
Abstract
Keywords
Many people living with long-standing physical conditions such as spinal cord injury (SCI) or multiple sclerosis (MS) experience health problems and functional limitations that are a direct result of the underlying pathology of their medical condition. These limitations are often described as “primary” to their condition. However, it is also well-recognized that there exist a number of “secondary” health problems and symptoms that are indirectly caused or influenced by their primary diagnosis. These “secondary health conditions” (SHCs) may include symptoms such as chronic pain or fatigue, impairments such as worsening spasticity or balance problems, or related health problems such immunosuppression, urinary tract infection, or pressure ulcers ((U.S.) Institute of Medicine, 1991). SHCs in many cases create as much or more impairment than primary problems associated with the disabling diagnosis, especially by contributing to problems in employment (Schiavolin et al., 2013), social function (Ataoglu et al., 2013), and mental health (Padua et al., 2009). These difficulties are especially troubling given that many SHCs are known to be either preventable or treatable.
Despite an understanding of the importance of these conditions, defining what exactly constitutes an SHC and what does not has represented a challenge to the disability research field. Although a consensus definition of SHCs has proved elusive (Rimmer, Chen, & Hsieh, 2011), a hallmark report from the Institute of Medicine defines a secondary condition as one that “is causally related to a disabling condition (i.e., occurs as the result of a primary disabling condition) and that can be a pathology, an impairment, or an additional disability”((U.S.)., Institute of Medicine, 1991). In a recent conceptual paper on this topic, Rimmer and colleagues (Rimmer et al., 2011) provided a theoretical framework of SHCs that distinguishes between a “comorbidity” (i.e., a medical condition that may not be directly or indirectly related to the disability, such as diabetes), an “associated condition” (i.e., a condition that is directly associated with the etiology, such as paralysis), and a “secondary condition” (i.e., a medical or health problem that is not directly related to the disability diagnosis, occurs after the onset of the primary disability, and is more prevalent in people with disability, such as pain, fatigue, or weight gain).
A number of recent efforts have also attempted to create conceptual models of SHCs and describe how they may interrelate in persons with disability. Such models are important because they provide unified definitions of the SHC concept and allow researchers to identify potential antecedents, risk factors, and consequences of SHCs. For example, a conceptual model proposed by Jensen et al. (Jensen et al., 2012) hypothesized that disability (i.e., impairment, activity restriction, and participation restriction) is bi-directionally associated with SHCs, and that age-related factors can have a direct effect on the development and trajectory of SHCs. However, despite progress toward a unified conceptual definition of SHCs and a better theoretical understanding of how they may interact, to date very little work has sought to develop or test quantitative models of SHCs based on statistical relationships present in measured data. Furthermore, most previous work has focused on the effect of individual SHCs on outcomes, rather than including multiple SHCs and outcomes in a single, overall model. Such a model may better represent the complexity of living with a disabling condition, where an individual may experience symptoms as overlapping, interrelated and difficult to separate.
Any model that attempts to quantify the relationships among SHCs in a sample of persons with disability must also consider age. Parallel to a general graying of Western populations, the average age of individuals living with physical disabilities is also increasing. This is due in part to an increasing life span associated with advances in medical knowledge (for example, in MS; Minden, Marder, Harrold, & Dor, 1993) and greater early survivorship (for example, in SCI; DeVivo, Krause, & Lammertse, 1999) as well as a higher risk for new-onset disabling conditions in formerly able-bodied older adults as they get older. The relationship between increasing age and various secondary health conditions has been evaluated in separate studies of persons with disability, with most suggesting an increased incidence of chronic health problems and physical secondary health conditions with older age (LaVela et al., 2012) and more psychosocial or somatic concerns in younger adults (Tate, Forchheimer, Karana-Zebari, Chiodo, & Kendall Thomas, 2012). Several studies have suggested that physical symptoms such as pain and fatigue may be the most severe and impairing during middle age (Cook, Molton, & Jensen, 2011; Jensen et al., 2012; Molton et al., 2013). However, to our knowledge, no studies have evaluated the effects of age on SHCs in a comprehensive model that included multiple SHCs and multiple disability populations.
The Present Study
The present study sought to statistically evaluate a model of SHCs and their impact in a large sample of people with either SCI, MS, post-polio syndrome (PPS), or neuromuscular disease (NMD). In accordance with previously established conceptual models of SHCs (Jensen et al., 2012; Rimmer et al., 2011), we included only conditions or problems that (a) were reported after disability onset, (b) have been reported in the literature as more prevalent in persons with disability, and (c) did not simply represent a risk factor for developing SHCs (such as social isolation).
We also attempted to separate SHCs from chronic comorbid medical conditions (such as diabetes or osteoarthritis), and from the functional limitations that symptoms might cause, including problems with activities of daily living (ADLs). This was done in concordance with the Institute of Medicine’s (Field, Jette, Martin, & Institute of Medicine (U.S.), 2006) view that secondary conditions concept should be limited to physical and psychological health conditions, and not include other domains that might be influenced by the presence of a disability, such as activity limitations or barriers to social participation. This distinction allowed us to develop a model in which these individual domains can be viewed as mutually interactive.
As a final step, we tested the effects of chronological age on SHCs on key model parameters. Based on the considerations discussed above, we hypothesized that, in a large sample of individuals with early-onset physical disabilities,
A statistical model that separated SHCs from functional outcomes and chronic comorbid medical conditions would provide a good fit to measured data;
SHCs and chronic comorbid medical conditions would each be significantly, and negatively, associated with functional outcomes;
Chronological age would predict greater physical SHCs, poorer functional outcomes, and greater prevalence of chronic comorbid conditions, and demonstrate a U-shaped association with psychosocial SHCs (with greater psychosocial concerns in mid-life).
Method
Participants
Participants were 1,862 individuals recruited for an ongoing longitudinal survey study examining the frequency and impact of secondary health conditions in persons aging with early-onset physical disability. To be eligible, participants were required to be 18 years of age or older; be able to read, write, and understand English; and have a self-reported diagnosis of MS, SCI, NMD, or PPS. A full description of study inclusion and exclusion criteria is available from the study authors.
Measures
Measures for the present study included 10 individual scales, containing a total of 64 items. Although most individual items were contained in standardized scales, they were not forced to remain with the other items in their respective scales during the factor analyses (described later in this article). In many cases, item content from one scale overlapped with item content from another scale in the same factor, which allowed for better measurement of key constructs.
Demographic and diagnosis variables
All participants provided demographic and basic medical information, including sex, education and income level, geographic region, years of disability, and disability diagnosis. Self-reported age was verified via computation from reported birth date.
Secondary health conditions
Depression
Depressive symptoms were assessed using the Patient Health Questionnaire (PHQ-9). The PHQ-9 has been used frequently in populations with physical disability, and its validity and reliability have been supported (Bombardier et al., 2012; Fann et al., 2005; Kroenke, Spitzer, & Williams, 2001).
Pain intensity
Pain intensity was measured using four 11-point numeric rating scales (NRS) from 0 “no pain” to 10 “pain as bad as can be.” Participants rated the average, worst, least, and current intensity of their pain in the past 7 days. NRS pain scales have demonstrated acceptable psychometric properties in general and in persons with disabling conditions (Hadjistavropoulos et al., 2007; Jensen, 2010; Jensen & Karoly, 2000; Jensen, Karoly, O’Riordan, Bland, & Burns, 1989).
Medical symptoms
The presence and average severity of a range of common physical symptoms experienced over the past week were assessed using an 11-point NRS, in which a 0 score indicated “none” and a 10 indicated that the symptom was “as bad as you can imagine.” Specifically, participants rated their average severity of weakness, fatigue, imbalance, numbness (anywhere in the body), numbness in hands or feet only, vision loss, shortness of breath, disturbed sleep, and spasticity. The psychometric properties of NRS scales in this population have been supported in previous studies (Jensen & Karoly, 2000; Jensen et al., 1989).
Speech and swallowing
The average severity of speech problems and swallowing problems were assessed via two items in which participants were asked to rate “how much of a problem” these symptoms were on a 0 “not at all” to 5 “very much” scale. Questions were adapted from previous studies that presented valid and reliable data (Smith, Della Sala, Logie, & Maylor, 2000; Yorkston et al., 2003).
Sleep disturbance
Sleep problems were assessed using eight items taken from the Sleep Disturbance item bank of the NIH Patient Reported Outcomes Measurement Information System (PROMIS). Participants were asked to rate their sleep (in terms of maintenance, quality, initiation, etc.) in the past 7 days on a 5-point scale. The validity and reliability of PROMIS item banks have been evidenced in persons with disabilities (Buysse et al., 2010; Cook, Bamer, Amtmann, Molton, & Jensen, 2012).
Skin problems and urinary tract infections
The history of skin problems and urinary tract infections was measured using questions from the 2001 Washington State Behavioral Risk Factor Surveillance System (BRFSS) Disability Supplement. Two questions asked participants whether they had skin problems (pressure sores or ulcers) or a urinary tract infection in the past 12 months (Kinne, Patrick, & Doyle, 2004; Wilber, Mitra, Walker, & Allen, 2002).
Fatigue
Fatigue was assessed using seven items selected from the PROMIS item bank. Questions were rated on a 1 “never” to 5 “always” scale and asked participants to rate various experiences of fatigue and exhaustion in the past 7 days. This PROMIS Fatigue item bank has been validated for use in populations with disabilities (Cook et al., 2012; DeWalt, Rothrock, Yount, & Stone, 2007).
Medical comorbidities
Chronic health conditions
Prevalence of chronic conditions such as hypertension, coronary heart disease, arthritis, and diabetes was measured with items taken from the National Health Interview Survey (NHIS) Adult Core from the Center for Disease Control (CDC).
Functional impairments
Instrumental activities of daily living (IADLs)
Participants’ ability to perform ADLs was measured with the Instrumental Activities of Daily Living survey, from the NHIS Phase II Supplement on Aging Questionnaire (Scotch, 1994). Questions were scored on a 0 “no difficulty” to 3 “unable to do” scale based on the ability to perform various daily tasks, such as bathing, dressing, eating, and walking a quarter of a mile.
Physical functioning
Physical functioning was measured using a 12-item short form from the PROMIS Physical Function item bank. The measure asked participants to rate how much difficulty they would have doing various activities, including putting on or taking off a jacket, walking more than a mile, carrying groceries, doing housework, or standing up from a low couch, on a 1 to 5 scale (DeWalt et al., 2007; Rose, Bjomer, Becker, Fries, & Ware, 2008).
Procedures
Participant recruitment
We recruited participants using several strategies. Invitations (n = 1,692) were sent to potential subjects who participated in previous University of Washington Studies through the University of Washington Disability Registry (n = 398), the University of Washington Center on Outcomes Research in Rehabilitation (n = 473), and through disability specific registries (Northwest Regional Spinal Cord Model Systems and the University of Rochester NMD Research Registry, n = 375). Some participants responded to web and print advertisements (n = 795) posted in clinics and with disability support organizations (National MS Society, Post-Polio Health International, Muscular Dystrophy Foundation).
We then mailed surveys to all eligible and interested subjects (n = 2,041) along with a postage paid return envelope. Reminder letters were sent 3 to 6 weeks after the survey was mailed to those who had not yet returned their survey. Research assistants reviewed returned surveys (N = 1,877; 91% response rate) for missing data and made up to three follow-up calls to retrieve the data. All participants were sent a check for $25 after their survey was returned. All procedures were approved by the University of Washington Institutional Review Board, and signed informed consent was obtained from all participants.
Of the 1,877 surveys that were returned, 15 were excluded due to lack of signed consent, lack of valid diagnosis of disability, return of survey after the dataset was finalized, or a request to withdraw from the study. The remaining 1,862 surveys were included in the final data set (MD = 340, PPS = 446, MS = 584, SCI = 492).
General analytic approach
For conceptual clarity, after selecting the self-reported secondary conditions for the analyses, we then divided them into three broad categories. The first category contained items that were primarily physical in nature, including symptoms such as infection, problems with skin integrity, weakness, neurological problems, and muscle problems. We labeled this group “physical secondary health conditions.” The second group contained symptoms that involved primarily psychological distress (e.g., depression) or somatic experiences with a significant psychosocial component (e.g., fatigue). We labeled this group “psychosocial secondary health conditions.” This decision to separate these two groups was made to be consistent with the common language describing secondary health conditions, which very frequently distinguishes between “physical and mental health problems” (Brandt, Pope, & Institute of Medicine (U.S.). Committee on Assessing Rehabilitation Science and Engineering, 1997; Jensen et al., 2012; Pope & Tarlov, 1991). 1 The third category contained items referring to pain intensity and was labeled “Pain.” We felt that pain warranted its own category separate from the “physical” and “psychosocial” domains, because (a) chronic pain is widespread and impairing in persons with disability and (b) the experience of chronic pain may contain both physical and psychosocial elements in equal proportion, such that placing these items entirely in a “physical” or “psychosocial” category is inconsistent with current biopsychosocial perspectives on pain.
Because we were interested in a model that represented a broad view of health and function, we also included two categories representing additional difficulties faced by those aging with disabling conditions. The first of these contained diagnosable chronic disease states or medical comorbidities, such as diabetes, hypertension, and heart disease. In Rimmer and colleague’s (Rimmer et al., 2011) model, these are labeled “comorbidities,” but we chose to label them “chronic medical conditions” (CMCs) to be consistent with the larger geriatric literature. Conceptually, some CMCs are more prevalent in particular disability groups, and might therefore have been included in the “secondary health conditions” category. However, we chose to keep them separate to aid in clarity of interpretation of the model. Finally, to determine the effect of SHCs on day to day activities, we created a second additional factor that contained problems with function, including ADLs and ambulation. This factor was labeled “functional impairments.”
Data analysis and statistical package
The present study used Structural Equation Modeling (SEM). SEM is a statistical technique that allows for both exploratory and confirmatory modeling of a large number of variables simultaneously, making it an ideal approach for testing theoretical models. A major strength of the SEM approach is that it allows for the creation of “latent” variables, which are conceptual variables that are not measured directly but rather estimated from several measured variables. These latent variables are free of measurement error in the sense that the creation of latent variables allows one to estimate the unreliability of measurement in the model, and thereby accurately estimate the “pure” associations among latent variables.
SEM analyses were conducted using the software program Mplus 6.0 (Muthen & Muthen, 2010). Mplus creates unbiased estimates of parameters using a full information maximum likelihood approach, under the assumption that missing data are missing at random. All paths were tested for significance using a t-criteria of >1.96 (p < .05). Model fit was established using a multiple fit index approach following guidelines suggested by Hu and Bentler (Hu & Bentler, 1999), including a standardized root mean squared residual (SRMR) of <.06, a root mean squared error of approximation (RMSEA) of <.05, and a Comparative Fit Index (CFI) of >.95.
Analyses for the present study were conducted in a series of six steps, described below.
First, based on the extant literature, we specified a model based on the five broad categories described above. This meant assigning each of our 64 symptoms to three categories representing SHCs (Physical SHCs, Psychosocial SHCs, and Pain) and to two categories representing related concepts (CMCs and functional impairments). Specifically, items were placed as follows: CMCs (4 items related to the presence of a diagnosed medical condition, including hypertension, coronary heart disease, osteoarthritis, and diabetes) Physical SHCs (12 items related to symptoms directly associated with a disabling condition, such as spasticity, numbness, and weakness) Psychosocial SHCs (31 items related to a range of difficulties reflecting emotional distress, including mood and sleep) Pain (5 items related to pain intensity over the past week) Functional impairments (23 items describing ability to perform tasks of daily living, including ADLs, IADLs, and ambulation)
Next, we split our sample randomly into two groups of 931 individuals (i.e., a “split half”) and performed exploratory factor analysis (EFA) on each of the five groups of variables described above. This was done to determine how the items in each group organized themselves. We allowed that this might include creation of second-order latent factors containing multiple first-order latent factors.
Using the other split half of 931 individuals, we performed confirmatory factor analysis (CFA) on each of the latent factors identified in Step 2, to confirm the stability of the factor structure identified in the EFA.
Using the entire sample, we then tested a model including all identified latent factors and evaluated relationships among key model parameters.
After establishing a stable model with good fit indices, we evaluated the linear and curvilinear effects of age on key model parameters.
Results
Descriptives
Participants in the study were between 20 and 94 years old (M = 56.13, SD = 13.31), were primarily non-Hispanic White (94%), and were more likely to be women (63%) than men. Participants were generally well-educated, with 86% having had some form of education beyond high school. More than half (58%) of the participants were married, with 53% reporting an individual income of less than $25,000/year (24% of the participants report annual household income under $25,000). Regarding time since diagnosis, participants with PPS (n = 446) reported a mean duration since being diagnosed of 16.08 years (SD = 9.95), followed by those with SCI (n = 492; 15.67 years [SD = 11.22]), those with MS (n = 584; 15.27 years [SD = 10.12]), and those with MD (n = 340; 14.73 years [SD = 11.45]).
Participants with PPS were significantly older (M = 67.22) than participants with other diagnoses, and participants with SCI were significantly younger (M = 50.02) than participants with other diagnoses, F(3, 1858) = 191.05, p <.001. These descriptive data are presented in Table 1.
Selected Demographic Characteristics.
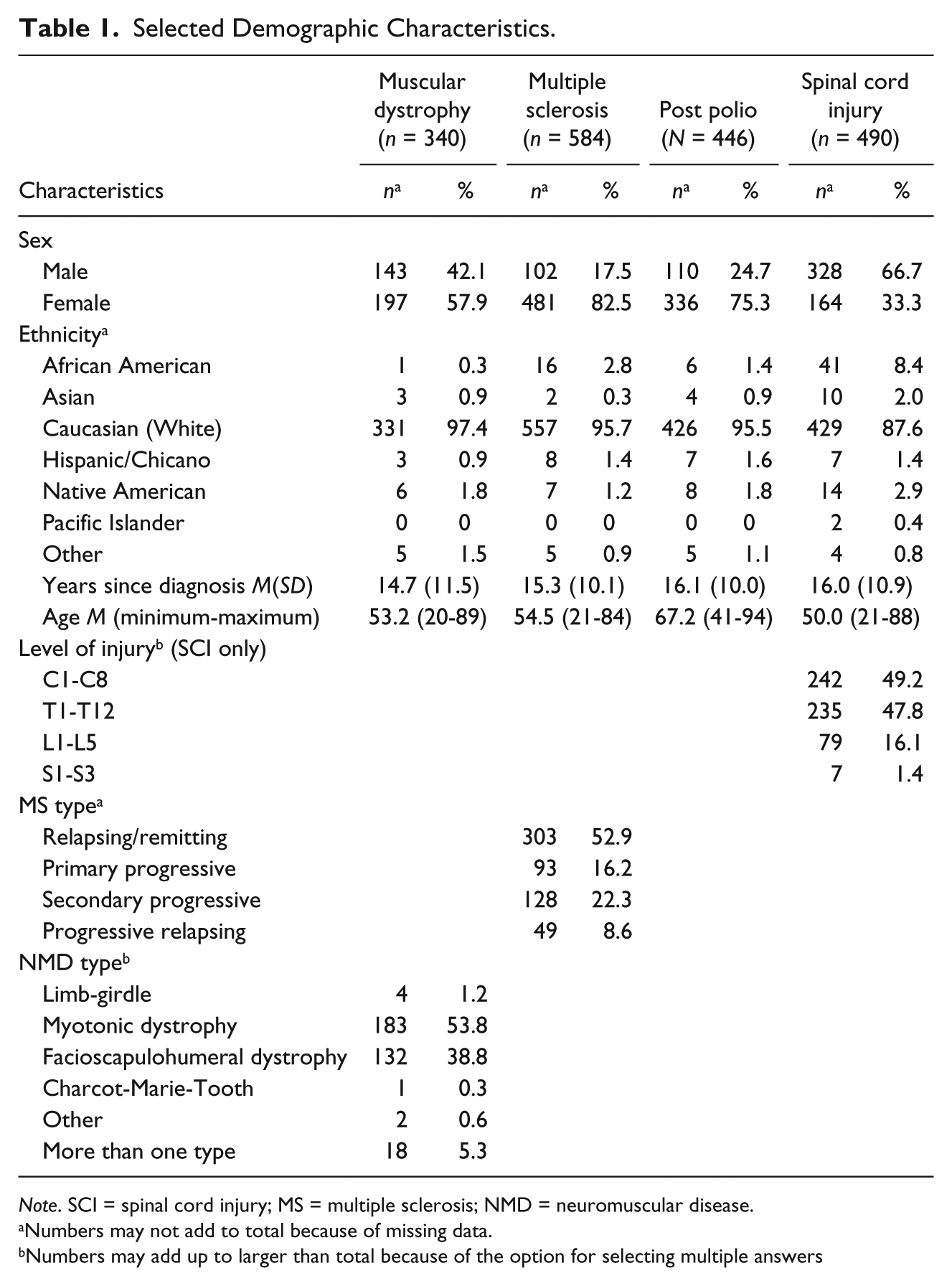
Note. SCI = spinal cord injury; MS = multiple sclerosis; NMD = neuromuscular disease.
Numbers may not add to total because of missing data.
Numbers may add up to larger than total because of the option for selecting multiple answers
Establishing the Measurement Model
As described above, EFA was performed on each of the five domains (Physical SHCs, Psychosocial SHCs, Pain, functional impairments, and CMCs), using a split-half of the full sample. Following the EFA process, CFA was then performed on the same latent factors separately using the remaining 931 individuals (the remaining half of the sample). For this step, correlated error terms were allowed within each first-order latent if suggested by significant Lagrange modification indices. For the sake of space, the individual EFA and CFA models comprising the larger measurement model are not presented as figures in this article, but are available from the study authors.
Physical SHCs
Analysis of the EFA results for the Physical SHC factor suggested a second-order structure containing four first-order factors. The first contained only two items describing weakness and imbalance, and was labeled “Weakness.” The second contained three items describing numbness (general numbness, and numbness of the hands and feet) as well as spasticity. This factor was labeled “Neurological Problems.” The third factor contained four items describing problems with speech, swallowing, breathing, and vision. This factor was labeled “Speech/Vision.” Finally, the fourth factor contained two items related to infection (urinary tract infection and skin integrity problems). This factor was labeled “Infection.” Model fit for the second-order latent (containing all four first order latents) was acceptable, SRMR = .022; RMSEA = .062; 90% CI = [.048-.076]; CFI = .993. CFA of the physical SHC latent confirmed the four-factor structure identified in the EFA. Modification indices suggested correlated error terms among several items, likely due to overlap in content (general numbness and numbness in hands and feet, and problems with speech and problems with swallowing). The final CFA model was a good fit to the data, SRMR = .032; RMSEA = .036; 90% CI = [.026-.047]; CFI = .985.
Psychosocial SHCs
Data from the EFA of the psychosocial SHC variables suggested a second-order factor containing three first-order factors. The first contained 10 items describing sleep problems, including difficulties initiating and maintaining adequate sleep. This factor was labeled “Sleep Problems.” The second factor contained 7 items describing depressed mood (all of which came from the PHQ-9). This factor was labeled “Depression.” The third factor contained 5 items describing fatigue severity and impact, and was labeled “Fatigue.” Initial model fit for the Psychosocial SHC latent was acceptable SRMR = .06; RMSEA = .08; 90% CI = [.08-.09]; CFI = .90. CFA confirmed the three-factor structure. Errors were allowed to correlate within each factor, specifically among pairs of sleep, mood, and fatigue items based on significant Lagrange modifiers. Following correlation of error terms, the final model was a good fit to the data, SRMR = .04; RMSEA = .05; 90% CI = [.044-.055]; CFI = .97.
Pain
To support our decision to make Pain a separate latent factor, rather than include pain items within the “Physical” or “Psychosocial” factors, we first tested an alternative model for each of these second-order latents, which included pain items. In both cases, model fit decreased, justifying Pain as its own category. As a separate factor, EFA of the five Pain items supported a unidimensional structure, and this was confirmed in the CFA sample: SRMR = .03; RMSEA = .20; 90% CI = [.18-.22]; CFI = .96. Allowing correlation of suggested error terms, fit improved slightly, SRMR = .01; RMSEA = .13; 90% CI = [.08-.19]; CFI = .99.
CMCs
The CMCs factor showed a unitary factor structure consisting of four items associated with being diagnosed with a CMC (presence of hypertension, presence of diabetes, presence of coronary heart disease, and presence of osteoarthritis). Model fit for the latent was excellent, SRMR = .011; RMSEA = .023; 90% CI = [.000-.056]; CFI = .993. CFA confirmed a single factor structure, and modification indices suggested no correlated error terms. Model fit for the CFA was also good, SRMR = .006; RMSEA = .00; 90% CI = [.00-.08]; CFI = 1.00.
Functional impairments
Data from the EFA of the functional impairments latent factor suggested one second-order factor containing three first-order latent factors. The 1st of these factors contained 10 items describing problems with activities of everyday living, including bathing, dressing, toileting, and getting in and out of bed without help. This factor was labeled “ADLs.” The second factor contained 7 items describing higher-level activities, including preparing meals, shopping for groceries, using a telephone, and independent medication management. This factor was labeled “IADLs.” Finally, the third factor contained 6 items describing ambulation and ability to engage in moderate physical activity. Items included ability to walk for a quarter mile, ability to walk on a steep surface, ability to carry groceries, and ability to walk for 15 min. This factor was labeled “Ambulation.” Model fit for the functional impairments latent was acceptable, SRMR = .036; RMSEA = .094; 90% CI = [.091-.099]; CFI = .912. CFA of the functional impairments latent confirmed the three-factor structure specified in the EFA. Per significant Lagrange modification indices, errors were allowed to covary within each factor, among pairs of particular items describing ambulation, activity, eating, toileting, bathing, and using the telephone. The final model was also an adequate fit to the data, SRMR = .076; RMSEA = .097; 90% CI = [.094-.100]; CFI = .907.
Structural Model
After establishing adequate psychometric properties for the first- and second-order factors in the model, we tested an overall structural model including all these factors simultaneously using the entire sample (n = 1,862). Residual variances between the following first-order factors were allowed to correlate based on LaGrange modification indices (due to overlap in question content): Infection and Neurological Problems, and ADLs and IADLs. This model demonstrated adequate fit to the data: χ2(1944) = 9887.83, p < .001, χ2 / df = 5.08; CFI = .91; RMSEA = .047; 90% CI = [.046-.048]; SRMR = .060. The full model, including all items and loadings, is presented in Figure 1, with a list of individual items and their abbreviations in Table 2. A simplified visual model to aid in interpretation of these results is presented in Figure 2.
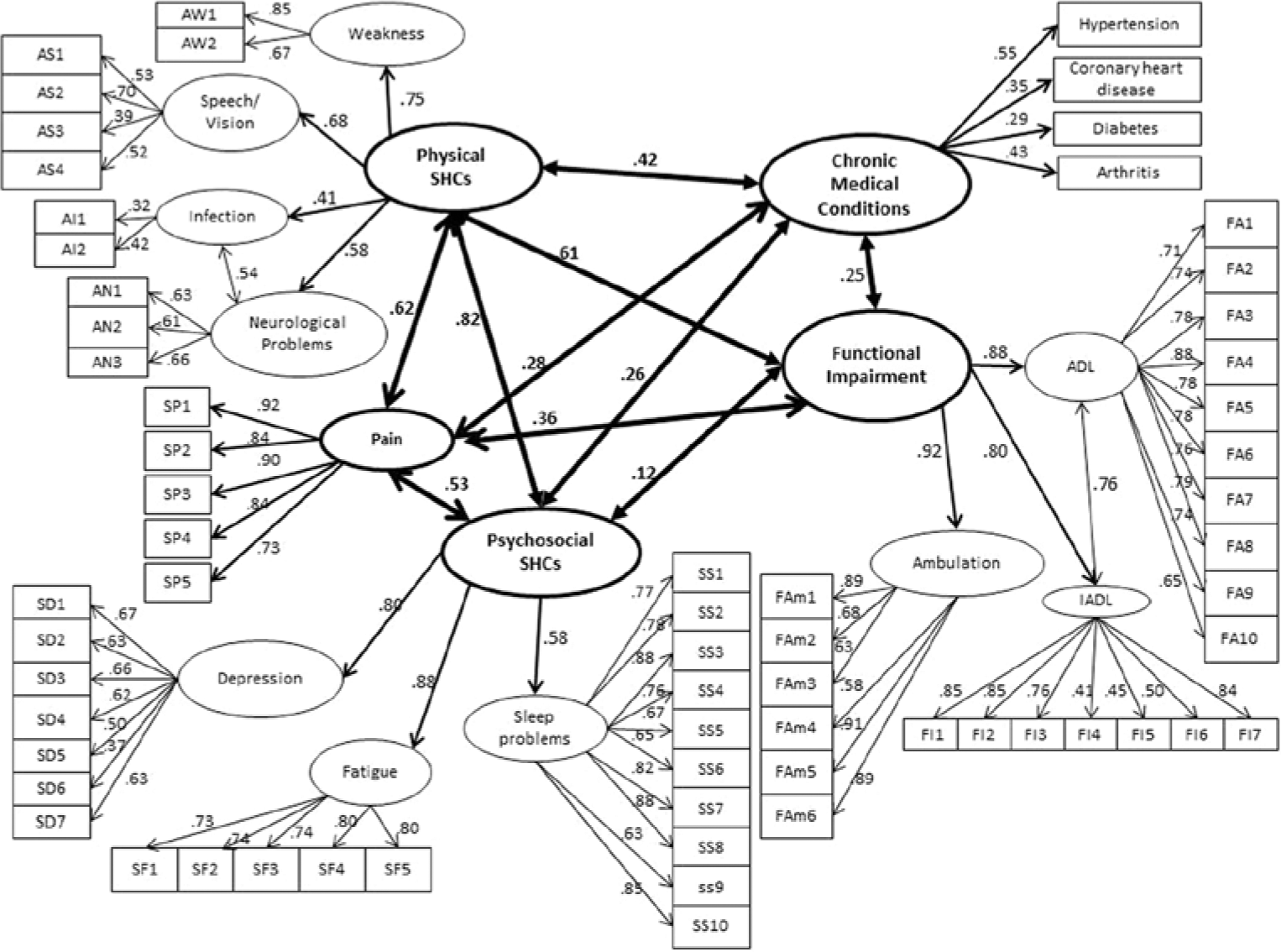
Fully standardized structural model.
List of Figure 1 Scale Items and Their Respective Item Codes.
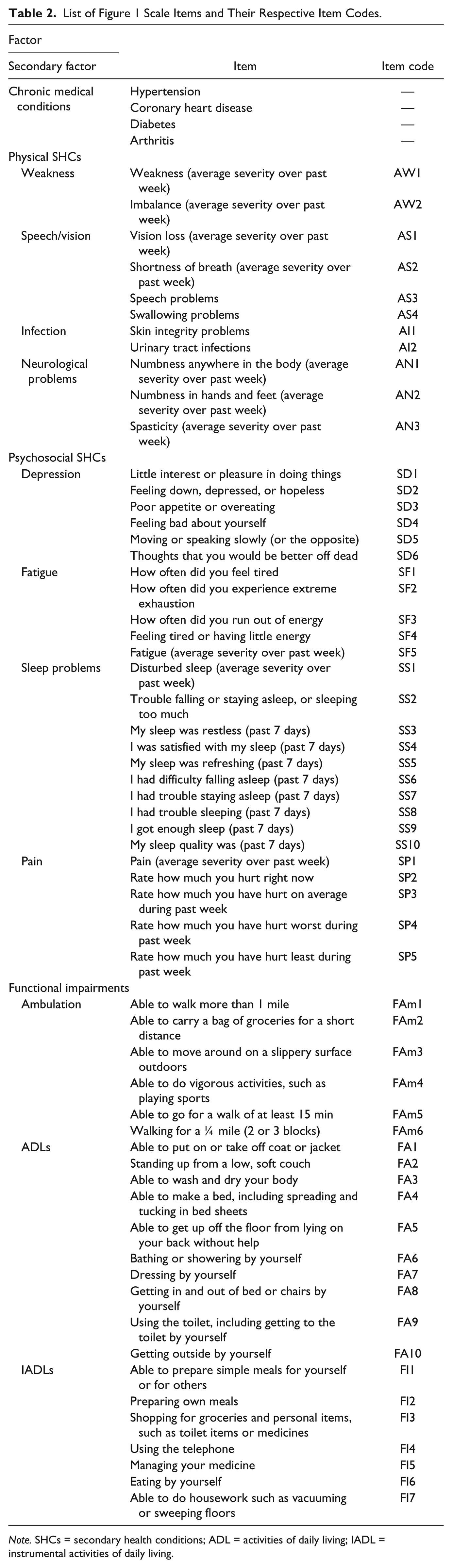
Note. SHCs = secondary health conditions; ADL = activities of daily living; IADL = instrumental activities of daily living.
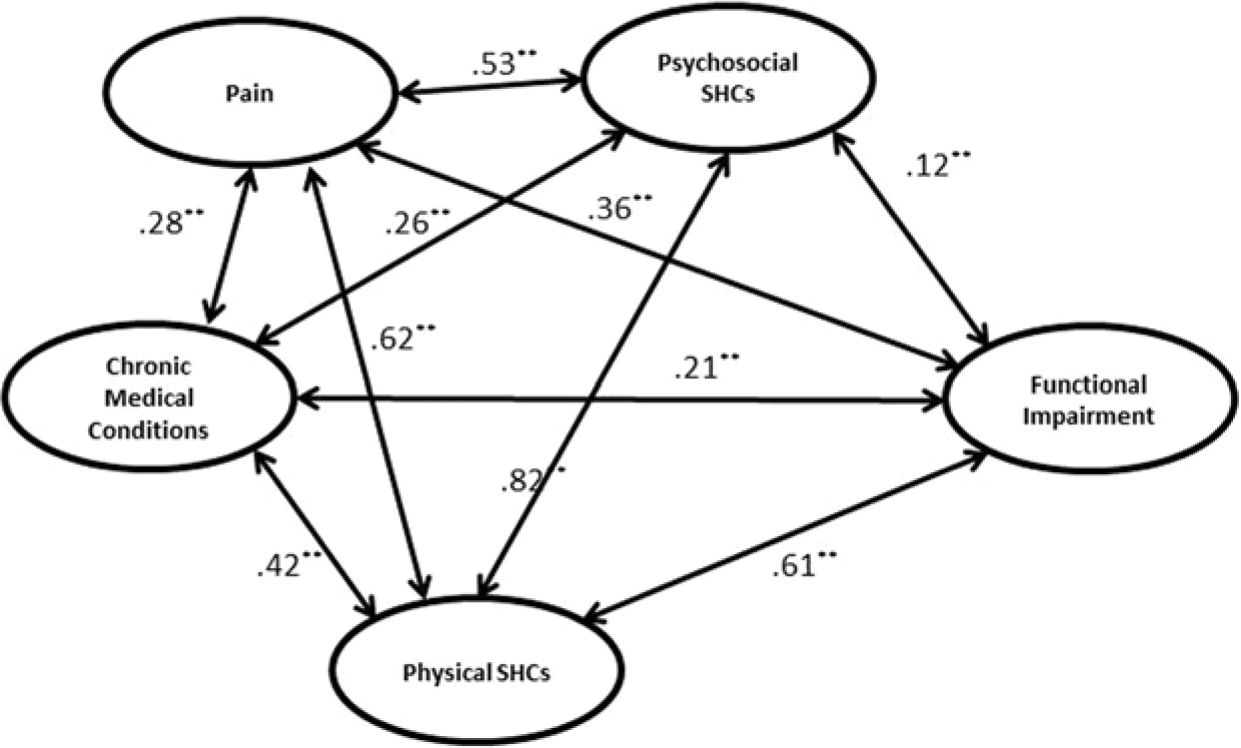
Simplified interpretive model.
Relationships among symptom domains
To control for multiple comparisons in the model, alpha for significance of any given path was adjusted to p < .001. As expected, results demonstrated strong relationships among the four symptom or disease-based latent domains, including between Physical SHCs and Psychosocial SHCs (β = .82, p < .001), Psychosocial SHCs and CMCs (β = .26, p < .001), and Physical SHCs and CMCs (β = .42, p < .001). As expected, the Pain factor was also significantly associated with Physical SHCs (β = .62, p < .001), with Psychosocial SHCs (β = .53, p < .001), and with the presence of CMCs (β = .28, p < .001).
Similarly, all four of these symptom-based latent domains were significantly associated with functional impairments. The functional impairments factor was related to CMCs (β = .25, p < .001), Physical SHCs (β = .61, p < .001), Psychosocial SHCs (β = .12, p < .01), and Pain (β = .36, p < .001). These pathways can be seen in Figure 1.
Effect of chronological age
To evaluate the effects of chronological age on factors in the model, we hypothesized the existence of both linear and curvilinear (i.e., U-shaped) relationships of age with SHCs, functional impairments, and CMCs. To test age hypotheses, we performed a separate analysis that included all the paths specified in Figure 1, as well as paths from centered versions of age and age2 to each second-order latent factor. Where a significant curvilinear relationship was detected, we performed follow-up testing by dividing age into three broad categories: 0-44, 45-64, and 65+. For simplicity of presentation, this model is not presented in full here, but fit indices were essentially the same with the inclusion of the age and age2 variables and pathways, χ2(2064) = 10482.42, p < .001, χ2 / df = 5.08; CFI = .90; RMSEA = .047; 90% CI = [.046-.048]; SRMR = .06.
Results of the linear age analyses suggested that increasing age was associated with greater Physical SHCs (.21, p < .001), greater functional impairments (.25, p < .001), and greater frequency of CMCs (.67, p < .001). Age was not linearly associated Psychosocial SHCs (−.04, p = .17) or Pain (−.01, p = .61).
Regarding the curvilinear age analyses, for CMCs and Physical SHCs, the curvilinear term was not significant after alpha correction, suggesting that the relationship between age and increased prevalence of health problems and physical SHCs is approximately linear, with older adults reporting more of these kinds of problems than younger adults. However, there were also several instances in which data showed that the relationship of age and outcome was better conceptualized as curvilinear. For Psychosocial SHCs, the age2 term was significant (−.13, p < .001), and follow-up testing revealed that individuals in the middle-aged group (i.e., those between 45 and 65 years) reported more Psychosocial SHCs than did either younger or older adults (.15, p < .001). Being over age 65 years was associated with lower levels of Psychosocial SHCs (−.13, p < .001), and being younger than 45 years did not show a statistically significant difference from the other groups after alpha correction (−.05, p = .05). The curvilinear term was also significant in the case of the functional impairments factor (.08, p < .001). Individuals over age 65 years reported the greatest levels of functional impairments as compared with the other groups (.19, p < .001). Being middle-aged or in the youngest age group was associated with lower levels of functional impairment, and this line increased with age in an asymptotic curve, rather than in linear fashion (younger = −.12, p < .001; middle-aged = −.08, p < .001). Finally, there was a curvilinear effect of age on the Pain factor (−.07, p <.001), suggesting that middle-aged individuals reported the highest pain levels (.08, p <.001), relative to younger or older adults.
Discussion
This study sought to statistically evaluate the interrelationships among a number of symptoms, conditions, and impairments that have a higher prevalence in persons with physical disabilities, and to determine the effect of age on these problems. We based our approach on published conceptual models of secondary health conditions in persons with disability (e.g., (Rimmer et al., 2011), using a large, cross-sectional sample of people with MS, NMD, SCI, or PPS.
The key finding from these analyses is that, from a statistical perspective, secondary health conditions and their impact may be conceptualized in five broad, interrelated categories: (a) “physical secondary health conditions,” (including somatic problems such as infection, weakness, and difficulties in speech); (b) “psychosocial secondary health conditions,” (including problems such as depression, fatigue, and sleep difficulty); (c) “pain,” (d) “functional impairments,” (including difficulties with ambulation and ADLs); and (e) “CMCs” (including bodily systems problems such as hypertension and diabetes). The first four of these represent SHCs in the purest sense, and the last factor (functional impairments) represents an area that, although technically not an SHC by a conservative definition, provides important information about health and function. This five-factor model was a good fit to the data in our sample and may be an appropriate framework for epidemiological studies investigating the broad health context of people with physical disability.
These data also suggest that, at least in this sample, certain kinds of SHCs showed stronger relationships to function than others. For example, physical problems (including pain, weakness, and neurological symptoms) were more powerful detractors of daily function than were psychosocial concerns (e.g., depression, fatigue, and difficulties with sleep). However, the fact that physical and psychosocial elements contributed significantly to poorer daily function emphasizes the need for a comprehensive, multidisciplinary, and well-coordinated treatment approach that has been advocated elsewhere. As expected, CMCs such as hypertension, diabetes, and arthritis were associated with functional impairments, although to a lesser extent, than were physical symptoms or pain.
Our age analyses revealed several interesting relationships. First, physical symptoms and the presence of CMCs appear to increase more or less linearly with age. This is a fairly obvious finding and highlights the reality that older adults are at greater risk for conditions such as hypertension and diabetes. However, we can now see that this same trend exists for persons aging with physical disability. It has also been suggested that individuals with disabling conditions may develop systemic health problems at an increased rate relative to the able-bodied population [i.e., the “accelerated aging hypothesis,” (Denes, 1965; Ohry, Shemesh, & Rozin, 1983)], although we are unable to test this hypothesis in this data sample. Regardless, to the extent that these chronic conditions are treatable, effective management is critical in promoting function and well-being for older adults with physical disabilities. Given that a number of studies have shown obesity and inactivity as key mediating variables in the relationship between age and metabolic conditions, the findings also emphasize a need for widespread and accessible interventions to target weight gain and inactivity in people aging with physical impairments.
Age also demonstrated several curvilinear relationships. In our sample, psychosocial distress and psychosocially-influenced somatic symptoms (including pain, fatigue, and insomnia) formed a U-shaped curve, reaching their greatest severity during mid-life. This may be interpreted as evidence that the phenomenon sometimes described as a “midlife slump” in other samples (e.g., Blanchflower & Oswald, 2008) also exists for persons with physical disabilities. This finding is consistent with other work, which suggests that this tendency to greater distress and pain during mid-life may be even more pronounced or longer-lasting in disability (Cook et al., 2011; Molton et al., 2013). From a life-contextual perspective, this may be because mid-life is associated with a number of unique stressors, including career peak, retirement planning (or early retirement), financial strain, empty nest, and, in some cases, the phenomenon of “sandwich generation” (i.e., caring for children and aging parents simultaneously). Especially for someone with a long-standing physical disability, this is likely a period of the highest environmental demand colliding with emerging physical health problems, creating a disparity between environmental expectations and perceived ability to meet those expectations. The findings also highlight the importance of providing support especially to middle-aged persons with disabilities. This support might include, for example, self-management tools to manage the impact of SHCs such as pain and fatigue in the workplace, to prevent early involuntary retirement.
This study has a number of important limitations. First and foremost, findings are based on self-report, cross-sectional data. Self-report of activities may be prone to embellishments and omissions, and the cross-sectional nature of our study limits our ability to draw any conclusions about causation among study variables. For example, we can conclude from these data that pain is associated with self-report of functional limitations; however, we cannot conclude that pain causes these limitations or vice versa. Furthermore, there are many secondary health conditions and CMCs experienced by people with disabilities that were not measured in this study, and many additional factors (such as social support and access to medical care) that we did not address in these analyses. The merging of four separate disability groups brought with it its own problems and complexities, including the fact that models based on multiple groups may not be as useful to clinicians providing care to one group or another, and are confounded by demographic and medical factors. However, this approach allowed us the sample size necessary to test overall, global models of the relationship among symptoms, disease, function, and age, across disability. Regardless, this was certainly a trade off in terms of specificity of the data, and further work may test the proposed models in individual impairment groups.
In considering these results, it is also important to remember that the purpose of this analysis was not to generate a comprehensive list of “secondary” conditions for people with disabilities. In fact, such a list would likely not be useful, because the distinction between what is “secondary” versus what is “primary” or “associated” depends in large part on the specific disabling diagnosis. We made the decision not to distinguish between “secondary” and “associated” conditions in our comprehensive model to include as many disabling conditions as possible in our analyses. Although our approach was data driven, it was not completely atheoretical, as we classified each symptom and condition into a broad latent group a priori. This decision-making process was naturally imperfect. For example, in our analyses we made a distinction between “psychosocial” and “physical” SHCs. This decision was made to be consistent with previous language describing secondary health conditions as reflecting “physical or mental health problems” (Brandt et al., 1997; Jensen et al., 2012; Pope & Tarlov, 1991). By making this distinction, we do not mean to imply that such “psychosocial” SHCs do not have physical cause—such a statement about sleep, for example, would be patently ridiculous for individuals with SCI. Rather, we thought that these symptoms all shared a link with underlying distress that might be (and in fact, was) captured in our analyses. However, the placement of such conditions in the “physical” versus “psychosocial” group is naturally imprecise, as such placement may be idiosyncratic to a particular disability or may not reflect that many of these symptoms have biopsychosocial antecedents and impacts. Moreover, we found considerable overlap between these two latent groups, as evidenced by their very high intercorrelation (.82, p < .05). In short, we separated these groups to help simplify interpretation of the model and be consistent with previous models, but such a separation may not be essential.
Other limitations stem from the generalizability of our sample. Although we made significant efforts to recruit underrepresented groups of individuals with disability, our sample was largely Caucasian. Moreover, and because these data were taken from a study focusing on aging with disabilities, the mean age was 56 years. It is unclear whether these models would generalize to younger or more diverse samples of persons with disability.
Despite these limitations, taken together, the study findings emphasize the importance of SHCs in persons aging with physical disability and underscore the importance of effectively measuring and treating SHCs to maximize independent function. Further work, including longitudinal analysis of large databases, is required to define and refine the “secondary health conditions” concept and determine which symptoms are the most affecting for which populations, and when.
Footnotes
Authors’ Note
The article contents do not necessarily represent the policy of the U.S. Department of Education, and readers should not assume endorsement by the U.S. Federal Government.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The contents of this manuscript were developed under grants from the Department of Education, NIDRR grant numbers H133F110019 and H133B080024. However, those contents do not necessarily represent the policy of the Department of Education, and you should not assume endorsement by the Federal Government.