionnaire along with data from the Participant Lifestyle Questionnaire. In 2008, a random sample of one-half of the HRS respondents was given the Participant Lifestyle Questionnaire, which included an extensive battery of psychosocial items, which respondents self-administered and then returned to HRS offices. The response rate for the core questionnaire was 88.4%, and the response rate for the Participant Lifestyle Questionnaire was 89.0%. Most variables for this study were downloaded from the University of Michigan HRS web site; however, a few of the variables were downloaded from the RAND HRS web site (e.g., household income, Activities of Daily Living [ADL] limitations).
The study sample was restricted to community-dwelling White, Black, and Hispanic persons who were aged 65 and older. Persons of other races were excluded due to small sample size. If a respondent lived with a spouse/partner, the spouse/partner was interviewed, but a zero sample weight was assigned if the spouse/partner was not a member of one of the eligible birth cohorts included in the HRS design; these respondents were excluded from our study. Respondents who were edentate (had lost all of their teeth) were also excluded because research showed the dental health behaviors of dentate and edentate populations were different (Tennstedt, Brambilla, Jette, & McGuire, 1994). Respondents with missing data on the variables employed in this study were excluded. The amount of missingness among the variables was generally small, not exceeding 2.8% except for the measure of global social interaction (4.6%). The sample size for this study was 2,978.
Measures
Dental care service utilization
We use information about visiting a dentist to represent dental care service utilization. The HRS asked each respondent, “In the past 2 years, have you seen a dentist for dental care, including dentures?” Our dependent variable was measured as 1 = visited a dentist in the past 2 years and 0 = did not visit a dentist in the past 2 years. No other information on oral health or dental health care service participation was available in the HRS core or participant lifestyle questionnaires.
Social relationship variables
We included eight social integration indicators in this study. The first type of social integration was marital status. Marital status was measured as 1 = currently married and 0 = not married. The second set of social integration measures were based on self-reported frequency of interactions with children, other relatives, and friends. The HRS questionnaire asked, “On average, how often do you do each of the following with any of your children (or other family members; or friends) (not counting any who live with you)?” Types of interaction included meet up with them, speak on the phone with them, and write or email them. Response options were 3 or more times a week, once or twice a week, once or twice a month, every few months, once or twice a year, and less than once a year or never. Respondents who reported having no children, no friends or no other relatives, respectively, were assigned the last category. Persons who reported interacting with each type of social network member at least once or twice a month were assigned 1 and those interacting less frequently were assigned 0. We created social interaction indexes for each type of social network member by combining scores for meeting, phoning, and writing (range for all indexes was 0-3). We also created a global measure of social interaction among all types of social network members by combining the indexes for children, other family members, and friends (range 0-9).
Another subjective indicator of structural integration was self-reported feelings of loneliness. We created an index of loneliness based on five items from the HRS questionnaire. The HRS asked, “How often do you feel ‘you lack companionship’, ‘left out’, ‘isolated from others’, ‘in tune with the people around you’, and ‘alone’?” Response options were 3 = often, 2 = some of the time, and 1 = never. For respondents who had at least two valid responses among the five items, we combined responses across each of these items and averaged the scores to form an index of loneliness (range 1-3).
Social participation was identified with two variables. Respondents were asked how often during the past year they attended religious services. Response options included more than once a week, once a week, 2 or 3 times a month, 1 or more times a year, and not at all. We created a dichotomous social participation variable for attendance at religious services, whereby 1 = at least monthly and 0 = rarely or not at all. Respondents were also asked whether they engaged in volunteer work for a formal organization during the previous year, and if so, how many hours they contributed to this activity. We created three dichotomous volunteer variables that included did not volunteer (no hours; reference group), volunteered 1 to 99 hours, and volunteered 100 or more hours.
Neighborhood social cohesion represented the last of the social integration indicators. The HRS asked respondents to rank from 1 to 7 how they felt about their local area, where local area was defined as about a 20-min walk or about 1 mile from their home: “I really feel a part of this area,” “Most people in this area can be trusted,” “Most people in this area are friendly,” and “If you were in trouble, there are lots of people in this area who would help you.” For respondents who had at least two valid responses, we combined responses across each of these items and averaged the scores to form a neighborhood social cohesion index (range 1-7).
Next, we included three social support indicators. First, perceived social support, a subjective indicator of social support, was measured with the following question: “Suppose in the future, you needed help with basic personal care activities like eating or dressing. Do you have relatives or friends who would be willing and able to help you over a long period of time?” Respondents who were already receiving support for help with ADLs were not asked this question. Because these respondents were currently receiving social support, we considered these respondents to expect they could also receive such support in the future, if the need arrived. Respondents who replied “don’t know” were included as not perceiving social support, if needed in the future. The dichotomous perceived social support variable values included 1 = yes and 0 = no.
Second, actual social support was measured by receipt of financial support during the year prior to the survey of US$500 or more from each of three groups: children, other relatives or friends, and parents. We combined responses to these questions to form a dichotomous variable of receipt of financial support, where 1 = yes and 0 = no. Third, potential social support was measured with one indicator, child geographic proximity. Although we did not locate any previous research that included proximity of kin as a measure of social relationships that may be related to dental care service utilization, we include such a measure because for older persons having someone living close by may be indicative of the potential for instrumental support (e.g., transportation). Child proximity was measured by whether one or more of the respondent’s children lived with 10 miles of them (1 = yes, 0 = no). If the respondent did not report any living children, they were assigned a value of 0.
Covariates
Many older persons do not have dental insurance, in part because coverage by Medicare (restorative care only) and Medicaid (typically for emergency services only) is limited and in part because when private coverage is available, it is provided by an employer (Moeller et al., 2010). The majority of the older population did not participate in the labor market. Lack of dental insurance is a major reason why some older persons did not visit the dentist regularly. The absence of dental insurance coverage is shown routinely to be related to a lower likelihood of visiting a dentist or seeking other types of dental care in the United States (Kiyak & Reichmuth, 2005). We included a measure of dental insurance on the basis of two questions: (a) If respondents visited a dentist in the 2 years prior to interview, they were asked, “Were your dental expenses completely covered by insurance, mostly covered, only partially covered, or not covered at all by insurance?” and (b) if respondents reported not visiting a dentist in the 2 years prior to interview, they were asked, “If you did need to see a dentist, would you expect any of the cost to be covered by insurance?” If respondents reported they had received coverage or had coverage in case they needed to see a dentist, they were considered to have dental insurance (1 = yes, 0 = no).
Research showed that age is associated with visiting a dentist, such that as age increases, the likelihood of seeing a dentist decreases (Skaar & Hardie, 2006). Age was included as a continuous variable (range 65-97 years). Gender is related to use patterns, with women generally being more likely to visit a dentist than men are (Skaar & Hardie, 2006). A dichotomous variable was created for gender (1 = female, 0 = male). Race and ethnic group differences in utilization of dental services have also been identified in previous research (Ramirez, Ahluwalia, & Teresi, 2011). Non-Hispanic Whites are more likely to visit a dentist than are Blacks and Hispanics (Kiyak & Reichmuth, 2005). We generated a set of three dichotomous race and ethnic variables that included non-Hispanic Black, non-Hispanic White (reference group in regression analyses), and Hispanic (Hispanics could be of any race).
Socioeconomic status (SES) is related to dental care in later life, whereby those with more current income are more likely to obtain preventive and restorative services (Cohen et al., 2011; Kiyak, 1987; Skaar & Hardie, 2006). The two indicators of SES employed in this analysis were education and household income (Kiyak & Reichmuth, 2005). Number of years of education was included as a continuous variable (range 0–17 years or more). Annual household income was also included (logged dollars). We used the household income variable provided by the RAND Corporation, which imputed values for missing data.
General health and disability status have also been found to limit the amount of engagement with the dental care service profession (Lai & Hui, 2007; Wu et al., 2007). Dolan et al. found that older persons reporting more ADL and IADL limitations were less likely to visit a dentist. Disability status was measured with two variables. First, the number of ADL limitations (bathing, dressing, eating, transferring in and out of bed, toileting) are summed (range = 0-5). Second, the number of Instrumental Activities of Daily Living (IADL) limitations (difficulty with preparing meals, shopping, using the phone, taking medications, and handling money) are summed (range = 0-5). Older persons who self-reported fair or poor health have been found to go to the dentist less frequently than those who reported excellent, very good, or good health (Brown et al., 1999; Dolan, Peek, Stuck, & Beck, 1998). In the HRS, self-reported health was based on a 5-category scale, including poor, fair, good, very good, and excellent. We dichotomized this variable into 1 = fair or poor health and 0 = good, very good, or excellent heath. We also included a measure of depression based on a short version of the CESD depression scale (0-8). Results regarding the direction of the relationship between depression and other emotional problems and dental care service utilization are mixed (Marino et al., 2007; Wu et al., 2005). Presence of chronic health conditions have been identified as a correlate of underutilization of dental services (Ramirez et al., 2011; Wu et al., 2007). We employed a count of number of health conditions, including arthritis, cancer, diabetes, heart problems, hypertension, lung disease, memory-related disease, psychiatric problems, and stroke (range 0-9). People who have smoked or who currently smoke have also been hypothesized to see dental professionals less often than nonsmokers (Dolan et al., 1998; Wu et al., 2007). Smoking behavior was measured as 1 = currently smoked and 0 = did not currently smoke.
Analytic Strategy
We evaluated whether multicollinearity created any statistical bias in the regression estimates. The results of tests including variance inflation factors (VIF) and tolerance levels indicated relationships among the covariates did not yield any bias. Correlations among the social relationship variables were moderately strong. In the regression models, we examined the social relationship indicators one at a time. All analyses were based on weighted data (mean-centered respondent weight). Although several weights were provided in the HRS data file, respondent weights are recommended when using individuals as the units of analysis (HRS, 2012). Mean-centered weights did not increase sample size. We employed the “svy” option in STATA to correct the standard errors of estimates for the multistage cluster sample design of the HRS (STATA 10).
We began our analyses by describing the study sample using the variables identified above. We also described the sample by whether or not the respondent had visited a dentist in the past 2 years. We then generated a series of binomial logistic regression models, with hierarchical inclusion of sets of variables. The first model included only the social relationship indicator without any adjustment for covariates. The second model introduced the demographic controls. The third model introduced the socioeconomic and dental insurance variables. The final model (full model) introduced the health and disability indicators. The results for the final (fully adjusted) models are reported in the Appendix.
Results
The descriptive characteristics for dental visits, demographic variables, socioeconomic characteristics, and health are presented in Table 1. Approximately three quarters (77.4%) of the sample had visited a dentist in the 2 years prior to the interview. The mean age was 74.2 years. The majority of the sample participants were female (56.4%), with nearly 90% non-Hispanic White, 6% non-Hispanic Black, and 4.0% Hispanic. Approximately one third (36.3%) of the total sample had some kind of dental insurance. The respondents reported 13.0 mean years of education and a median annual household income of US$38,403. Approximately one quarter (23.5%) self-reported their health as fair or poor. The level of disability was relatively low, with 0.26 ADL limitations reported, on average, and 0.19 IADL limitations reported, on average. Respondents reported an average of about one depressive symptom (1.2) and less than one in ten (8.9%) reported that they currently smoked. With the exception of age and gender, these covariates were statistically significantly related to whether an older person visited a dentist in the past 2 years. In general, persons who did not visit a dentist were more likely to be non-Hispanic Black or Hispanic, had lower SES, had more health concerns, and were more likely to smoke.
Dental Visits, Demographic, Socioeconomic, and Health Characteristics (% Unless Otherwise Noted).
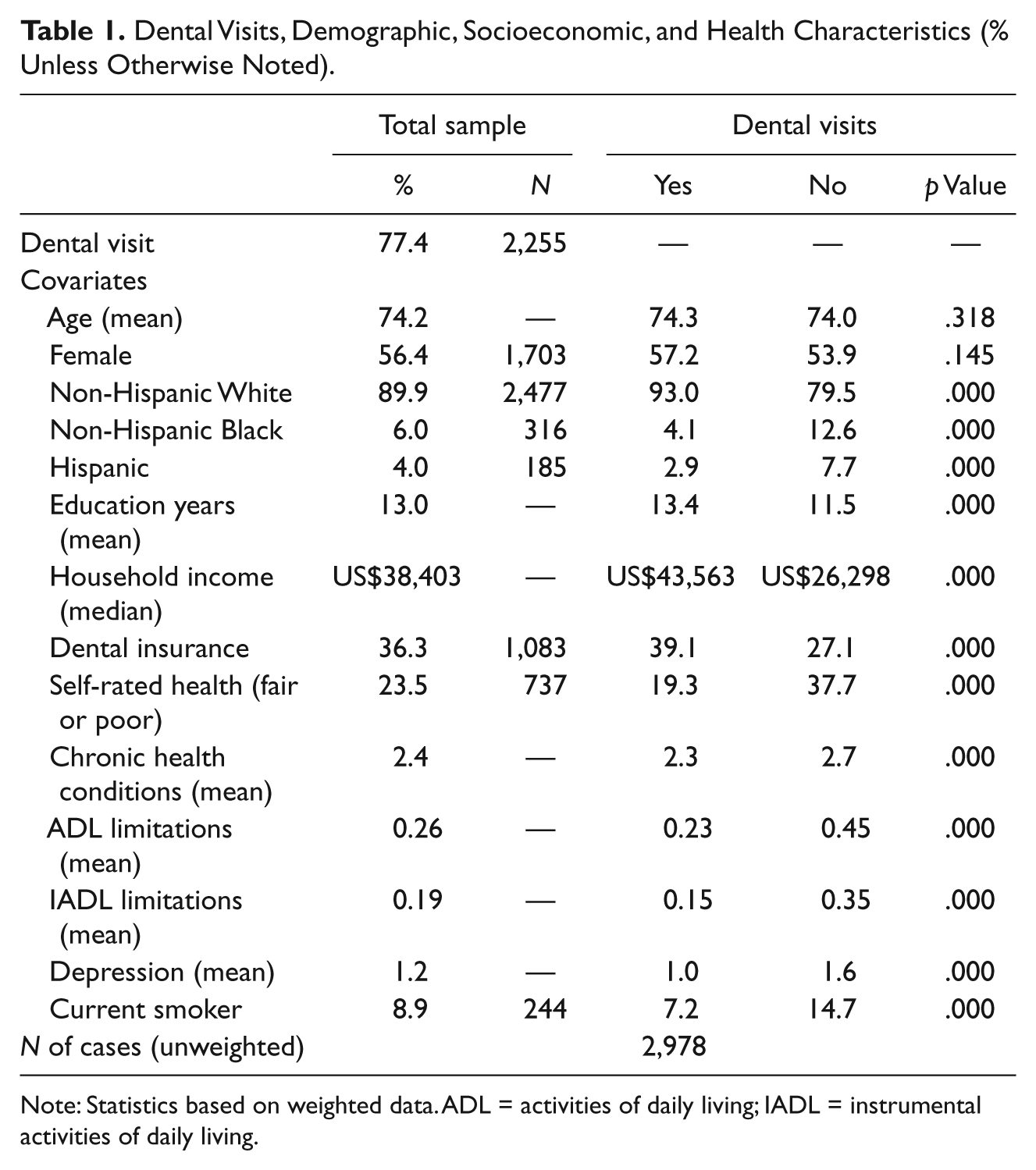
Note: Statistics based on weighted data. ADL = activities of daily living; IADL = instrumental activities of daily living.
A detailed description of the social relationship characteristics of the sample is presented in Table 2; social integration characteristics were presented first. A majority of respondents were currently married (57.7%). For the global indicator of social interaction, the mean score was 5.9 (within a range of 0-9). The indicators of social interaction with children, other family, and friends ranged from 1.8 (other family) to 2.1 (children and friends), within a range of 0 to 3. The mean score on the loneliness index was 1.6 (range 1-3). In terms of social participation, 57.5% of the respondents reported attendance at religious services at least monthly. Our analyses also showed that approximately one third (37.6%) of the respondents participated in a volunteer activity in the previous year. Among those who volunteered, about one in five engaged in a modest amount of activity (1-99 hr) and about the same fraction volunteered at a higher level (100 hr or more). The mean score on the neighborhood social cohesion index was 5.7 (range for the index was 1-7).
Social Relationship Characteristics (% Unless Otherwise Indicated).
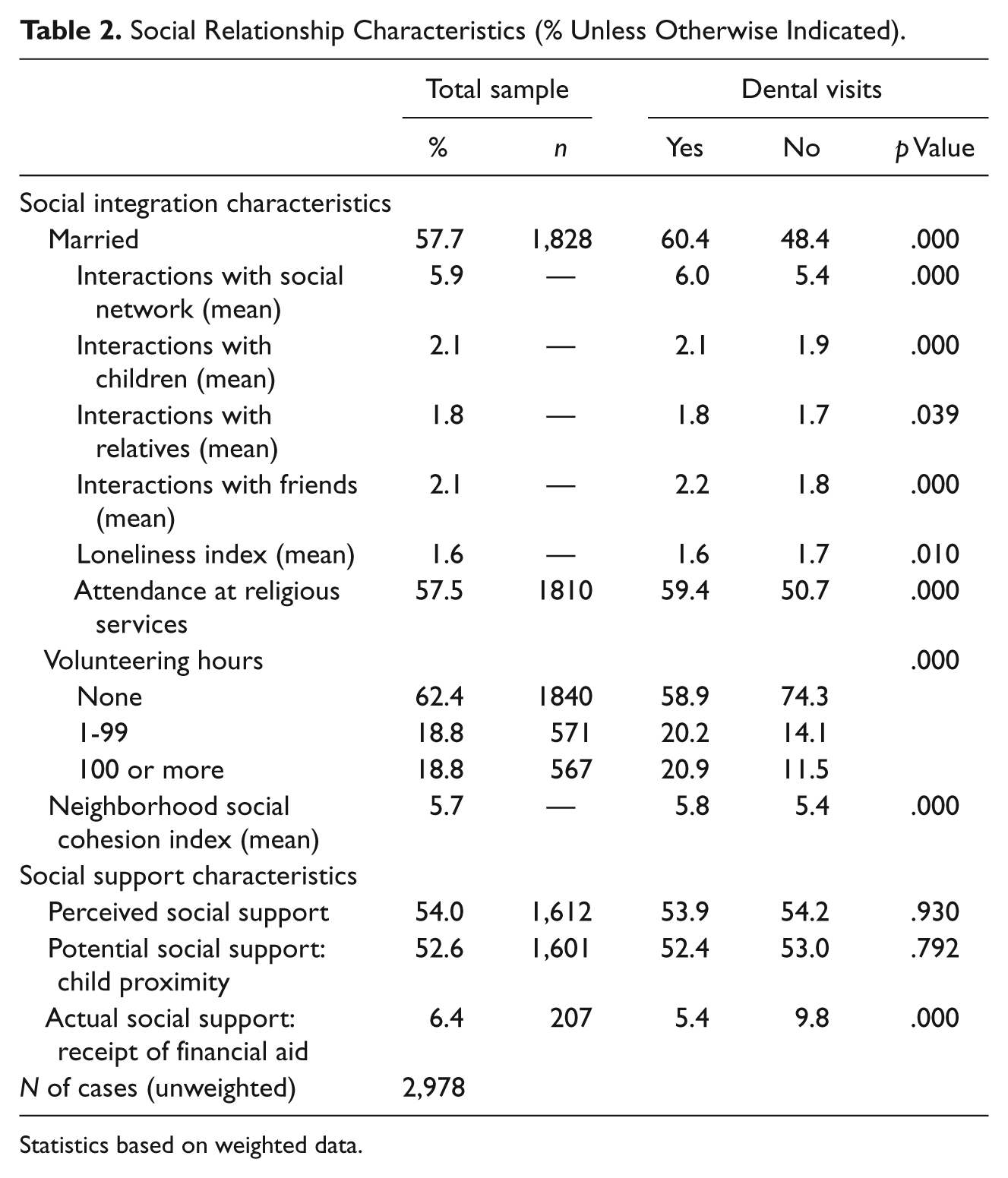
Statistics based on weighted data.
Social support characteristics show that for perceived social support, approximately one half of the sample respondents (54.0%) reported if they needed someone to provide help with an ADL (or already received such support), they had someone in their network who would provide assistance. Receipt of financial support in the amount of US$500 or more in the previous year for this sample was relatively uncommon (6.4%), and more than half of the respondents had one or more children who lived within 10 miles of them (52.6%).
We next compared the social relationship characteristics of those who visited a dentist with those who did not visit a dentist. Compared to respondents who did not visit a dentist, those who visited a dentist had a higher rate of marriage and reported higher mean levels of social interaction with network members. Social participation was higher for those who had visited a dentist for all three indicators. Respondents who visited a dentist had slightly lower scores on the loneliness index. In terms of social support characteristics, perceived social support and child proximity showed no statistically significant difference with regard to whether a dentist was visited. Somewhat unexpectedly, those respondents who visited a dentist reported a lower percentage of receiving financial support than those who did not visit a dentist.
Binomial logistic regression results are presented in Table 3. Again, we presented the results (odds ratios and 95% confidence intervals) in four hierarchical steps (Model 1, unadjusted; Model 2, adjusted for demographic characteristics; Model 3, adjusted for socioeconomic factors; and Model 4, adjusted for health and disability). In the unadjusted models, the likelihood of visiting a dentist was associated with most of the indicators of social relationships and in the expected direction. In terms of the results for the models of each of the social integration characteristics, respondents who were married, who had higher levels of social interaction, who were less lonely, who attended religious services more often, who volunteered, and who lived in socially cohesive neighborhoods were more likely to have visited a dentist in the past 2 years.
Binomial Logistic Regression Results: Dental Visits With Social Relationship Characteristics (Odds Ratios and 95% Confidence Interval).

Model 1 is unadjusted for covariates.
Model 2 is adjusted for demographic factors.
Model 3 is adjusted for income, education, and dental insurance coverage.
Model 4 is adjusted for health and disability factors.
In terms of social support characteristics, the unadjusted models showed that respondents who received financial aid were less likely to have visited a dentist in the past 2 years. There was no association between visiting a dentist and perceived social support or potential social support (having children living within 10 miles). In most cases, these results remained statistically significant after adjusting for demographic and socioeconomic characteristics. The exception to this pattern was for interactions with children, which became statistically nonsignificant when adjusting for socioeconomic factors. After adjusting the models for self-reported health, disability status, number of chronic health conditions, depressive symptoms, and smoking status, the relationship among these indicators of social relationships became statistically nonsignificant. Two indicators of social relationships remained statistically significant after introducing health and disability factors—attendance at religious services and receipt of financial aid. In addition, the geographic proximity with children and dental visits relationship became statistically significant after introducing controls for health and disability.
To conserve space, we did not report the full results for each step of our modeling strategy (results available upon request). However, in the Appendix we provided the results for the fully adjusted models (Model 4) for each social relationship indicator. Across all of the models, the results were generally consistent with the bivariate results reported in Table 1. As age increased, the likelihood of visiting a dentist increased. Women were more likely to visit a dentist than men. Compared to non-Hispanic Whites, non-Hispanic Blacks were less likely to visit a dental care provider, but there was no difference between Hispanics and non-Hispanic Whites. Respondents with higher education, more household income, and dental insurance were also more likely to have visited a dentist. Depressive symptoms were not related to dental care service utilization. Poor self-rated health, more IADL limitations, and being a current smoker were negatively related to the likelihood of seeing a dentist. The introduction of the health covariates reduced the statistical significance of several of the social relationship indicators. It was likely that health and social relationships were related such that those in the poorest health had fewer social relationships and thus were less likely to visit a dentist (see below).
Discussion
For a nationally representative sample of older persons, we described the empirical relationships for the likelihood of visiting a dentist with several indicators of two domains of social relationships: social integration and social support. About three quarters (77.4%) of the HRS respondents sample had visited a dentist in the 2 years prior to the interview. This figure was higher than other national estimates based on a single-year reference period (Dolan et al., 2005). We also found that many of the indicators of the two domains of social relationships considered here (social integration and social support) were related to an increased likelihood of seeing a dental health care professional. This was consistent with research in the area of general health (House et al., 1988), general health care service utilization (Counte & Glandon, 1991; Wolinsky & Johnson, 1991), and more specifically, with the somewhat limited research on dental care service utilization (Kiyak & Reichmuth, 2005). For example, compared to being widowed, divorced, or never married, being married was related to an increased likelihood of seeking dental care. Marital status has long been established as an important social condition for protecting health and well-being (House et al., 1988). Also, it was likely that interacting socially with others, both in informal situations (e.g., with friends; in the neighborhood) and in more formal circumstances (e.g., attending religious services; volunteering), provided older persons with the motivation and resources to seek preventive care and restorative treatment. Furthermore, perceived social isolation, measured here with a loneliness index, was related to a lower probability of seeking dental care.
Two of our findings were somewhat unexpected. First, persons who received financial aid from children, other family members, and friends were less likely to visit a dentist than those who did not. It may be that those who received financial aid were sufficiently financially distressed that using these external resources for dental care was considered less important than for seeking other kinds of health care or for taking care of other economic needs. It may also be that receiving tangible support, like financial resources, may lower self-esteem and sense of control by increasing a sense of dependency, in turn, promoting less positive oral health behaviors, such as visiting a dentist.
We also found that in the unadjusted models and the models adjusted for age, gender, race, ethnicity, and SES living close to one or more children was not associated with going to a dentist. However, once we adjusted for subjective evaluations of health, disability status, depressive symptoms, number of health conditions, and current smoker status, the relationship between child proximity and visiting a dentist became statistically significant. Under these modeling circumstances, those older persons who reported living within 10 miles of at least one child were more likely to visit a dentist than those older persons who did not have a child living near them. This may have been the result of a suppressor effect among one or another of the health variables.
There are likely a number of pathways through which social relationships influence dental care service use. One possible pathway through which social integration may have been related to dental care service utilization is oral health literacy (Lee, Arozullah, & Cho, 2004). The lack of information on why HRS respondents visited a dentist and the lack of information on oral health literacy means we cannot evaluate this issue directly. However, observers note that many older persons have low dental health literacy, in part, because they were socialized at a time when oral health and dental care service utilization were seen as less important (Kiyak & Reichmuth, 2005). It is possible that the receipt of social support may have alleviated low dental health literacy by overcoming limitations in knowledge of good oral health and by reinforcing norms of appropriate self-care.
As noted earlier, social integration is likely to have indirect relationships with dental care utilization. It is possible that higher levels of social integration—both informally with spouses, children, and friends and engagement in formal organizations—improves self-esteem, provides meaning to life, enhances the sense of control over one’s life, and provides social control for positive health behaviors. It is also possible that persons with greater levels of social integration are more likely to appraise their relationships in a positive light, consequently feeling better about themselves, and believing it is necessary to take care of their oral health. If social integration has these benefits, including reducing loneliness, then both preventive and restorative dental care service utilization may be more likely.
This study, however, did not evaluate the quality of social relationships between the respondents and their social network members. Not all social relationships are positive, and conflicted and problematic social relationships may not promote health care service utilization and overall health. When persons are embedded in social groups whose health behaviors and values are detrimental to well-being and when interpersonal relationships are conflicted, health outcomes and health behaviors may be negative (Ingersoll-Dayton, Morgan, & Antonucci, 1997; Rook, 1984; Stafford, McMunn, Zaninotto, & Nazroo, 2011). Future research should address how both the quantitative and qualitative nature of social relationships is related to dental care service utilization.
Future research should also examine how the association between social relationships and oral health is mediated by dental care service utilization for a better understanding of the etiology of good oral health. One pathway in the model of social environment and oral health would take into consideration how social relationships affect under-the-skin biological processes that, in turn, are related to oral health. Such studies may also help with designing interventions for better oral health. However, Cacioppo and Hawkley (2003) note that most interventions to increase social connectedness with the goal of improving overall health do not seem to produce much in the way of positive outcomes (however, see Fried et al., 2004). This is one reason why understanding these complex pathways to optimal oral health in later life needs additional investigation.
Nevertheless, there are policy implications associated with this research. Older adults have limited dental care insurance coverage compared to other adults and are less likely as an age group to see a dentist on a regular basis. This is the case, in part, because most older persons are out of the labor force and thus do not have employer-based dental insurance coverage (82% of our study sample participants were not working) and only limited dental care coverage is provided by Medicaid and Medicare. The lack of widespread, publicly supported, coverage combined with cohort differences in attitudes about dentists and norms regarding caring for one’s dental needs makes understanding the social environment of older persons that much more important, especially when it comes to access to and use of dental care services (see Kiyak & Reichmuth, 2005). Given the link between oral health and general well-being among older persons, it would be prudent to find the resources to provide dental insurance under the social insurance programs available to older persons in the United States.
Limitations
This study was limited to cross-sectional data, and therefore, we did not account for change in dental care service utilization over time or account for changes in social relationships. Because the data were cross-sectional, we cannot make causal statements about the relationship between social relationships and dental care service utilization. In fact, social relationships and health care service utilization may both be endogenous and influenced by health and disability status. Longitudinal data and corrections (e.g., identification of instrumental variables for a two-stage regression model) for this potential endogeneity are needed to understand better the causality among these variables.
We also did not have indicators of oral health status, which some research has found to be related to utilization of dental services, although the research findings are equivocal (Wu et al., 2007). Some observers have commented on the reduction in social interaction and participation among older persons as they age; thus, these issues need further evaluation when it comes to dental care service utilization and overall oral health. We also do not know the reason for the dental visit; it may have been for preventative or restorative purposes. It may be that social relationships have a different effect on dental visits based on the specific reason for the visit. It may be, for example, that social relationships are more impactful for routine visits and less so for restorative care. Additional research with other data sources is necessary to address this issue.
We noted there may be cohort differences that influence the probability of seeking dental care in later life. Baby boomers may be different from the depression cohort when it comes to the relative importance placed on oral health and on experiences that shape attitudes about dentists. We did not examine cohort effects in this study, but this represents an additional avenue for future investigation.
Conclusion
We found evidence for an association between dental care service utilization and a variety of indictors of social integration and social support among a sample of older persons in the United States using nationally representative data from the HRS. These results were generally consistent with results from other studies in developed nations and with the relatively small number of studies in the United States. Additional research on this topic is required to understand more fully the complex relationships among the social environment and oral health.
Footnotes
Appendix
Results for Fully Adjusted Models (Odds Ratios)
| (1) | (2) | (3) | (4) | (5) | (6) | (7) | (8) | (9) | (10) | (11) | (12) | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Married | 1.232 | |||||||||||
| Children proximity | 1.268* | |||||||||||
| Interactions with social network | 1.043 | |||||||||||
| Interactions with children | 1.059 | |||||||||||
| Interaction with relatives | 1.029 | |||||||||||
| Interaction with friends | 1.121 | |||||||||||
| Loneliness index | 1.181 | |||||||||||
| Attendance at religious services | 1.300* | |||||||||||
| Volunteer no hours (reference category) | ||||||||||||
| 1-99 hr | 1.250 | |||||||||||
| 100+ hr | 1.295 | |||||||||||
| Neighborhood social cohesion | 1.084 | |||||||||||
| Perceived social support | .903 | |||||||||||
| Receipt of financial aid | .616* | |||||||||||
| Age | 1.032** | 1.030** | 1.031** | 1.030** | 1.030** | 1.031** | 1.029** | 1.027** | 1.030** | 1.029** | 1.029** | 1.029** |
| Female | 1.507** | 1.438** | 1.409** | 1.431** | 1.439** | 1.406** | 1.436** | 1.390** | 1.420** | 1.442** | 1.450** | 1.476** |
| Non-Hispanic White | ||||||||||||
| Non-Hispanic Black | 0.414*** | 0.406*** | 0.413*** | 0.410*** | 0.406*** | 0.419*** | 0.405*** | 0.375*** | 0.397*** | 0.422*** | 0.409*** | 0.435*** |
| Hispanic | 0.881 | 0.922 | 0.912 | 0.902 | 0.901 | 0.917 | 0.904 | 0.876 | 0.913 | 0.932 | 0.900 | 0.922 |
| Education | 1.192*** | 1.198*** | 1.186*** | 1.188*** | 1.189*** | 1.182*** | 1.189*** | 1.191*** | 1.183*** | 1.189*** | 1.189*** | 1.193*** |
| Household income | 1.378** | 1.441*** | 1.425*** | 1.430*** | 1.435*** | 1.425*** | 1.444*** | 1.426*** | 1.426*** | 1.427*** | 1.432*** | 1.426*** |
| Dental insurance | 1.889*** | 1.881*** | 1.885*** | 1.881*** | 1.880*** | 1.882*** | 1.879*** | 1.875*** | 1.876*** | 1.891*** | 1.876*** | 1.870*** |
| Self-rated health (fair or poor) | 0.705** | 0.704** | 0.721** | 0.716** | 0.713** | 0.726** | 0.713** | 0.727* | 0.730* | 0.719** | 0.710** | 0.707** |
| Chronic health conditions | 0.952 | 0.946 | 0.949 | 0.949 | 0.950 | 0.951 | 0.949 | 0.950 | 0.952 | 0.952 | 0.951 | 0.954 |
| ADL limitations | 0.915 | 0.915 | 0.916 | 0.916 | 0.915 | 0.912 | 0.913 | 0.923 | 0.915 | 0.919 | 0.906 | 0.912 |
| IADL limitations | 0.835* | 0.838* | 0.848* | 0.843* | 0.841* | 0.855* | 0.841* | 0.850 | 0.850 | 0.842* | 0.829* | 0.845 |
| Depression | 0.978 | 0.978 | 0.976 | 0.976 | 0.974 | 0.975 | 0.978 | 0.978 | 0.976 | 0.981 | 0.971 | 0.974 |
| Current smoker | 0.569** | 0.561** | 0.570** | 0.563** | 0.560** | 0.575** | 0.553** | 0.581* | 0.593* | 0.562** | 0.560** | 0.562** |

Note: ADL = activities of daily living; IADL = instrumental activities of daily living.
p < .05. **p < .01. *p < .001.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.