
Abstract
Although the elimination of health disparities and the prevention of disability in late life are top public health priorities (Committee on Understanding and Eliminating Racial and Ethnic Disparities in Health Care, 2002; U.S. Department of Health and Human Services, 1991), little progress has been achieved as Black older adults consistently exhibit higher rates of disability than White older adults (D. O. Clark & Maddox, 1992; Committee on Understanding and Eliminating Racial and Ethnic Disparities in Health Care, 2002; Coppin et al., 2006; Kelley-Moore & Ferraro, 2004; Kington & Smith, 1997; Koster et al., 2005; Mendes de Leon, Barnes, Bienias, Skarupski, & Evans, 2005; Schoeni, Martin, Andreski, & Freedman, 2005; Thorpe, Bell, LaVeist, & Simonsick, 2009; Thorpe, Kasper, et al., 2008; Thorpe et al., 2012). A number of explanations such as socioeconomic status (SES), health behaviors, and health status have been tested; yet, racial differences in disability persist. Because of the expected growth in the aging population, which includes a substantial increase in minorities and decrease in the number of Whites by 2050 (Federal Interagency Forum on Aging-Related Statistics, 2008), elucidating factors that underlie the racial-related inequalities in disability is paramount.
Efforts to improve the understanding of racial disparities in disability are limited by two issues. First, race and SES are inextricably linked with Blacks having considerably fewer socioeconomic resources than Whites (Braveman et al., 2005; LaVeist, 2005; Thorpe, Brandon, & LaVeist, 2008; Williams & Collins, 1995). Because of this strong relationship between race and SES, the ability to determine how race and SES operate to produce disparities in disability is complicated (LaVeist, Pollack et al., 2011; LaVeist et al., 2008). Typically to address race and SES confounding, a multivariate approach is used whereby SES is included in the regression model. This is a well-recognized approach; however, it may not always be sufficient (see LaVeist, Thorpe, Mance, & Jackson, 2007, for details).
The second problem in understanding racial disparities in disability is the confounding between race and residential segregation. The United States is very racially segregated; as a result, African Americans and Whites generally live in separate communities, where they have different social and environmental risk exposures. According to segregation theories such as Risk Exposure Theory and Resource Deprivation Theory (LaVeist, 2005), minority communities have social and environmental risks typically characterized by high crime (Lee, 2000) and poor housing (Black & Macinko, 2008; Williams & Collins, 2001), and are less likely to have as many health-promoting resources as White communities (Gaskin, Dinwiddie, Chan, & McCleary, 2012a, 2012b). This differential exposure to neighborhood stressors can contribute to a person’s ability to perform certain social roles and tasks. Specifically, neighborhoods that contain fewer healthy food choices, parks, sidewalks, recreational spaces, and medical facilities may negatively affect the adoption of health-promoting behaviors that can impede the progression or delay the onset of disability.
Prior work examining race and disability has largely focused on individual measures such as SES (D. O. Clark, 1993; D. O. Clark & Maddox, 1992; Coppin et al., 2006; Koster et al., 2005; Liao, McGee, Cao, & Cooper, 1999; Peek, Coward, Henretta, Duncan, & Dougherty, 1997; Schoenbaum & Waidmann, 1997; Thorpe, Bowie, Wilson-Frederick, Coa, & LaVeist, 2013; Thorpe, Brandon, & LaVeist, 2008; Thorpe et al., 2012; White-Means & Hammond, 1993) or health-related factors (Kelley-Moore & Ferraro, 2004; Kington & Smith, 1997; Koster et al., 2007; Mendes de Leon, 1997). However, other investigators have sought to understand the interrelationships among key individual factors such as sex, SES, and disability (Johnson & Wolinsky, 1994; Mendes de Leon et al., 2005; Thorpe, Szanton, Bell, & Whitfield, 2013; Wray & Blaum, 2001) Findings from all of these studies highlight the importance of disentangling key confounders such as sex, SES, and health factors to advance our understanding of race differences in disability.
In addition to individual-level factors, there is a growing body of literature that focuses on the association between neighborhood factors and disability (Balfour & Kaplan, 2002; Beard et al., 2009; C. R. Clark et al., 2009; Freedman, Grafova, Schoeni, & Rogowski, 2008; Glass & Balfour, 2003; Lang, Llewellyn, Langa, Wallace, & Melzer, 2008; Nordstrom et al., 2007; Pruchno, Wilson-Genderson, & Cartwright, 2012; White et al., 2010). These studies have consistently demonstrated that neighborhood indicators, including social vulnerability, wealth, violence, presence of physicians, traffic, trash, and litter, are related to disability in older adults. Also, studies assessing the impact of where one resides on race disparities in disability have found that geographic area affect disability (Lin, 2000). However, we are unaware of any study that has sought to determine whether social and environmental conditions contribute to racial differences in disability.
Accounting for social context in health disparities research has demonstrated a substantial reduction or lack of racial differences in health outcomes, such as hypertension (Thorpe, Kasper, et al., 2008), obesity (Bleich, Thorpe, Sharif-Harris, Fesahazion, & LaVeist, 2010), health services use (Gaskin, Price, Brandon, & LaVeist, 2009), and diabetes (LaVeist, Thorpe, Galarraga, Bower, & Gary-Webb, 2009) in a racially integrated community without racial differences in income. This evidence suggests that social context is an important, yet understudied, determinant of health (LaVeist, Pollack et al., 2011; LaVeist et al., 2007; Williams & Collins, 2001). However, the extent to which racial disparities in disability are manifestations of differential social contexts rather than race is largely unknown. Furthermore, data sources available to disentangle race, SES, and segregation simultaneously are sparse. Thus, the purpose of this study was to examine racial disparities in disability within a sample of White and African American community-dwelling older adults living in the same social context with similar socioeconomic resources.
Method
Study Population
Exploring Health Disparities in Integrated Communities (EHDIC) is an ongoing multisite study of racial disparities within communities, where African Americans and Whites live together and where there are no racial differences in SES, as measured by median income. This analysis is based on data from the first EHDIC study site in Southwest Baltimore, Maryland (EHDIC-SWB), a low-income urban area.
EHDIC-SWB was a cross-sectional face-to-face survey of the adult population (aged 18 and older) of two contiguous census tracts collected between June and September 2003. In addition to being economically homogeneous, the study site was also racially balanced and well integrated, with almost equal proportions of African American and White residents. In the two census tracts, the racial distribution was 51% African American and 44% White, and the median income for the study area, which was US$24,002, did not differ by race. The census tracts were block listed to identify every occupied dwelling in the study area. During block listing, 2,618 structures were identified. Of those, 1,636 structures were determined to be occupied residential housing units (excluding commercial and vacant residential structures). At most, five attempts were made to contact an eligible adult in 1,244 occupied residential housing units. A total of 65.8% of the occupied housing units were enrolled in the study. This resulted in 1,489 study participants (41.9% of the 3,555 adults living in these two census tracts recorded in the 2000 Census). Because our survey had similar coverage across each census block group, including the study area, the bias to geographic locale and its relationship with SES should be minimal (LaVeist et al., 2008).
Comparisons with the 2000 Census for the study area indicated that the EHDIC-SWB sample included a higher proportion of African Americans and women, but was otherwise similar on other demographic and socioeconomic indicators (LaVeist et al., 2008). Specifically, our sample was 59.3% African American and 44.4% male, whereas the 2000 Census data showed the population was 51% African American and 49.7% male. Age distributions in our sample and the 2000 Census data were similar with a median age range of 35 to 44 years for both samples. The lack of racial difference in median income in the Census, US$23,500 (African American) versus US$24,100 (White), was replicated in EHDIC-SWB, $23,400 (African American) versus $24,900 (White).
The survey was administered in person by a trained interviewer and consisted of a structured questionnaire that included demographic and socioeconomic information, self-reported height and weight, self-reported health behaviors and chronic conditions, and three blood pressure (BP) measurements. The EHDIC study has been described in greater detail elsewhere (LaVeist et al., 2008). The Committee on Human Subjects Research at the Johns Hopkins Bloomberg School of Public Health approved the study. These analyses are based on the 347 African American and White adults ages 50 years and older in the EHDIC-SWB sample.
Measures
The outcome variable, disability, was based on questions that asked participants to report their level of difficulty in performing instrumental activities of daily living (IADL). This included using the telephone, preparing their own meals, doing housework, getting to places outside of walking distance, shopping for groceries, taking their own medicine, and handling their own money (Fillenbaum, 1988; Hogan, Ebly, & Fung, 1999; McDowell & Newell, 1987; Lawton & Broday, 1969). A binary variable was created for each IADL to indicate whether the individual had difficulty in performing that specific task or not. The four responses included the following: (a) have difficulty but can do without help, (b) have difficulty and need some help, (c) never do the task, and (d) unable to do the task. After summing these binary variables, a dichotomous variable for disability was created to identify those individuals who had difficulty in a least one IADL. This approach is similar to the approach of other investigators (Freedman, Martin, Schoeni, & Cornman, 2008; Thorpe, Clay, Szanton, Allaire, & Whitfield, 2011; Volpato et al., 2002).
Race was based on participant self-identification as African American or White. Demographic variables included age (years), sex (1 = male, 0 = female), education level (less than high school graduate, high school graduate/General Educational Development [GED], more than high school graduate), marital status (1 = married, 0 = not married), and household income (continuous).
Health-related characteristics included health insurance (1 = yes, 0 = no), current smoker (1 = yes, 0 = no), current drinker (1 = yes, 0 = no), weight status, and chronic conditions. Using self-reported height and weight, body mass index (BMI) was calculated by dividing weight in kilograms by height in meters squared (kg/m2). Weight status consisted of three categories. Participants whose BMI was between 18 and 24 kg/m2 were considered to be normal weight, those with BMI between 25 and 29 kg/m2 were considered to be overweight, and those with BMI ≥ 30 kg/m2 were considered to be obese. Chronic conditions included heart attack, hypertension, stroke, diabetes, asthma, cancer, and depressive symptoms. Participants reported whether they received a physician diagnosis of heart attack, hypertension, stroke, diabetes, asthma, and cancer. Depressive symptoms were based on the Patient Health Questionnaire (PHQ) depression module (Spitzer, Kroenke, & Williams, 1999). Those who answered “more than half the days” or “nearly every day” on four or more of the questions (including at least one of the two following questions: “little interest or pleasure in doing things” or “feeling down, depressed, or hopeless”) were classified as having depressive syndrome. Each of the conditions was coded as binary variables (1 = condition present, 0 = condition absent) and summed to create a variable representing the number of chronic conditions. A dichotomous variable was created to classify participants who reported two or more chronic conditions relative to those who reported none or one chronic condition.
Statistical Analyses
The Student’s t and chi-square tests were used to assess the mean and proportional differences between African American and White adults for demographic and health-related factors by sex. Because there are sex differences in reporting of disability (Beckett et al., 1996; Guralnik et al., 1994; Newman & Brach, 2001), all analyses were stratified by sex. Multivariable logistic regression models were specified to examine the association between disability and race adjusting for age, marital status, income, education, insurance status, weight status, drinking and smoking status, and two or more chronic conditions. These variables have been found to be associated with race and/or disability in previous work (Balfour & Kaplan, 2002; Beard et al., 2009; C. R. Clark et al., 2009; Freedman, Grafova, et al., 2008; Glass & Balfour, 2003; Kelley-Moore & Ferraro, 2004; Kington & Smith, 1997; Koster et al., 2005; Koster et al., 2009; Lang et al., 2008; Mendes de Leon, 1997; Nordstrom et al., 2007; Pruchno et al., 2012; Thorpe, Brandon, & LaVeist, 2008; Thorpe et al., 2012; Thorpe, Szanton, Bell, and Whitfield, 2013; White et al., 2010). Probability values (p < .05) were considered statistically significant, and all tests were two-sided. Analyses were conducted using STATA software, Version 10 (Stata, Inc., College Station, Texas).
Results
The distribution of the demographic and health-related characteristics for women by race is shown in Table 1. African American women were on average younger and less likely to report disability than White women. There were no racial differences observed with respect to being married, income, education level, health insurance status, weight status, being a current smoker or drinker, or two or more health conditions.
Distribution of Demographic and Health-Related Characteristics by Race for Women in the Exploring Health Disparities in Integrated Communities–Southwest Baltimore Study.
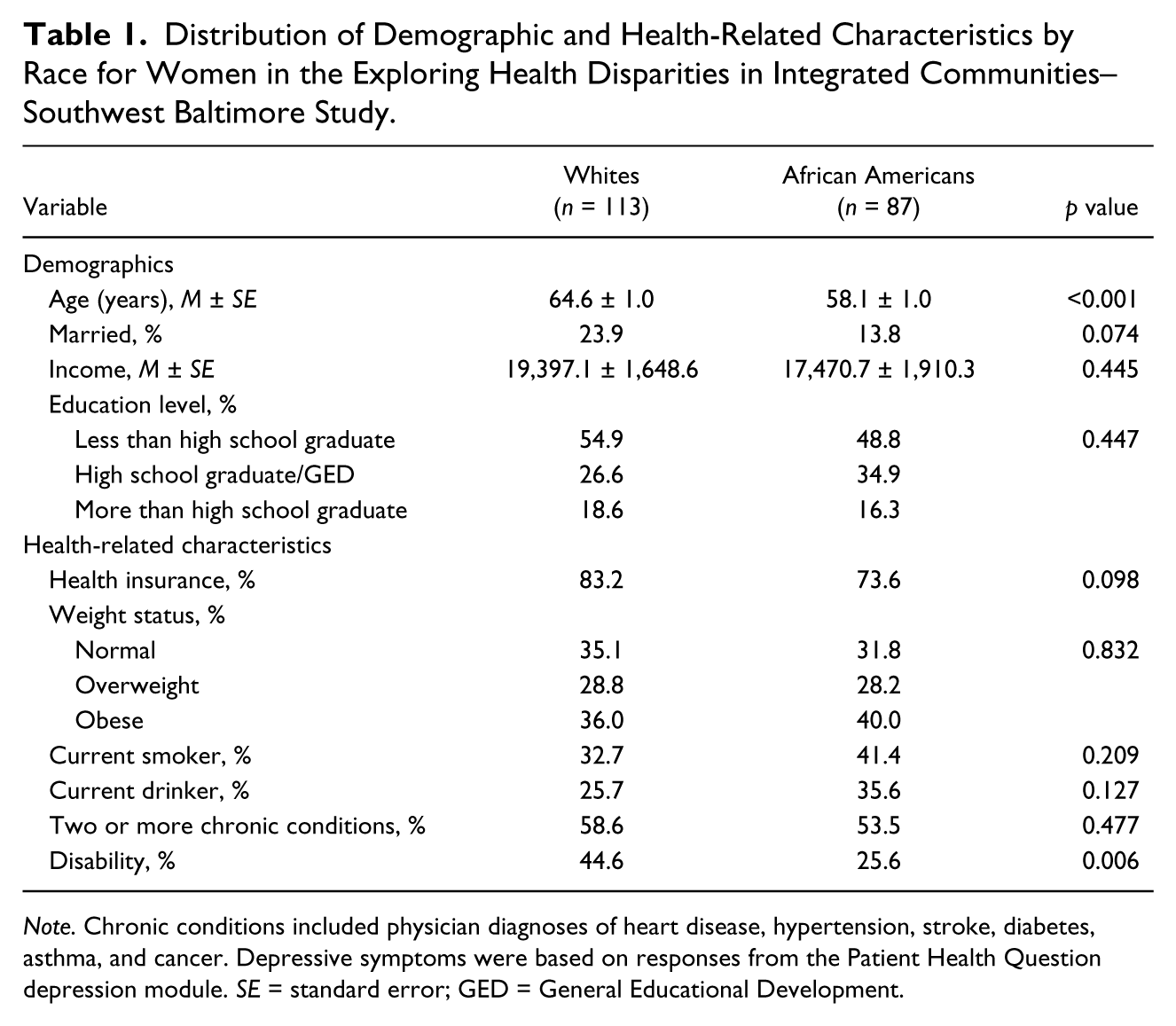
Note. Chronic conditions included physician diagnoses of heart disease, hypertension, stroke, diabetes, asthma, and cancer. Depressive symptoms were based on responses from the Patient Health Question depression module. SE = standard error; GED = General Educational Development.
The distribution of the demographic and health-related characteristics for men by race is shown in Table 2. African American men were less likely to report two or more chronic conditions or less likely to report disability than White men. Otherwise, the demographic and health-related profiles were similar for African American and White men. Specifically, there were no racial differences observed with regard to age, being married, income, education level, health insurance status, weight status, or being a current smoker or drinker.
Distribution of Demographic and Health-Related Characteristics by Race for Men in the Exploring Health Disparities in Integrated Communities–Southwest Baltimore Study.

Note. Chronic conditions included physician diagnoses of heart disease, hypertension, stroke, diabetes, asthma, and cancer. Depressive symptoms were based on responses from the Patient Health Question depression module. SE = standard error; GED = General Educational Development.
The distribution of the demographic and health-related characteristics for women by disability status is shown in Table 3. Women who reported disability were on average older, more likely to have an education that was less than a high school graduate, to have health insurance, and report two or more chronic conditions compared with those women who did not report disability. Women reporting disability were less likely to be African American, had a lower income than women, and were less likely to be a current drinker compared with women who did not report disability. There were no differences in disability status observed with respect to being married, weight status, and being a current smoker.
Distribution of Demographic and Health-Related Characteristics by Disability Status for Women in the Exploring Health Disparities in Integrated Communities–Southwest Baltimore Study.
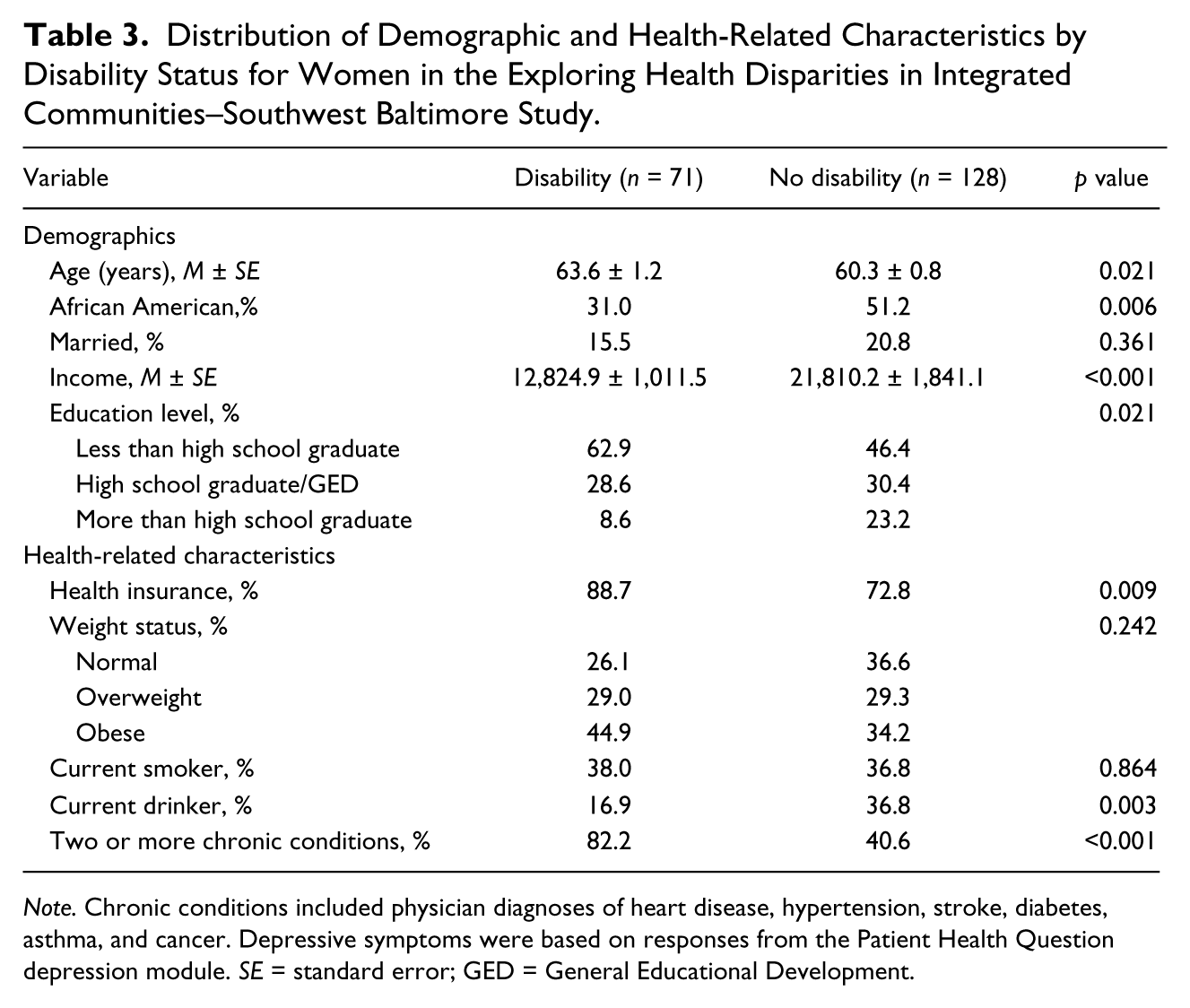
Note. Chronic conditions included physician diagnoses of heart disease, hypertension, stroke, diabetes, asthma, and cancer. Depressive symptoms were based on responses from the Patient Health Question depression module. SE = standard error; GED = General Educational Development.
The distribution of the demographic and health-related characteristics for men by disability status is shown in Table 4. Men who reported disability were on average older, more likely to have an education that was less than a high school graduate, and report two or more chronic conditions compared with those men who did not report disability. Men reporting disability were less likely to be African American and had a lower income compared with men who did not report disability. There were no differences in disability status observed with respect to being married, health insurance status, weight status, and being a current smoker or drinker.
Distribution of Demographic and Health-Related Characteristics by Disability Status for Men in the Exploring Health Disparities in Integrated Communities–Southwest Baltimore Study.
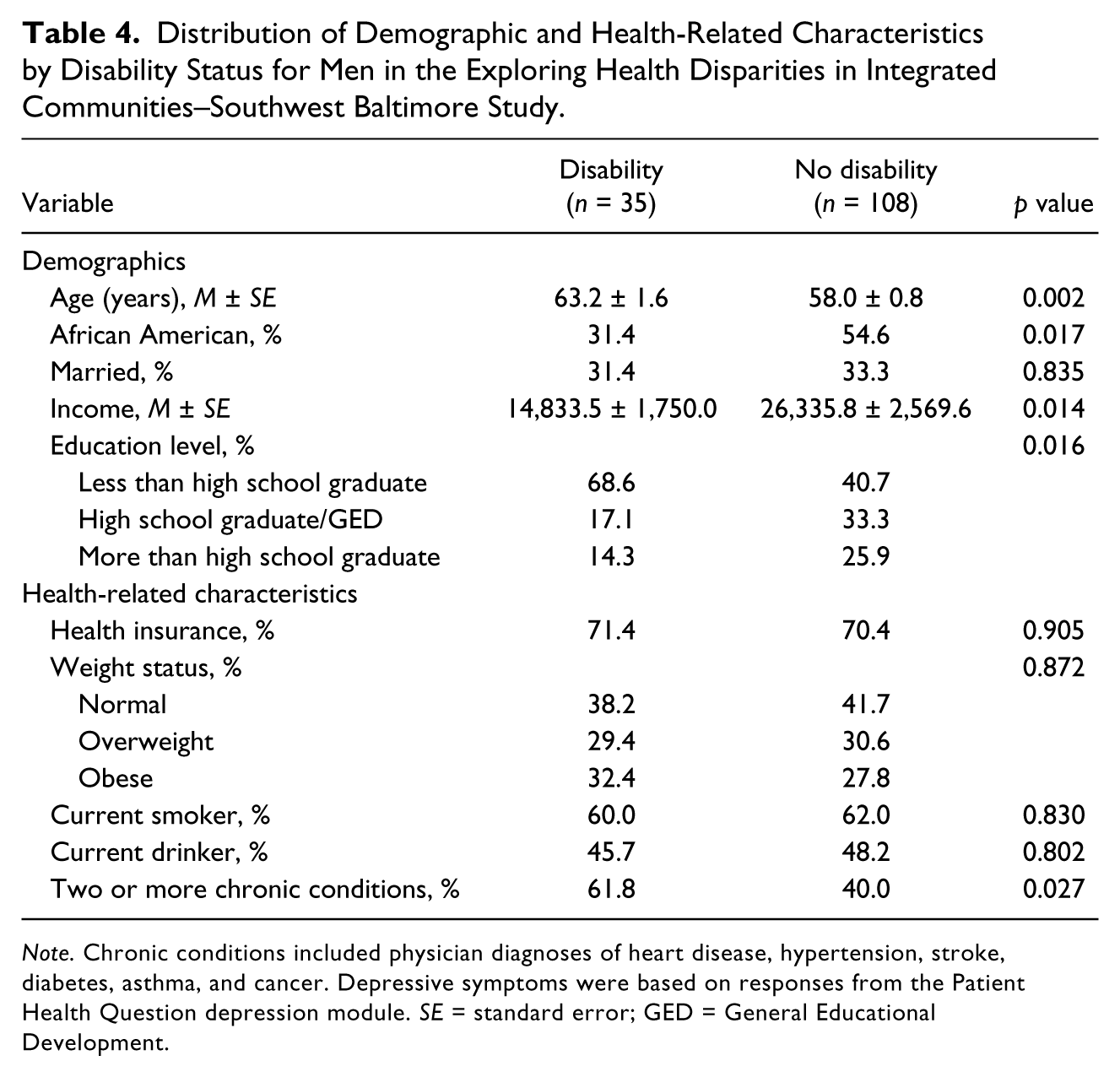
Note. Chronic conditions included physician diagnoses of heart disease, hypertension, stroke, diabetes, asthma, and cancer. Depressive symptoms were based on responses from the Patient Health Question depression module. SE = standard error; GED = General Educational Development.
The association between race and disability by sex is shown in Table 5. Accounting for age, marital status, income, education, insurance status, weight status, drinking and smoking status, and two or more chronic conditions, African American women (odds ratio [OR] = 0.32, 95% confidence interval [CI] = [0.14, 0.70]) and men (OR = 0.34, 95% CI = [0.13, 0.90]) had lower odds of reporting disability than Whites.
Association Between Race and Disability in the Exploring Health Disparities in Integrated Communities Study–Southwest Baltimore.
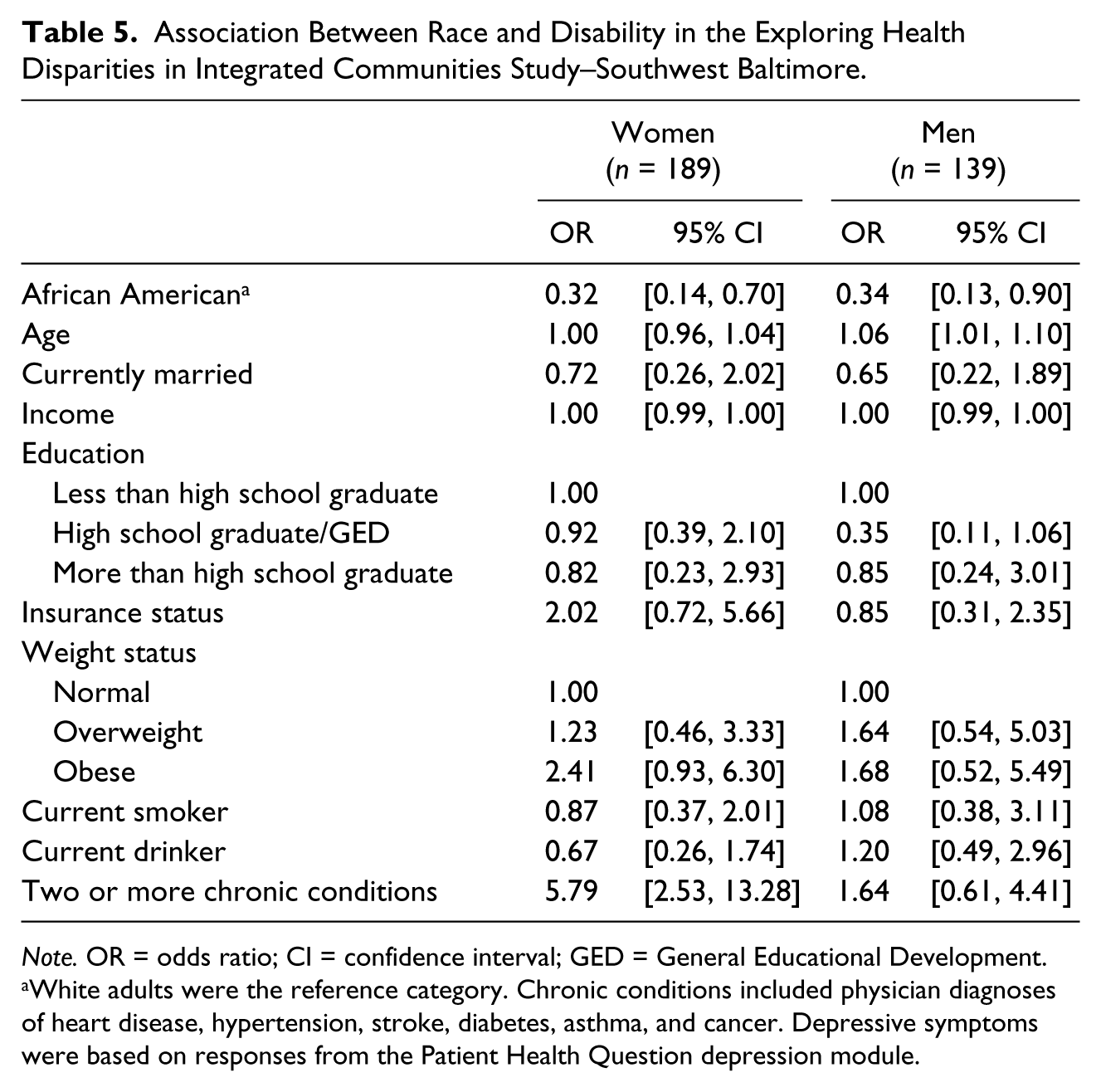
Note. OR = odds ratio; CI = confidence interval; GED = General Educational Development.
White adults were the reference category. Chronic conditions included physician diagnoses of heart disease, hypertension, stroke, diabetes, asthma, and cancer. Depressive symptoms were based on responses from the Patient Health Question depression module.
Discussion
This study examined racial differences in disability among African American and White community-dwelling older adults living in similar social and environmental conditions with similar income levels. Results provide evidence that within this urban, low-income racially integrated sample, older African Americans have lower odds of reporting disability compared with older Whites. These findings highlight the importance of social and structural inequalities in understanding disparities in disability between African Americans and Whites (Committee on Understanding and Eliminating Racial and Ethnic Disparities in Health Care, 2002; Thorpe, Koster et al., 2011). Thus, social context should continue to be considered as an important determinant of disability.
African Americans had lower odds of reporting disability than Whites, who live in similar social and environmental conditions. This finding is inconsistent with prior studies that only accounted for individual-level variables (D. O. Clark & Maddox, 1992; Kelley-Moore & Ferraro, 2004; Mendes de Leon et al., 2005; Schoeni et al., 2005; Thorpe, Kasper, et al., 2008). In those studies, African Americans exhibited poorer functioning than Whites. However, these studies may have been attributing racial differences in disability to what was actually a result of differences in health risk environments in which African Americans and Whites typically live (LaVeist, Pollack et al., 2011; LaVeist, Thorpe, et al., 2008; Thorpe, Koster et al., 2011).
Among the previous literature that examined the effect that neighborhood factors or characteristics have on disability (Balfour & Kaplan, 2002; Beard et al., 2009; C. R. Clark et al., 2009; Freedman, Grafova et al., 2008; Glass & Balfour, 2003; Lang et al., 2008; Nordstrom et al., 2007; Pruchno et al., 2012; White et al., 2010), very few have examined the impact of neighborhoods or geography on racial disparities in disability. For example, Lin (2000) demonstrated that region of the United States was important in racial disparities and disability. He found that both Blacks and Whites who lived in the South had a higher risk of disability than Whites compared with other regions. African Americans typically live in South. Yet, national statistics do not account for the fact that African Americans tend to live in the region of the country where they have higher rates of disability. Our findings extend to African American and White older adults who live under similar social and environmental conditions and have similar socioeconomic resources.
The health profile of the White older adults is a plausible explanation for our findings. Pathology (health conditions) is the first stage of the disablement process (Nagi, 1976; Verbrugge & Jette, 1994). In general, White older adults have a better health profile than African American older adults (Committee on Understanding and Eliminating Racial and Ethnic Disparities in Health Care, 2002; Thorpe, Koster et al., 2011; Thorpe et al., 2008). But, in this urban, low-income racially integrated community, White older adults had a similar health profile compared with African American older adults (LaVeist, Pollack et al., 2011). This suggests that when White older adults endure similar health risk exposures of a low-income urban environment as African Americans, such as low accessibility to healthy foods, spaces for exercise, and health care resources, their health and function are similar to or worse than African American older adults who typically live in these communities.
The United States remains a highly segregated country (Iceland, 2004, 2009; Iceland, Weinberg, Steinmetz, & U.S. Census Bureau, 2002; Wilkes & Iceland, 2004). Few studies account for segregation, although upward of 60% of African Americans would need to move to another census tract to achieve complete integration between African Americans and non-Hispanic White Americans (Iceland et al., 2002; LaVeist, Gaskin, & Trujillo, 2011; Massey & Denton, 1993). Residential segregation tends to have a negative impact on the health and function of those with fewer financial resources. That is, residential segregation typically concentrates poor African American older adults, and in this case poor White older adults in geographic areas where there seems to be less access to health care facilities and resources (Gaskin et al., 2009; Williams & Collins, 2001). The fact that African American and White older adults typically live in vastly different social environments—environments where they have aged in place—facilitates differences in the quality and type of care they have available to them (Gaskin et al., 2009; Landrine & Corral, 2009; Williams & Collins, 2001).
Racial segregation has also been found to be associated with negative neighborhood characteristics such as poor housing conditions (Black & Macinko, 2008), high crime (Lee, 2000), and lower availability of fresh fruits and vegetables (Moore & Diez Roux, 2006; Powell, Slater, Chaloupka, & Harper, 2006). This differential exposure to neighborhood stressors can influence health outcomes such as disability. For example, environments with fewer healthy food choices, parks, sidewalks, recreational spaces, and medical facilities may negatively affect health outcomes that subsequently lead to disability. Public health research should consider the environmental and social context in which a person lives because it greatly influences access to health resources as well as exposure to health risks (Gaskin et al., 2009; Gaskin et al., 2012a; LaVeist, Pollack et al., 2011; Williams & Collins, 2001).
The EHDIC study represents a new direction in health disparities research, one that accounts for as much unmeasured heterogeneity as possible in a naturally occurring environment that is often associated with race but not accounted for in most statistical analyses. In addition, EHDIC-SWB accounted for the confounding of race and SES that is present in many studies including national samples (LaVeist, Pollack et al., 2011). These results are consistent with other studies using EHDIC-SWB data (Bleich et al., 2010; Fesahazion et al., 2011; Gaskin et al., 2009; LaVeist et al., 2009; Thorpe et al., 2013), whereby African Americans have as good or better health profile than Whites living in this low-income urban community. Very few data sources are available to examine racial disparities in disability with no racial differences in income, modest differences in education, and account for the differential social and environmental conditions in which White and African American older adults generally live. Nevertheless, interpretation of these results should be considered in the following context. The external validity of our results may be limited because EHDIC-SWB was conducted in a low-income urban population. It is unknown whether these results would differ in higher SES groups and non-urban environments. Furthermore, because our analyses only included African American and White participants, they are not generalizable to other ethnic groups. It is worth noting that some of the parameter estimates in the models for men and women have wide CIs associated with them. Despite these limitations, this study contributes to our understanding of racial disparities in disability by using a study design that significantly minimizes the confounding of race, SES, and residential segregation.
Within this well-integrated, low-income urban community, African Americans had lower odds of reporting disability than Whites. This finding corroborates the notion that disability is influenced by one’s environment (Verbrugge & Jette, 1994). In addition, findings within an integrated, low-income urban sample support efforts to ameliorate racial disparities in disability by focusing on the social context in which people live. Future research in racial disparities in disability would benefit from creative approaches to examining racial disparities in disability within samples, which account for socioeconomic and environmental factors.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research conducted by the first author was supported by a grant from the National Institute for Minority Health and Health Disparities (P60MD000214) and Pfizer, Inc.