
Abstract
Background
The population of older people is increasing globally (United Nations Population Division [UNPD], 2011). It is projected that the population of older people will be greater than the population of children under 14 years of age by 2050, and that most of these older people will be living in low income countries (United Nations Development Programme [UNDP], 2008; UNPD, 2011). By 2012, there were 59.7 million people aged 60 and above in Africa, constituting 6% of the population in Africa. The population is projected to increase to 215 million older people (10%) of the population in Africa by 2050 (United Nations Population Fund [UNFPA], 2012; UNPD, 2011). In Uganda, the population of older people is projected to increase from 1.4 million (3.9%) of the total population in 2012 to 5.4 million (5.8%) by 2050 (UNDP, 2008; UNPD, 2011).
While population aging is an indicator of development, reflecting conditions such as sanitation, nutrition, better medical services, and improving economies, it may also have negative socioeconomic consequences to which society will need to adapt (UNFPA, 2012). A growing ageing population is likely to impact the health systems of countries in Sub-Saharan Africa that are not prepared for the increased demand for services due to chronic diseases associated with ageing and other non-communicable diseases. These diseases are now increasingly becoming common as a result of the epidemiological transition from infectious diseases to non-communicable diseases (UNFPA, 2012). In addition, low-income countries of sub-Saharan Africa are facing the problem of HIV/AIDS among older people (Negin & Cumming, 2010) with older people being directly or indirectly affected (Nyirenda et al., 2013; Scholten et al., 2011).
Because of these demographic and epidemiological transitions, there is need for research on common medical problems that affect older people in Africa, to inform policy and practice on the development of interventions that can improve older people’s health and well-being. Although research has been done in Uganda and the rest of sub-Saharan Africa on the epidemiology and the impact of some diseases on aging (Mugisha et al., 2013; Naidoo et al., 2010; Nyirenda et al., 2013; Scholten et al., 2011; Seeley, Wolff, Kabunga, Tumwekwase, & Grosskurth, 2009), to the best of our knowledge, little has been done on anemia among older people; even though it has been shown to be a common medical condition among older people in studies conducted in high income countries (Gaskell, Derry, Moore, & McQuay, 2008).
Anemia is the most common disorder of the blood, and is characterized by a decrease in number of red blood cells or less than the normal quantity of hemoglobin in the blood. It is defined by the World Health Organization (WHO) as a hemoglobin (Hb) concentration of less than 130 g/L in adult men and less than 120 g/L in adult non-pregnant women (WHO, 1968). Estimates on global prevalence of anemia from WHO (from 1993 to 2005) show that 23.9% (164 million) older people are affected by anemia globally (De Benoist, McLean, Egli, & Cogswell, 2008). These estimates do not include older people in Africa because of the lack of prevalence surveys on anemia among the older people in this region.
Studies conducted on anemia in older people in high-income countries have shown that the burden of anemia is higher in older Blacks than Whites (Dong et al., 2008; Guralnik, Eisenstaedt, Ferrucci, Klein, & Woodman, 2004; Patel et al., 2007; Vanasse & Berliner, 2010; Zakai et al., 2005). Moreover, that anemia in older people is associated with several serious consequences including increased risk of mortality (Kikuchi, Inagaki, & Shinagawa, 2001; Woodman, Ferrucci, & Guralnik, 2005), worse cognitive function (den Elzen et al., 2009; Lucca et al., 2008), disability and poor physical function (Penninx et al., 2003) as well as generally poor quality of life (Thein et al., 2009; Thomas, 2004). These negative consequences have been shown to occur even when older people are affected by mild anemia (den Elzen et al., 2009; Kikuchi et al., 2001; Lucca et al., 2008; Penninx et al., 2003; Penninx et al., 2004; Woodman et al., 2005).
Studies on anemia in older people from high income countries have also shown that the commonest types of anemia among older people are due to nutritional deficiencies (i.e., iron deficiency, vitamin B12 deficiency, and folate deficiency), chronic inflammation, chronic kidney disease, and unexplained anemia (Guralnik et al., 2004; Vanasse & Berliner, 2010). Of these types, iron deficiency anemia has been shown to account for one third of all nutritional anemia among older people (Guralnik et al., 2004). In sub-Saharan Africa, iron deficiency anemia in adults is commonly caused by nutritional deficiencies, infections with soil transmitted helminths, malaria, and genetic disorders of hemoglobin (Balarajan, Ramakrishnan, Ozaltin, Shankar, & Subramanian, 2011). Although data on types of anemia among older people are scarce in Uganda, iron deficiency anemia may be important among older people, because of poor nutrition, due to widespread poverty and limited access to food (Ministry of Gender, Labor and Social Development [MOGLSD], 2009; Najjumba-Mulindwa, 2003).
Anemia control programs in low-income countries have not targeted older people because they are either not thought to be at an increased risk of developing anemia or due to lack of data on anemia among the older people. Data on older people’s perceptions of anemia are scarce in both high- and low-income countries. Most of the data available on anemia in older people in high-income countries is quantitative data. There is need for qualitative data to complement statistical data. The few data that are available in Africa are from women of reproductive age groups (Galloway et al., 2002; Young & Ali, 2005). Understanding older people’s perceptions of anemia is important in developing targeted and effective public health interventions to control anemia among the older people.
As part of a mixed methods research project to study the epidemiology, impact, and perceptions of anemia among older people in a rural Ugandan population, we collected both quantitative and qualitative data to establish whether older people understand what anemia is, how to identify older people with anemia, and the common causes of anemia among older people. We explored older peoples’ perceptions on whether they thought they had anemia, the understanding of the consequences of anemia and how the condition is treated.
Study Setting
This study was conducted between January 2012 and January 2013 in a general population cohort (GPC; Asiki et al., 2013). The GPC is a population-based cohort study of around 20,000 people living within the Kyamulibwa subcounty of Kalungu district in rural South-West Uganda. The cohort was established in 1989 by MRC/UVRI Uganda Research Unit on AIDS to describe trends in the prevalence and incidence of HIV infection and their determinants in the general population. The initial recruitment was conducted in 1989/1990.
Every year since 1989, annual house-to-house “rounds” of census and survey have been carried out until 2012 when the house to house survey method was changed, and participants were invited and surveyed at central hubs (a building rented for the purpose in the village) in each of the study villages.
Demographic, socio-medical, and serological data are collected. Information regularly obtained includes data on fertility, mortality, migration, sexual behavior, perceptions of HIV infection, and HIV status.
The GPC runs a clinic and a clinical laboratory at the Kyamulibwa field office where GPC participants can access free treatment.
In addition to conducting annual HIV sero surveys, the GPC also provides a population for recruitment for other studies including social science research aimed at an in-depth understanding of social aspects of health, including research on the health and well-being of older people.
The Anemia Survey Among Older People
The anemia survey was nested in the GPC round 23 and was conducted between January 2012 and January 2013. Eligible participants were all older people aged 50 years and above resident in the GPC study area during the survey period, who consented to participate.
Quantitative Data Collection
A questionnaire on anemia was developed based on existing questions in the GPC survey questionnaire, the WHO study on global ageing and adult health (Naidoo et al., 2010) questionnaire, and the cross-cultural assessment of nutrition in older subjects questionnaire (Gross, 1997). Questions on anemia perceptions and other risk factors for anemia were also included. Specifically for this article, the anemia perception questions included whether older people perceived themselves to be anemic at the time of the interview and for those who did, the reasons why they thought they were anemic. The anemia study questionnaire was translated into the local language and back translated into English and necessary adjustments made. The questionnaire was then pilot tested with 63 older people. The final questionnaire was then programmed on ultra mobile personal computers (UMPCs), which were used for data collection. All older people in the GPC were first enumerated and mobilized through community meetings, and home visits. Those that consented to participate in the anemia survey were either interviewed from the village central hubs or were interviewed from the GPC study clinic. All interviews were conducted by trained interviewers from the GPC. After the interviews, blood samples and two consecutive stool samples were obtained to study the epidemiology and types of anemia among the older people. Hemoglobin was measured at the Kyamulibwa clinic laboratory as part of the full blood count on the same day the blood was collected. Anemia was defined using the WHO criteria. All older people who were found with anemia or any other illnesses during the survey were referred for free treatment at the GPC clinic.
Sample Recruitment Strategy for the Qualitative Study
Ten older people were purposively selected to participate in in-depth interviews. The GPC covers 25 villages. In the selection of these participants, we first excluded 5 study villages (2 villages that are within or near Kyamulibwa trading centre and 3 other villages that had less than 50 older people). We then randomly selected 10 villages from the remaining 20 GPC villages. Using the census lists of the GPC, we randomly selected one older participant from each of these 10 villages to participate in the in-depth interviews. However, we ensured that these 10 older people selected included both males and females and older people with ages above and below 65 years. If this was not achieved in the first selection, we replaced the randomly selected participant and randomly choose a new one. The selected participants were then invited to participate in the interviews. The sample comprised of 6 females and 4 males. Six of these were aged 65 years and above, with 2 participants above 80 years.
Qualitative Data Collection
Selected participants were visited in their homes 2 to 3 days prior to the date scheduled for the interview. The participants were informed about the interview and what was requested of them. For those who felt uncomfortable giving the interview in their home, an appointment was made and an MRC vehicle was sent to bring the participants to the MRC offices where the interview was carried out. All the in-depth interviews were conducted by the first author. The interviews covered the following topics: demographic characteristics of the study participants, the diseases of the blood in this community, the disease of the blood known as anemia (whether participants had ever heard about it and from whom, and what was said about the disease), local terms used to describe anemia, whether participants perceived themselves to have anemia, and reasons for their perceptions. In addition, participants were asked what the common causes of anemia among older people in their villages may be, how they can know that an older person has anemia, what older people in the villages do when they think they have anemia and what was likely to happen if an older person developed anemia. The interviews also asked which diseases affect older people in this study community. For the three people interviewed at home, the interviewer was also able to observe living conditions and the general setting in which the person lived. All the interviews were recorded using audio recorders and notes were taken. Notes taken during the interview were expanded by the first author within 12 hr after the interview. For the first three interviews, the first author read all scripts immediately after writing up, and noted emerging themes as well as checking that topics to be covered, as defined by the research questions were adequately covered. Where some data were missing, follow-up interviews were arranged. The transcription and translation of the interviews from the local language was done by the first author, assisted by a social science research assistant.
All those interviewed at the GPC clinic had medical complaints and since there was free transport for them to the clinic, they sought treatment after the interviews.
Ethical Issues
Ethical clearance was obtained from London School of Hygiene and Tropical Medicine ethics committee, the Uganda Virus Research Institute Science and Ethics Committee and the Uganda National Council for Science and Technology. We obtained a written/thumb printed consent from all the older people who participated in this study. We also obtained consent to tape record the interviews and to use their quotations in papers and reports.
Data Analysis
Qualitative data were analyzed using thematic content analysis. Data collected from in-depth interviews were transcribed and a preliminary review for initial themes and patterns occurring within the data was done by the first author and discussed with co-authors. The data were anonymized, coded, and organized in a code matrix, stratified according to age, sex, and the emerging themes and subthemes (Ritchie & Lewis, 2003). Patterns and relationships emerging across the data were established and summarized.
Quantitative data were uploaded from the UMPCs and synchronized on the main GPC database daily. After data collection, the anemia survey data were extracted from the main GPC database, cleaned and analyzed using STATA software version 11 and proportions calculated. We compared differences between men and women using the Student’s t test. Because the qualitative sample was drawn from the quantitative sample and findings could be linked by unique numerical identifier, qualitative data were cross referenced with quantitative data and synthesis of findings done.
Results
In total, 1,455 (77%) people 50 years and above in GPC participated in the anemia survey. Six older people were excluded from the analysis because of uncertainty over their age. Finally, 1,449 participants contributed to this analysis. The description of study participants who participated in the anemia survey is shown in Table 1. One hundred and forty-six males (24.1%) and 148 females (17.5%) had anemia. The prevalence of anemia was significantly higher in men than women (p = .002). After stratifying for those aged below and above 65 years, 88 males (33.8%) and 60 females (17.4%) above 65 years had anemia. Four participants that gave qualitative data had anemia, one with chronic severe anemia, which was confirmed from his medical records at the GPC study clinic.
Description of Study Participants in the Anemia Survey.
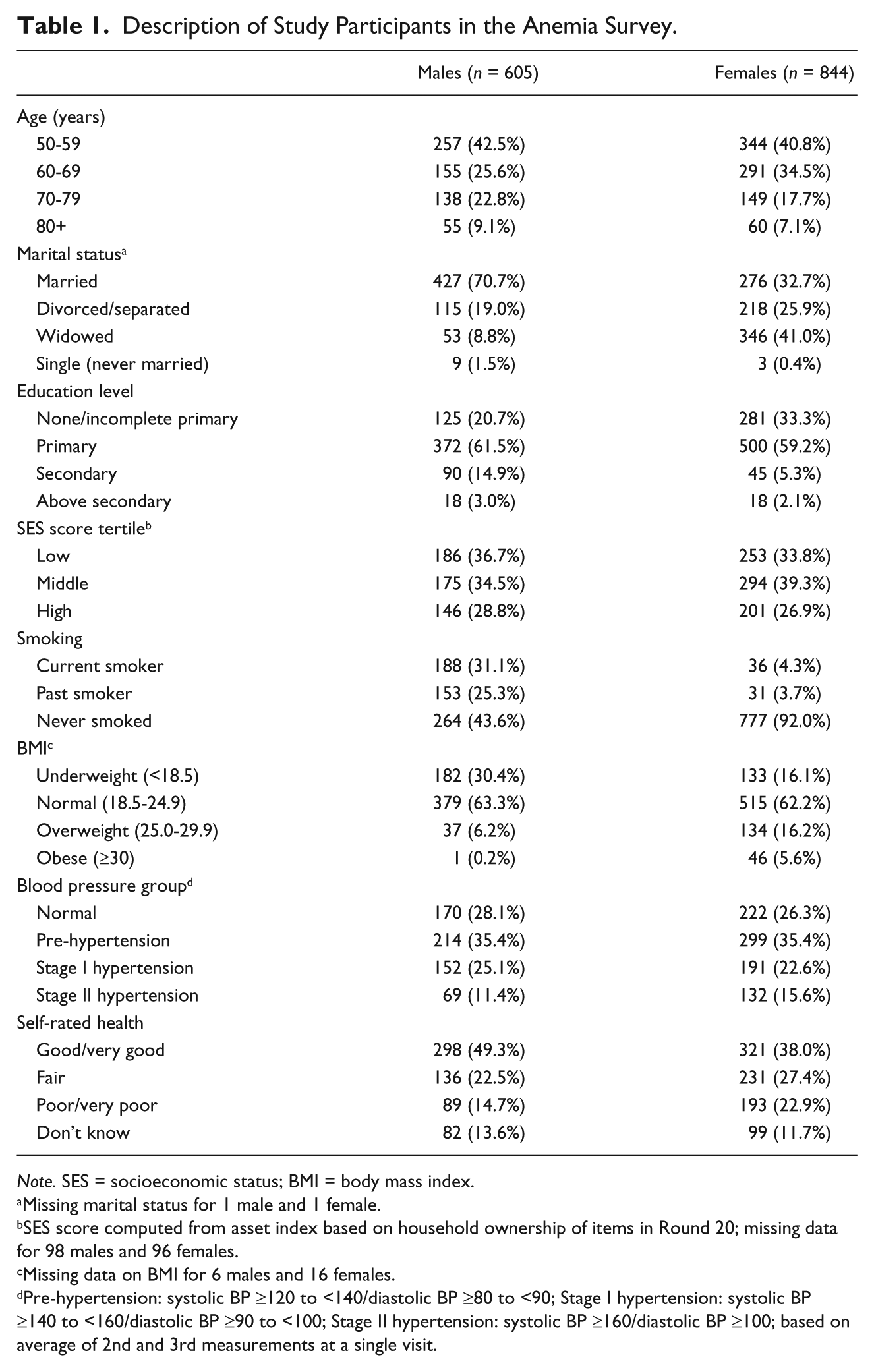
Note. SES = socioeconomic status; BMI = body mass index.
Missing marital status for 1 male and 1 female.
SES score computed from asset index based on household ownership of items in Round 20; missing data for 98 males and 96 females.
Missing data on BMI for 6 males and 16 females.
Pre-hypertension: systolic BP ≥120 to <140/diastolic BP ≥80 to <90; Stage I hypertension: systolic BP ≥140 to <160/diastolic BP ≥90 to <100; Stage II hypertension: systolic BP ≥160/diastolic BP ≥100; based on average of 2nd and 3rd measurements at a single visit.
Perceptions on Being Anemic
From quantitative data, 82 (13.6%) males and 90 (11.1%) females thought they had anemia (Table 2). Among those that gave qualitative data, 8/10 older people thought they had anemia while 2 participants did not know whether they had anemia or not. One of these, a male aged 88 years said “ . . . I don’t know whether I have anemia or not. It is the doctors like you who should tell me if I have little blood [anemia] because you studied a lot, but for me a Muganda [local person], I cannot tell . . . .”
Self-Perceptions of Anemia.
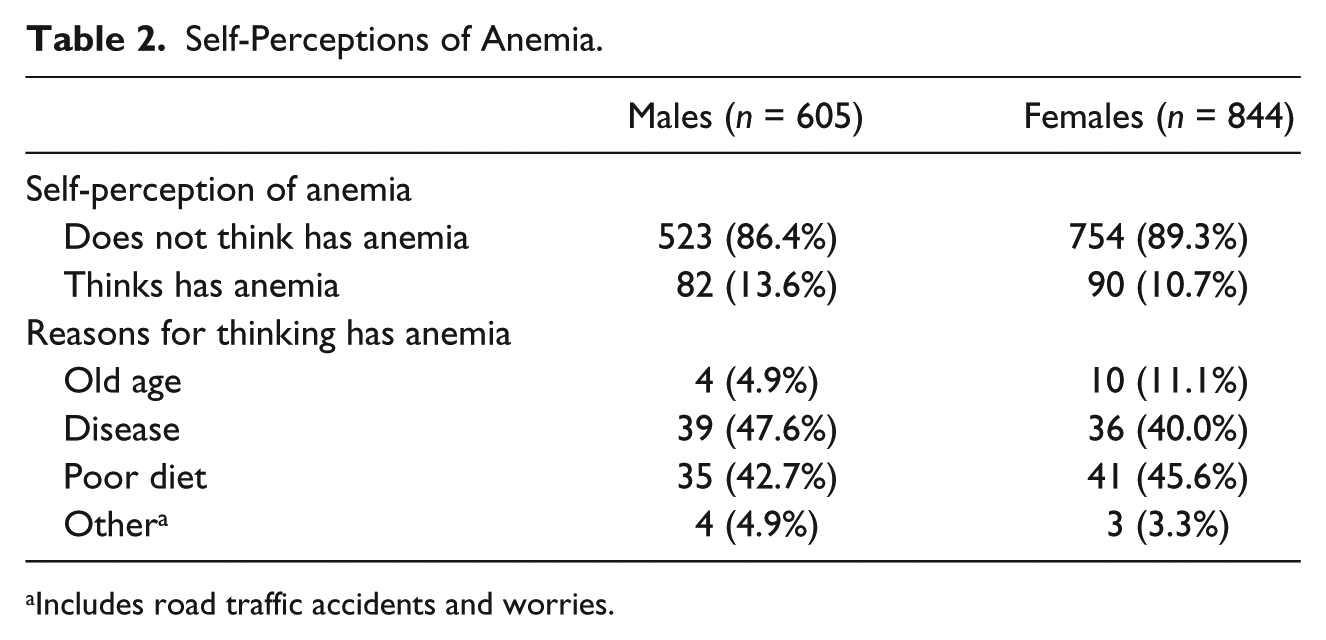
Includes road traffic accidents and worries.
The different reasons why older people thought they had anemia by sex, from the quantitative data are shown in Table 2. All the differences between men and women were statistically significant (p < .05). Among those who thought that they had anemia from the qualitative data, 6/8 thought they had anemia because they had symptoms suggestive of anemia such as “dizziness,” “weakness,” and “paleness of their bodies,” while 2/8 thought they had anemia because of poor feeding. From the quantitative data, there was strong evidence that people with anemia were more likely to perceive that they had anemia (18.4% vs. 10.2%, p < .001).
Local Terms Used to Describe Anemia
In this community, there was no local name for anemia. Older people used the following words to describe whether one was anemic “alina omusayi mutono” (he or she has little blood), “omusayi gumuweddemu” (his or her blood has run out), and “talina musayi ogumala” (he or she no longer has enough blood he requires). When asked about how they identify older people that are anemic, they said they identify them by the symptoms they develop. These symptoms included “kamuli” (yellowing of eyes or skin), “okuzimba” (swelling), “okutukulatukula,” or “okwelukirira” (paleness of the body), “okutangala amaaso” (paleness of the eyes), “okusanyalala” (paralysis or numbness), and “okutambula nga bazunga” (feeling dizzy and staggering while walking). Other terms used included “okugwamu amanyi” (weakness) and “kamunguluze” (dizziness).
Perceived Causes of Anemia Among the Older People
The causes of anemia among older people mentioned in these interviews included diseases such as malaria, HIV, and other chronic illnesses; excessive alcohol consumption; bleeding and poor feeding. Another cause mentioned was having many wives, A man, age 59 years, said, “When you have many wives when you are old, they suck the little blood you have from you . . . .”
The other causes mentioned were lack of bedding and working hard for long periods. A woman, age 67, said,
. . . some older people don’t have a place to sleep and don’t have beddings and yet they work hard for long periods. This can make them have little blood (anemia) . . .
Another cause of anemia mentioned was worry. An 82-year-old man with chronic anemia said,
. . . old age per se does not cause people to have little blood [anemia] if the person is feeding well and is not depressed by thoughts and worries that older people normally have . . .
One older woman mentioned “biwuka” or intestinal worms as a cause of anemia. She remembered worms because of her experience of anemia when she was still of child-bearing age. She said she had severe anemia and received a blood transfusion from a nearby hospital and on discharge, she was told the cause of her anemia was “too many worms in her stomach.” Therefore, she believed these worms could cause anemia among older people.
All 10 older people interviewed in the qualitative study attributed anemia to inadequate diet. When asked to describe what they understood by this, the following were mentioned: taking tea without sugar (3 older female respondents: 2 aged 55 and 1 aged 70), not eating meat for long periods (woman aged 69 and a man aged 88), eating foods like posho (maize flour boiled and mingled with water) and cassava for a long time (a woman aged 67 and a man aged 88), eating green vegetables (2 males; 1 aged 70 and another aged 67), eating good food (a male aged 82 with chronic severe anemia), and eating starch without vegetables or meat/fish (a woman aged 55). They thought these forms of poor diet caused anemia.
What Older People Do When They Think They Have Anemia or Symptoms of Anemia?
All the participants said that when they suspected that they had anemia, they would manage it at home or in the community and in case they failed to improve, then they would seek biomedical treatment from the health facilities. Two main methods of treating anemia in these communities were described which include herbal treatment and removing the “bad” blood responsible for the anemia.
Most of the older people interviewed (9/10) said the initial treatment used was a local herb known as “Muzukizi,” upon suspicion that one had anemia. This herb has green leaves and red roots and is grown in most homesteads within banana plantations (one of the main crops grown). It is administered either topically by mixing it with bathing water or orally by squeezing it in water and drinking its juice. Respondents differed on acceptable and administered dosages of the herb. When asked about the dose, one older person said “the plants (leaves) are crushed and mixed with water and boiled in the saucepan and when it cools, you take one plastic mug [500 ml] two or three times in a day.” Another older lady said “I have always used it when my daughter had anemia; we made for her 3 cups which she drank and became well.” When another man was asked about the dosage he said “tutebereeza” (we guess) the amount to take. Some older people said that this herb is good for treating anemia in pregnant women. One woman said “it is a helpful drug because even pregnant women with anemia use it, to prevent ‘Kamuli’” (neonatal jaundice).
Other herbs mentioned were avocado leaves, papaya leaves, “kirobo” (a herb with red roots), “akakwansokwanso” (a herb that makes a red coloration when squeezed in water), “ssere,” and a “kikalakala.” What seemed common with all these herbs is that most of them have reddish colorations that look like blood or turned red when squeezed in water. Older people said they used these herbs mainly because they are easily accessible, are free, or cost very little. Other older people believed that these herbs are very effective. One older woman (aged 58) said,
. . . people trust these herbs and think that they really work. Some people may be having enough money to go to hospital, but even those with money will first take these herbs when they have little blood [anemia] . . .
When treating symptoms suggestive of anemia especially headache and dizziness, where the head is perceived to be the problem part of the hair is shaved and a blood vessel is located and tied. In the first method called “okusama” in the local language, the blood vessel with “bad” blood responsible for the symptoms is cut with a knife or razor blade and the “bad” blood is left to ooze out. In the second method known as “Kuwubira,” the procedure is the same as in the “okusama” but, after the blood vessel has been cut, they apply a horn of a cow and the vacuum created sucks the “bad blood” out of the cut area. One man aged 82 years with a history of chronic anemia said “I have under gone this procedure but this was some years back. I had very severe headache. After the procedure, the headache disappeared and I felt well.” Another man aged 88 years said “In my village, older people no longer do it (kusama) but in other villages they do it.” He went on to say “but in my village they still do it (‘kusama’) on children with ‘bikubuuko’” (enlarged spleens).
What Happens When Older People Develop Anemia?
Most of the older people mentioned death, weakness, and failure to work as consequences of anemia. One moderately anemic lady aged 63 years said,
. . . before they found out that I had little blood [anemia], I had a lot of health problems . . . I felt weak . . . I went to many clinics and they thought I had asthma. I was treated but I did not improve. I did not know that my blood was not enough. I think if they had not taken blood from me to check my blood . . . I was going to die; having little blood can be very dangerous.
Another man aged 82 years said,
. . . they will get dizziness all the time if anemia is not treated. Because of this dizziness, it will prevent them from working and if not treated, they will eventually die.
When older people were asked to mention some of the diseases they thought were common among older people in their community, only one woman aged 58 years mentioned anemia. Other complaints such as musculoskeletal disorders (severe backache, joint pains and leg pains) were mentioned by all the participants. Other illnesses mentioned included fever (mentioned by six participants), high blood pressure (mentioned by four participants), gonorrhea/urinary retention (mentioned by three participants), upper epigastric pains (mentioned by three participants), and vision problems (mentioned by two participants).
Discussion
Whereas majority of the older people in this community have heard about anemia, there is no local name for it so people describe it by its symptoms. Most of the older adults perceived themselves as having anemia either based on symptoms or the perceived causes of anemia. Older people seemed to understand the consequences of untreated anemia. In addition, the use of herbs and other traditional methods for treatment of anemia were common. Older people seemed knowledgeable on symptoms suggestive of anemia and were mentioned. However, these symptoms of anemia are not specific to anemia. Other diseases such as hypertension, malaria, and renal disease can present with similar symptoms.
Most of the respondents were knowledgeable on the symptoms of anemia because they had experienced anemia themselves or a person in their family had experienced anemia. In studies done elsewhere in low income countries in women of reproductive age, women also described anemia by its symptoms like headache, dizziness, paleness, become yellow, fainting, weight loss and loss of appetite (Galloway et al., 2002; Young & Ali, 2005). This is not entirely surprising given that most of them may have previously attended antenatal care, where health education talks on anemia in pregnancy are normally offered.
Although respondents perceived anemia to be caused by poor diet or perceived themselves to be anemic because of their diet, their definitions of “poor diet” were varied. A number of older people understood it to be taking “tea without sugar” (which is something people who cannot afford sugar have to do). This may not be related to anemia but may be a reflection of the poverty levels older people in this community face which affects their diet. These findings agree with studies conducted among women of child-bearing age in low income countries, where most of the women associated anemia to poor diet (Ailinger, Moore, Pawloski, & Cortés, 2009; Jarrah, Halabi, Bond, & Abegglen, 2007; Jefferds, 2002; Young & Ali, 2005), but unlike in our study, these women were able to mention some foods rich in iron. The explanation for these differences may be the fact that women in the reproductive age groups are frequently educated on anemia especially those who attend antenatal care during pregnancy, unlike older people in our study population.
Finally on perceived causes, a number of older people perceived anemia to be caused by the ageing process alone. It is worth noting that although some cases of anemia may not have any identifiable cause and have therefore been linked to ageing, studies have shown that most of the anemia in people of advancing age can often be linked to an underlying cause and should be investigated and treatment provided (Ershler, 2003).
There was a strong preference for using herbs for the treatment of anemia even when free treatment is available (from the GPC clinic). This is not surprising because herbal remedies are often used for the treatment of common ailments in the study area. The use of herbs for treatment of anemia is a practice found in other places. In one study conducted in Kenya, it was noted that people within the East African region use medicinal plants in the treatment of anemia and extracts studied from eight of these medicinal plants showed that they had iron content (Omolo, Chhabra, & Nyagah, 1997).
It is not clear whether herbs used in this study population for treatment of anemia have any hematinic properties and further studies should be carried out on these herbs.
We used a mixed methods approach by collecting both qualitative and quantitative data to study older people’s perceptions on anemia. We believe this is one of the strengths of our study because this approach enabled us to augment the quantitative findings with more detailed explanations from the qualitative findings.
To the best of our knowledge, this is the first study to give some insights on older people’s perception of anemia in rural Uganda. This study advances knowledge on what older people in Uganda think about anemia, how they are able to identify older people with anemia, what they perceive to cause anemia and traditional treatments they use for anemia.
From the literature search we conducted, we were unable to find similar studies that have been conducted among the older people. As a result of this, interpretation of our findings in relation to other studies conducted among older people was limited. Most of the comparisons we have made in this article are with studies conducted in women of the reproductive age groups who may be different from older people. More similar studies among older people in different settings will build on the findings from this study.
This study has public health implications. In Uganda, older people are not included in anemia control programs. This study has established that anemia is a common disease among the older people although older people did not mention it as one of the common diseases. The knowledge of older people on the common causes of anemia was limited. In addition, use of traditional medications was very common. Based on findings from this study, we would recommend the following:
Anemia prevention and control programs should also target the older people through provision of education on the causes of anemia, common symptoms of anemia, available local foods rich in iron, and on the available biomedical treatments for anemia.
Research on the herbs used for anemia treatment to establish if they have any hematinic properties and could therefore be integrated in the interventions to control anemia.
Footnotes
Acknowledgements
We would like to acknowledge MRC/UVRI, Uganda Research Unit on AIDS, for funding this study. We would also like to acknowledge the following staffs from the GPC who participated in the fieldwork for collection of data for this article: Gershim Asiki, Alex Kalabarinde Mbabazi Peregrino, Charles Dickens Mweruka, Victoria Nakibirango, Grace Tumwekwase, and Laban Waswa and Monica Kuteesa. We would also like to thank all the older people within the GPC who participated in this study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for this research was provided by the MRC/UVRI, Uganda Research Unit on AIDS.