
Abstract
It is acknowledged that advanced age is a risk factor for both falling and disability. Every year approximately one-third of the community-dwelling population aged 65 years and older experience a fall at least once, and by the age of 80 this proportion increases to 50% (O’Loughlin, Robitaille, Boivin, & Suissa, 1993; Tinetti, Speechley, & Ginter, 1988). These falls account for 87% of fractures in the elderly (Fife & Barancik, 1985). Moreover, aging is also perceived as a risk factor for disability. Among the population of 70 years and older, 20% to 30% report disability in Instrumental Activities of Daily Living (IADL) or Activities of Daily Living (ADL) (Manton, & Land, 2002). Therefore, it is worthwhile to identify clinically applicable tools/tests that can predict falls and disability in the older population.
Standardized physical performance tests are commonly used in aging studies for their ability to predict subsequent health-related outcomes such as falls and disability. For example, higher scores on the Short Physical Performance Battery (SPPB) have been reported to be predictive of lower likelihood of disability in ADL and mobility-related disability at 4-year follow-up in older persons older than 70 years of age (Guralnik, Ferrucci, Simonsick, Salive, & Wallace, 1995). The SPPB includes a standard sit-to-stand test, which involves recording the time to transfer from a sitting position to standing five times successively without using the upper extremities (5tSTS) (Guralnik et al., 2000; Lord, Murray, Chapman, Munro, & Tiedemann, 2002). Because of the simplicity in its administration in both clinical and research environments, 5tSTS is often used for assessing physical function of older persons, particularly lower limb function, (Ferrer, Lamarca, Orfila, & Alonso, 1999; McCarthy, Horvat, Holtsberg, & Wisenbaker, 2004) and predicting subsequent health-related outcomes. More recently, Wang et al. (2011) performed a study in 287 community-dwelling older adults in order to examine the predictive validity of different types of mobility-related performance tests to predict older adults’ mobility disability status after a 2-year period. The results showed that adjusted for age and gender, 5tSTS could significantly predict older adults’ mobility disability status 2 years later. Similar to 5tSTS, the ability to stand up from a sitting position once has also been used to predict health-related outcomes, such as falls. In Nevitt et al.’s study (1989) of participants aged 60 and above, having difficulty standing up from a chair without arm support was reported to be an independent predictor of multiple falls (≥2 falls) over a 1-year period. However, in their study, being unable or requiring more than or equal to 2 s to stand up were both defined as “having difficulty in standing up from a chair,” which was, to some extent, different from commonly defined “inability to complete sit to stand” (Szulc, Claustrat, Marchand, & Delmas, 2003).
It is evident that the sit-to-stand test, especially 5tSTS test, is a useful measure of physical function to predict health-related outcomes in older adults. However, the independent role of inability to complete 5tSTS and the time to finish 5tSTS if completed to predict subsequent disability in ADL and IADL, and falls requires further research. The purpose of this study was to investigate whether the inability to finish 5tSTS and the time to perform 5tSTS at baseline can predict falls, fall-related fracture, and disability in ADL and IADL at 3-year follow-up in mobile older persons.
Materials and Method
Participants
The InCHIANTI study population is a representative population of older persons living in the Chianti area (Tuscany, Italy). The overall purpose of the InCHIANTI study is to translate epidemiological research into designing geriatric clinical tools and develop therapeutic approaches for older persons with mobility problems (the website of the InCHIANTI study). The study design and data collection have been previously described (Ferrucci et al., 2000). The present study used the baseline data of 1998 and the 3-year follow-up data. A total of 948 mobile (who were able to walk 7 m at a self-selected speed without using an assistance of a walker) older participants (age ≥ 60) with a Mini Mental State Examination (MMSE) score ≥ 18 (Tombaugh, & McIntyre, 1992) were initially included. For the current analysis, 562 participants (out of the 948 participants) who were free from falls and ADL- and IADL-related disability at baseline were included. The protocol was approved by the ethical committee of the Italian National Institute of Research and Care of Aging and participants provided informed consent.
Outcome Measures
5tSTS performance
5tSTS performance was evaluated at baseline. Participants were asked to stand up from a standard chair (chair height: 0.46 m) as quickly as possible for five times without hand-support. Two outcomes were recorded, the ability to complete 5tSTS and the time to finish it for those who completed the test. The 5tSTS performance was then divided into five categories where Group 5 (worst performance) = inability to complete the test, Group 4 = test completed in > 16.6 s, Group 3 = test completed in 13.7–16.6 s, Group 2 = test completed in 11.2–13.6 s and Group 1(best performance) = test completed in < 11.2 s (Guralnik et al., 1994).
Falls and disability
Self-reported number of falls and fall-related fractures were recorded retrospectively (for the previous year) at baseline and at the 3-year follow-up. The participants were asked the questions “Did you ever fall down in the last 12 months? If yes, how many times did you fall down in the last 12 months?” and “If you were injured when you fell, what was the worst injury?” in order to record falls and fall-related fractures.
Disability status at both baseline and 3-year follow-up were assessed using questionnaires. Participants were asked to report the number of ADLs) including bathing, dressing, eating, getting into and out of bed or chair, walking across a room, and using the toilet, for which they needed help. The need for assistance on any of these activities was recorded as ADL-related disability. The IADLs included preparing meals, shopping for groceries, managing money, making phone calls, light housework, heavy housework, getting to places outside of walking distances, and managing medications. The participants who needed help for any of these activities were regarded as having IADL-related disability. For prediction of both incident falls and disability, the participants who did not report a fall in the previous year and ADL- and IADL-related disability at baseline were included. For the prediction of fall-related fracture, only the participants who reported a fall/falls at the follow-up were included in the analysis. Most of the participants (11/15) who had ADL-related disability at the follow-up also had IADL-related disability, with only four participants who had ADL-related disability without having IADL-related disability.
Covariates
Potential confounders including age, sex, body mass index (BMI), depressive symptoms, handgrip strength, and mobility disability were recorded at baseline mainly because of their association with falls, ADL-, or IADL-related disability. Old age (Dargent-Molina et al., 1996), high BMI (Wallace et al., 2002), depression and impaired mobility (Tromp et al., 2001), and low handgrip strength (Stalenhoe, Diederiks, Knottnerus, Kester, & Crebolder, 2002) are all fall-risk factors. Moreover, gender disparities in fall risk have also been observed (Stevens & Sogolow, 2005). In addition, age (Dargent-Molina et al., 1996), BMI (Sharkey, Branch, Giuliani, Zohoori, & Haines, 2004), and depressive symptoms (Holroyd, Currie, & Wooten, 2005) are also associated with development of ADL- or IADL-related disability. Depressive symptoms were assessed using the Center for Epidemiological Studies Depression scale (CES-D; Radloff, 1977). Handgrip strength was measured using a handheld dynamometer (hydraulic hand BASELINE, Smith & Nephew, Agrate Brianza, Milan, Italy). Participants were asked to perform the task twice with each hand, and the maximum strength recorded in the four trials was used for the analyses. Mobility disability was ascertained based on the 7 m walking test and self-report. Participants were regarded as having mobility disability if any of the following were present: self-selected gait speed slower than 0.8 m/s in the 7 m walking test; self-reported inability to walk up a flight of 12 to 15 steps without any help or self-reported difficulty in walking a quarter mile distance without stopping.
Statistical Analysis
Separate logistic regression analyses were performed to test the ability of 5tSTS performance to predict incident falls, fall-related fracture, and ADL- and IADL-related incident disability. The regression analyses were adjusted for the covariates that were different (p < .1) between the two groups of interest (i.e., incident falls vs. no fall, fall-related fracture in incident fallers at the follow-up vs. no fracture, incident ADL-related disability vs. no ADL-related disability and incident IADL-related disability vs. no IADL-related disability). Statistical analyses were performed using SPSS version 19.0 (SPSS Inc. IL, USA). A p value of < .05 was considered to be statistically significant.
Results
The characteristics of the 948 participants and the two groups of participants used in the analysis (fall, ADL- and IADL-related disability prediction, and fall-related fracture prediction) and the participants in the five 5tSTS groups are displayed in Table 1a and 1b.
Characteristics of the Study Populations.
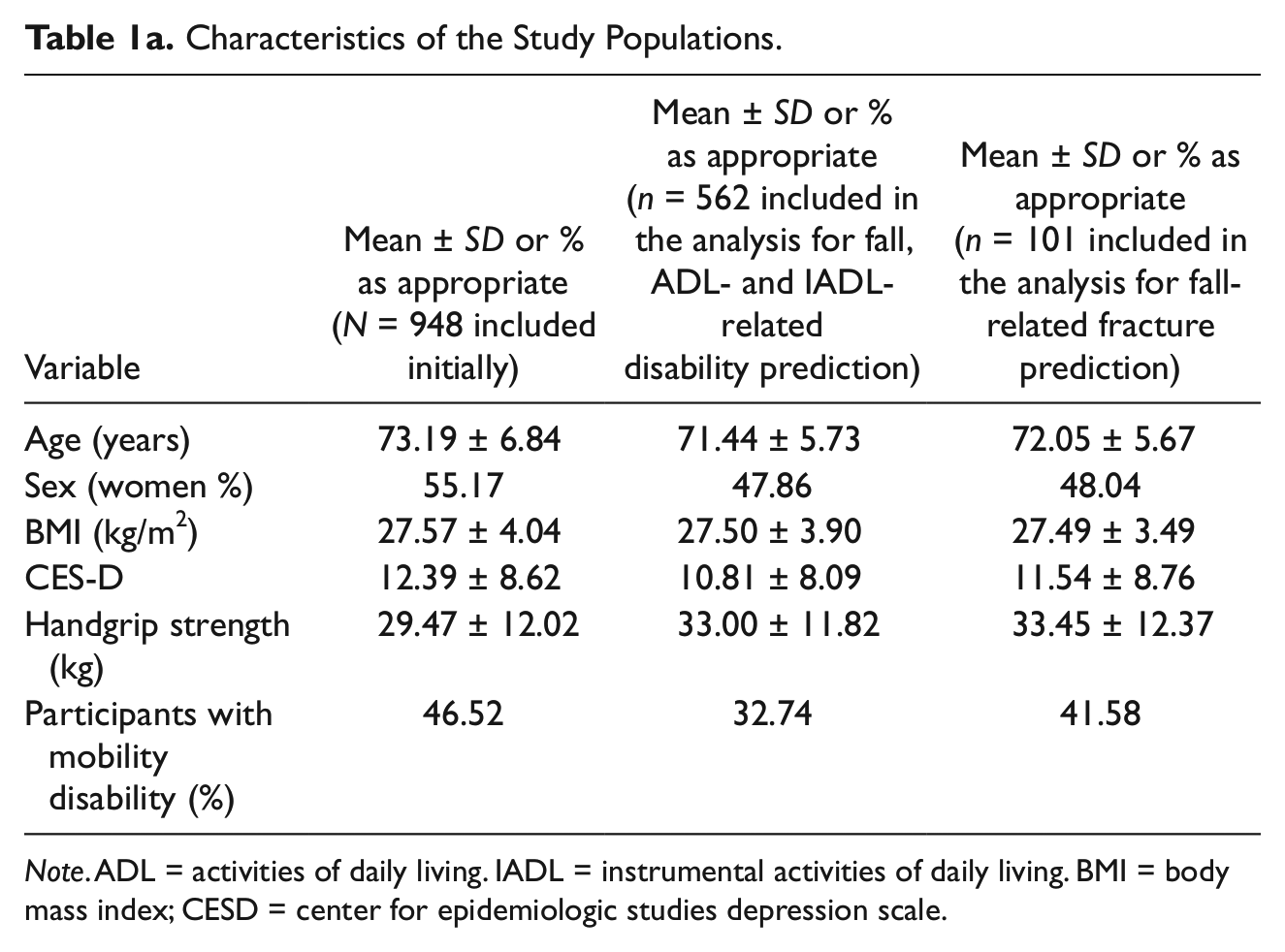
Note. ADL = activities of daily living. IADL = instrumental activities of daily living. BMI = body mass index; CESD = center for epidemiologic studies depression scale.
Characteristics of the Participants in the Five 5tSTS Groups.

Note. BMI = body mass index; CESD = center for epidemiologic studies depression scale.
Out of 562 participants who did not report any fall and ADL- and IADL-related disability at the baseline, 101 (49 women) reported at least one fall at the follow-up. Amongst the fallers, 10 (seven women) participants reported fall-related fracture/s. Out of the 562 participants, 15 (six women) reported incident ADL-related disability and 60 (44 women) reported incident IADL-related disability at the follow-up, respectively.
The results of fully adjusted logistic regression models are presented in Table 2. Inability to complete 5tSTS was marginally associated with incident falls, and significantly associated with ADL- and IADL-related incident disability at the follow-up. For the participants who could not finish 5tSTS (Group 5), the odds of reporting a fall at the follow-up were 4.22 times (OR = 4.22, CI = 0.82, 21.71, p = .09) greater than those who required the shortest time (< 11.2 s). For those who were in Group 5, the odds of developing ADL-related disability were 24.70 times (OR = 24.70, CI = 2.83, 215.44, p < .01) greater than those in Group 1. For the individuals in Group 3, Group 4, and Group 5, the odds of incident IADL-related disability were 2.49 times (OR = 2.49, CI = 0.88, 7.06, p = .09), 4.22 times (OR = 4.22, CI = 1.17, 15.26, p = .03) and 17.10 times (OR = 17.10, CI = 1.87, 156.39, p = .01) greater than those in Group 1, respectively (Table 2).
Results of Logistic Regression Analysis with 5tSTS as a Predictor of Falls, Fall-Related Fracture, ADL- and IADL-Related Disability at 3-Year Follow-up.

Note: ADL = activities of daily living. IADL = instrumental activities of daily living. Group 5 = inability to stand up without hand support or inability to complete the test, group 4 = test completed in > 16.6 s, group 3 = test completed in 13.7 – 16.6 s, group 2 = test completed in 11.2 to 13.6 s and group 1 = test completed in < 11.2 s). aadjusted for mobility disability. bnot adjusted for covariates. cadjusted for age and mobility disability. dadjusted for age, sex, center of epidemiological studies depression scale score, mobility disability, and handgrip strength.
Discussion
Inability to complete 5tSTS at baseline was marginally associated with self-reported fall/s at the 3-year follow-up in this older population. However, neither inability to complete 5tSTS nor the time to finish it was associated with a fall-related fracture. Older persons who could not finish 5tSTS or required longer time to finish it were highly likely to report ADL- and IADL-related disability at the 3-year follow-up. The cognitive condition of participants may have an impact on the data, especially on self-reported records. People with MMSE scores ≥ 18 but < 24 may have mild cognitive impairment, thereby making their responses less valid. However, when the data were reanalyzed excluding the participants with MMSE score < 24 the results remained consistent. To our knowledge, this is the first study that demonstrated the independent role of 5tSTS in predicting incident fall. Previously, Nevitt et al. (1989) reported that difficulty in standing up from a chair without arm support (being unable or taking 2 s or longer to stand up) was an independent predictor of two or more falls over a 1-year period, but was not a predictor of a single fall. However, the study sample of Nevitt et al. (1989) comprised participants who reported at least one fall at baseline. Conversely, the present study did not include participants who reported previous fall/s. Further, unlike the Nevitt et al. study (1989), the present study did not use a time-related cut-off level as an indication of successful indication of completion of 5tSTS even though they were asked to complete 5tSTS as fast as possible.
The association between 5tSTS and self-reported fall/s at the follow-up was only marginal. According to Rubenstein and Josephson’s review (2002) of the findings from 12 studies on risk factors of falls, the most important risk factors are gait and balance disorders or muscle weakness. Our previous work (Deshpande, Zhang, Metter, Guralnik, & Ferrucci, 2011) demonstrated that inability to stand up from sitting without using hand-support was associated with low BMI which may be an indicator of frailty and general muscle weakness (Eva, 2008). Further, lower limb somatosensory impairment was associated with both deterioration in balance (Deshpande, Metter, & Ferrucci, 2010) and inability to stand up from a chair once (Deshpande, Zhang, Metter, Guralnik, & Ferrucci, 2011). Therefore, the possible association between the inability to stand up from sitting without hand-support and balance may also coexist. In this study, the majority of the participants who could not finish 5tSTS (five out of six in Group 5) were actually not able to stand up from sitting without hand-support even once, despite having no time constraint. In spite of the previous studies suggesting the association between 5tSTS and falls, inability to finish 5tSTS in this study was not significantly but only marginally predictive of subsequent falls, and longer time to finish it was not a predictor. It could probably be ascribed to the small number of people in Group 4 (19) and 5 (6) in this study. The ability of 5tSTS to predict subsequent falls deserves further investigation.
In this study, 5tSTS performance was not a predictor of subsequent fall-related fracture. Out of 101 participants who reported a fall/s at the 3-year follow-up, only 10 had fall-related fractures. The small sample size could lower the power of the analysis. In addition, whether or not a fall results in a fracture can be ascribed to bone quality and the force of the fall (Nevitt & Cummings, 1993). A previous study has reported that the time to finish 5tSTS was not associated with bone mineral density, which is a very important measure to assess bone quality, at any skeletal site (Lindsey, Brownbill, Bohannon, & Ilich, 2005). As a result, 5tSTS may not be a significant predictor of subsequent fall-related fracture.
To our knowledge, this is the first study that examined the independent ability of 5tSTS to predict IADL-related disability even after adjusting for multiple confounders. Overall, increasingly poorer performance on 5tSTS was associated with a gradual increase in risk of future disability. The findings suggest that poor performance on 5tSTS at baseline might indicate the existence of a stage of preclinical disability which is an intermediate stage in which impairments have not passed a threshold of severity and only have a mild impact on functional ability that individuals would not recognize as frank disability (Fried, Herdman, Kuhn, Rubin, & Turano, 1991). In our study, inability to complete or longer time to perform 5tSTS may represent preclinical or subclinical disability, which did not concurrently impact IADL. Inability to complete 5tSTS was also a predictor of ADL-related disability. However, 5tSTS performance was a stronger predictor of IADL disability than ADL disability. ADL are basic self-care tasks, while IADLs require more complex skills. A previous study pointed out that IADL are activities requiring greater physical demands and implied the necessity of higher cognitive integrity than ADL (Millán-Calenti et al., 2010). Therefore, it is more likely for older people to reach the stage of preclinical disability of IADL-related disability earlier compared to that of ADL-related disability, which could be recognized by changes in the performance of a highly demanding task such as 5tSTS.
The SPPB, which includes 5tSTS in addition to normal walking speed and standing balance, was predictive of development of subsequent ADL-related disability (Guralnik, Ferrucci, Simonsick, Salive, & Wallace, 1995). In their study, those with the lowest summary SPPB scores (the score used was 4/12 to 6/12 which is a cumulative summary score) were 4.2 times as likely to have disability at four years as those with the highest performance scores. Further, the χ2 analysis in their study demonstrated that overall proportion of participants with 4-year incident ADL disability was significantly different in the four groups based on the time to complete 5tSTS. However, in their study participants who did not complete any of the three tests included in SPPB were excluded, leading to the exclusion of participants who could not complete 5tSTS. When we performed a chi square test to examine the proportion of participants with incident ADL disability at the 3-year follow-up by excluding those who could not complete 5tSTS (i.e., by including only groups 1, 2, 3, and 4), the result showed no significant difference (data not shown). This difference in the results could be ascribed to differences in the populations as well as the length of the follow-up time.
Inability to finish 5tSTS was predictive of development of ADL-related disability; while longer time to finish 5tSTS was not associated with development of ADL-related disability. It is possible that compared to 5tSTS, SPPB, or even self-selected gait speed alone (whose ability to predict ADL-related disability was almost as good as the full SPPB, Guralnik et al., 2000), are better predictors of ADL disability. An SPPB score is derived from a combined score on gait speed at a self-selected pace, standing balance and 5tSTS. Self-selected gait speed and standing balance task included in SPPB are a relatively easier task compared to neuro-mechanically demanding 5tSTS. As a result, it is possible that 5tSTS has a better and more systematic relationship with IADL, which, as mentioned above, requires greater physical demands and necessitates higher cognitive integrity than ADL (Millán-Calenti et al., 2010). Identifying predictors of IADL disability is critical as IADL disability indicates an earlier stage of disablement process and has been found to be closely associated with future frailty (Nourhashémi et al., 2001).
In this study, we adopted the 5tSTS performance categories used in Guralnik et al.’s study (1995). This categorization led to an unbalanced sample size in the five groups, with preponderance of people in the two best-performing categories (Group 1 and 2). This is likely due to a much better general performance status of the InCHIANTI population compared to the population in Guralnik et al.’s study (1995). However, the small number of people (25) in the worst-performing groups (Groups 4 and 5) may cause variability in the estimation of the predictive ability of 5tSTS. Therefore, we used the quartiles calculated in our population (group 5 = inability to stand up without hand-support or inability to complete the test, group 4 = test completed in > 11.6 s, group 3 = test completed in 10.0 – 11.6 s, group 2 = test completed in 8.7 – 10.0 s and group 1 = test completed in < 8.7 s) to further verify such prediction, and the results were similar: inability to finish 5tSTS was marginally associated with falls (p = 0.051, OR = 5.41 CI = 0.99, 29.56), and significantly predictive of ADL (p = 0.02, OR = 20.85 CI = 1.66, 262.04) and IADL-related disability (p = 0.04, OR 10.88 CI = 1.08, 109.88) at the follow-up. Nonetheless, longer time to finish 5tSTS was not significantly associated with falls and development of ADL- or IADL-related disability. Further, when those who could not finish 5tSTS were excluded from this analysis the results showed that being in the worst performing group according the study-specific quartiles (> 11.6 s to complete 5tSTS) was not significantly predictive of any outcome measures (falls and ADL- and IADL-related disability). These findings suggest that unlike the cut-off point of > 16.6 s, the study specific cut-off level of > 11.6 s is not sensitive to detect higher likelihood of developing IADL disability.
Our study has some limitations. First, the study population living in Chianti, Italy is homogenously Caucasian and may not represent multiracial elderly populations living in metropolitan areas. Second, we investigated the ability of 5tSTS to predict outcomes only at the 3-year follow-up; it is possible that 5tSTS can predict subsequent disability and falls at an even shorter follow-up. Falls were recorded for only the year prior to the follow-up and therefore, the number and pattern of falls between baseline and year 2 is not known. Third, the data suggests that the slope of age-related decline in performance of 5tSTS is different in men (0.15) and women (0.21). However, the regression coefficient of the interaction between sex and age in the regression model (time to finish 5tSTS as the dependent variable) was not significant. Furthermore, some of the numbers were too small to perform separate analysis for men and women. Therefore, in the present analyses, the predictive ability of 5tSTS performance was evaluated by adjusting for sex. Lastly, it is possible that there are other potential confounders such as peripheral neuropathy, osteoarticular diseases or lifestyle factors which could be adjusted; however, they are not included, because they may be reflected by the presence of mobility disability, which has already been taken into consideration (Baird & Sands, 2004; Benbow, Wallymahmed, & MacFarlane, 1998; Koster et al., 2007).
In conclusion, 5tSTS performance is only marginally associated with subsequent falls, and a significant predictor of ADL- and IADL-related disability. Older persons who are not able to finish this task may report ADL and IADL disability at the 3-year follow-up. Additionally, compared to those who can complete 5tSTS in < 11.2 s, those who require > 16.6 s to finish 5tSTS also have a significantly higher likelihood of developing IADL-related disability at 3-year follow-up. Overall, the results may indicate that the standard 5tSTS test may be used as a quick screen by clinicians to specifically monitor older persons at the risk of initiation of the disablement (IADL disability) process.
Footnotes
Author’s Note
Reprints will not be available from the authors.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The InCHIANTI study was supported as a “targeted project” (ICS 110.1\RS97.71) by the Italian Ministry of Health and in part, by National Institute on Aging Contracts N01-AG-916413, N01-AG-821336, N01-AG-5-0002, and NIA Grant R01 AG027012 and the Intramural Research Program, National Institute on Aging, NIH.
The authors certify that no party having a direct interest in the results of the research supporting this article has or will confer a benefit on the authors or on any organization with which the authors are associated AND, if applicable, we certify that all financial and material support for this research (e.g., NIH or NHS grants) and work are clearly identified in the title page of the manuscript.