
Abstract
Close relationships are often beneficial for health. They provide emotional support that buffers negative effects of stress as well as instrumental support that positively influences health behaviors (Cohen, 2004). They offer physical intimacy (Stadler, Snyder, Horn, Shrout, & Bolger, 2012), a sense of belonging, and a reason to live (House, Robbins, & Metzner, 1982). Marriage, the central close relationship for most adults, is a strong predictor of life satisfaction and longevity (Wilson & Oswald, 2005), with marriage becoming increasingly important and adaptive in late life (Carstensen, Gottman, & Levenson, 1995; Levenson, Carstensen, & Gottman, 1994). Despite their well-established benefits, close relationships including marriage can also be stressful and negatively affect health (Robles & Kiecolt-Glaser, 2003). For example, within marriage, interpersonal stressors, stressors that involve close relationships such as conflict and bereavement, have been shown to negatively affect a person’s psychological and physical health (Bolger, DeLongis, Kessler, & Schilling, 1989; Monin & Schulz, 2009; Robles & Kiecolt-Glaser, 2003; Stroebe, Schut, & Stroebe, 2007). At the same time, there is a literature showing gender differences in reactivity to interpersonal stressors, such that women are more affected by interpersonal stress than men (Kiecolt-Glaser & Newton, 2001; Monin & Clark, 2011; Wanic & Kulik, 2011). What is not known is how both older adult men and women are affected by their partners’ interpersonal stress and suffering.
In the present study, we used mixed methods to examine older adults’ verbal accounts of an instance when their spouse was suffering. We were interested in the extent to which talking about a partner’s suffering that is interpersonal in nature (e.g., social conflict, death, or separation from a family member) rather than intrapersonal (e.g., chronic pain, loss of a job) is associated with increased reactivity. Moreover, we were interested in exploring the gender differences in this process for husbands and wives.
Reactivity to a Spouse’s Interpersonal Versus Intrapersonal Stress
Although all types of stressors are likely to spill over to close relationship partners, for instance through emotional contagion (Hatfield, Cacioppo, & Rapson, 1993; Monin & Schulz, 2009), interpersonal stressors may be especially stressful because spouses are likely to experience many of the same interpersonal stressors together in their marriage (e.g., marital conflict) and in their family (e.g., death of a relative). This means that one person’s stress is also the other person’s direct stress. For example, it is likely that if one partner is stressed about their marriage, the other person is as well (Bolger et al., 1989). Studies show that marriage problems can lead to excessive sympathetic arousal as evidenced by increased blood pressure (BP) and heart rate and negative long-term outcomes including coronary events and mortality for both partners in the relationship (Kiecolt-Glaser et al., 1993; Robles & Kiecolt-Glaser, 2003). Although older adults are shown to respond more adaptively to marital conflict and stressors (Carstensen et al., 1995), other types of interpersonal stressors outside the marriage affecting either spouse could potentially be distressing, especially when they involve those in close relationships because according to socioemotional selectivity theory, older adults tend to focus and place value on their close relationships (Carstensen, 1995).
Loss of a friend, family member or loved one represents another common type of interpersonal stressor in older adulthood that is likely to be shared between spouses, even when this loss affects one spouse more than the other. This reasoning fits with family systems theory, which emphasizes that grief is shaped by one’s social context and family members are likely very attuned to each other’s grief processes (Rosenblatt, 1988). In addition, it may be that psychological or existential suffering due to the loss of a family member is a particularly salient and distressing concern for older adult spouses compared with other intrapersonal types of suffering (e.g., coping with a chronic condition, losing a job). Spouses may have more difficulty supporting their partners with bereavement than with other stressful circumstances especially when the person who is bereaved is having difficulty dealing with the loss (Gilbert, 1989). It may also be the case that issues of mortality elicit existential concerns for both partners (Fry, 2001).
Little is known about how partners may perceive and experience their partners’ interpersonal suffering. Although past research has shown that interpersonal stress and suffering is linked to poor health of an individual (Bolger et al., 1989), it is unclear how this affects their close relationship partners. We hypothesize that, when older adult spouses talk about their partner’s experiences of suffering, spouses who emphasize their partner’s interpersonal suffering, compared with other more individualistic and intrapersonal types of suffering, will experience greater cardiovascular and emotional reactivity (Hypothesis 1).
We examine cardiovascular reactivity, an important measure of emotional distress that is particularly relevant to the health of older adults. Emotional distress is known to increase cardiovascular reactivity, and over time, risk for cardiovascular disease (Monin et al., 2010). We examine cardiovascular reactivity as measured by changes in BP. In a review of the literature, Chida and Steptoe (2010) showed that systolic BP (SBP) and diastolic BP (DBP) reactivity are both associated with increased risk of cardiovascular disease. Specific mechanisms for this are increased carotid intima-media thickness (IMT) and hypertension (both risk factors for cardiovascular disease). This has been found in both men and women and in older adults (Chida & Steptoe, 2010; Jennings et al., 2004; Matthews, Woodall, & Allen, 1993; Menkes et al., 1989).
Gender Differences
It is also well established that interpersonal stressors affect men and women differently. Men seem to benefit from close relationships more than women regardless of quality, whereas women are more sensitive to and differentially affected by the quality of their relationships (Cohen, 2004). In addition, relationship stressors pose a greater risk to women, who are generally more responsive to interpersonal conflict and social rejection. For example, in a laboratory experiment, faced with a social rejection challenge (social isolation by trained confederates), women showed more reactivity than their male counterparts who responded more to achievement tasks (Stroud, Salovey, & Epel, 2002). Although a recent meta-analysis shows that women have the same level of satisfaction as men in their marriages overall (Jackson, Miller, Oka, & Henry, 2014), women are generally more responsive to marital conflict than men are as evidenced by greater physiological reactivity (Kiecolt-Glaser & Newton, 2001; Monin & Clark, 2011; Wanic & Kulik, 2011). Relationship interdependence theory suggests this can occur because gender socialization encourages women to take on the role of caregivers and nurturers, and consequently women are more attuned to others’ emotions and better at empathizing (Kiecolt-Glaser & Newton, 2001).
Women’s interpersonal tendencies would suggest that they are more likely than men to focus on interpersonal stressors. Gender role theory suggests that women are viewed as being more concerned with relationships than men (Helgeson, 1994). What is unknown, however, is how this affects their husbands. Are husbands attuned to their wives’ interpersonal stressors? In other words, are husbands more likely to describe their spouses’ suffering as interpersonal compared with wives? Do these interpersonal stressors also have an impact on husbands’ reactivity? We hypothesize that older adult men are more likely to describe their wives’ experiences of suffering as interpersonal (e.g., involving their marriage or family members) compared with women describing their husbands’ experiences of suffering as interpersonal (Hypothesis 2). Moreover, according to the theory of gender role strain (Pleck, 1995), it could be the case that men who are more interpersonal, conflicting with gender norms, may experience discrepancy strain and thus may be particularly vulnerable to their partner’s interpersonal suffering. Therefore, we also explore whether men who talk about their spouses’ suffering as interpersonal are more physiologically reactive than women who talk about their spouses’ suffering as interpersonal.
The present study examines individuals’ accounts of their partners’ suffering to compare the effects of their interpersonal and intrapersonal suffering. We are interested in the content of the account as reflective of the extent to which the participant focuses on relationships. Using quantitative analysis to examine associations between gender, interpersonal focus, and reactivity, we operationalized interpersonal focus with use of social and family-oriented words using a linguistic analysis program, and we coded speeches for interpersonal versus intrapersonal topics, and examined their effects on individuals’ emotional and physiological reactivity when describing their partners’ suffering. We expanded on our results with inductive qualitative analysis (beyond the dichotomous coding of interpersonal vs. intrapersonal) to explore the potential mechanisms behind our quantitative findings.
Method
Participants
The present study analyzed data from a multi-method study that examined how providing social support influenced cardiovascular reactivity to a spouse’s suffering for the support provider. Seventy-seven individuals with a self-reported musculoskeletal condition (IMCs; i.e., osteoarthritis, lower back pain) and their heterosexual spouses were recruited from newspaper advertisements and community bulletins. Eligibility criteria were as follows: (a) The IMC had to be more than 50 years old, (b) the couple had to be married or in a marriage-like relationship and live together for at least 6 months, (c) the spouse could not have a musculoskeletal condition, and (d) if the spouse had another chronic condition that caused pain, the spouse had to have less pain on average than the IMC. Three of the spouses indicated at the lab session that they had osteoarthritis or lower back pain. Excluding them from analysis did not change the results. Participants also completed the Short Portable Mental Status Questionnaire—Mini-Mental State Examination (SPMSQ; Pfeiffer, 1975), to evaluate their cognitive functioning, and those who correctly answered at least 7 out of 10 items were considered to be eligible for the study. Spouses who were taking beta-blockers, a class of drug affecting heart rate, were excluded because of the aims of the parent study.
Forty-five of the spouses were male and 32 were female. The mean age of the male spouses was 64.91 (SD = 8.57) and of the female spouses 62.06 (SD = 7.82). Most spouses were White (100% of wives and 91.1% of husbands). Spouses were highly educated, with 62.5% of wives and 68.8% of husbands having completed at least some college. Couples reported being married an average of 31.05 years (SD = 16.37). Seventy-seven percent of couples had children. Household income was such that 48% reported earning less than US$50,000, 42% reported earning US$50,000 to US$99,999, and 10% reported earning more than US$100,000.
IMCs reported that they had been experiencing chronic pain from a musculoskeletal condition for 123.77 months on average (SD = 129.79, range = 0-636). Sixty-seven (87.01%) IMCs reported that they had been suffering from osteoarthritis in at least 1 location. Fifty (64.90%) reported arthritis in a second location. Twenty-nine (38%) reported their primary site of pain to be knees, 12 (18%) back, 10 (13%) feet or ankles, 7 (10.4%) hips, 7 (10.4%) hands/fingers, and 2 (3%) shoulders. The remaining participants reported having lower back pain without arthritis.
Procedure
Spouses first sat quietly for a 3-min period while their BP was monitored continuously to yield baseline cardiovascular measurements. Spouses then provided baseline self-reported emotions of distress. Next, spouses’ BP was monitored as they watched their partner complete a pain-eliciting household task in which the partner carried 10 pounds of groceries for a 3-min period. Then spouses’ BP was measured again as they provided verbal accounts about a time at which their partners suffered. Emotions were self-reported after each task.
Verbal accounts of partners’ suffering
The verbal account was preceded by a 3-min period during which speakers were asked to think about what they were going to say to ensure reactivity during the verbal account was not an artifact of the act of speaking. Spouses were asked to think about a time their partners were suffering (i.e., what was happening, where they were). The researchers described suffering as “physical discomfort or experiencing pain, feeling psychologically distressed, or upset about the meaning or purpose of life,” and told participants to focus on their partners’ suffering and not any social support they provided. The thinking period was followed by a 3-min verbal account in which they described the incident and were video recorded.
Of the 77 speeches, 76 were included for analysis; 1 was excluded because of a recording error. At the end of the study, participants completed a background interview assessing characteristics of the spouses (i.e., gender, age, education, income, and ethnicity). In the present study, we limit our analysis to the measures taken during the baseline period and during the suffering speech as well the data from the background interview. From this point on, we will refer to the IMC as the “partners” and their spouses as the “speakers.”
Measures
Interpersonal language
Speakers’ recorded speeches were transcribed. The Linguistic Inquiry and Word Count (LIWC) text analysis program (Pennebaker, Mayne, & Francis, 1997) was used to examine the extent to which participants used interpersonal language in their speeches describing suffering, including social and family-oriented words, which could indicate a greater focus on relationships. Family words (e.g., father, sister, aunt) was a subcategory of social words (e.g., talk, they, child). The family and social word categories were used to test the hypotheses that men would use more interpersonal words to describe their partners, and that those using more interpersonal words would show greater physiological and emotional reactivity. The LIWC, which counts the use of words associated with various meanings, has been evidenced as a reliable and valid tool to help evaluate the meaning of language (Pennebaker et al., 1997; Pennebaker, Chung, Ireland, Gonzales, & Booth, 2007).
Interpersonal themes
In addition to the LIWC analyses, two independent coders categorized the content of the speeches as either interpersonal or intrapersonal by identifying themes of the overall stressor the speaker described. For example, the coder indicated the stressor was interpersonal if it dealt with the death of a family member or a conflict between spouses. In contrast, other intrapersonal episodes of suffering focused more on the self, for example, a heart attack or a loss of job. Of the speeches (n = 76), 22 focused on interpersonal themes, whereas 54 focused on other intrapersonal episodes of suffering. There was 100% intercoder agreement. This variable was used in our quantitative analysis.
BP reactivity
The speaker’s sitting SBP and DBP were measured at baseline and during the speech. Three readings were taken during each period, and the means for each period were calculated. In our analysis, we used raw scores for BP during the speech as the outcome, controlling for baseline BP.
Emotional reactivity
At the beginning of the lab session (baseline) and immediately following the speeches, speakers rated their felt emotions on a seven-point Likert-type scale ranging from (1) “not at all” to (7) “extremely” (Eisenberg et al., 1989). For the present study, we were specifically interested in adjectives representing distress: “disturbed,” “uneasy,” and “distressed” (α = .85). The mean rating for distress was 3.51 (SD = 1.80, range = 1.00-7.00).
Statistical Analysis
Correlation analyses were completed to examine potential covariates with gender as well as word use and use of interpersonal themes in the spouses’ speeches. We also examined associations between self-reported distress and BP measures.
To test the hypothesis that speaking about a partners’ interpersonal suffering would be associated with greater cardiovascular and emotional reactivity as compared with speaking about intrapersonal suffering (Hypothesis 1), we conducted multivariate linear regressions for each of the language and theme variables (i.e., family and social words and interpersonal topics). The models each included one of the language or theme variables, with word count and gender as covariates, to predict cardiovascular outcomes (SBP and DBP) as well as self-reported distress. Baseline measures of the outcome variables were also included in the models.
We then conducted a multiple linear regression analysis to test the hypothesis that male speakers would use more social and family words and interpersonal themes in describing their wives’ suffering (Hypothesis 2). To explore whether more interpersonal men or women would differ in terms of reactivity, we also examined the effects of the interaction between gender and each interpersonal variable (e.g., family words) on reactivity in the regression models. Finally, to examine potential clinical significance of the BP reactivity, we conducted a follow-up analysis in which we calculated mean changes in SBP and DBP from baseline to the speaking period. We report the mean increases separately for speakers who used interpersonal themes versus intrapersonal themes. We also report the mean BP change scores separately for speakers who used high amounts of social and family words and speakers who used low amounts of social and family words. High and low groups were generated with median-splits. We evaluate the potential significance of the means based on past studies showing scores that predict clinical outcomes (Jennings et al., 2004).
A Qualitative Exploration of Interpersonal Suffering
We went into greater depth to examine how speakers talked about interpersonal suffering and to better understand the processes through which interpersonal suffering of one spouse might be experienced by the other spouse, with implications for health. Through repeated reading of speech transcripts and careful line-by-line analysis, we identified salient themes related to interpersonal suffering. We used coding procedures with ATLAS.ti (2008) to identify examples of these themes in our data and then closely examined coded data to identify the dimensions of these themes.
Quantitative Results
Preliminary analysis
See Table 1 for average use of each word type. Correlational analyses revealed that for gender, there was a significant association with age, with male speakers more likely to be older (see Table 2). There was also a significant association between gender and education, with female partners more likely to have achieved higher levels of education. We also found that male speakers were more likely to be retired, χ2 = 4.01, p < .05.
LIWC Results for Word Use.
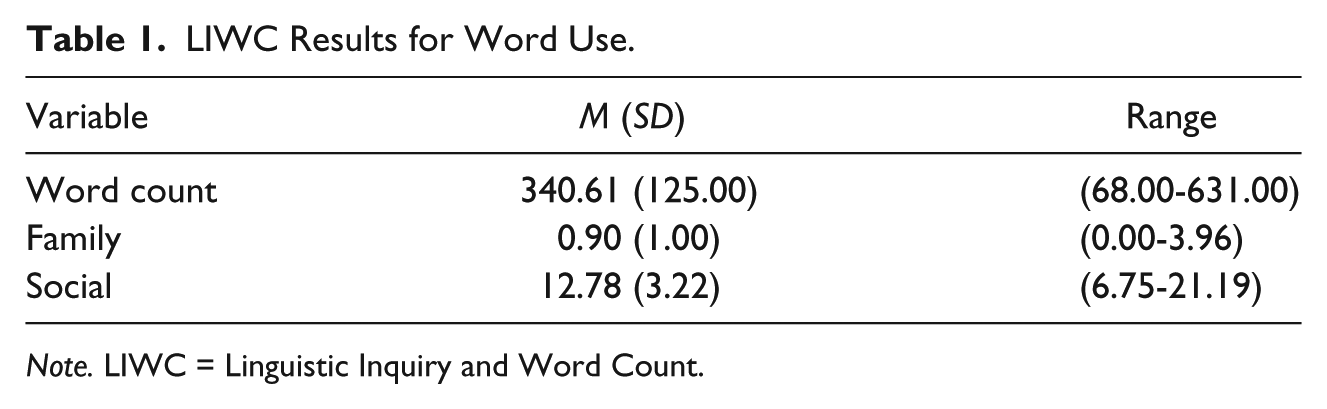
Note. LIWC = Linguistic Inquiry and Word Count.
Intercorrelations Among Word Use and Socio-Demographic Variables.
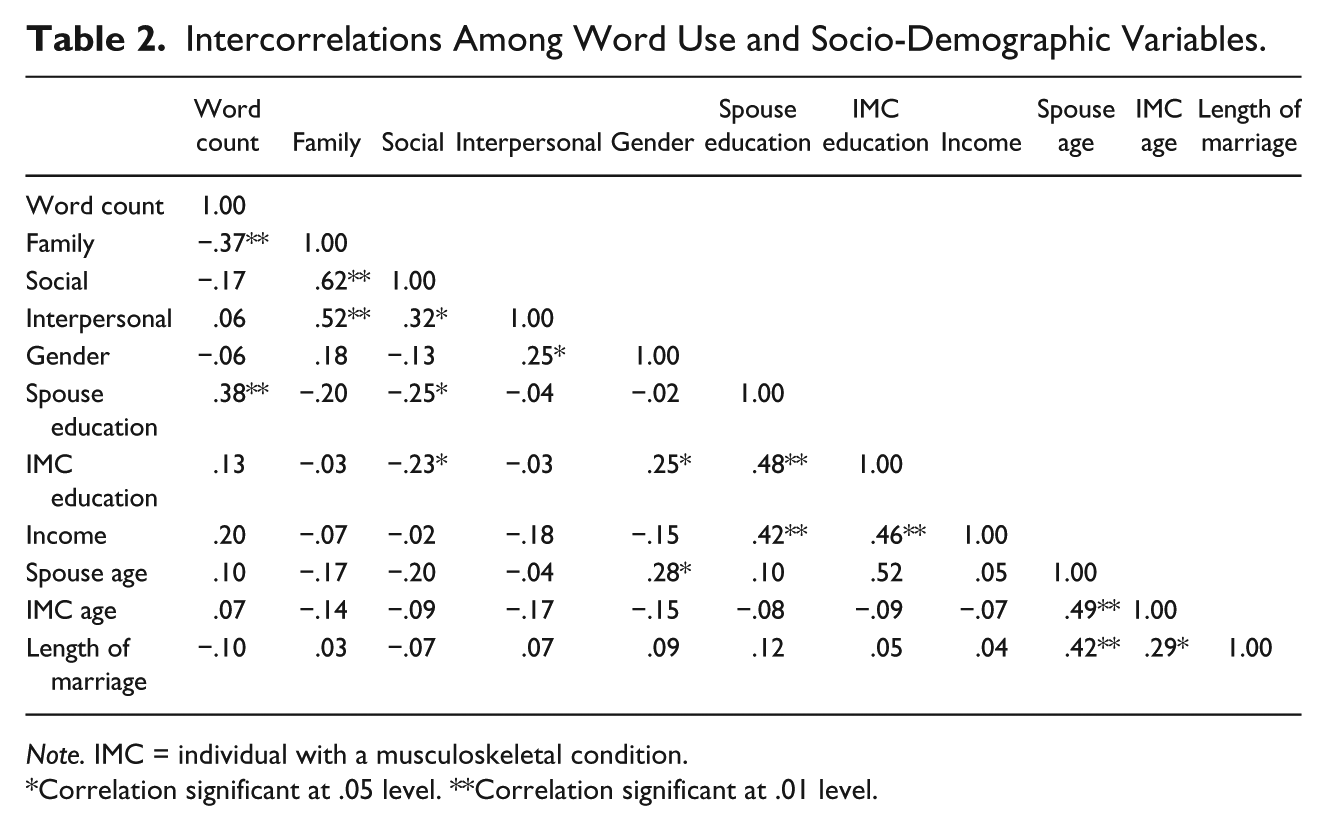
Note. IMC = individual with a musculoskeletal condition.
Correlation significant at .05 level. **Correlation significant at .01 level.
For word use, use of social words was negatively associated with both speaker and partner education. The three interpersonal predictors (interpersonal theme, social words, and family words) were significantly correlated with each other. Finally, use of family words was positively associated with word count (see Table 2). We adjusted for all of these significant covariates in our analyses.
Multiple linear regression analyses including the significant covariates were conducted to test the hypothesis that describing a partner’s incident of suffering as interpersonal was associated with greater cardiovascular reactivity (SBP and DBP) and distress (see Table 3) than talking about intrapersonal suffering. Specifically, we entered gender, the outcome as measured at baseline (e.g., baseline SBP, DBP, or distress), word count, and one of each language or word variables (e.g., interpersonal theme, social words, and family words) predicting each of the outcomes (e.g., speech SBP, DBP, or distress) in separate models. We entered the three interpersonal predictors (interpersonal theme, social words, and family words) separately in the models because of multicollinearity. Consistent with the hypothesis, results indicated that interpersonal themes and family word use were directly related to SBP reactivity. However, these effects were not significant for DBP or self-reported distress, and the broader category of social word use was not significantly linked with the reactivity measures.
Multiple Regression Models Predicting BP and Emotional Distress.
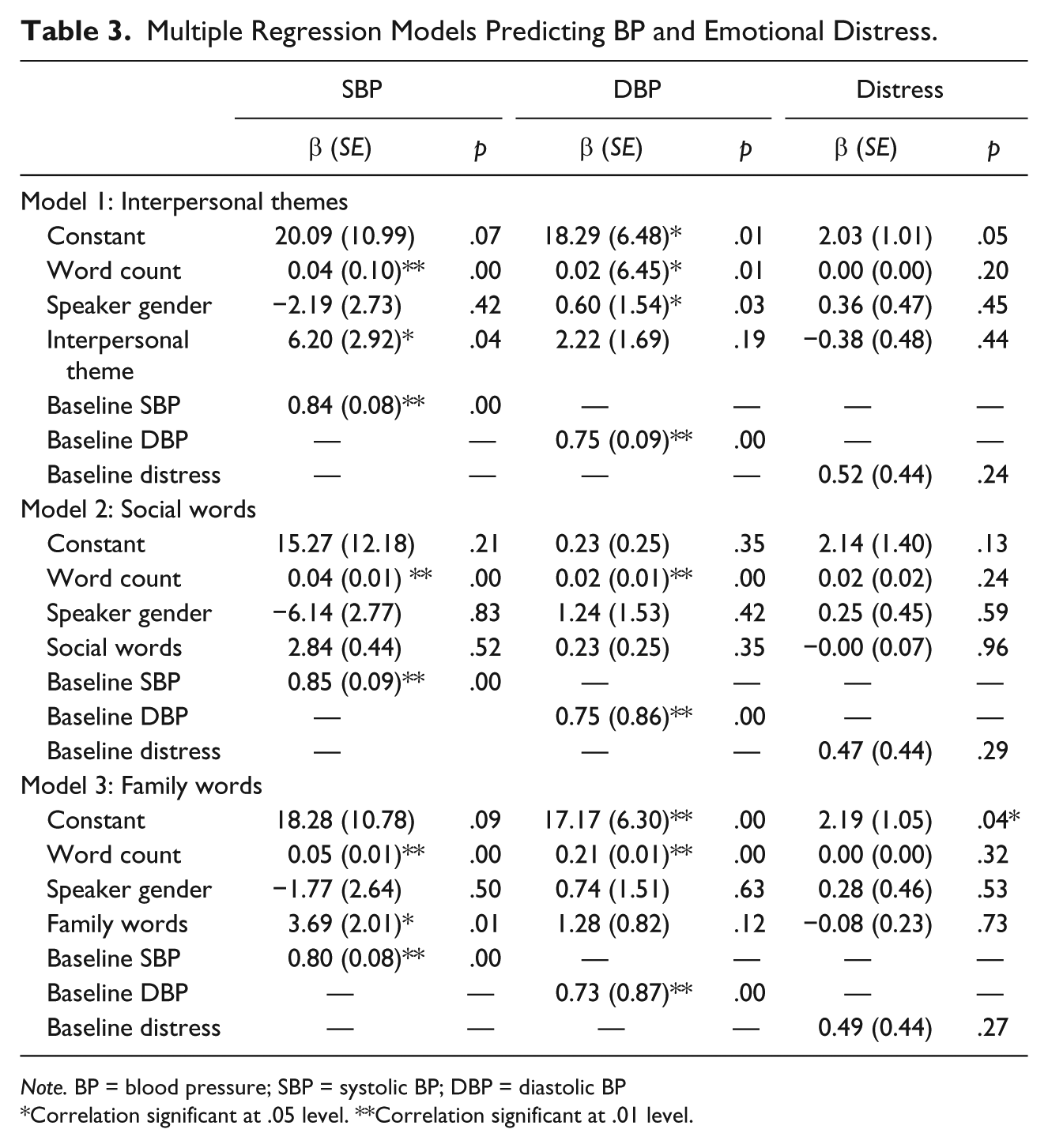
Note. BP = blood pressure; SBP = systolic BP; DBP = diastolic BP
Correlation significant at .05 level. **Correlation significant at .01 level.
A chi-square analysis revealed that male speakers used more interpersonal themes than female speakers in describing their spouses’ stress (χ2 = 4.77, p < .05). Multiple linear regression analyses including the significant covariates gender, speaker age, speaker retirement, speaker employment status, and partner education showed a significant association between gender and family words; β = .52, SE = 0.26, t(76) = 2.03, p < .05; with husbands more likely to use family words in describing their wives’ suffering than wives were in describing their husbands’.
Exploratory analysis of gender differences in the associations between interpersonal words and reactivity
For an exploratory analysis, we also examined the effects of the interaction terms for gender and social words, family words, and interpersonal codes separately predicting BP and self-reported distress in each of the regression models. There were no significant interaction effects suggesting that men and women are equally affected by suffering of spouses.
Clinical Significance of BP Reactivity
For those using interpersonal themes, the mean increase in SBP was 15.52 mmHg and 7.3 mmHg for DBP compared with 10.86 mmHg and 6.27 mmHg in those using intrapersonal themes. For those using high social words, mean increases were 12.58 mmHg and 7.50 mmHg for SBP and DBP, respectively, compared with 12.01 mmHg and 5.63 mmHg in the low social word group. Finally, the mean increases for those with high family word use were 11.31 mmHg and 6.32 mmHg for SBP and DBP, respectively, compared with 13.48 mmHg and 6.91 mmHg in those with low family word use. The larger BP increases in the low family word group is due to the fact that those who used less family words tended to speak much less (word count of 368 compared with 295 for high family). This is why we controlled for word count in our primary analysis.
Qualitative Results
To understand why accounts of interpersonal suffering were associated with greater cardiovascular reactivity, we conducted qualitative analysis of the verbal accounts describing relationship-focused suffering. Of these 22 speeches, 16 of the speeches were provided by men. Ten of the 22 speeches (8 by men) directly pertained to death and/or bereavement. Other topics described by both men and women included a conflict with a mother, an argument between spouses, a child moving away, and a daughter-in-law suffering third-degree burns. In further analysis of the speeches, we identified two distinct patterns in the way participants spoke about their partners’ interpersonal-focused suffering: suffering together and empathy for psychological suffering associated with loss.
Suffering together
Several partners described events that were potentially equally impactful for both of them. This is something unique to an interpersonal stressor as, for example, two people can be equivalently affected by the death of a child. In these cases, suffering was described as a shared experience, with participants not differentiating their partners’ pain from their own. One participant described the death of his wife’s father (and specifically her personal suffering) as the hardest part of their marriage for both of them.
That was the hardest part of our marriage because she missed her father, because she had her father for all of her life—70 years, and we went through hard times then because she was feeling physically and emotionally drained of the death of her father, so we, you know, just were feeling very distraught about it. (Participant 73, husband)
He discussed the stress that his wife experienced, but quickly shifted to using the collective “we,” indicating that her suffering was a shared experience.
Shared suffering in the interpersonal context is not just emotional, but also physical. Another participant described how this shared emotional suffering could be embodied to produce physical exhaustion. When describing his wife’s suffering after the death of her mother, he said, Both of us were uh physically drained by the time we got through with the day and my mother-in-law was moved to hospice and it was about two days later that she had passed away but we thought we did everything we could do to make her comfortable. (Participant 68, husband)
In one example, a wife described her husbands’ stress after he unsuccessfully attempted to save a neighbor’s life. She at first described her husband as “emotionally upset,” and “physically, just drained,” stating that she “was feeling very bad for him,” but then she shifted to presenting it as something they were both experiencing: And, uh, about a week later, they came over to thank my husband in person, and they brought pastries, which I thought were very nice. So, uh, it wasn’t a total loss because when they thanked us, we felt great. And that’s it. (Participant 38, wife)
This is another example, in which a spouse described an interpersonal event as a collective experience of suffering; however, in this example, the event is not something that she experienced independently or directly, but rather something she felt because of her close relationship to the person experiencing it.
Empathy for loss
One thing that is so stressful about interpersonal suffering in late life is that it is so often related to loss. Almost half of the interpersonal speeches were about death. Loss may be especially distressing because not only do people face the stressor itself but they may confront their own mortality and grapple with existential questions.
These events entail empathy as well as shared suffering. Loss is one example where the stressor usually affects both spouses in their own ways. Even if the deceased person was an in-law, the speakers still had their own relationship with them. One participant described his wife’s stress surrounding the death of his brother-in-law.
I felt sad that—because I liked her brother very much, and he was a fantastic person. So, um, she was she was just overwhelmed and upset that she didn’t have a chance to say goodbye, and wished he had lived a lot longer. (Participant 15, husband)
He described both his own sadness and his wife’s emotional suffering after losing her brother.
One participant talked about the loss of a son, and how it affected both her and her husband, but noted that her husband was particularly affected.
. . . the way I was feeling was just sad from this horrific event in our lives. But I was working, and so I was able to go out . . . I had an emotional respite from grieving. But my husband was engulfed in it. (Participant 10, wife)
The speaker’s concerns were twofold, as she shared the same grief as her husband in the face of the loss, yet she was also closely attuned to her husbands’ severe distress.
Incidences of loss were also particularly troubling for speakers because they led to the speakers’ facing more existential questions and dealing with their emotions around death in general.
I wasn’t feeling that good either because I knew she was very close with her mother and uh, to have her mother go that quick to see her one day and the next day she was gone, it’s tough. (Participant 65, husband)
This speaker was empathetic because he understood his wife had a close relationship with his mother, but he also spoke generally about the pain associated with recognizing the impermanence of life.
Another speaker described how when her mother died, her husband’s stress was manifested in physical pain. She suggested that this had a lot to do with the stress of being reminded of his mortality.
We had lost his mom and dad a while ago, but I think this was coming to mind . . . that his parents were gone, now my mom was gone, and just kinda remind you of your mortality. You know, thinking about how he was going to take care of himself, and take care of us—my daughter and me, and if this pain was something that was serious would he be alright or was he going to have to be hospitalized? (Participant 74, wife)
It is notable that this population of older adults so frequently chose to refer to a period of loss when describing an incident of suffering. This might be an indication that they are at a stage of life where death is a more common experience, and they may be more aware of issues of mortality.
These verbal accounts revealed that participants were inclined to describe their partners’ interpersonal suffering as entangled, shared suffering between both partners. There was also much emphasis on a spouses’ suffering in the wake of the death of a loved one, perhaps because loss is a suffering experience of great relevance to this older study population who may be faced with more reminders of mortality (Fry, 2001). Marital conflict was emphasized less. This could be due to the nature of our particular sample; however, it is also consistent with research showing that older couples tend to experience less conflict (e.g., Carstensen et al., 1995) and are better at dealing with interpersonal problem solving than younger adults (e.g., Blanchard-Fields, Mienaltowski, & Baldi Seay, 2007).
Discussion
As we expected, talking about a spouse’s interpersonal stressors was associated with greater reactivity than talking about intrapersonal stressors in both husbands and wives as evidenced by elevated SBP. These results are supported by emotional contagion theory (Hatfield et al., 1993), which suggests that stress and suffering is a shared experience in close relationships, especially among older adults who provide support to a loved one with a chronic condition (Monin & Schulz, 2009). However, our results extend this notion further to suggest that interpersonal suffering, suffering that stems from relationships both inside and outside the marriage, is particularly distressing for older adult spouses. Not only do interpersonal stressors affect individuals, but they also affect their spouses more than other types of suffering. Moreover, these results support the idea that close relationships remain important as both men and women age, according to socioemotional selectivity theory (Carstensen, 1995) and more recent research suggesting that older adults continue to be engaged with their close social networks (Cornwell & Laumann, 2015; Cornwell, Laumann, & Schumm, 2008).
Through in-depth analysis of the verbal accounts of a partner’s suffering, we were able to identify some of the mechanisms for the stress associated with focusing on a spouse’s interpersonal suffering. Individuals discussed their feelings of shared suffering, in which they did not differentiate their partners’ and their own stress during the event. One of the reasons spouses may suffer from their partners’ interpersonal suffering is because they go through the experience together. For example, when something goes wrong with a child, because it is both partners’ child, it is directly meaningful for both partners. In essence, when a person is asked to describe their partner’s suffering, they are also discussing their own suffering. It is also noteworthy that so many participants chose to describe an episode of loss when simply directed to describe a time their partners were suffering. These experiences exemplified shared suffering, as partners often lost a person to whom both spouses were close. Furthermore, even in cases in which the speakers were less close with the deceased, watching their partners suffer beside them may have triggered existential suffering in the speakers themselves. In this sample, marital conflict or conflict with other family members was not as frequently described as an experience of suffering, and shared bereavement was a much more prominent theme.
However, reactivity in the case of a partner’s bereavement could be due to empathy even in the cases in which speakers were not grieving themselves. For example, Participant 30 discussed his wife’s sister’s death as the overall stressor stating, “I did not know her sister personally, so I’m a little detached at some points. But as far as what she’s feeling, you know, I relate to.” This event affected him only because of his empathy for his spouse. Another speaker (25) described his empathy: I was crushed because, as bad as I felt about the situation, I was worried about her. She has gone through so much in the past three years, from cancer, to losing to her sister, to her best friend, to her nephew committing suicide, and then this.
These were both instances in which the partners’ suffering is separate yet the speakers are affected by it. Thus, empathy by itself can be a mechanism for reactivity to a partner’s interpersonal suffering. However, it is important to make the distinction between empathy and shared suffering. Whereas empathy often occurs in reaction to both intrapersonal and interpersonal partner suffering, shared suffering may be more specific to partner interpersonal suffering.
Previous literature on interpersonal stress that has primarily focused on marital conflict has established its negative effects on women (Robles & Kiecolt-Glaser, 2003) even in later life (Heffner et al., 2006). Our findings suggest that like their wives, husbands are distressed by interpersonal suffering when they perceive how it affects their partners. This supports newer research suggesting that gender differences in interpersonal processes may not be so prominent (Jackson et al., 2014). In addition, as our qualitative findings suggest, it may also be that the stress may stem more from the death of a loved one rather than other forms of interpersonal stress such as conflict. Although we did not find that more interpersonal-focused men are more reactive, our findings suggest that men are equally as affected as wives by their partner’s interpersonal stress. This is important because men will be particularly affected by these phenomena, as we found that men are more likely to view their wives’ suffering as interpersonal. Although past research shows that women are at heightened risk for stress from interpersonal stressors (Ewart, Taylor, Kraemer, & Agras, 1991; Robles & Kiecolt-Glaser, 2003), our findings take this a step further, showing that husbands are also aware of this and that it has negative consequences for their own cardiovascular health.
It should also be noted that men and women might think about their partner’s suffering differently, as evidenced by husbands reporting that their wives’ suffering was more often interpersonal. When asked to talk about their partner’s suffering, women may focus primarily on their partners’ distress and less on themselves, whereas men may think about how they were also involved in the incidents. In other words, it could be that husbands’ accounts of their wives suffering were influenced by husbands’ agency to some extent as well as reflecting their wives’ communion (Diehl, Owen, & Youngblade, 2004).
The use of BP as a measure of reactivity yields important clinical significance. Several studies have identified SBP and DBP reactivity to stress (e.g., cold pressor tasks) as predictive of hypertensive status at upward of 20 years follow-up (Armario et al., 2003; Carroll, Smith, Sheffield, Shipley, & Marmot, 1995; Matthews et al., 1993; Menkes et al., 1989). Although past research typically described a linear relationship between reactivity to stressful tasks (e.g., cold pressor, video game, mental math) and hypertension, previous studies have established a normative mean increase of 11.4 mmHg for SBP and 10.6 mmHg for DBP for cold pressor tasks (Hines & Brown, 1936). Our findings suggest mean changes in SBP for those with high social words (12.58 mmHg) and those using interpersonal themes (15.52 mmHg) exceed normative means. Furthermore, Jennings et al. (2004) established that every SBP increase of 7mm in response to mental stress was associated with a .035 mm increase in carotid IMT (a preclinical measure of heart disease). As a .03 mm per year increase in carotid IMT thickness was associated with risk for myocardial infarction or coronary death (Hodis et al., 1998), these increases are suggestive of clinically significant risk.
Strengths and Limitations
This study is novel in that it used both objective linguistic markers for the interpersonal content of the speeches as well as an overall code for interpersonal context and in-depth qualitative analysis to further examine the potential mechanisms for our findings. We also used both objective and subjective measures of stress through cardiovascular measurements as well as self-report. Also, this study population included IMC (osteoarthritis or lower back pain) and their spouses, which has implications for the study conclusions. For example, spouses were describing suffering of their partners with musculoskeletal conditions, who are faced with physical pain on a regular basis. Although this may have led to more of a focus on individualistic suffering experiences (e.g., physical pain from osteoarthritis), it is notable that many of their spouses chose to discuss interpersonal incidents, and were more affected by them.
There were a few limitations. The sample was almost entirely White, and a more diverse sample may have revealed cultural differences in perceptions of suffering and partners’ reactivity to it. Because the data were cross-sectional, we could not capture how experiences may change over time. In addition, in the qualitative analysis, we were unable to compare the relationship-focused speeches of men and women because of the limited number of relationship-focused speeches by women. Also, our cardiovascular findings were specific to increased SBP reactivity. SBP reactivity has been most consistently identified as strongly associated with cardiovascular outcomes (Izzo, Levy, & Black, 2000; Chida & Steptoe, 2010; Jennings et al., 2004). Nonetheless, future research should replicate the physiological effects across multiple measures (e.g., heart rate, pre-ejection period, heart rate variability). Finally, we did not find that participants reported feeling more subjectively distressed by partner’s interpersonal suffering although they were more physiologically reactive. This is common in emotion studies, where physiological measures are distinct from subjective experiences (Mauss, Levenson, McCarter, Wilhelm, & Gross, 2005), and may suggest that spouses are unaware of the impact that interpersonal events have on them. This may be especially the case for men who are less likely to report vulnerability. However, this discrepancy could also be a result of the time course of the reaction, as participants completed their subjective measures of distress after the speech whereas BP was assessed during the speech. BP readings may have represented the immediate response whereas the reports of distress were lagged.
Implications
Although many of the partners with musculoskeletal conditions did not require caretaking from their spouses, our study results have implications for informal caregiving relationships in older adults. They suggest that male caregivers may experience the stress of their role differently. The fact that men talked more about interpersonal stressors suggests that they may be particularly attuned to their wives’ interpersonal suffering, and this may affect the type of care they provide. As the gender gap narrows for older adult caregiving couples such that men are more often providing care to their spouses (Robinson, Bottorff, Pesut, Oliffe, & Tomlinson, 2014), it is important to understand the gender differences in how spouses’ perceptions of their partners’ suffering affect them.
Because we found that both husbands and wives are affected by their partners’ interpersonal suffering, this underscores the importance of examining couples as a whole. Therefore, interventions that help and empower people to cope with stress as well as grief should include both husbands and wives (Martire, Schulz, Helgeson, & Small, 2010). Our findings also suggest that dyadic interventions that emphasize communal coping (Lyons, Mickelson, Sullivan, & Coyne, 1998) are likely to help older adults deal with increasing individual and shared stressors such as chronic disease through social support.
Conclusion
These results add to the existing literature on social relationships and late life marriage and health by showing that not only do interpersonal stressors affect individuals but also their close relationship partners. This is the first study to our knowledge that reveals husbands as attuned to their wives’ experiences of suffering as more interpersonal, and to show that both husbands and wives are more reactive when their spouses undergo interpersonal rather than intrapersonal distress. Understanding the interpersonal processes of stress in close relationships among older adults will be enhanced by a more informed knowledge of the types of stressors that cause emotional understanding of interpersonal suffering, so future research is necessary to further explore how this may pose risks to both older men and women. Our mixed-methods approach examining older couples allowed us to reveal the layers of impact of one’s interpersonal stress, as well as some of the mechanisms for a partner’s reaction to it. Couples studies involving older adults are particularly important and necessary in identifying and addressing how people experience and cope with stressors that often become more frequent as people age.
Footnotes
Acknowledgements
We would like to thank Jordana Confino for her assistance with transcription.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding sources include a career development award to Joan Monin from the National Institute on Aging, National Institutes of Health (K01 AG042450-01A1), and an award from Yale’s Pepper Center (P30AG021342), and an award to Becca Levy from the National Institute on Aging (R01 AG032284).