
Abstract
Many older adults experience some degree of cognitive decline with age. Usually, cognitive decline manifests as mild cognitive impairment, which is cognitive functioning within the normal range, but the individual complains about memory problems (Bennett et al., 2002; Larrieu et al., 2002). More severe, mid- and later-life cognitive decline often results from disease processes that interfere with normal brain functioning (Alzheimer’s Association, 2012). The extant literature is replete with studies that identify life-course factors that influence normal and disease-related changes in cognitive functioning among older adults (Borenstein, Copenhaver, & Mortimer, 2006; Douthit & Dannefer, 2006; Glymour & Manly, 2008). However, to date, no studies have considered the influence of military service on later-life cognitive trajectories even though a large percentage of men from early- and mid-20th-century birth cohorts served in the military (Wilmoth & London, 2011). The impetus to address this gap in the literature derives from evidence that male veterans have lower odds of memory-related disability than male nonveterans (Wilmoth, London, & Parker, 2011) and that health changes among older men, which may be associated with later-life cognitive change, differ by veteran status and by military service experience (Wilmoth, London, & Parker, 2010).
In this article, we draw on the life-course perspective and prior research on the life-course consequences of military service (Wilmoth & London, 2013) to argue that prior military service—as indicated by veteran, war service, and period of service statuses—has enduring effects that have the potential to influence later-life cognitive functioning. We begin by briefly reviewing the extant literature on life-course factors that influence later-life cognition and outlining a theoretical rationale for including veteran status in empirical models of later-life cognitive change. We then use data from the 1995-2006 waves of the Health and Retirement Study (HRS) to estimate growth curve models that examine differences in men’s cognition trajectories by veteran status. We focus on men because there are so few older women from early- and mid-20th-century birth cohorts who experienced military service. Specifically, building on prior research (Wilmoth et al., 2010), we address the following research questions:
Life-Course Influences on Later-Life Cognition
Previous research indicates that numerous early- to mid-life characteristics associated with military service also shape later-life cognition. For example, ascribed characteristics, such as sex and race/ethnicity, are important sources of variation in later-life cognition. Findings regarding the associations between sex and cognitive decline or dementia are mixed (Edland, Rocca, Petersen, Cha, & Kokmen, 2002; Lindsay et al., 2002), with some studies finding women to be at greater risk for dementia and other studies finding no significant difference between men and women. By contrast, racial/ethnic differences in cognitive functioning in later life are well-established (Sloan & Wang, 2005), with most studies finding that minority elders perform less well than Whites on cognition scales. Usually, controlling statistically for education and other potentially mediating socioenvironmental factors substantially reduces observed associations (Mehta et al., 2004).
Previous research has also documented relationships between socioeconomic status (SES) and cognitive functioning in childhood, adulthood, and old age (Everson-Rose, Mendes de Leon, Bienias, Wilson, & Evans, 2003; Kaplan et al., 2001). Few studies examine the relationship between early-life SES—which is usually measured by parental educational attainment, occupational prestige, and family SES, or a composite index of these characteristics—and cognitive decline in old age (Borenstein et al., 2006; Brown, 2010; Everson-Rose et al., 2003; Luo & Waite, 2005). However, childhood socioeconomic disadvantage has been linked to adult health status and behaviors, major depression, and physical functioning in later life (Guralnik, Butterworth, Wadsworth, & Kuh, 2006; Turrell, Lynch, Leite, Raghunathan, & Kaplan, 2007), which are factors that are associated with later-life cognitive functioning. Thus, childhood socioeconomic disadvantage may affect cognitive functioning in later life by influencing early-childhood cognitive development, as well as by shaping midlife cognition-related demographic, economic, health, and well-being outcomes that influence trajectories of cognitive development and decline across the adult life course.
A variety of factors in mid- and later life have been linked to cognitive functioning in older adults, including education (Lindsay et al., 2002), income, marital status, and some health behaviors (Herzog & Wallace, 1997). Impaired cognitive function is associated with various diseases or conditions in older adults, including cardiovascular disease, stroke, hypertension, and diabetes (Blaum, Ofstedal, & Liang, 2002; Haan et al., 2003; Taylor, 2008). In light of evidence documenting relationships between socioeconomic disadvantage, health problems, and cognitive functioning, some researchers have conceptualized decreased cognitive functioning in later life as a “marker of lifelong adversity” (Moody-Ayers, Mehta, Lindquist, Sands, & Covinsky, 2005, p. 933).
Military Service and Later-Life Cognition
Although there is an extensive literature on the life-course consequences of military service that compares veterans to nonveterans (Wilmoth & London, 2013), few studies have examined whether cognition varies by veteran status. This is unfortunate given that many of the early-life factors that the literature identifies as being associated with later-life cognition are also associated with veteran status. For example, various disabilities and health problems prevent military service in all eras, although the particular disqualifying conditions and preinduction physical exam rejection rates have changed over time (Wolf, Wing, & Lopoo, 2013). Among early- to mid-20th century birth cohorts, men (Campbell, 2013; Kelty & Segal, 2013), Whites (Lutz, 2008, 2013), and those from socioeconomically disadvantaged backgrounds (Bennett & McDonald, 2013) disproportionately served in the military. However, the midcentury racial integration of the military, policy changes related to women’s participation, the draft, and the subsequent shift to the All-Volunteer Force have changed service-related opportunities for racial/ethnic minorities, women, and individuals from various social classes.
Other factors are potentially affected by military service, such as educational attainment (Bennett & McDonald, 2013), employment (Kleykamp, 2013), income (Bennett & McDonald, 2013; Kelty & Segal, 2013), marriage and family outcomes (Burland & Lundquist, 2013; London, Allen, & Wilmoth, 2013; Usdansky, London, & Wilmoth, 2009), and health and disability (MacLean, 2013; Wilmoth et al., 2010, 2011). Although the effects of military service on these cognition-related mid- and later-life outcomes is variable across historical periods, policy contexts, and individual characteristics (Wilmoth & London, 2013), these factors have the potential to mediate the relationship between military service, which tends to begin and end relatively early in the life course, and later-life cognitive functioning.
Adopting a life-course perspective draws attention to the need for researchers to consider selection into military service in studies of the “effects” of military service, control for selection to the extent possible with available data and methods, and interpret results cautiously (Wolf et al., 2013). A life-course perspective also facilitates the examination of both the effect of prior military service on later-life cognition, net of early-life controls, and the possible pathways by which military service influences cognitive change in later life.
Although there is a substantial literature that examines cognition among veterans (Roca, Hart, Kimbrell, & Freeman, 2006; Wray et al., 2012; Yehuda, Golier, Tischler, Stavitsky, & Harvey, 2005), no studies examine veteran status differences and change in later-life cognitive outcomes. One recent study based on data from the 2000 U.S. Census of Population documents that veteran status is significantly associated with self-reported memory-related disability, although the direction of the association differs for women and men (Wilmoth et al., 2011). Overall, 7.56% of female veterans and 6.13% of male veterans reported memory-related disability, compared with 5.69% of female nonveterans and 4.78% of male nonveterans, respectively. In sex-specific multivariate logistic regression models that controlled for age, race/ethnicity, marital status, education, citizenship, and region, the odds of having a memory disability were significantly higher among female veterans than among female nonveterans (adjusted odds ratio [AOR] = 1.18, p < .001) and significantly lower among male veterans than among male nonveterans (AOR = 0.93, p < .001). Although this study did not report results by age, these findings demonstrate that veteran status is associated with memory-related disability and raise questions about how and why veteran status affects cognition in later life.
There are various theoretical reasons to expect that later-life cognition might differ by veteran status. On the one hand, veterans may have better cognitive functioning in later life than nonveterans because the military has relatively stringent physical, mental, and moral standards for admission and rejects potential recruits who are overweight, in poor health, or have apparent moral shortcomings (Sackett & Mavor, 2006). To the extent that the factors that select people into the military are associated beneficially with cognitive development or subsequent cognitive decline across the life course, such selectivity has the potential to contribute to the appearance of a positive association between veteran status and better later-life cognition.
Beyond selection, military service may generally contribute to better cognitive outcomes by increasing access to training and education through the GI Bill, health care, and a range of other resources that improve living conditions (Wilmoth & London, 2011). It may also contribute to better employment, earnings, and wealth outcomes (Kleykamp, 2013; Street & Hoffman, 2013), although recent evidence indicates that, among the working-aged, the veteran advantage with respect to poverty and material hardship is substantially eroded when the veteran is disabled (Heflin, Wilmoth, & London, 2012; London, Heflin, & Wilmoth, 2011). Veterans may also see some long-term benefits from the physical training and fitness required during the period of active-duty service, or from exercise and lifestyle patterns that carry over from the active-duty period into later life in ways that are beneficial for health and well-being, and, ultimately, cognition. In addition, entering the military may “knife off” negative influences from earlier in life and provide a “bridging environment” to better health care resources, education, and training opportunities through the Department of Veterans Affairs (Bound & Turner, 2002; Elder, 1986, 1987; MacLean, 2005; Sampson & Laub, 1996). Although access to these resources varies by race/ethnicity and historical context (Mettler, 2005; Teachman & Call, 1996), it is plausible that military service may be associated with better cognition in later life by setting veterans, particularly those from disadvantaged backgrounds and unharmed by their service, on better trajectories through life than similar nonveterans.
On the other hand, veterans may have worse later-life cognitive functioning than nonveterans because they are selected disproportionately from disadvantaged backgrounds (Bennett & McDonald, 2013). Early-life disadvantage may have lifelong consequences for cognition outcomes despite stringent preservice screening and the potential for military service to function as a positive turning point in the life course. More direct, negative influences of military service on cognition may result from service-connected injuries or exposure to hazardous environments that impair health and well-being, and, ultimately, cognitive functioning. The military has historically exposed service members to risky health behaviors, either by subsidizing tobacco products or by placing service members in environments conducive to heavy alcohol and substance use (Bedard & Deschênes, 2006; Clipp & Elder, 1996; Elder & Clipp, 1988, 1989; Elder, Clipp, Brown, Martin, & Friedman, 2009; Miech, London, Wilmoth, & Koester, 2013). Combat exposure is also linked to greater risk of short-term injuries and long-term physical disability (Elder, Shanahan, & Clipp, 1997), and physical and mental health problems (Elder et al., 2009; Vogt, King, King, Savarese, & Suvak, 2004). Relatively early-life traumatic brain injuries or service-connected sensory impairments may negatively affect cognition in later life.
Much of the literature on cognitive function in veterans is linked to the psychological effects of combat, such as posttraumatic stress disorder (PTSD), with or without the presence of other psychological disorders (Roca et al., 2006; Yaffe et al., 2010; Yehuda et al., 2005). Golier and colleagues (2002) hypothesized that PTSD affects memory in older adults by accelerating memory decline. Their research on Holocaust survivors linked severe and prolonged trauma, and resulting long-term PTSD, to greater cognitive burden later in the life course (Golier et al., 2002). Similar cognitive deficits were found in older combat veterans with PTSD (Yehuda et al., 2005), although their cognitive deficits manifested differently. The negative effects of combat exposure are seen among veterans of all wars (Frey-Wouters & Laufer, 1986; Kulka et al., 1990; Teachman & Call, 1996); however, as is the case with other health outcomes (Wilmoth et al., 2010), veterans who served during different historical periods and wars may have different cognitive trajectories.
Veterans, in general, and war veterans, in particular, might also suffer worse cognitive functioning in later life due to associated declines in physical health. A recent longitudinal study documents that older male veterans had better health than nonveterans around retirement age, but experienced greater age-related changes in health than nonveterans net of a range of early-life and time-varying later-life controls (Wilmoth et al., 2010). Similarly, men who served during wartime had better health at the mean age, but more-rapid age-related changes in health than men who did not serve during wartime. Among war veterans, Vietnam War veterans were in poorer health at the mean age, but they experienced less substantial age-related health changes than men who served during previous wars. World War II (WWII) and Korean War veterans experienced particularly steep age-related increases in activities of daily living (ADL) limitations and decreases in self-rated health compared with Vietnam War veterans.
The known connections between cognitive function and a variety of chronic conditions in older adults, and the documented differences in health change between older veterans and nonveterans, as well as veterans with differing military service experiences, point to the need for research that examines whether there are veteran status disparities in later-life cognitive functioning. Based on current knowledge regarding the effects of military service across the life course, we expect later-life cognitive functioning to be poorer, and declines in cognitive functioning to be steeper, among veterans (compared with nonveterans), war service veterans (compared with nonwar service veterans), and veterans who potentially had longer durations of service because they served during multiple wars (compared with veterans who served only during WWII or the Korean War).
Method
Sample
This study uses data from the 1995 to 2006 longitudinal Assets and Health Dynamics Among the Oldest Old (AHEAD), HRS, and RAND HRS files (henceforth HRS). The analytic sample for this study includes 6,863 men born between 1895 and 1941. During the 11 years of the study, these men contributed 21,438 observations to the person–period file that we use to estimate growth curve models. The person–period file only contains observations for HRS age-eligible respondents who were old enough to participate in the cognition portion of the interview (i.e., age 65 years or older) and able to complete the self-interview without the assistance of a proxy. Because so few Vietnam War veterans were old enough to participate in the cognition portion of the interview (i.e., less than 2% served only during the Vietnam War), we deleted all Vietnam War veterans from the analytic sample. As noted previously, the analysis does not include women because less than 1% (135) of the 14,491 women in the HRS served in the military.
Measures
Dependent Variables
The HRS measured cognitive functioning using a modified version of the Telephone Interview for Cognitive Status (TICS) instrument. In the late 1980s, the developers of the TICS drew on then-current state-of-the-science understandings of the dimensions of cognition (Zsembik & Peek, 2001) and designed it to collect a comprehensive range of information on cognitive functioning. The TICS is a validated measure of cognitive functioning (Zsembik & Peek, 2001) that is based on Folstein’s Mini Mental Status Exam (MMSE). The MMSE is a commonly used instrument for assessing dementia in clinical settings that can be reliably administered by telephone (Freedman, Aykan, & Martin, 2001; Herzog & Wallace, 1997). For the HRS, the TICS was modified to measure six tasks, with a maximum score of 35 points. These tasks evaluate memory and executive function as aspects of cognitive function, and weight fluid cognitive measures more heavily than in the original instrument (Freedman et al., 2001; Herzog & Wallace, 1997).
Military Service Variables
The retrospective report of service in the military identifies men who have experienced “active military service,” not including service in the military reserves. Respondents who report military service answer follow-up questions about start and stop dates. We assumed that service was continuous and used these dates to determine service during WWII (1941-1946) and the Korean War (1950-1955). We used start and stop dates for the wars that are the same as those used by the Veterans Administration to determine eligibility for wartime service benefits. They include periods of combat as well as occupation. We then constructed three military service measures: veteran status (yes = 1), wartime service (yes = 1), and period of service (only WWII, only Korea, and both WWI and Korea). We use the veteran status and wartime service variables to identify the appropriate subpopulations of veterans and wartime veterans for specific analyses.
Control Variables
The analysis includes a broad range of control variables, which prior research indicates are associated with both veteran status and later-life cognition. The first set of control variables are retrospectively reported early-life characteristics that occurred prior to military service: race/ethnicity, early-life socioeconomic disadvantage, and early-life health. Race/ethnicity includes non-Hispanic White (reference), non-Hispanic Black, non-Hispanic other race, and Hispanic (of any race). Early-life disadvantage is an indexed scale, which is comprised of four dichotomously coded variables: mother’s education and father’s education (<8 years = 1; ≥8 years = 0); father’s occupation (unskilled manual = 1, nonmanual, skilled, and professional = 0); and family SES (poor = 1, not poor = 0). Per the procedure outlined in Wilmoth et al. (2010), respondents missing on a given variable were assigned to the zero category for that variable. We then summed these four variables and divided by 4. This procedure yields an early-life disadvantage scale that is a conservative estimate of early-life disadvantage because misclassification would bias toward the null. The scale ranges from 0 to 1, with higher values indicating greater disadvantage. We also include a variable that is equal to one for all individuals for whom at least one of these variables was missing and set to zero. In addition, the analysis includes a retrospectively reported measure of health at age 16 years, which includes the following categories: excellent, very good or good health (reference category), fair or poor health, and missing.
The other variables, which reference mid- to late-life characteristics that might mediate the relationship between military service and later-life cognitive function, are measured many years after military service has ended. All of these mid- to late-life variables, except education, are time varying across the 11-year study period. Marital status includes four categories: married (reference), never married, divorced/separated, and widowed. Education is measured at entry into the HRS and includes high school or less (reference), any college, and more than college (i.e., graduate or professional school). Household income is measured in dollars. Labor force status is recoded as a binary variable (in the labor force = 1). Two health behaviors are measured dichotomously: ever smoked cigarettes (yes = 1) and currently drinks alcohol (yes = 1). Body mass index (BMI) is used to identify men who are underweight (BMI < 18.5), normal weight (reference category, 18.5 ≤ BMI < 24.9), and overweight (BMI ≥ 25.0). Self-rated health, vision, and hearing are five-category, ordinal measures (excellent, very good, good, fair, or poor); these scales are reverse coded such that higher values indicate better self-rated health, vision, and hearing. Number of health conditions is a summary variable, which is based on asking respondents if they ever had any of the following conditions: high blood pressure, diabetes, cancer, lung disease, heart disease, stroke, psychiatric problems, and arthritis. Responses are coded dichotomously (yes = 1) and summed to indicate the number of health conditions that each respondent reported (ranging from 0 to 8). Respondents were also asked whether they had any difficulty with bathing, eating, dressing, walking across a room, and getting in or out of bed. Responses are coded dichotomously (difficulty = 1) and summed to create an indicator of ADL limitations that ranges from 0 to 5.
Finally, we include two methodological controls. One variable measures dropping out of the study prior to the 2006 wave (yes = 1) and the other measure dying during the 11-year time span of the study (yes = 1).
Sample Description
Overall, in the analytic sample, 64% of men are veterans. Among veterans, 93.5% served during wartime. Among wartime veterans, 56% served only during WWII, 36% only during the Korean War, and 7% served during both wars.
In a supplemental analysis, we examined the characteristics of the overall sample and the veteran subsamples (tables available from the first author upon request). The results document significant differences between veterans and nonveterans, veterans with and without wartime service, and wartime veterans who served during different historical periods. For example, relative to nonveterans, veterans are more likely to be White, which reflects the fact that a high proportion of veterans in the HRS come from older cohorts and served in historical periods in which African Americans and Latinos were less likely to be in the military (Lutz, 2008, 2013). Consistent with health selection processes for entering the military, veterans are also less likely to report poor early-life health. Most likely as the result of receiving GI Bill benefits, veterans are more likely to have attended college, or to have more than college educational attainment, and have higher mean household incomes than nonveterans. Veterans are more likely to be married, to have ever smoked, to currently drink alcohol, and to report better self-rated health, vision, and hearing, but they also report more chronic conditions and are less likely to be in the labor force. Overall, veterans are less likely to be lost to follow-up or to have died during the study period (i.e., before the 2006 wave of the survey).
As noted above, the vast majority of veterans in this sample are wartime veterans. Those veterans who served during wartime are significantly older than those who did not. They are less likely to be in the labor force and to currently drink alcohol, but more likely to be married. Compared with nonwar veterans, war service veterans have lower rates of any college and more than college education and a lower mean household income, and are more likely to report poor early-life health and higher levels of childhood disadvantage. On average, compared with peacetime veterans, wartime veterans have poorer self-rated health, vision, and hearing; more chronic conditions; and higher rates of depression. They are also more likely to be lost to follow-up or to die before the 2006 wave of the study.
The characteristics of veterans reflect, in large part, the characteristics of WWII veterans, who represent the largest share of veterans in this sample. Among wartime veterans, WWII only and Korean War only veterans report higher rates of poor childhood health than do veterans of both wars. Compared with those who served during the Korean War only or both wars, those who served during WWII only are older, are more likely to have experienced early-life socioeconomic disadvantage, are less likely to have any college education, have the lowest mean household income, and report poorer self-rated health, vision, and hearing. They are the most likely to be non-Hispanic White, widowed, depressed, and to have ever smoked, and the least likely to be in the labor force, to be married, and to be overweight or obese. WWII veterans are more likely to have died before the 2006 wave, but are less likely to be lost to follow-up than are veterans of the Korean War only or both wars.
Analysis Plan
The multivariate analysis takes these differences across groups into account by estimating conditional growth curve models using the PROC MIXED procedure in SAS. A person–period file is used to estimate growth curve models for the overall sample, the veteran subsample, and the war service veteran subsample. Our modeling approach allows us to account systematically for the unique characteristics and experiences of men with different military service experiences. A simple comparison of veterans and nonveterans confounds differences between veterans that are related to wartime service; similarly, a comparison of war service and nonwar service veterans masks differences between those who served during different wars. In addition, by focusing only on veterans in some analyses, concerns about selection into military service are minimized because everyone in these subsample analyses met the criteria for service that were in place at the time of enlistment or conscription. Similarly, restricting the period of service analysis to wartime veterans minimizes the impact of issues related to selection into wartime service and variation in the risk of surviving active duty between those who did and did not serve during war.
In all of these analyses, we define time in terms of chronological age (as opposed to study duration) because we are interested in modeling age-related changes in cognition. The grand mean age for all sample members, which is equal to 74.5 years, is used to center age. It is noteworthy that the grand mean, which is used to estimate intercept effects, is between the ages of 70 and 75, when veterans from different war periods can be directly compared at the same chronological age. This unique feature of the analysis enables us to make meaningful comparisons across veterans who served in WWII only, the Korean War only, and both wars.
Models are estimated for total cognitive function; observations lacking valid cognition scores are dropped from the analysis. All models include age and age squared to test for nonlinearity in the relationship between age and cognition scores. In addition, we include terms that interact age and age squared with the military service variables to account for potential nonlinearity in the slope that estimates age-related changes in cognitive functioning in relation to military service. The models also control hierarchically for early-life and mid- to late-life characteristics, as well as methodological controls for attrition and death over the study period, although the coefficients for controls are not shown (full models are available upon request). We focus on interpreting the coefficients for the effect of veteran status on cognition at the mean age of 74.5 years and the effect of veteran status on age-related changes in cognitive functioning. Positive coefficients indicate that men with a given military service characteristic have higher cognitive functioning than the reference group, whereas negative coefficients indicate the opposite.
We also present figures showing the predicted cognition scores at ages 50 through 90 years by veteran status for the full sample, the veteran subsample, and the war service veteran subsample, respectively. These predicted values represent men: who are non-Hispanic White, married, out of the labor force, nonsmokers, nondrinkers, and normal weight; who report good early-life health, a high school degree or less, no chronic health conditions or ADL limitations, and average early-life disadvantage, household income, vision, hearing, and self-rated health; and who did not die during or drop out of the study. It is important to note that these values are model-based predictions generated from sample observations that span up to 11 years of later life. In the analysis of the war service veterans, there are limited numbers of WWII veterans at younger ages, because most of the group was past those ages upon entry into the study. Similarly, the majority of Korean War veterans were too young for a substantial number to have aged into the oldest age ranges during the observation period. Therefore, the figures for the war service veteran subsample present trajectories over the age ranges that capture the majority of each group’s observations. Five-year intervals containing less than 5% of the observations for a given group are not included in the figures.
Results
Descriptive Results
As shown in Table 1, veterans have better cognitive functioning than nonveterans. Herzog and Wallace (1997) claim that the lowest 5% of the range of cognition scores in a given sample indicate the portion of that sample living with severe cognitive impairment. In this sample, that 5% cut point for severe cognitive impairment is 11 points on the 35-point TICS scale. Overall, the mean cognition score of 21 suggests that the level of cognitive functioning in the sample is moderate.
Mean Cognition Scores by Veteran Status.
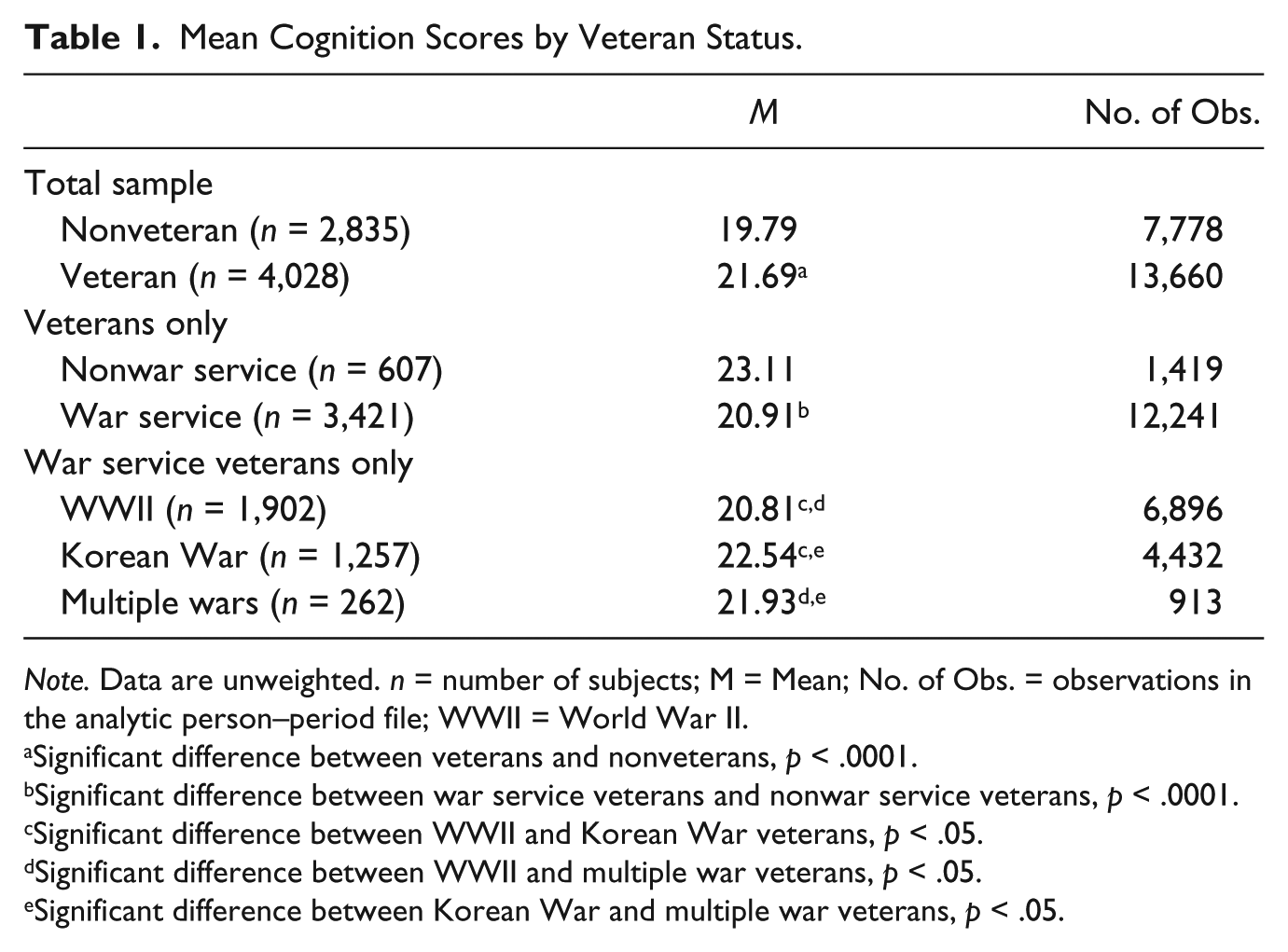
Note. Data are unweighted. n = number of subjects; M = Mean; No. of Obs. = observations in the analytic person–period file; WWII = World War II.
Significant difference between veterans and nonveterans, p < .0001.
Significant difference between war service veterans and nonwar service veterans, p < .0001.
Significant difference between WWII and Korean War veterans, p < .05.
Significant difference between WWII and multiple war veterans, p < .05.
Significant difference between Korean War and multiple war veterans, p < .05.
Table 1 also shows that nonwar veterans have better cognitive function than war service veterans. In addition, among the three groups of war service veterans, Korean War veterans have the highest cognition scores and WWII veterans have the lowest scores. These bivariate differences may be due to variation across the groups in age and in early- and mid- to late-life characteristics, which are controlled in the multivariate analyses that follow.
Multivariate Trajectory Analysis
Table 2 presents hierarchical growth curve models predicting cognitive function. Separate panels are shown for the effect of veteran status in the full sample, war service among the subsample of veterans, and historical period of service among the subsample of war service veterans. Four hierarchical models are displayed in the table. Model 1 includes only those variables pertaining directly to military service and age. Model 2 includes controls for race and ethnicity, early-life socioeconomic disadvantage, and early-life health, which influence selection into military service. Model 3 includes additional controls for education, income, labor force participation, marital status, current alcohol consumption, smoking, BMI, sensory function, self-rated health, chronic conditions, and ADL limitations, which potentially mediate the association between veteran status and later-life cognition. Model 4 includes additional controls for attrition from and death during the course of the study, respectively. As expected, all models indicate that cognitive function declines with age among all groups. These models also indicate that this rate of cognitive decline becomes steeper as individuals get older.
Growth Curve Models Predicting Cognition Trajectories.
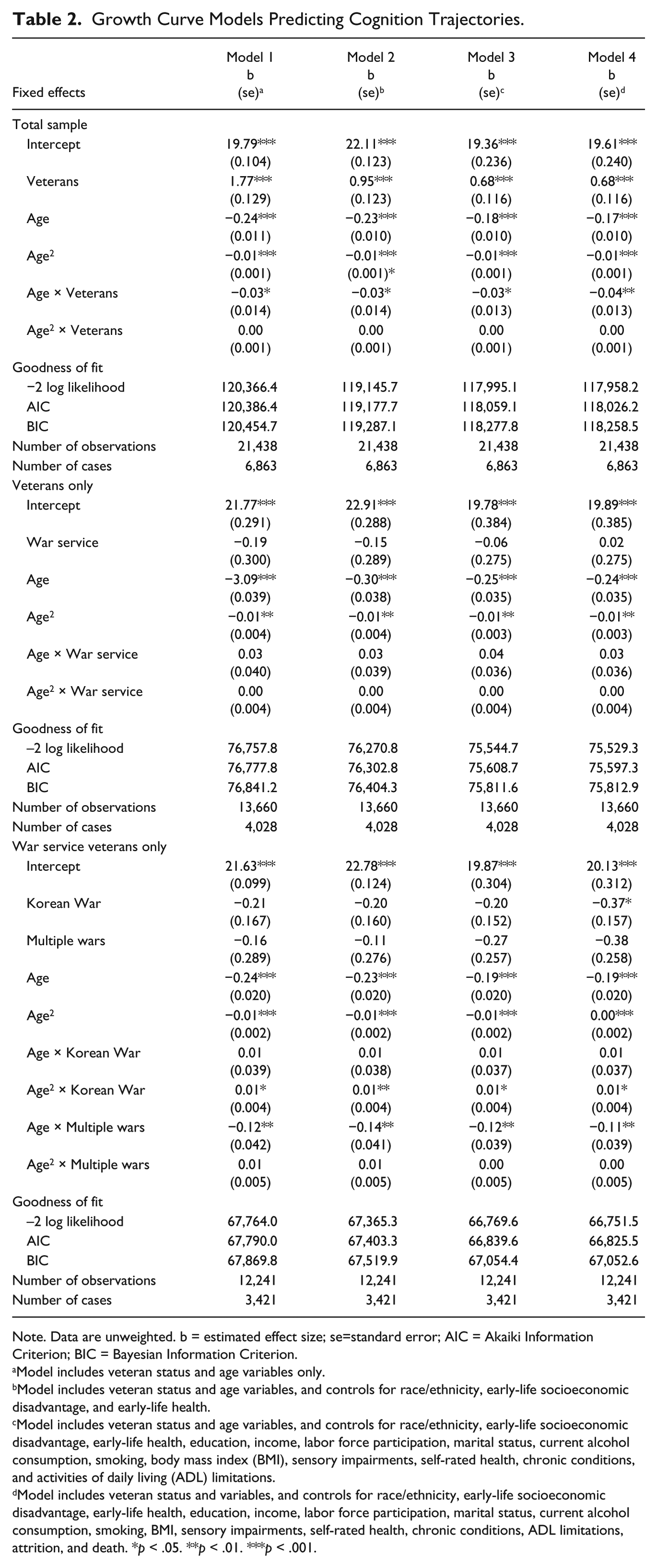
Note. Data are unweighted. b = estimated effect size; se=standard error; AIC = Akaiki Information Criterion; BIC = Bayesian Information Criterion.
Model includes veteran status and age variables only.
Model includes veteran status and age variables, and controls for race/ethnicity, early-life socioeconomic disadvantage, and early-life health.
Model includes veteran status and age variables, and controls for race/ethnicity, early-life socioeconomic disadvantage, early-life health, education, income, labor force participation, marital status, current alcohol consumption, smoking, body mass index (BMI), sensory impairments, self-rated health, chronic conditions, and activities of daily living (ADL) limitations.
Model includes veteran status and variables, and controls for race/ethnicity, early-life socioeconomic disadvantage, early-life health, education, income, labor force participation, marital status, current alcohol consumption, smoking, BMI, sensory impairments, self-rated health, chronic conditions, ADL limitations, attrition, and death. *p < .05. **p < .01. ***p < .001.
Results presented in the top panel of Table 2 indicate that veterans have significantly better cognitive function than their nonveteran peers at the mean-centered age of 74.5 years. However, veterans experience a steeper rate of cognitive decline than nonveterans, and the rate of cognitive decline among veterans increases as they age. Controlling for early-life characteristics that influence selection into the military reduces the difference in cognitive functioning between veterans and nonveterans by 46%; however, the veteran status difference remains statistically significant. Additional controls for mid- to late-life characteristics further attenuate, but do not eliminate, the effect of veteran status on cognitive functioning. Moreover, they do not explain the veteran status difference in the rate of cognitive decline. Controls for attrition and mortality, included in the fully specified model, do not provide any additional explanation of the effect of veteran status on cognitive functioning, but they do result in a slightly steeper rate of cognitive decline among veterans.
Figure 1 illustrates the predicted differences in cognitive function and cognitive decline between veterans and nonveterans, when controlling for all variables included in Model 4. As seen in Figure 1, the mean cognition trajectory for veterans has a steeper slope than for nonveterans. Although veterans are predicted to have better cognitive function at age 74.5 years, and an even larger advantage in terms of cognitive function around age 65, the steeper slope indicates that as they age, their cognitive functioning becomes increasingly similar to that of their nonveteran peers.

Predicted cognition trajectories by veteran status, with controls.
The results displayed in the second panel in Table 2 indicate that, compared with the small minority of veterans who served during peacetime, war service veterans do not experience significantly different levels of cognitive function later in life, nor do they experience significantly different rates of decline in cognitive function as they age. The cognition trajectories displayed in Figure 2, which are derived from the fully controlled Model 4, show how similar the cognition levels are between war service veterans and nonwar veterans in this sample. Both lines are very similar to the line for all veterans displayed in Figure 1.
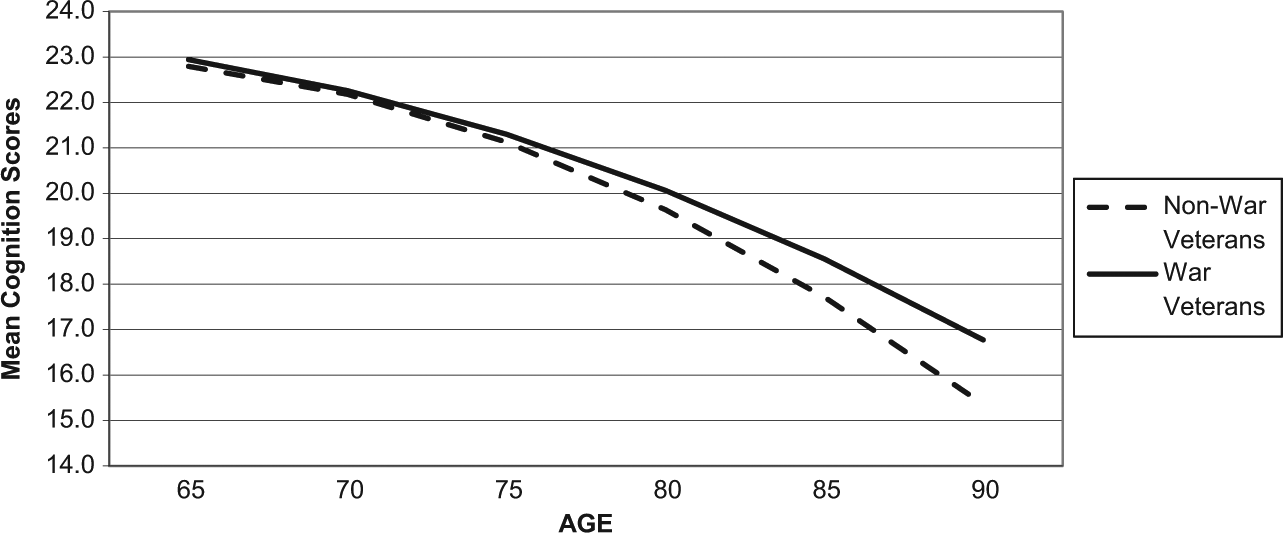
Predicted cognition trajectories among veterans by war service, with controls.
The results displayed in the third panel in Table 2 indicate that, compared with WWII only veterans, Korean War only veterans have lower cognition scores at the mean-centered age, but veterans of both wars do not have significantly different levels of cognitive function. However, both Korean War veterans and veterans of both wars have different trajectories of decline when compared with WWII veterans. The difference in cognition scores between Korean War and WWII veterans at the mean-centered age is only significant in Model 4, which includes controls for attrition and death. Supplemental analyses (not shown) indicate that Korean War veterans are less likely to die during the study period than WWII veterans, which suppresses the cognitive differences between these two groups. Once the better survival of Korean War veterans is taken into account, their poorer cognitive functioning early in later-life (ages 65-70) is revealed. The effects of serving during the Korean War or both wars on cognition trajectories increase when controlling for early-life characteristics influencing selection into the military, but the addition of mid- and later-life characteristics fully attenuates these effects.
These differing trajectories are visible in Figure 3, which shows the predicted cognition trajectories for all three groups of war service veterans based on results from Model 4. As seen in Figure 3, the slope of the cognition trajectory for veterans of the Korean War only is not as steep as the slope for WWII only veterans; it has a slightly different nonlinear shape than the WWII only trajectory, with decline slowing as this group advances in age. This difference in the shape of the trajectories suggests that there is a crossover around the mean-centered age of the sample. This crossover implies that the Korean War only veterans, who are younger than the WWII only veterans, may be experiencing better cognitive functioning at later ages than the WWII only veterans. In contrast, the trajectory for veterans of both wars is steeper than that of WWII only veterans. This trajectory also has a different shape than the trajectory for WWII only veterans; there is no quadratic effect for cognitive decline among veterans of multiple wars, resulting in a more linear trajectory. This steeper rate of decline suggests that veterans of both wars may be worse off in terms of cognitive functioning in later years, compared with veterans who fought in WWII only.

Predicted cognition trajectories among veterans by war service, with controls.
Discussion
The current gap in knowledge about whether and how veterans and nonveterans differ with respect to later-life cognition trajectories is problematic because older veterans are a large, policy-relevant demographic group. In 2010, more than 9.1 million people ages 65 years and older were veterans, which represents 23% of the population in that age group. The majority (96%) of these older veterans are men (Wilmoth & London, 2011), but these men’s lives are linked to spouses, children, and grandchildren in meaningful ways. In recent years, the National Institute on Aging and the National Institute on Nursing Research have funded support programs for dementia caregivers in Veterans Administration medical centers (Nichols, Martindale-Adams, Burns, Graney, & Zuber, 2011). As the baby boom generation ages, and Americans in general live longer, the Alzheimer’s Association (2011) projects that larger numbers of older adults will be affected by dementia and other cognitive disorders. It is conceivable that Veterans Health Administration medical centers will see similar increases in the numbers of older veterans affected by cognitive impairments. An increase in the number of veterans with cognitive disorders and dementia will create greater need for home and community-based supportive services, as well as increased need for care and caregiver support in the Veterans Health Administration medical system. Non-Veteran Affairs (VA) programs may also serve a larger number of veterans, who may have different needs and access to different provisions than nonveterans (Wilmoth & London, 2011). For policy and planning purposes, it is important that we develop a better understanding of whether men’s later-life cognition trajectories vary by veteran status.
This research provides some insight into these issues by examining whether cognition trajectories vary between male veterans and nonveterans in the general population. In addition, given the heterogeneity of the veteran population, we examine differences in cognition trajectories between war service veterans and nonwar service veterans, as well as between war veterans who served during WWII only, the Korean War only, and both wars. The models also control for a range of early- and mid- to late-life characteristics to account for selection and mediation to the extent possible given data constraints.
Consistent with previous analyses of cognitive function in the HRS (Brown, 2010), findings indicate that cognitive functioning declines at an increasing rate with age, regardless of veteran status. The findings also affirmatively answer the first research question posed in this study, while providing limited evidence of selection or mediation raised by the second research question. Similar to the findings of Wilmoth et al. (2010) regarding physical health trajectories, we found differences in trajectories of cognitive change between veterans and nonveterans, and among veterans from different periods of war service.
Overall, veterans experience better cognitive functioning relative to nonveterans around retirement age, but decline more rapidly over time, such that cognitive functioning is similar in both groups among the oldest old. The veteran status difference that remains after including controls for early-, mid-, and late-life characteristics implies some protective effect of military service that is not measured in these models. The predicted cognition trajectory of veterans indicates that they may be better off during the first part of later life, but they will experience more rapid cognitive decline as they get older. Among the oldest old, veterans will not have a substantially lesser or greater need for cognition-related long-term support services than the general population.
We found no significant differences between war and nonwar veterans. However, among war veterans, those who served during the Korean War only have lower cognitive scores around retirement age, but less steep age-related declines in cognitive functioning compared with the war service veterans who served during WWII only. Controlling for early- and mid- to late-life characteristics, as well as attrition and mortality, did not attenuate the differences in cognition trajectories among the three different groups of war service veterans. Thus, the long-term support service needs of war service veterans do not appear to be different from the needs of nonwar veterans. There is no significant effect of war service on cognitive function and no difference in the rate of cognitive decline as these veterans age. However, when we consider the differences in cognitive decline between the different groups of war service veterans, we see that the long-term support service needs of war service veterans may differ depending on their period of service. While Korean War veterans are experiencing slightly lower cognitive functioning around retirement age, they do not appear to be on a trajectory of decline that is as steep as the trajectories of veterans from WWII and multiple wars. Given this, Korean veterans may not have the same level of need as we are seeing in WWII veterans today, whereas veterans who have served in multiple wars may have service needs that are more similar to those of WWII veterans. Overall, these analyses demonstrate the utility of making intercohort comparisons, which provide insight into the ways in which differences in life experiences across cohorts shape later-life trajectories.
These results indicate that veteran status is related to later-life cognitive function and decline. Veterans, in general, have better cognitive function than nonveterans. While such a result is consistent with an explanation based on positive selection into military service, the models control for early-life factors, such as child health, socioeconomic disadvantage, and race/ethnicity. Thus, future research that measures other early-life factors that select men into military service and affect later-life cognition is needed to further evaluate the selection hypothesis.
Beyond selection factors, we are also able to control for a large range of potentially mediating variables that affect cognitive function in later life, including a range of mid- to late-life sociodemographic characteristics and health behaviors. These mid- and late-life factors do not explain the differences in cognitive functioning between war service veterans who served during different historical periods. This suggests a long-lasting effect of military service on later-life cognition, which operates through factors and processes that are not included in our models. For example, nationally representative data sets often lack detailed information about military service experiences that could shape later-life cognitive trajectories, such as training received and duties performed, exposure to combat, physical and mental health conditions acquired during service, and service-connected disability ratings. Obtaining a better understanding of the service-related experiences of veterans could shed light onto the extent to which the observed differences in later-life cognitive functioning are directly or indirectly shaped by military service.
The military is an institution that has multiple domains of influence on individual lives, which vary over historical time as the conditions of military service change (Kelty & Segal, 2013). WWII veterans experienced a “citizen’s military” in which service during early adulthood was prevalent among a broad cross-section of men. During the post-WWII period, the military retained a “citizen-solider” quality, although service became less normative. Therefore, veterans from the war and nonwar eras included in this analysis experienced different induction conditions, rates of overseas deployment, exposure to combat, service-related life-course disruption, and access to and use of veteran’s benefits. The influences of these experiences combine in particular ways to generate variation in the effect of military service on cognitive outcomes between veterans who served during different historical time periods.
Although it offers new insights into the factors affecting later-life cognitive trajectories, this analysis is limited to some extent by the constraints of the available data. While we can demonstrate that military service early in life does shape later-life cognitive trajectories, we cannot fully examine the pathways through which military service might influence cognitive functioning in later life. First, the data contain a limited number of measures of early-life circumstances that could have affected selection into the military, as well as later-life cognitive functioning. Also, the HRS does not contain detailed information about military service (such as exposure to combat, overseas deployment, branch of service, rank, training, and duties performed, or the use of various veteran’s benefits after service was completed), which have been shown to be important in other studies of health (Elder et al., 2009; MacLean, 2013).
Second, we were unable to examine cognitive trajectories among Vietnam War veterans because most were not old enough to participate in the cognition portion of the HRS interview. In addition, the HRS does not currently contain a large number of men or women who came of age after 1973. Such veterans served during the “All-Volunteer Force (AVF)” era, which is a historical period when military service became a less-normative part of early adulthood and career service became more common among those who enlisted (Kelty & Segal, 2013). As more Vietnam- and AVF-era veterans become age-qualified for the cognition interviews in the HRS, future waves of the data will include large enough numbers of these groups of veterans to include them in similar models. Future research should include these additional waves of the data to examine whether more-recent cohorts of veterans have different cognitive trajectories, and therefore support service needs, than earlier cohorts.
Third, it is important to acknowledge that part of the observed variation across men who served during different wars might be due to the age window of observation for the cognition trajectories in this analysis. The average age of the Korean War only veterans is substantially younger than that of the WWII only veterans. Over the duration of the study, there is overlap in the ages of these two groups that allows for direct comparisons of trajectories. However, it remains to be seen how the cognition trajectories of the younger members of the sample will progress as they move into the oldest old age range.
Finally, mortality selection may be a concern; the men in this analysis represent a select group who survived to older ages. Thus, our findings are conditioned upon surviving to the age of inclusion in the HRS sample. Although selective survival may be a concern in the present study, it is important to note that the potential influence of selective survival is not unique to our study. It affects all studies that use samples like the HRS, which begin data collection in mid- to late life, to study variation in outcomes across groups with different mortality schedules. To date, this problem has been largely unaddressed due to the lack of statistical procedures for correcting the potential bias generated by this unobserved heterogeneity. Developing such procedures is an important direction for future research (Wolf et al., 2013).
Despite these limitations, this study has many strengths, including the distinctions made between veterans and nonveterans, veterans with and without wartime service, and veterans of different wars, and its use of controls for early-life characteristics and time-varying characteristics during the period of study. It provides detailed information about changes in men’s cognitive functioning during an 11-year period in mid- to late life among individuals whose birth years span more than 50 years of American history and experiences include two major military ventures of the mid-20th century: WWII and the Korean War. Our findings contribute to our understanding of how early-life social and institutional factors shape cognitive function in later life, while also providing specific, new insights regarding how men’s later-life cognitive trajectories, and their potential need for long-term support services, vary in relation to military service.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institute on Aging (Grant 5R01AG028480, Principal Investigator: Janet M. Wilmoth).