
Abstract
The midlife is an important lifestage with respect to onset of poor functioning. The National Health Interview Survey identified that 15% of persons aged 45 to 64 had some functional limitations or disability and, of those, 50% reported that their functional limitations or disability developed between the ages of 40 and 55 years (Adams & Marano, 1995). Assessment of midlife disablity has largely relied on report of functional limitations or difficulty preforming activities of daily living. In the Study of Women’s Health Across the Nation (SWAN), a longitdinal multisite study of midlife women, 29.6% of the cohort (aged 45-57 years) reported moderate functional limitations and 11.0% reported severe limitations (Tseng et al., 2012). Similarly, data from a British cohort of middle-aged adults reported 3% to 5% prevalence of uppper and lower body limitations at age 43 years; by age 53 years, the prevalence increased to 21% to 28% (Murray et al., 2011). Important correlates of middle-aged disability include obesity (Imai et al., 2008; Nosek et al., 2008), depression symptoms (Wolinsky et al., 2007), and chronic disease comorbidity (Melzer, Gardener, & Guralnik, 2005).
Physical functioning and functional limitations are an important part of the disablement process (Nagi, 1976; Verbrugge & Jette, 1994). While the disablement model (active pathology → impairment → functional limitations → disability) has served as the prevailing guide for disability research, and importantly considers transition to disability as a process, it has been critiqued as focusing only on medical pathologies as the initating factor in the cascade toward disablement. Recognition that functional limitations may be due to factors without a well-defined pathology, or that limitations may be more more social or situational in nature has prompted an international collaboration to develop a biopsychosocial model that includes personal, social, and environmental factors in addition to health conditions as important determinants of disability.
The World Health Organization’s (WHO) International Classification of Functioning (ICF), which conceptualizes disability as a general construct not only defined by underlying pathology, includes 6 domains: (a) diseases/disorders; (b) body functions/structure; (c) activity; (d) participation; (e) environmental factors and (f) personal factors. This biopsychosocial model allows for examination of non-disease-related disability, which may be important among middle-aged populations who may not yet have manifested overt disease. To support assessment of ICF-conceptualized disability, the WHO developed the Disability Assessment Schedule (WHO-DAS). It is recognized and promoted as a universal and standardized measure of disablity, suitable for national and international comparisons of disability prevalence and determinants across populations and age groups (Garin, Ayuso-Mateos, & Almansa, 2010; Ustün et al., 2010).
While the WHO-DAS has been used to examine disability and its correlates in several clinical popoulations including those with mental health conditions, migraine, Parkinson’s Disease, multiple sclerosis, and traumatic brain injury, few studies have examined the prevalence of WHO-DAS assessed disability in the general population. Data from a Spanish population cohort study among individuals aged 75 years and older report that 10% of individuals had severe or extreme disablity and that this prevalence was slightly higher among women (Virués-Ortega et al., 2011b). In the same population, Alzheimers Disease and depression were highly predictive of severe/extreme disability (Virués-Ortega et al., 2011a).
Adoption of the ICF framework by U.S. researchers has been met with tepid enthusiasm (Guralnik & Ferrucci, 2009; Jette, 2009) given the large body of work supported by the Nagi model (Nagi, 1976). However, recent work demonstrated that depression and obesity were associated with WHO-DAS assessed disbility among a sample of middle-aged women but that the association with disability differed by domain (Arterburn et al., 2012). While characterization of these domain-specific differences is the strength of the ICF framework, there are currently no other published studies reporting the prevalence of WHO-DAS assessed disability and its correlates among a community-dwelling U.S. population.
Obtaining disability prevalence estimates and gaining a better understanding of processes that begin or become prominent in the midlife is essential to plan effective clinical or public health interventions, particularly because the midlife represents a time in which individuals may be more amenable and able to respond to interventions. This article estimates the prevalence of WHO-DAS assessed disability among a cohort of midlife women and aims to identify factors associated with disability in that population.
Method
Study population
The SWAN study is a multiethnic cohort study of the menopause transition and its associated health consequences. First established in 1996, the Michigan site is one of seven clinical sites for SWAN and includes a population-based sample of eligible women from two Detroit-area communities identified using a community census based on the electrical utility listings of the targeted communities. Households were contacted by telephone (if available) or in-person; the response rate for inclusion in the cohort was 58.9% among eligible women (Sowers et al., 2000).
At the study’s inception in 1996, a total of 543 eligible women were recruited into the Michigan SWAN cohort, including 325 African American and 218 White women. Eligiblity criterion at baseline included 42 to 52 years of age, having an intact uterus, having had at least one menstrual period in the previous 3 months, no use of reproductive hormones in the previous 3 months, and self-identification as either African American or White race/ethnicity. Data for this analysis were collected at the 2011 study visit in which 77% of the still-living Michigan SWAN women participated. The analytic sample represents 376 women with a 2011 study visit; of those, 326 had an in-person visit that included physical measurements for assessment of body size. The University of Michigan Institutional Review Board approved the study protocol and written informed consent was obtained from each participant.
Measures
Disability assessment
Disability was assessed at the 2011 follow-up visit using the WHO-DAS instrument, which includes 36 questions across six domains including (a) understanding and communicating (6 items); (b) getting around (5 items); (c) self care (4 items); (d) getting along with people (5 items); (e) engaging in life activities (8 items); and (f) participation in society (8 items). Each item is scored using a 5-point Likert-type format that grades the difficulty on that task experienced by the respondent. Domain-specific scores and a summary index score were calculated for each participant and scaled to a 100-point scale whereby higher scores represent higher disability. Established cutpoints for ICF disability were used with scores as follows: no problem (0-4); mild problem (5-24); moderate problem (25-49); severe problem (50-95) and extreme problem (95-100; Maierhofer, Almazan-Isla, Alcalde-Cabero, & de Pedro-Cuesta, 2011; Virués-Ortega et al., 2011b). Potential demographic and health status correlates of disability were assessed concurrently with the WHO-DAS at the 2011 follow-up visit unless noted otherwise.
Explanatory variables
Potential correlates of disability including health status and conditions, demographic and environmental factors were considered to the extent that they were available.
Health status and conditions
Height (cm) and weight (kg) were measured using a stadiometer and calibrated balance-beam scale and used to calculate body mass index (BMI) in (kg/m2). Participants were categorized as obese (BMI ≥ 30 kg/m2) or nonobese (BMI < 30 kg/m2). Menopausal status was defined as surgical menopause (hysterectomy) versus natural postmenopause or unable to determine due to exogenous hormone use. Two participants were still having menses at the 2011 follow-up visit and were excluded from analyses in which menopause status was a covariate.
We measured the prevalence of 10 health conditions including diabetes, hypertension, knee osteoarthritis (OA), peripheral neuropathy (PN), depression, liver problems, peripheral vascular disease (PVD), cancer, heart attack, and stroke. For this investigation, health conditions were retained for statistical analysis if the prevalence was >10% and it was determined a priori that they could be associated with disability. Diabetes status was based on a self-report of a health care provider diagnosis of diabetes or current use of diabetes medications. Hypertension was defined as self-reported doctor’s diagnosis of hypertension, use of antihypertensive medications, or measured systolic blood pressure ≥140 mmHg or diastolic blood pressure ≥90 mmHg. Knee OA was defined as a Kellgren-Lawrence score ≥ 2 in either knee (Kellgren & Lawrence, 1963) based on radiographs obtained at the 2010 follow-up visit (if available) or 2009 follow-up visit. PN was defined as ≥ 4 on the self-reported Michigan Neuropathy Screening Instrument (MNSI) symptom questionnaire (Herman et al., 2012) or ≥ 20% failure rate on monofilament testing (Nang et al., 2009). Depressive symptomatology was defined as a score ≥16 on the Center for Epidemiologic Studies Depression Scale (Radloff, 1977). Liver problems, PVD, cancer, heart attack, and stroke were self-reported.
Demographic and environmental factors
Age was calculated as date of visit minus date of birth. Race/ethnicity was self-reported at baseline as African American or White. Level of economic strain was coded as none versus some or substantial economic strain based on participant response to the question “How difficult is it to pay for the very basics such as food, medical care, and housing?” Level of education at baseline (less than high school, high school, some college, college, or more than college) and marital status (never married, formerly married, or married) were also reported.
Statistical Analysis
Frequencies and percents of the categorical WHO-DAS domain and summary scores were calculated to estimate disability prevalence and corresponding 95% confidence intervals (CI). Means and standard deviations (SD) or frequencies and percents of demographic and health status variables were examined overall and by disability severity. The statistical significance of differences by disability category were evaluated using analysis of variance for continuous variables and chi-square tests for categorical variables. For analytical purposes, overall and domain-specific disability was dicotomized as none or mild disability (referent) versus moderate, severe, or extreme disability. A multinomial model with disability as none versus mild versus moderate-extreme was considered but, given the very low prevalence of “no disability” among women with peripheral neuropathy or depressive symptoms, it did not produce reliable estimates.
Prevalence odds ratios (OR) were calculated using multivariable logistic regression models. All demographic and environmental factors and all health status variables with > 10% prevalence were considered for inclusion in the multivariable models. Final model selection was based on model fit (evaluated using Akaike’s Information Criterion) and statistical significance of each variable. Potential interactions between the health conditions and demographic/environmental factors were tested and all were found to be nonsignificant.
Results
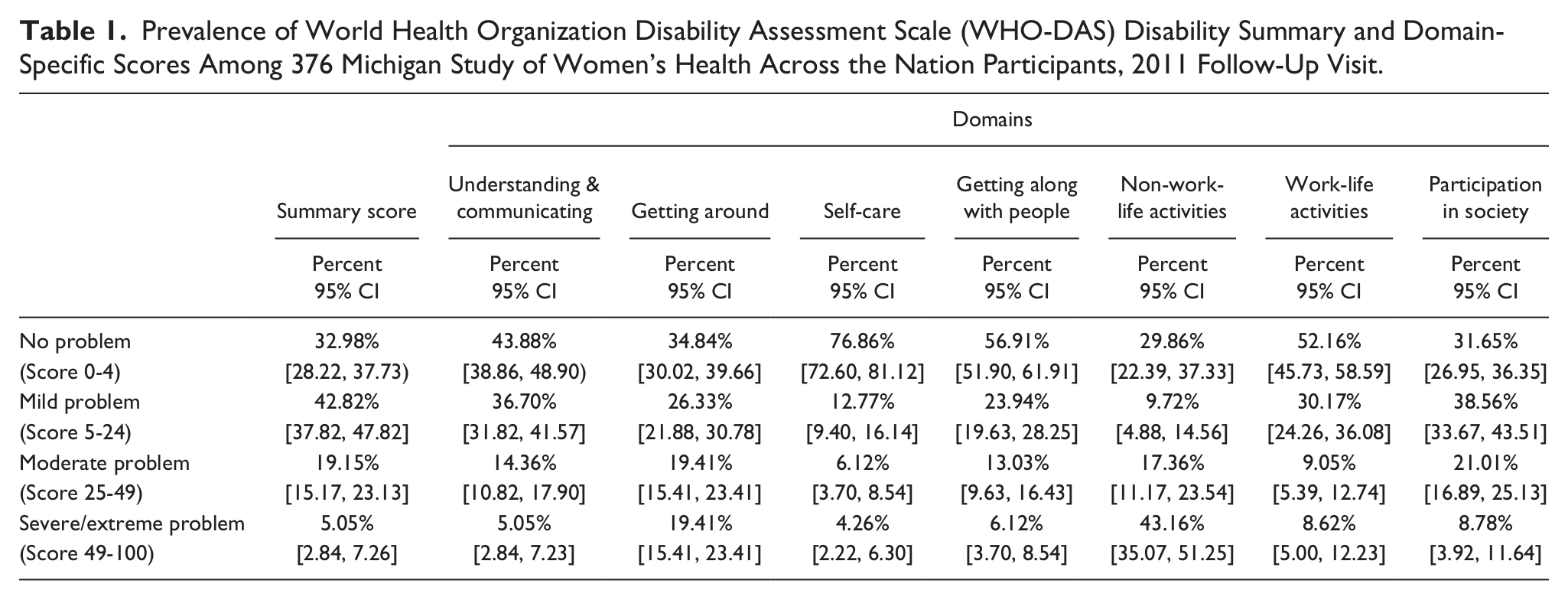
Nearly 25% of women in this late middle-aged population reported moderate, severe, or extreme disability (Table 1). With the exception of the self-care domain, the prevalence of moderate, severe, or extreme problems was at least one in five for all domains, including understanding and communicating (19%), getting around (39%), getting along with people (19%), work-related life activities (18%), and participation in society (30%).
Prevalence of World Health Organization Disability Assessment Scale (WHO-DAS) Disability Summary and Domain-Specific Scores Among 376 Michigan Study of Women’s Health Across the Nation Participants, 2011 Follow-Up Visit.
The average age of this sample was 60.6 years (SD = 2.8; range 55.9-67.7 years). By design, 60% were African American and 40% were White. Nearly half of women reported economic strain. The majority of women were obese (61%) and there was a high prevalence of health conditions including knee osteoarthritis (70%) and hypertension (61%). In the bivariate analyses (Table 2), economic strain, obesity, knee osteoarthritis, peripheral neuropathy, and depressive symptoms were associated with global disability (p < .001).
Demographic and health characteristics Among 376 Michigan Study of Women’s Health Across the Nation Participants, Overall and by WHO-DAS Disability Category.

Degrees of freedom (df). Test statistics are from ANOVA global F test for continuous variables (age) and from chi-square test for categorical variables (all others).
Table 3 reports the results from the multivariable logistic regression model with global disabiltiy as the dependent variable and including the health status/condition measures, race/ethnicity, and economic strain as independent variables. African American race/ethnicity and economic strain were statistically signficantly associated with greater global disability. In terms of health conditions, only peripheral neuropathy and depressive symptomatology were statistically signficantly associated with greater global disability. Peripheral neuropathy was associated with 4.6 times greater odds of moderate-severe global disability (OR = 4.55, 95% CI [2.21, 9.38]) and depressive symptomatology was associated with more than 6 times greater odds of disability (OR = 6.24, 95% CI [3.16, 12.34]), independent of the impact of demographic and other health status/conditions.
Multivariable Logistic Regression of Demographic and Health Status Correlates of Global Disability Among Michigan Study of Women’s Health Across the Nation Participants.
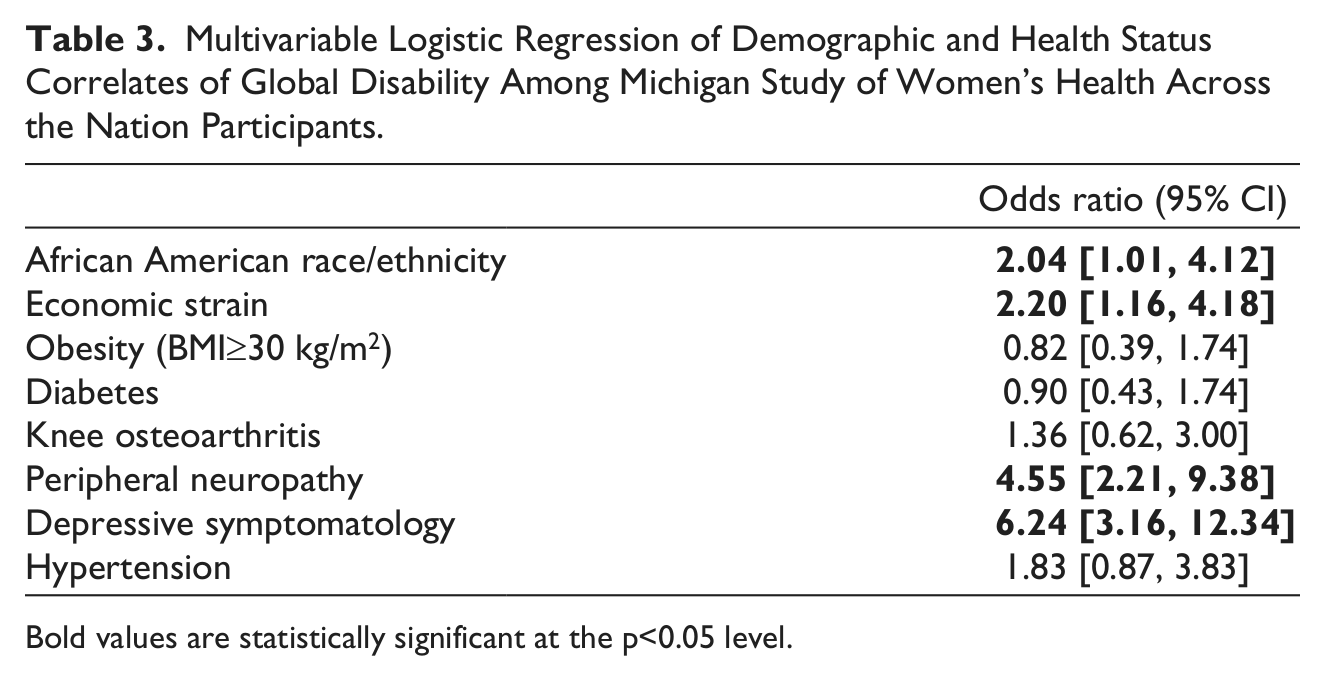
Bold values are statistically significant at the p<0.05 level.
Table 4 includes the results of 5 separate sets of multivariable logistic regression domain-specific models; each set of models included one health status/condition measure as the main independent variable of interest and was adjusted for race/ethnicity, economic strain, and obesity status. Peripheral neuropathy was associated with the getting around, getting along with people, life activities, and participation in society domains. Depressive symtpoms were significantly associated with all disability domains. The magnitude of these associations ranged from 3 times greater odds of moderate-severe disability among those with depressive symptoms for getting around (OR = 3.17, 95% CI [1.72, 2.85]) to more than 7 times greater odds for self care (OR = 7.05, [2.90, 17.11]). While obesity, knee osteoarthritis, and hypertension were not associated with global disability, each of these measures were associated with Domain 2 (getting around). Obese women had nearly 3 times greater odds of Domain 2 disability (OR = 2.89, 95% CI [1.72, 4.86]) as compared to nonobese women. In these domain-specific models, economic strain was associated with moderate-severe disability for all domains, whereas race/ethnicity was only associated with the understanding and communicating, life activities and participation in society domains.
Multivariable Analysis of Health Status Correlates of Domain-Specific Disability Among Michigan Study of Women’s Health Across the Nation Participants. a
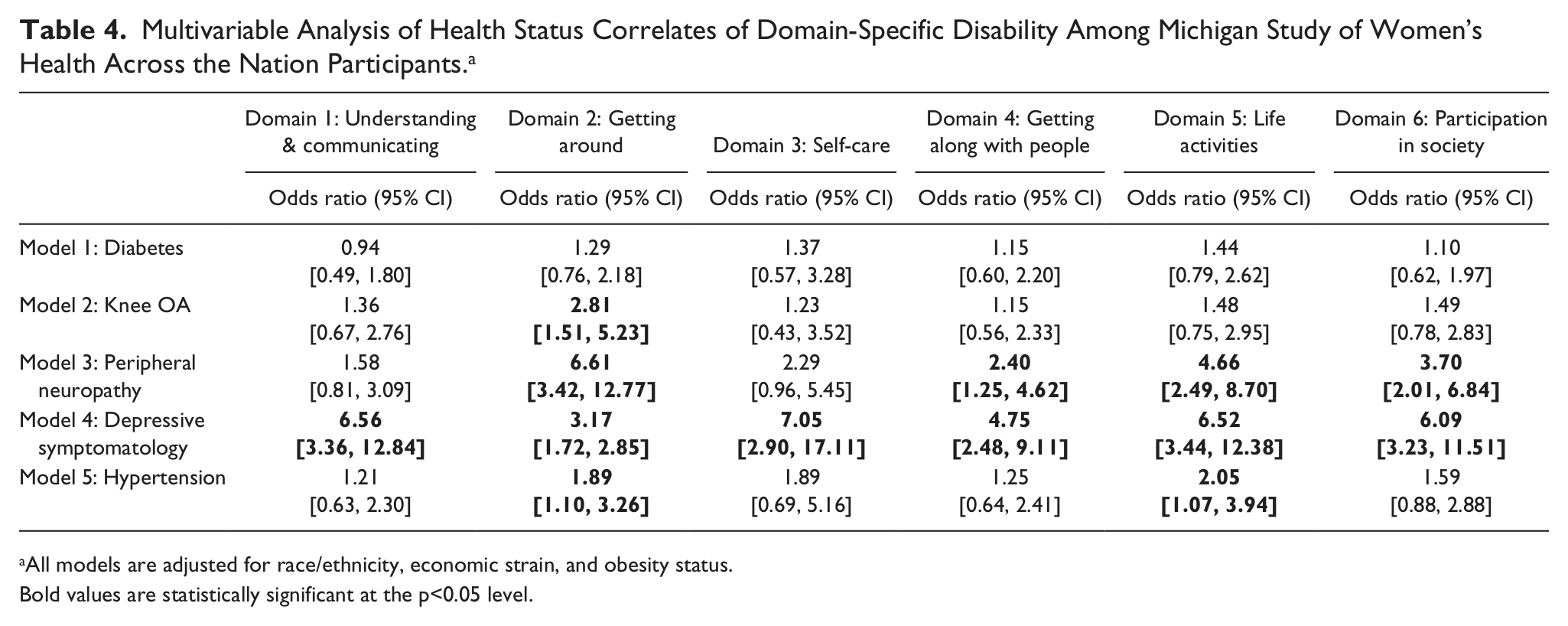
All models are adjusted for race/ethnicity, economic strain, and obesity status.
Bold values are statistically significant at the p<0.05 level.
Conclusions
Evidence suggests that the development of functional limitations begins during midlife (Adams & Marano, 1995; Tseng et al., 2012) and the prevalence of late midlife disability has been reported to range from 20% to 30% (Centers for Disease Control and Prevention [CDC], 2009; Murray et al., 2011; Sowers et al., 2006). These prevalences are similar to the estimate of global disability prevalence we report using the WHO-DAS questionnaire (25%). Traditional measures of disability including functional limitations and difficulties in activities of daily living may underestimate disability that is related to one’s personal, social, and environmental factors. Notably, our study found that the prevalence of disability for the mobility domain (“getting around”) was nearly 40% and the prevalence of disability for the non-work-life activity domain was in excess of 60%. These findings suggest that the burden of disability in the middle-aged population may far exceed traditional estimates and that middle-aged women may experience substantial difficulty with mobility.
A major strength of this study is our utilization of the WHO-DAS, which allowed for examination of not only global disability but also domain-specific measures. Compared to previously used models, the WHO-DAS provides a unifying framework and language to characterize disability in the United States and international settings, emphasizing participation and the interaction of an individual and his or her environment (Jette, 2009). Our data suggest that there is great value in assessing domain-specific disability because it provides a more in-depth examination of the nature of one’s disability, as evidenced by the drastic difference in disability prevalence across domains. Similar to what has been observed in elderly Spanish cohorts (de Pedro-Cuesta et al., 2011; Virués-Ortega et al., 2011b), getting around and non-work-life activities were the most common domains in which we observed disability among this middle-aged cohort. However, in contrast, the prevalence of disability in this population was lowest for the self-care domain, whereas in elderly populations the participation in society and getting along with people domains were the least affected (de Pedro-Cuesta et al., 2011).
Furthermore, our examination of multiple domains allowed us to understand which types of health conditions were associated with different aspects of disability. In a middle-aged population like ours, where disability may be predominantly associated with acute and specific physiology, a focus on prevention and an enabling environment may be more useful than for very old frail individuals (Guralnik & Ferrucci, 2009). As the ICF framework conceptualizes that one’s functional status is due to not only health conditions but also the interactions between one’s contextual factors, this multidomain aspect of the WHO-DAS allows us to consider different support needs for different domains—an important detail that may be missed by examining only global disability. In our study, only peripheral neuropathy and depression were associated with the global disability measure but knee osteoarthritis and hypertension were also associated with at least one of the domain-specific measures.
While obesity has been reported to be an important risk factor for disability (Peytremann-Bridevaux & Santos-Eggimann, 2008; Sirtori et al., 2012), our findings support this association only in the domain associated with mobility (Domain 2). While obesity may be more broadly associated with all aspects of disability due to the reported psychological symptoms of anxiety and depression among obese individuals (Van Hout, Van Oudheusden, & Van Heck, 2004), our data suggest that in this middle-aged population, obesity is associated with mobility limitations, which have been well documented among obese women (Vincent, Vincent, & Lamb, 2010). Our findings support work by Raggi et al. (2009, 2010) that mobility domains were the most relevant measures among the comprehensive ICF core set of indicators for obesity.
Economic strain was one of the strongest and most consistent correlates of both global and domain-specific disability in this study. Although the cross-sectional nature of our study precludes us from being able to determine if the economic strain contributed to disability onset or was a consequence of being disabled, work from other studies suggests that economic hardship is an important predictor of disability. Among middle-aged African American adults, childhood financial strain was associated with physical disability in adulthood (Szanton, Thorpse, & Whitfield, 2010). Furthermore, income inadequacy predicted age at disability onset among an elderly cohort of British individuals with the age of disability onset being 7 years earlier among those with income inadequacy as compared to those with adequate income report (Matthews, Smith, Hancock, Jagger, & Spiers, 2005). Thus women with economic disadvantage may be especially vulnerable to disability. The association of economic strain and disability persisted after adjustment for health status, thereby suggesting that the impact of economic hardship likely goes beyond the greater burden of comorbid conditions. Intervention strategies should target not only improvement of health status but also economic security issues in an effort to prevent or forestall the onset of disability in economically vulnerable populations.
Several studies have reported an association between depression and disability and previous work suggests that depression is more likely to be a consequence of being disabled (Barry, Soulos, Murphy, Kasl, & Gill, 2012; Chen et al., 2012; Ormel, Rijsdijk, Sullivan, van Sonderen, & Kempen, 2002) than vice versa. While our work confirmed the importance of the depression-disability association, our cross-sectional design precludes us from exploring the timing of this relationship.
Peripheral neuropathy is a well-documented as a risk factor for poor lower-extremity function, including slower gait, poorer balance, and falls (Richardson & Hurvitz, 1995; Resnick et al., 2002; Strotmeyer et al., 2008; Ylitalo, Herman, & Harlow, 2013), consistent with the strong association we observed between peripheral neuropathy and the mobility disability domain (Domain 2). However, neuropathy was also associated with getting along with people, life activities, and participation in society. These findings are consistent with the few studies that have evaluated the effect of neuropathy on reduced quality of life in diabetes patients (Currie et al., 2006; Venkataraman et al., in press). While peripheral neuropathy is predictive of depression and psychosocial distress (Vileikyte et al., 2005), we found a relationship between neuropathy and disability independent of depressive symptoms. We hypothesize that the association between neuropathy and psychosocial disability domains may be mediated by the mobility domain, since decreased physical functioning may cause decreased emotional and social function as well (van Schie, 2008). Peripheral neuropathy is underappreciated as a cause of disability, particularly for midlife women with and without diabetes, and deserves further research attention.
Limitations of our analysis included the cross-sectional nature of the design and consequent focus on prevalent disability. It has been well documented that disability is often a dynamic and heterogeneous process, including both acute and chronic episodes in individuals (Hardy, Dubin, Holfort, & Gill, 2005). Longitudinal studies are needed to be able to better describe the dynamic process of disability and to discern whether our observed associations of demographic and health status measures are predictive of disability onset or a consequence of being disabled. Our analysis was also limited to a relatively small sample of middle-aged women living in one geographic area of the United States; thus our results may not be generalizable to other populations.
In conclusion, we report a relatively high prevalence of global and domain-specific disability among late middle-aged women. Health conditions including knee osteoarthritis, peripheral neuropathy, and hypertension were most strongly associated with the mobility domain (getting around, Domain 2) whereas depressive symptoms and economic strain were more strongly associated with domains reflecting interactions of individuals with their environment (life activities, participation in society). Notably, obesity was not associated with the global disability and was only associated with the mobility domain. Future programs to prevent disability should include consideration of mental health and equity issues as important targets for intervention.
Footnotes
Acknowledgements
We thank the study staff at each site and all the women who participated in SWAN.
Authors’ Note
Clinical Centers: University of Michigan, Ann Arbor—Siobán Harlow, PI 2011-present, MaryFran Sowers, PI 1994-2011; Massachusetts General Hospital, Boston, MA—Joel Finkelstein, PI 1999-present; Robert Neer, PI 1994-1999; Rush University, Rush University Medical Center, Chicago, IL—Howard Kravitz, PI 2009-present; Lynda Powell, PI 1994-2009; University of California, Davis/Kaiser—Ellen Gold, PI; University of California, Los Angeles—Gail Greendale, PI; Albert Einstein College of Medicine, Bronx, NY—Carol Derby, PI 2011-present, Rachel Wildman, PI 2010-2011; Nanette Santoro, PI 2004-2010; University of Medicine and Dentistry—New Jersey Medical School, Newark—Gerson Weiss, PI 1994-2004; and the University of Pittsburgh, Pittsburgh, PA—Karen Matthews, PI.
NIH Program Office: National Institute on Aging, Bethesda, MD—Winifred Rossi 2012-present; Sherry Sherman 1994-2012; Marcia Ory 1994-2001; National Institute of Nursing Research, Bethesda, MD—Program Officers.
Central Laboratory: University of Michigan, Ann Arbor—Daniel McConnell (Central Ligand Assay Satellite Services).
Coordinating Center: University of Pittsburgh, Pittsburgh, PA—Maria Mori Brooks, PI 2012-present; Kim Sutton-Tyrell, PI 2001-2012; New England Research Institutes, Watertown, MA—Sonja McKinlay, PI 1995-2001.
Steering Committee: Susan Johnson, Current Chair; Chris Gallagher, Former Chair.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Study of Women’s Health Across the Nation (SWAN) has grant support from the National Institutes of Health (NIH), DHHS, through the National Institute on Aging (NIA), the National Institute of Nursing Research (NINR) and the NIH Office of Research on Women’s Health (ORWH) (Grants NR004061; AG012505, AG012535, AG012531, AG012539, AG012546, AG012553, AG012554, AG012495). The content of this article is solely the responsibility of the authors and does not necessarily represent the official views of the NIA, NINR, ORWH or the NIH.