
Abstract
Keywords
Social and behavioral gerontologists have made significant inroads in the study of wisdom (Ardelt, 2003; Baltes, 2004; Staudinger & Gluck, 2011). As there is no consensus in the literature on how to define wisdom, we rely on a definition that is comprised of the main components of wisdom that are identified by Baltes (2004). He argues that wisdom is reflected in concern with the important and difficult questions about the conduct and meaning of life that is tempered by an awareness of limits of knowledge and the uncertainties in life. Baltes (2004) goes on to point out that wise people make a superior judgments and offer sound advice, and they display an uncanny ability to orchestrate knowledge and virtues. As Schwartz and Sharpe (2006) point out, there is more than one type of wisdom. We focus on practical wisdom, which is defined as a “ . . . master virtue essential to solving problems of specificity, relevance, and conflict that inevitably arises whenever character strengths must be translated into action in concrete situations” (Schwartz & Sharpe, 2006, p. 377).
In the process of assessing practical wisdom, we address two issues that embed this important virtue in a broader theoretical context. The first has to do with identifying the social factors that contribute to the development of wisdom while the second involves seeing whether practical wisdom is associated with health.
Although a number of social forces may shape practical wisdom, we focus on the potentially important influence of the church (Davies, 2011). Justification for this orientation is found by returning to the discussion of wisdom that is provided by Baltes (2004). Recall that he identified wisdom, in part, as the ability to orchestrate knowledge and a range of virtues. As Lundberg (2010) points out, one of the primary goals of every major faith tradition in the world is to transmit a number of virtues including, humility, compassion, gratitude, and altruism. A key issue that arises at this juncture has to do with identifying the precise ways in which these virtues are transmitted in religious settings. A central premise in the work that follows is that the virtues that comprise practical wisdom are transmitted socially in the church. This premise is supported by the observations of Staudinger and Gluck (2011), who maintain that “the importance and facilitative effect of a ‘wisdom mentor’ can be found in almost all approaches to wisdom, be they ancient or contemporaneous, religious or scientific” (p. 233). Consistent with these insights, we assess the potentially important role that is played by informal spiritual support that is provided by fellow church members. Krause (2008) defines spiritual support as assistance that is provided by fellow church members for the explicit purpose of encouraging support recipients to apply religious teachings and principles in daily life.
We are not the first to examine the relationship between religious involvement and wisdom. However, the research that has been done so far provides conflicting findings. For example, Le (2008) reports religious involvement is associated with wisdom, but Brezina and van Oudenhoven (2012) were unable to find a significant relationship between the two. These conflicting findings can be attributed to the way religion was measured in these studies. Brezina and van Oudenhoven (2012) rely solely on a measure of religious preference. In contrast, the significant findings reported by Le (2008) involve institutional measures of religion (e.g., attendance at worship services) and private religious practices (e.g., private prayer or mediation). Measures of religious preference, church attendance, and private prayer fall short because they do not provide an intuitively pleasing sense of how involvement in religion may make people wise.
A different set of problems arises with studies that were designed to assess the relationship between wisdom and health-related outcomes. So far, most of this research has been concerned with psychological well-being (e.g., Ardelt, 1997; Wink & Dillon, 2003), while fewer researchers have examined the relationship between wisdom and physical health status (Ardelt, 2000, Ardelt, 2003). Moreover, problems with studies that assess wisdom and physical health outcomes make it difficult to reach firm conclusions. Some investigators report that wisdom is associated with self-rated health as well as the number of acute and chronic health conditions that are experienced by study participants (Judge, Ilies, & Dimotakis, 2010). However, these researchers rely solely on a measure of cognitive ability to assess wisdom. As Baltes (2004) points out, this measurement strategy does not adequately reflect the complex nature of this core virtue. In contrast, other researchers assess the relationship between religious involvement and health with more widely used measures of wisdom, but these investigators have not been able to observe a statistically significant relationship between wisdom and health (Proctor, Maltby, & Linley, 2011).
In the research that follows, we develop and test a conceptual model that anchors the genesis of wisdom in social relationships that arise in the church (i.e., spiritual support) and proposes that wisdom may, in turn, be associated with better self-rated health. In the process, we flesh out the theoretical underpinnings of these relationships by bringing additional constructs to the foreground.
Religious Involvement, Wisdom, and Self-Rated Health
The conceptual model we developed to examine the relationships among religious involvement, wisdom, and health is presented in Figure 1. Two steps were taken to simplify the presentation of this theoretical scheme. First, the elements of the measurement model (i.e., the factor loadings and measurement error terms) are not shown in this diagram even though a full measurement model was estimated when this conceptual scheme was evaluated empirically. Second, the model in Figure 1 was estimated after the effects of age, sex, education, marital status, and race were controlled statistically (i.e., were treated as exogenous variables).

A conceptual model of religious involvement, practical wisdom, and self-rated health.
Although a number of relationships are embedded in our study model, the following core theoretical linkages capture the overall theoretical thrust of this conceptual scheme: (1) people who go to church more often will receive more spiritual support from fellow church members, (2) individual who get more spiritual support at church will have greater wisdom, (3) greater wisdom is associated with a stronger sense of hope, and (4) people who are more hopeful will be more likely to rate their health in a favorable manner. The theoretical rationale for these relationships is provided below.
Church Attendance and Spiritual Support
There are two reasons why church attendance serves as the point of departure in our model. First, attendance at worship services is an important conduit for the transmission of religious beliefs and principles (i.e., virtues) that form the backbone of wisdom. Fundamental religious tenets and virtues are embedded in the sermons, hymns, and congregational prayers that are part of the typical worship service. This is one reason why Stark and Finke (2000) propose that “confidence in religious explanations increases to the extent that people participate in religious rituals” (p. 107).
Second, as Krause (2008) argues, religious principles are also transmitted and reinforced informally through spiritual support that is exchanged among church members. But in order for an individual to receive spiritual support, they must obviously come into contact with potential support providers. Attendance at worship services provides an opportunity for this type of contact to take place. However, it is unlikely that spiritual support will be exchanged simply because two individuals come into contact with each other at church. Instead, spiritual support is more likely to be provided when two people have a longer history of coming into contact with each other because developing a sound relationship history may be especially important for the successful delivery of this type of support. As McFadden, Knepple, and Armstrong (2003) point out, discussing personal spiritual matters can be a sensitive issue and as a result, a person may feel put-off or resentful if someone they do not know well attempts to discuss spiritual issues with them. As these insights reveal, spiritual support is more likely to successfully take root when both the provider and the recipient feel comfortable in the relationship they have developed. Repeated interaction through regular church attendance helps foster this type of relationship. It is for this reason that we predict in Figure 1 that more frequent church attendance will be associated with receiving more spiritual support.
Spiritual Support and Wisdom
Sociologists and psychologists have been arguing for over 100 years that religion is, at its base, a social phenomenon (e.g., Simmel, 1898/1997). One important element of this argument involves the way in which religious principles are socially transmitted. This issue is forcefully argued in Berger’s (1967) classic sociological theory of religion. He maintains that religious worlds “ . . . are socially constructed and socially maintained. Their continuing reality, both objective . . . and subjective . . . depends upon specific social processes, namely those processes that ongoingly reconstruct and maintain the particular worlds in question” (Berger, 1967, p. 45). These insights make it possible to develop the following four-part argument. First, as we argued earlier, the fundamental precepts of the major faith traditions consist of a number of core virtues (Lundberg, 2010). Second, practical wisdom has to do with the implementation of these virtues in daily life (Schwartz & Sharpe, 2006). Third, religious beliefs and precepts are developed and maintained socially (Berger, 1967). Fourth, by definition, informal spiritual support is a major venue for the transmission of religious beliefs and virtues (Krause, 2008). Based on this reasoning, it is hypothesized in Figure 1 that individuals who receive more spiritual support from fellow church members will have greater practical wisdom.
Wisdom and Hope
As Baltes (2004) points out, people who are wise have acquired a set of skills that help them navigate the vicissitudes of life by making sound judgments and giving good advice that enhances their own well-being as well as the well-being of others. If a person possesses this type of knowledge, skill, and virtue, then they should be more hopeful about future because they are likely to feel that no matter what life may bring, they will do what is right, good, and justifiable. Evidence that wisdom is associated with hope is provided in a recent study by Moraitou and Efklides (2012).
Hope and Health
A well-developed body of research that was primarily conducted in secular settings suggests that greater hope and optimism are associated with better health. For example, Peterson, Seligman, and Vaillant (1988) examined the effect of optimism on health over a 35-year period. They found that people who were more optimistic at the baseline survey enjoyed better health over time. Similar results have emerged from studies that were conducted in religious settings. For example, Idler and Kasl (1997) report that the older people who go to church more often tend to be more optimistic, and older adults who are more optimistic have fewer problems with physical functioning over time. There are a number of reasons why older people who are more hopeful are likely to be healthier. For example, a sense of hope promotes positive emotions that are likely to reduce the risk of developing mental health problems (Nunn, 1996) that may, in turn, influence physical health (Cohen & Rodriguez, 1995). In addition, as Giltay, Geleijnse, Zitman, Buijsse, and Kromhout (2007) point out, older adults who are more hopeful tend to adopt healthier lifestyles and better dietary habits over time. And there is some evidence that greater hope and optimism are associated with a range of biological markers of health including better immune functioning (Forgeard & Seligman, 2012), more serum antioxidants (Boehm, Williams, Rimm, Ryff, & Kublansky, 2013), and less inflammation of the arteries (Roy et al., 2010).
Aging and Wisdom
As the data for our study were provided by middle-aged and older adults, it is important to reflect on the ways in which aging may be related to the relationships we assess. However, it should be emphasized at the outset that we cannot evaluate this issue conclusively. Even so, it is helpful to take a preliminary look at this issue.
There are two ways in which aging may potentially be involved in the relationships among the variables in our study model. The first has to do with the relationship between aging and wisdom. Staudinger and Gluck (2011) report that a number of studies suggest that many people believe wisdom increases with age. These beliefs appear to be based on the notion that individuals who are older are wiser because they have greater experience with the ups and downs of life. However, Staudinger and Gluck (2011) go on to point out that empirical studies on the relationship between age and wisdom typically do not support the view that wisdom increases with age. As we report below, the data for our study were provided by a nationwide survey of people age 50 and older. Although these data do not allow us to examine differences in wisdom across the entire life course, the nearly half century age span in our sample (i.e., ages 50-95) makes it possible to take a preliminary look at this issue.
The second way in which aging may influence the relationships among the variables in our study model may be found by turning to the interface among aging, religious involvement, and wisdom. A considerable number of studies suggest that people who are presently older are more deeply involved in religion than individuals who are currently younger (see Krause, 2008, for a review of this research). If involvement in religion (i.e., church attendance and spiritual support) is associated with wisdom as we proposed earlier, and older people are more deeply involved in religion, then perhaps the relationship between religion and wisdom is stronger among people who are in late-life. Although this relationship cannot be evaluated with the data from the present study, it represents an important issue to examine in the future.
Method
Sample
The data for this study come from an ongoing nationwide survey of Whites and African Americans. Altogether, five waves of interviews have been conducted. The study population for the baseline survey was defined as all household residents who self-identified as either Black or White, were non-institutionalized, English-speaking, and at least 66 years of age. Geographically, the study population was restricted to all eligible persons residing in the coterminous United States (i.e., residents of Alaska and Hawaii were excluded). Finally, the study population was restricted to currently practicing Christians, individuals who were Christian in the past but no longer practice any religion, and people who were not affiliated with any faith at any point in their lifetime. This study was designed to explore a range of issues involving religion. As a result, individuals who practice a faith other than Christianity were excluded because it would be too difficult to devise a comprehensive battery of religion measures that would be suitable for individuals of all faiths.
The sampling frame consisted of all eligible persons contained in the beneficiary list maintained by the Centers for Medicare and Medicaid Services (CMS). A five-step process was used to draw the sample from the CMS Files (see Krause, 2002a, for a detailed discussion of these steps).
The baseline survey took place in 2001. The data collection for all waves of interviews was conducted by Harris Interactive (New York). A total of 1,500 interviews were completed, face-to-face, in the homes of the study participants. African Americans were over-sampled so that sufficient statistical power would be available to assess racial cultural differences in religion. The overall response rate for the baseline survey was 62%. Sampling information for Waves 2 to 4 is as follows: Wave 2 (2004), n = 1,024, (re-interview rate = 80%); Wave 3 (2007), n = 969, (re-interview rate = 75%); Wave 4 (2008), n = 718 (re-interview rate = 88%).
A fifth wave of interviews was completed in June, 2013. However, the sampling strategy for this round of interviews was complex. By the time the Wave 5 interviews were conducted, only 229 study participants were re-interviewed successfully. Many former study participants experienced significant health problems that were associated with their advanced age (M = 83.2 years). Moreover, a number of former study participants died (n = 611). So in order to have sufficient statistical power to conduct meaningful analyses, the following two-part sampling strategy was employed. First, we re-interviewed as many of the original study participants as possible (n = 229). The re-interview rate for people who had participated in the study previously was 63%. Second, this group was supplemented with a new sample of individuals who had not participated in the study previously (n = 1,306). In the process of fielding the sample of new study participants, we lowered the age for eligibility from 66 to 50. This was done to make it possible to evaluate issues involving religious involvement in midlife, which is not the focus of the current study. The re-interview rate for prior study participants was 63%. The response rate for people in the new supplementary sample was 45%.
The sample of individuals who had not participated previously in the study was obtained in the following manner. Based on data in the 2010 Census, 50 geographic areas (i.e., Census tracts) were selected to proportionately represent the population aged 50 and above who were either White or African American. All households within each Census tract were enumerated. One eligible person within each household was selected at random to participate in the study. The response rate for the individuals who had not participated in the study previously was 45%.
Altogether, a total of 1,535 individuals participated in the Wave 5 interviews. The analyses presented below are based on the Wave 5 data only because this was the first time that questions on wisdom were administered. Recall that belonging in a congregation and spiritual support figure prominently in our conceptual model. When the questionnaire for this study was being developed, the members of the research team felt it did not make sense to ask questions about belonging in a congregation or receiving spiritual support from fellow church members if study participants either never attend worship services or if they go to church only one or two times a year. Consequently, 381 individuals with low levels of church attendance were excluded from the analyses presented below, resulting in a sample size of 1,154. The full information maximum likelihood (FIML) procedure was used to deal with item non-response in the data (Enders, 2010).
Preliminary analysis revealed that the average age of the participants in the pooled study sample was 63.4 years (SD = 11.7 years), 35.9% were men, 43.0% were married at the time of the Wave 5 survey, 61.0% self-identified as White, and the average level of educational attainment was 13.1 years of schooling (SD = 2.3 years).
Measures
Table 1 contains the indicators that were used to assess the core constructs in Figure 1. The procedures that were used to code these items are provided in the notes of this table. Estimates of the reliability of the multiple-item measures will be presented later in this report after information on the measurement model has been provided.
Core Study Measures.
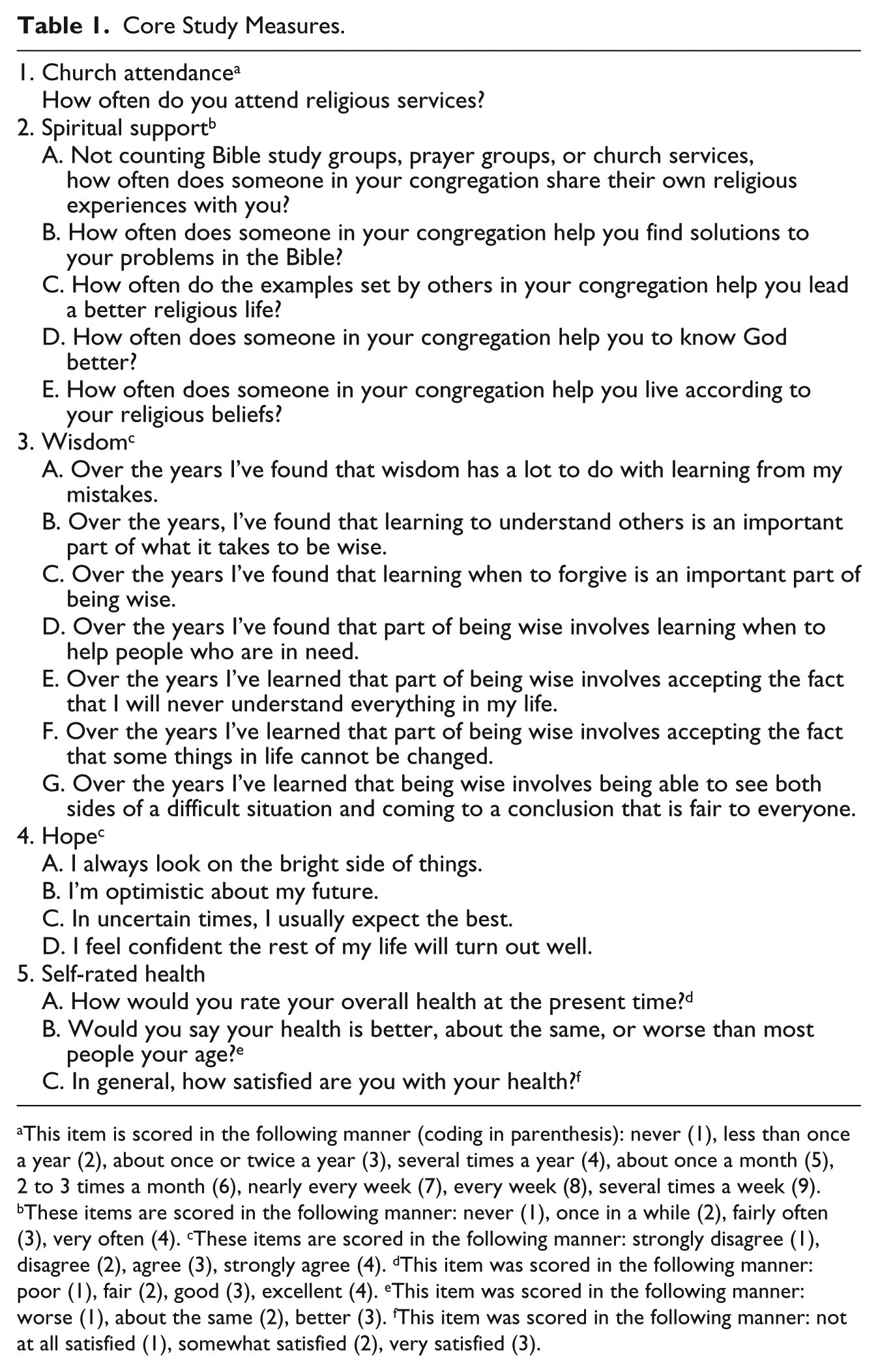
This item is scored in the following manner (coding in parenthesis): never (1), less than once a year (2), about once or twice a year (3), several times a year (4), about once a month (5), 2 to 3 times a month (6), nearly every week (7), every week (8), several times a week (9). bThese items are scored in the following manner: never (1), once in a while (2), fairly often (3), very often (4). cThese items are scored in the following manner: strongly disagree (1), disagree (2), agree (3), strongly agree (4). dThis item was scored in the following manner: poor (1), fair (2), good (3), excellent (4). eThis item was scored in the following manner: worse (1), about the same (2), better (3). fThis item was scored in the following manner: not at all satisfied (1), somewhat satisfied (2), very satisfied (3).
Church attendance
A single item was used to assess how often study participants attend worship services. A high score denotes more frequent church attendance. The mean of this ordinal measure is 6.7 (SD = 1.7). Scores on the church attendance measure ranged from 4 to 9.
Spiritual support
Five indicators that were developed by Krause (2002b) were used to assess spiritual support. A high score stands for study participants who received spiritual support more often. The mean spiritual support value is 13.0 (SD = 4.2).
Practical wisdom
Seven items were developed especially for this study to assess practical wisdom. Based on the procedures described by Krause (2002b), the following item development strategy was devised to create these measures. First, 41 open-ended in-depth interviews were conducted to see how the typical individual thinks about practical wisdom. Following this, the main themes that were extracted from these interviews were used to craft closed-ended items. Once a preliminary set of measures were in place, 40 cognitive interviews were conducted with a new sample of study participants. Cognitive interviews involve presenting respondents with newly developed closed-ended items followed by a series of open-ended probes. The probes are designed to determine if the item is understood in the intended manner and if there are better ways to phrase the question stems. Following this, the indicators were revised and evaluated with standard pilot testing procedures.
A high score on the practical wisdom indicators means that a person is more wise. The mean is 24.7 (SD = 3.0).
Hope
Hope was assessed with four measures. The first two come from the scale that was developed by Scheier and Carver (1985). The other two items were developed by Krause (2002b). A high score represents more hopeful study participants. The mean is 12.9 (SD = 2.0).
Self-rated health
Three items that are used widely in the literature were included in the interview schedule to assess self-rated health. A high score indicates a more favorable self-assessment of health. The mean is 7.2 (SD = 1.6).
Demographic control variables
Recall that the relationships among the constructs in Figure 1 were estimated after the effects of age, sex, education, marital status, and race were controlled statistically. Age and education were coded continuously in years. In contrast, sex (1 = men; 0 = women), race (1 = White; 0 = Black), and marital status (1 = presently married; 0 = otherwise) were scored in a binary format. Sex was determined by interviewer observation and race was based on self-identification.
Results
Model Estimation Issues
The model depicted in Figure 1 was evaluated with the maximum likelihood estimator in Version 8.80 of the LISREL statistical software program (du Toit & du Toit, 2001). Use of this estimator is based on the assumption that the observed indicators have a multivariate normal distribution. Preliminary tests (not shown here) revealed that this assumption had been violated in the current study. Although there are a number of ways to deal with departures from multivariate normality, the straightforward approach that is discussed by du Toit and du Toit (2001) was followed here. These investigators report that departures from multivariate normality can be handled by converting raw scores of the observed indicators to normal scores prior to estimating the model (du Toit & du Toit 2001, see p.143). Based on these insights, the analyses presented below were performed with observed indicators that were normalized.
Because the FIML procedure was used to deal with item non-response, the LISREL software program only provides two goodness-of-fit measures. The first is the FIML chi-square value (559.594 with 236 degrees of freedom, p < .001). Unfortunately, this statistic substantially underestimates the fit of the model to the data when samples are large, such as the sample in the current study. A better sense of the fit of the model to the data is provided by the second goodness-of-fit measure—the root mean square error of approximation (RMSEA). The RMSEA value for the model in Figure 1 is .035. As Kelloway (1998) suggests, values below .050 indicate a very good fit of the model to the data.
Reliability of the Observed Indicators
The factor loadings and measurement error terms that were derived from estimating a study model are important because they provide preliminary information about the reliability of the multiple-item measures. Widaman (2012) suggests that items with standardized factor loadings in excess of .600 tend to have good reliability. The standardized factor loadings in the current study range from .620 to .845, suggesting that the reliability of the multiple-item constructs is acceptable.
Although the factor loadings that are associated with the observed indicators provide useful information about the reliability of each item, it would be helpful to know something about the reliability for the scales as a whole. It is possible to compute these reliability estimates with a formula provided by DeShon (1998). This procedure is based on the factor loadings and measurement error terms. Applying the procedures described by DeShon (1998) to these data yield the following reliability estimates for the multiple-item constructs in Figure 1: spiritual support (.904), wisdom (.911), hope (.863), and self-rated health (.757). Taken as a whole, the data provided in this section suggest that the reliability of the multiple-item study measures is good.
Substantive Findings
The bivariate correlations among the latent constructs are provided in Table 2. The substantive findings that were derived from estimating the study model are provided in Table 3. Taken as a whole, the data in Table 3 provide support for the hypotheses that were developed earlier. More specifically, the results reveal that individuals who go to church more often report receiving more spiritual support from fellow church members (β = .276; p < .001). The findings further indicate that people who receive more spiritual support have greater wisdom (β = .283; p < .001). The results indicate that study participants who are wise also tend to be more hopeful (β = .384; p < .001). And people who are more hopeful are, in turn, more likely to rate their health in a favorable way (β = .328; p < .001).
Bivariate Correlations Among the Latent Study Variables.

The Relationships Among Religious Involvement, Wisdom, and Health (N = 1,154).
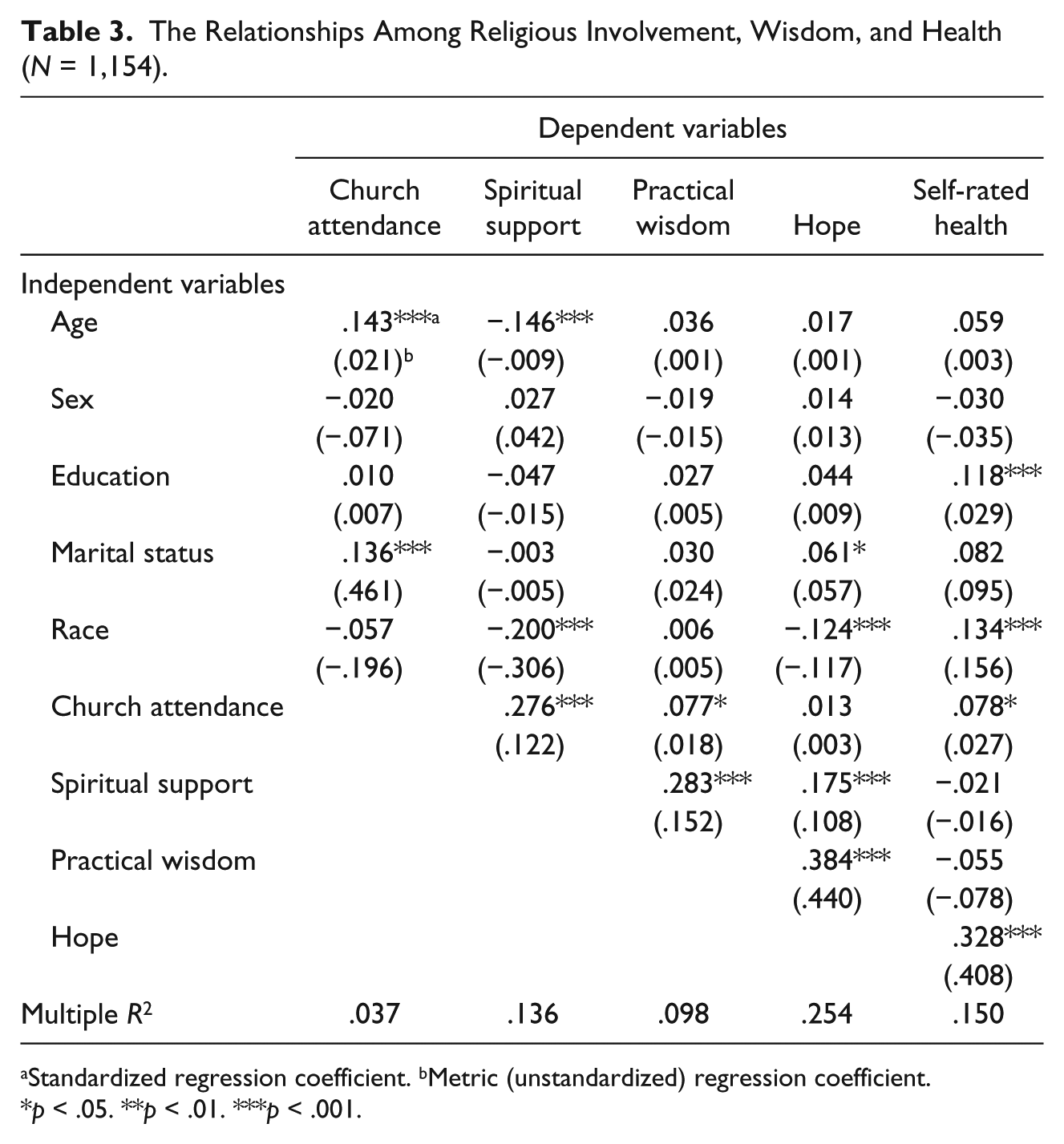
Standardized regression coefficient. bMetric (unstandardized) regression coefficient.
p < .05. **p < .01. ***p < .001.
The findings in Table 3 can be cast in a wider context. More specifically, the fact that wisdom is associated with spiritual support and hope in theoretically meaningful ways provides some evidence of the construct validity of the new wisdom measure.
The data in Table 3 are important, but they only reflect the direct effects of the study measures. Assessing the indirect and total effects that operate through the study model add greater depth to the study findings. An indirect effect means, for example, that more frequent church attendance is associated with more spiritual support and more spiritual support is, in turn, associated with better health. Adding this indirect effect to the direct effect in Table 3 provides a total effect which depicts the relationship between church attendance and health from a wider vantage point.
Two sets of direct, indirect, and total effects will be reviewed here to round out the role that practical wisdom plays in the study model. The first set has to do with the relationship between church attendance and wisdom. The direct effect that is shown in Table 3 suggests that more frequent church attendance is only weakly associated with greater wisdom (β = .077; p < .05). But a different picture emerges when the indirect effects of church attendance on wisdom that operate through spiritual support and belonging are taken into account (β = .078; p < .001; not shown in Table 3). Summing the direct and indirect effects suggests that the relationship between attending worship services and wisdom is stronger than it appears initially (total effect = .077 + .078 = .155; p < .001; not shown in Table 3). Put in a more substantive way, this means that going to worship services is associated with greater wisdom, in part, because people who go to church more often receive more spiritual support from fellow church members and they are more likely to feel they belong in the place where they worship.
The second set of direct, indirect, and total effects has to do with the relationship between wisdom and health. At first, the direct effect in Table 3 appears to indicate that wisdom is not significantly related to health (β = –.055; p < .001). But the indirect effect that operates through hope provides a different view (β = .126; p < .001; not shown in Table 3). This indirect effect indicates that people who are wise tend to rate their health in a more favorable manner primarily because they are more hopeful about the future. Moreover, the fact that the total effect of wisdom on health is not significant (β = .071; ns) suggests that hope may be the primary mechanism that links greater wisdom with better health.
Earlier, we briefly discussed research on age differences in wisdom. As the data in Table 3 reveal, we were unable to find a statistically significant direct effect of age on wisdom in our data (β = .036; ns). Further analyses (not shown in Table 3) suggest that the indirect effects of age on wisdom that operate through the study model are not statistically significant (β = –.019; ns). Therefore, the findings suggest that, within the age range in our sample, wisdom does not appear to vary by age.
Discussion
In their exhaustive review of the literature, Hood, Hill, and Spilka (2009) report that wisdom is explicitly described as a virtue in many faith traditions around the world. However, these researchers go on to point out that “little or no research” has investigated the relationship between any dimension of religiousness and wisdom (Hood et al., 2009, p. 429). The purpose of the current study was to address this gap in the literature. In an effort to obtain better insight into how religion might make people wise, we developed a conceptual model that placed an emphasis on the social aspects of congregational life. Findings from a nationwide survey provide support for the following line of reasoning: people who go to church more often get more spiritual support from the individuals who worship there, more spiritual support is associated with a greater sense of belonging in a congregation, and a greater sense of belonging appears to foster greater wisdom. In addition to studying how wisdom might arise, an effort was made to extend research on wisdom by seeing whether it is associated with better health in late and midlife. The data further reveal that wisdom is associated with better health and this relationship arises primarily because people who are wise are also more hopeful about the future.
Consistent with findings from other studies, we found little evidence that wisdom is associated with increased age. However, this conclusion must be viewed cautiously because of the restricted age range in our sample.
Although the findings from our work provide some potentially useful insights, a considerable amount of research on wisdom remains to be done. Three areas appear to be ripe for further investigation. First, we argued above that spiritual support was a primary conduit for the transmission of virtues that form the basis of wisdom. However, other virtues were not assessed empirically in our study model. Research is needed to see if fellow church members play a role in promoting virtues and if they do, we need to know which virtues they encourage. Second, it would also be helpful to examine the relationship between wisdom and other measures of physical health including functional disability as well as specific and acute health conditions. Third, research is needed to see if there are potential subgroup variations in the model we developed. For example, it would be important to see if the relationship between spiritual support and wisdom is different for older women and older men.
In the process of examining other issues in the study of wisdom, researchers should also address the limitations in our work. Three shortcomings are in need of attention. First, the data for this study were gathered at a single point in time and as a result, the temporal ordering among the constructs in our study model was based on theoretical considerations alone. Consequently, other researchers may legitimately propose other causal orderings among our study constructs. For example, alternative causal orderings could be proposed for the relationships between church attendance and health, hope and health, and spiritual support and wisdom. Clearly, this issue must be rigorously addressed with data that have been gathered at more than one point in time. Second, it is not possible to tell if the findings from this study generalize to individuals in other racial or ethnic groups (e.g., Latinos) or to people with faith traditions other than Christianity. Third, most of the constructs in our study model are assessed with ordinal measures. The model was then assessed with the maximum likelihood (ML) estimator. However, there is some debate in the literature about whether other estimators, such as weighted least squares (WLS), should be used under these circumstances (e.g., Olsson, Foss, Troye, & Howell, 2000). Consequently, researchers may wish to estimate models such as ours with the WLS estimator.
Research reviewed by Baltes (2004) suggests that written documents on wisdom date back to the third millennium before Christ. He goes on to report that every major civilization since that time has devoted considerable thought to wisdom. Baltes (2004) concludes his overview on the history of wisdom by noting that “ . . . each civilization, when it has reached a certain level of development, is bound to generate a literature about the problem of wisdom and wisdom-related knowledge and skills” (p. 44). We hope the issues we have raised and the findings we provide encourage other researchers to join us in the pursuit of issues that are as old as civilization itself yet still speak to the pragmatic concerns (i.e., health) of people as they grow older.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by grants from the John Templeton Foundation (Grant Number 20887) and the National Institute on Aging (RO1 AG014749).