
Abstract
Fear of falling can serve a protective function in that it may prevent potentially injurious falls. This adaptation may be particularly important in older adults, who face higher risk of falling and of experiencing fall-based injuries (Rubenstein, 2006). However, like other fears, fear of falling can become maladaptive if it promotes significant reductions in functional activity. Fear of falling is a salient predictor of reduced activity (e.g., physical exercise) in older adults (Bertera & Bertera, 2008), which can lead to physical deconditioning, reduced knee muscle strength, weaker hand grip strength, and deficiencies in balance (Delbaere, Crombez, Vanderstraeten, Willems, & Cambier, 2004). These physical changes can make activities of daily living more difficult, increasing the risk of falls and potentially even exacerbating fear of falling (Delbaere et al., 2004; Powell & Myers, 1995). Females may be particularly more susceptible to reductions in functional activity and related physical deconditioning because of predisposing factors, such as an increased likelihood of falling, being older (i.e., living longer), having a sedentary lifestyle, and being afraid to fall (Friedman, Munoz, West, Rubin, & Fried, 2002; Scheffer, Schuurmans, van Dijk, van der Hooft, & de Rooij, 2008; Statistics Canada, 2008; Trost, Owen, Bauman, Sallis, & Brown, 2002; Zijlstra et al., 2007).
Falls can be associated with several potentially aversive experiences, such as pain, embarrassment, fear, and sudden increases in physiological arousal (e.g., racing heart). As such, it is not surprising that individuals who have fallen are more likely to experience fear of falling, potentially because falls are inherently uncomfortable and can trigger realization that they are dangerous (Friedman et al., 2002). Restriction in activities that could potentially lead to falls could thus be interpreted as an adaptive response to a risk. Given these associations, it is reasonable to expect that avoidance would be strongest in individuals who have experienced a fall-based injury. A small body of research supports this possibility (Murphy, Williams, & Gill, 2002) and also demonstrates that older adults who have experienced a severe fall-based injury (i.e., fractures, joint dislocation, or laceration requiring sutures) are more likely to avoid activities compared with those experiencing minor injuries (i.e., lacerations not requiring sutures, bruises, abrasions, sprains, and minor soft tissue injury; Nevitt, Cummings, & Hudes, 1991). Similarly, a small number of falls resulting in serious injury may contribute more to restriction in activities than experiencing many non-injurious falls (Tinetti & Williams, 1998).
Despite the aforementioned findings, research in this area is relatively limited. For example, past studies are limited in their generalizability as a consequence of relatively small samples where females may be overrepresented, of collapsing injuries into broad categories (e.g., major injuries comprising fractures and dislocations), of not considering other potential relationships (e.g., minor injury vs. no injury, no injury vs. no fall), and of assessing avoidance in activities but not fear of falling. Moreover, previous research in this area has failed to take into account how these relationships may differ between sexes, which is a salient possibility given the notably higher prevalence of fear of falling and falls in females (Friedman et al., 2002; Scheffer et al., 2008).
The aim of the current study was to explore how specific types of fall-based injuries relate to fear of falling and restriction in activities separately in males and females. We made use of a large population-based sample of older Canadians to increase the generalizability of the findings and to ensure a proportionate amount of males and females and of adults of varying ages. We expected that individuals who have experienced a severe fall-based injury (e.g., bone fracture) would have greater odds of reporting fear of falling and restriction in activities compared with those who have experienced minor injuries (e.g., bruises). We hypothesized that this relationship would be present in both sexes, but that females who have experienced a severe fall-based injury would have the greatest odds of reporting fear of falling and restriction in activities.
Methods
Participants
Data were obtained from the Canadian Community Health Survey—Healthy Aging, a nationally representative sample of Canadian adults aged 45 and above living in private dwellings in the 10 provinces. The survey population did not include Canadians living in the three territories, Indian reserves, or Crown lands, or persons who were institutionalized, full-time members of the Canadian Forces, or living in some remote regions of the country (Statistics Canada, 2010). Sampling frames were based on the 2006 Census. Data from the survey were collected between December 2008 and November 2009. The majority of participants (94%) were interviewed in person. Telephone interviews were arranged when no interviewer speaking the participant’s language was available. Proxy interviews were arranged when participants were mentally or physically unable to complete the interview independently. In such a case, a knowledgeable household member would answer all questions on behalf of the participant. Questions to which the proxy did not know the answer were left unanswered. Efforts were made to limit the number of proxy interviews. 1 Data included 30,865 observed cases from age groups of 45 to 49 years (n = 2,459, 53.72% females), 50 to 54 years (n = 2,707, 56.41% females), 55 to 59 years (n = 4,788, 54.47% females), 60 to 64 years (n = 4,542, 52.44% females), 65 to 69 years (n = 3,958, 52.53% females), 70 to 74 years (n = 3,017, 54.42% females), 75 to 79 years (n = 2,967, 59.32% females), 80 to 84 years (n = 2,353, 66.17% females), and 85 years or older (n = 4,074, 66.08% females). The present study utilized data from adults 65 years and older (N = 16,369). Younger age groups were not asked questions about fear of falling, fall-based injuries, and restriction in activities related to fear of falling.
Measures
All included participants reported whether they had fallen (i.e., “In the past 12 months, did you have any falls?”) and whether they were worried or concerned they might fall (i.e., “Are you worried or concerned that in the future you might fall?”). A positive response to the latter was operationalized as fear of falling. Participants who had fallen reported their most severe injury resulting from a fall (i.e., “What has been your most serious injury or problem due to a fall within the past 12 months?”). The following possible types of injuries were read to participants and they were asked to select the most appropriate answer: no serious injury, sprain or strain, bruise, cut, discomfort, fracture of hip, fracture of leg, fracture of arm or wrist, fracture of back or vertebra, head injury, or other. The different types of bone fracture were combined into bone fracture in the final data set. Those who reported fear of falling indicated whether they restricted their activities as a result of their fear (i.e., “As a result of this concern [of falling], have you stopped doing some things you used to do or liked to do?”).
Analyses
Odds ratios (ORs) were calculated to test differences in fear of falling in males versus females (one OR), restriction in activities in males versus females (one OR), fear of falling in non-injurious falls versus no falls (calculated separately by sex; two ORs), restriction in activities in non-injurious falls versus no falls (calculated separately by sex; two ORs), fear of falling in different types of injuries versus no injury (calculated separately by sex; 14 ORs), and restriction in activities in different types of injuries versus no injury (calculated separately by sex; 14 ORs). ORs were considered statistically significant when their 95% confidence interval (CI) did not include the value of 1. All frequencies and ORs were weighted using Taylor Series Linearization to maximize national representativeness of the results.
Results
Odds of falling, fear of falling, restriction in activities, and specific types of injuries in each sex are reported in Table 1. Approximately 22% of females (2,279 observed cases) and 17% of males (1,311 observed cases) reported falling in the past 12 months. Bruises were the most commonly reported type of fall-based injury, followed by sprains or strains. Females had greater odds of falling in the past 12 months and of reporting fear of falling compared with males. Females did not have greater odds of restricting their activities due to fear of falling compared with males. Females who reported experiencing a non-injurious fall in the past 12 months were more likely to report fear of falling (OR = 2.49, 95% CI = [2.09, 2.96]) but not to restrict their activities due to fear of falling (OR = 0.98, 95% CI = [0.76, 1.26]) compared with females who did not fall. Similarly, males who reported experiencing a non-injurious fall in the past 12 months were more likely to report fear of falling (OR = 1.42, 95% CI = [1.16, 1.74]) but not to restrict their activities due to fear of falling (OR = 0.93, 95% CI = [0.66, 1.30]) compared with males who did not fall. ORs for fear of falling and restriction in activities according to specific types of injuries are reported in Table 2. Females who reported experiencing a bone fracture or head injury had increased odds of experiencing fear of falling compared with females who had fallen without injury. No other types of injury were associated with fear of falling in females. Females who reported experiencing a head injury had increased odds of restricting activities compared with females who reported falling without injury. No type of injury was associated with either fear of falling or reduction in activities in males.
Descriptive Statistics for Weighed Estimates.
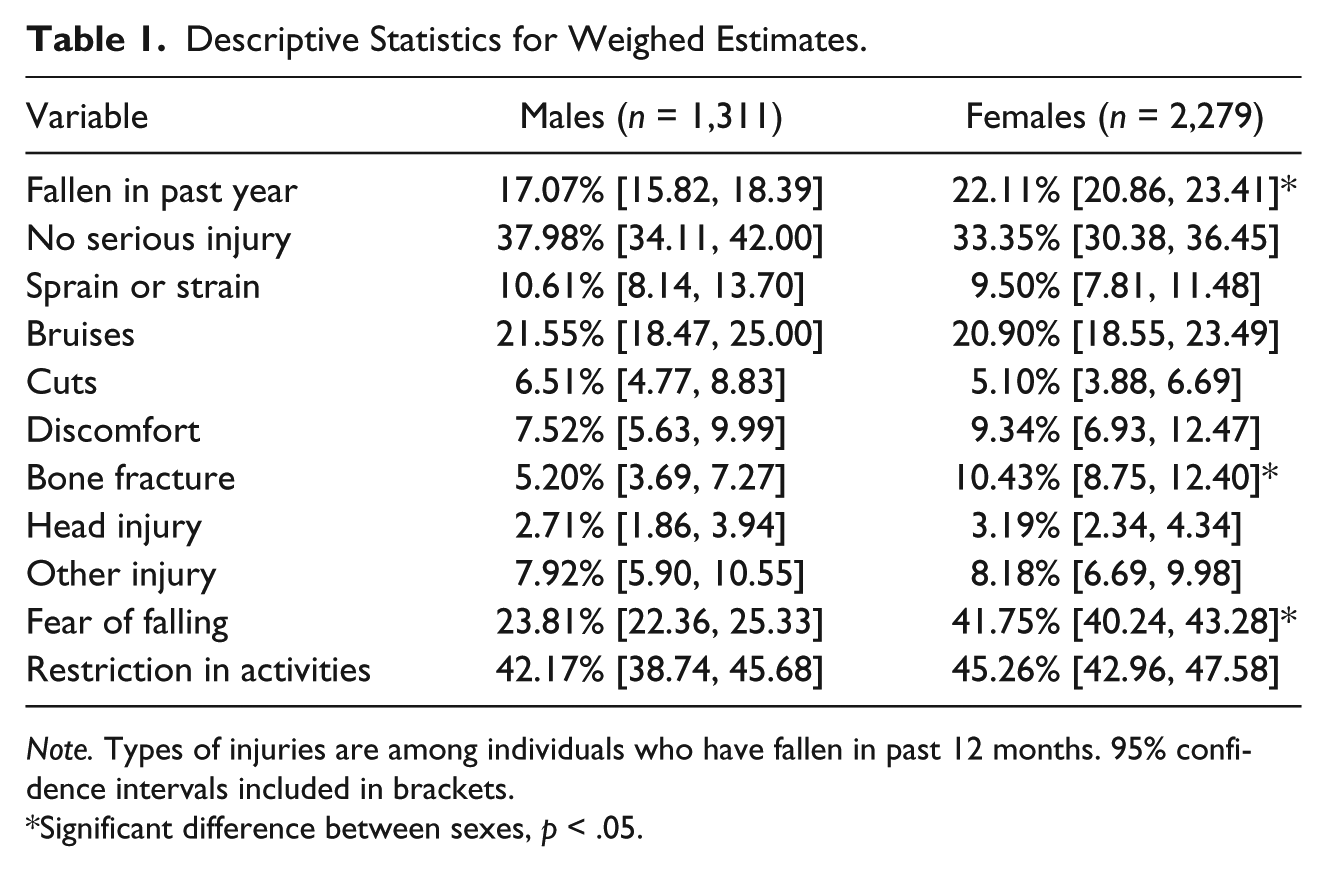
Note. Types of injuries are among individuals who have fallen in past 12 months. 95% confidence intervals included in brackets.
Significant difference between sexes, p < .05.
Odds Ratios of Experiencing Fear of Falling or Restriction in Activities in Males and Females Who Have Experienced Different Fall-Based Injuries Compared With No Injury.
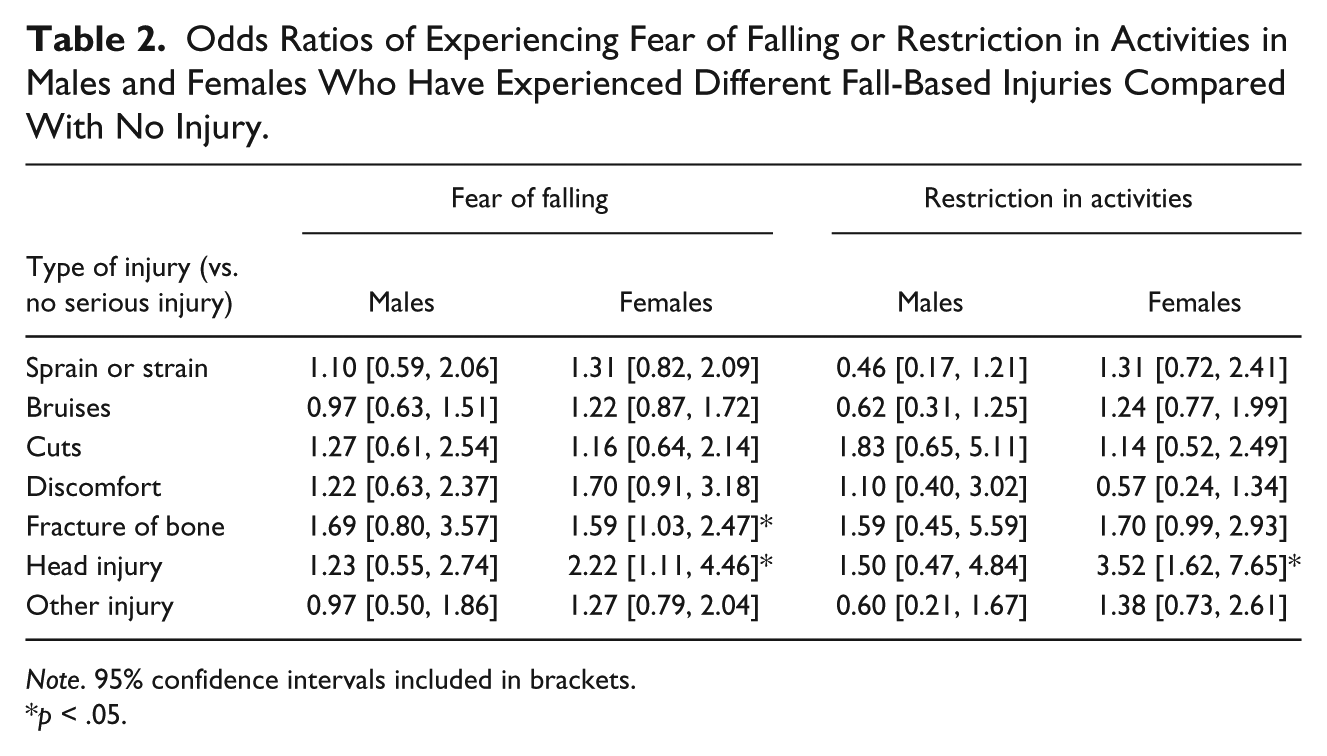
Note. 95% confidence intervals included in brackets.
p < .05.
Discussion
The goal of the current study was to investigate the role of different fall-based injuries in fear of falling and associated restriction in activities in a nationally representative sample of older males and females. Consistent with previous literature, older females were more likely to experience falls compared with males (Friedman et al., 2002; Murphy, Dubin, & Gill, 2003), possibly because females are more likely to be older, be visually impaired, and live a sedentary lifestyle (Resnikoff et al., 2004; Statistics Canada, 2008; Trost et al., 2002). Older females were also more likely to experience fear of falling compared with males.
Individuals who experienced physically innocuous (i.e., non-injurious) falls had increased risk of fear of falling regardless of sex when compared with individuals who did not fall, adding support to the posited relationship between fall experiences and fear of falling in older adults (Friedman et al., 2002). Non-injurious falls can be associated with significant detriments and lead to the realization that future falls could cause pain, injuries, or embarrassment. Older adults may also worry that future falls could lead to a loss of independence or to discharge to a long-term care facility if hospitalization is required. In this context, fear of falling and restriction in activities could be a reaction to manage perceived risks to health and lifestyle (Friedman et al., 2002).
The present findings challenge the intuitive expectation that the severity of injurious falls would be generally associated with fear of falling and restriction in activities. Indeed, in the current sample, the vast majority of fall-based injuries were not associated with fear of falling and restriction in activities when compared with non-injurious falls. Such findings contradict past research indicating that the risk of restriction in activities increases drastically with fall-based injury severity (Nevitt et al., 1991). In the current sample, individuals who had experienced a non-injurious fall had greater odds of experiencing fear of falling and associated restriction in activities compared with those who had not fallen; however, fall-based injuries were not linked to fear of falling or restriction in activities in males, and only extreme fall-based injuries were linked to fear of falling or restriction in activities in females (i.e., bone fractures and head injuries). In other words, females who have suffered a severe fall-based injury appear to be at greatest risk of experiencing fear of falling and of restricting their activities.
Females who have experienced a severe fall-based injury may be at greatest risk of experiencing fear of falling, restriction in activities, and related detriments (e.g., physical deconditioning, deficiencies in balance). Cognitive behavioral interventions have been demonstrated to reduce both fear of falling and restriction in activities in older adults (Zijlstra et al., 2009), and females who have experienced a severe fall-based injury may benefit most from this type of intervention. They may also benefit most from multifactorial risk assessment and management programs, which have been shown to be effective at reducing the likelihood and frequency of falls (Chang et al., 2004). Differences in the relationships between type of fall-based injury, fear of falling, and associated restriction in activities in males and females warrant further research to determine factors making females more vulnerable to falls and their associated behavioral and psychological consequences.
There were a number of limitations within the study. The use of proxy interviews in the sample, although infrequent, is a notable issue given that fear of falling and related restriction in activities may be highly subjective in nature. The cross-sectional nature of the study limits causal inferences regarding the relationships of interest. Future research should seek to replicate the results using a longitudinal approach and more elaborate measures of restrictions in activities (e.g., restrictions in physical exercise vs. activities of daily living). The dichotomous nature of our measures of fear of falling and restriction in activities limits response variability. Further research should seek to replicate the results using more elaborate measures of fear of falling such as the Falls Efficacy Scale (Tinetti, Richman, & Powell, 1990) and the Activities-Specific Balance Confidence Scale (Powell & Myers, 1995). Seriousness of injury was not quantitatively defined and some injury categories may overlap in seriousness (e.g., a major bruise could have been categorized as less serious than a minor cut). It is, however, unlikely that injuries that were considered minor in the current study (such as cuts or bruises) could be more serious than bone fractures or head injuries. The manner in which the number of falls was assessed did not allow for investigation of the long-term effect of falls on fear of falling and restriction in activities. Because only falls in the past 12 months were surveyed, it was impossible to discriminate between participants who have had many falls spanning several years, only falls in the past year, or no falls at all. Retrospective accounts of falls that occurred more than 12 months in the past could be considered unreliable and, as such, a comprehensive survey of falls over a longer time period would be more appropriate in a longitudinal research design.
The present findings extend current knowledge in regard to falls, fear of falling, and restriction in activities in older adults. Our study is the first to demonstrate sex-specific differences in the relationships between types of fall-based injuries, fear of falling, and restriction in activities within a nationally representative sample of older adults. Sex differences warrant further investigation and suggest the need for targeted interventions for females with severe fall-based injuries.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Michel A. Thibodeau was supported by a Canadian Institutes of Health Research doctoral award (FRN: 113434). Dr. Gordon J. G. Asmundson was supported by a President’s Chair for Academic Excellence in Adult Mental Health Research.