
Abstract
Although the association between education and health is one of the most powerful and robust relationships discovered in social science (Lynch, 2003; Mirowsky & Ross, 2003a), it is also one of the most difficult relationships to explain (Lynch, 2003). Questions such as how education links to health in the non-Western context and who has benefited more from education have not been fully answered. This study aims to examine whether and how education is associated with psychological distress both cross-sectionally and longitudinally among older adults (65+) in China. We also aim to explore the subgroup variations of the association by age, gender, and rural/urban residence, the typical demographic variables that stratify Chinese society. Hope our investigations will help to better understand the dynamic relationship between education and mental health in Chinese society.
In many ways, an examination of the association between education and distress among older Chinese and its subgroup-specific strength is an important test. First, after market reforms in China, education becomes increasingly important in Chinese society as returns to human capital are expected to increase under a competitive labor market that more efficiently rewards individual abilities (Cao & Nee, 2005). Second, given the tremendous aging tendency in China and its domestic and world impact (Poston & Zeng, 2008; Zeng, Vaupel, Xiao, Zhang, & Liu, 2002), it will be beneficial to learn more about the important predictors of mental health problems such as depression, the most common psychiatric condition among older people (Chen, Hu, Qin, Xu, & Copeland, 2004). One recent meta-analysis published in Chinese (L. Zhang, Xu, & Nie, 2011) revealed that the prevalence of depression among elderly Chinese is an astonishing 22.6%. Third, tracking older adults ranging from the young-old to the oldest-old for a long period of time may help to better disclose the lifelong causal effect of education (Dupre, 2007; Mirowsky & Ross, 2003; O’Rand, 1996). Fourth, focusing on China may offer new insights on the explanatory mechanisms linking education and distress. As Liang, Liu, and Gu (2001) pointed out, findings on socioeconomic status (SES) and health from Western societies may not be readily generalized to China given its unique socioeconomic and cultural characteristics. Finally, given the significant health disparities by demographic factors such as gender and region in China (i.e., Kaneda, Zimmer, Fang, & Tang, 2009; Liang et al., 2001; Pearson, 1995; Zimmer, Kaneda, Tang, & Fang, 2010; Zimmer, Wen, & Kaneda, 2010), it will be helpful to see whether education affects distress differently for different populations.
Education and Health
Numerous studies in the United States document that higher levels of education are positively associated with better health and longer life (Baker, Leon, Smith Greenaway, Collins, & Movit, 2011; Mirowsky & Ross, 2003; Montez, Hummer, & Hayward, 2012). Many studies have offered excellent reviews on the causal order of the association (Eide & Showalter, 2011; Mirowsky & Ross, 2003) and have empirically tested factors that may mediate the association (Mirowsky & Ross, 2003; Rogers, Hummer, & Everett, 2013; Ross & Wu, 1995). Moreover, some studies (Goesling, 2007; H. Liu & Hummer, 2008) suggest that educational health disparities have been increasing for some social groups due to growing disparities in socioeconomic resources related to education.
While the association between education and health becomes a social fact in the United States, whether the causal relationship exists and how the association operates among elderly in an Asian context such as China are not entirely clear. Most available studies have focused on physical health. Liang and colleagues (2001) found that education has direct and indirect beneficial effects on transitions in disability among older Chinese through social relations. A short report by J. Wu and colleagues (2003) revealed that rural Chinese with lower levels of education have a greater disposition of restricted activity, and this educational gap in physical health was broader in 2001 than in 1993. Using a regional sample in China, Elwell-Sutton et al. (2011) demonstrated that socioeconomic disadvantage across the life course, including low levels of education at early adulthood, is associated with poor self-rated health and chronic obstructive pulmonary disease. A couple of studies (Hu & Hibel, 2013; G. Liu & Zhang, 2004) on self-rated health echoed their findings. Similarly, Beydoun and Popkin (2005) disclosed that education is a strong predicator of functional decline and mild disability incidence among older Chinese (55+).
Compared with the relatively richer findings on physical health, to our knowledge, there is only one available study that explicitly examines the relationship between education and distress in mainland China using a nationally representative sample (Ross & Zhang, 2008). However, their study is based on cross-sectional data and primarily focuses on the very old population segment (i.e., individuals older than 75 years). A review of literature published in Chinese also disclosed that education is among the key factors that are related to depression among elderly Chinese (L. H. Guo et al., 2014; Lin, 2006; H. J. Liu, Meng, & Tang, 2004; Yang, Li, Wang, & Wu, 2007; L. Zhang et al., 2011). To understand the long-term effect of education on mental health and to extend findings to a more generally defined old population in China, the first aim of our study is to examine the education–distress relationship both cross-sectionally and longitudinally among older Chinese aged 65 and over.
Pathways Linking Education and Health
As an exogenous, universal, and stable indicator of SES (Ross & Wu, 1996), education suggests a type of internalized human capital that will lead to a variety of valuable cognitive skills that include abilities to read, write, calculate, think, reason, and solve problems. In other words, general intelligence generated by schooling will be progressively transformed into higher order cognitive skills to help individuals to constantly evaluate the environment and to make various decisions (Baker et al., 2011). These cognitive skills and abilities can help individuals find a fulfilling and creative job, accumulate economic and psychosocial resources, and weave disparate habits and practices into a coherent lifestyle, all of which in turn, promote health and well-being (Mirowsky & Ross, 1998; Ross & Wu, 1995).
Are those pathways (i.e., work and economic conditions, psychosocial resources, and health lifestyle) linking education and health identified in American society applicable in China among its older citizens? It is likely the case when economic conditions are considered (Hu & Hibel, 2013; Ross & Zhang, 2008). Therefore, in the present study, we retest the mediating effect of economic conditions. More importantly, given the unique cultural dynamic in China, we specify health lifestyle into various dimensions of leisure-time activities and test their relevance in mediating the effect of education on distress.
Engagement in meaningful leisure-time activities, a critical component of successful aging (Rowe & Kahn, 1998), can be considered an important aspect of a healthy lifestyle. Moreover, as Coleman (1993) mentioned, leisure activities are particularly useful in helping individuals develop and maintain social interactions and social relationships because they often take place within social groups. Therefore, if education shapes psychological well-being in late life, it may do so in part through leisure-time activities engaged in by the elderly. However, most previous studies have primarily focused on physical activities such as walking and strenuous exercise that are associated with high levels of education and low levels of distress (Hayes & Ross, 1986; Mirowsky & Ross, 2003; Ross & Bird, 1994; Ross & Wu, 1995). Other types of activities such as playing cards/mahjong, attending organized social activities, and readings that may stimulate cognitive abilities or enhance social interactions are often overlooked in this literature, although some studies suggest that these nonexercise leisure activities may have different prevalence and trends among older Chinese over time (Feng, Purser, Zhen, & Duncan, 2011).
Ross and Zhang (2008) are among the first to examine activities that link the association between education and distress among older Chinese. They found that better-educated older Chinese report lower levels of distress than do their less-educated counterparts in part because they engage in more cognitively stimulating and physical activities. Using the same data source, Sun and Liu (2006) demonstrated that customary activities, including doing housework, gardening, reading newspapers/books, watching TV/listening to the radio, playing cards/mahjong, and attending religious activities, have independent effects on survival. Based on their studies and previous literature on leisure activities (Coleman, 1993; Silverstein & Parker, 2002), we conceptualize a three-dimensional framework of leisure-time activities to be one of the important pathways linking the education–distress association among older Chinese (Figure 1).
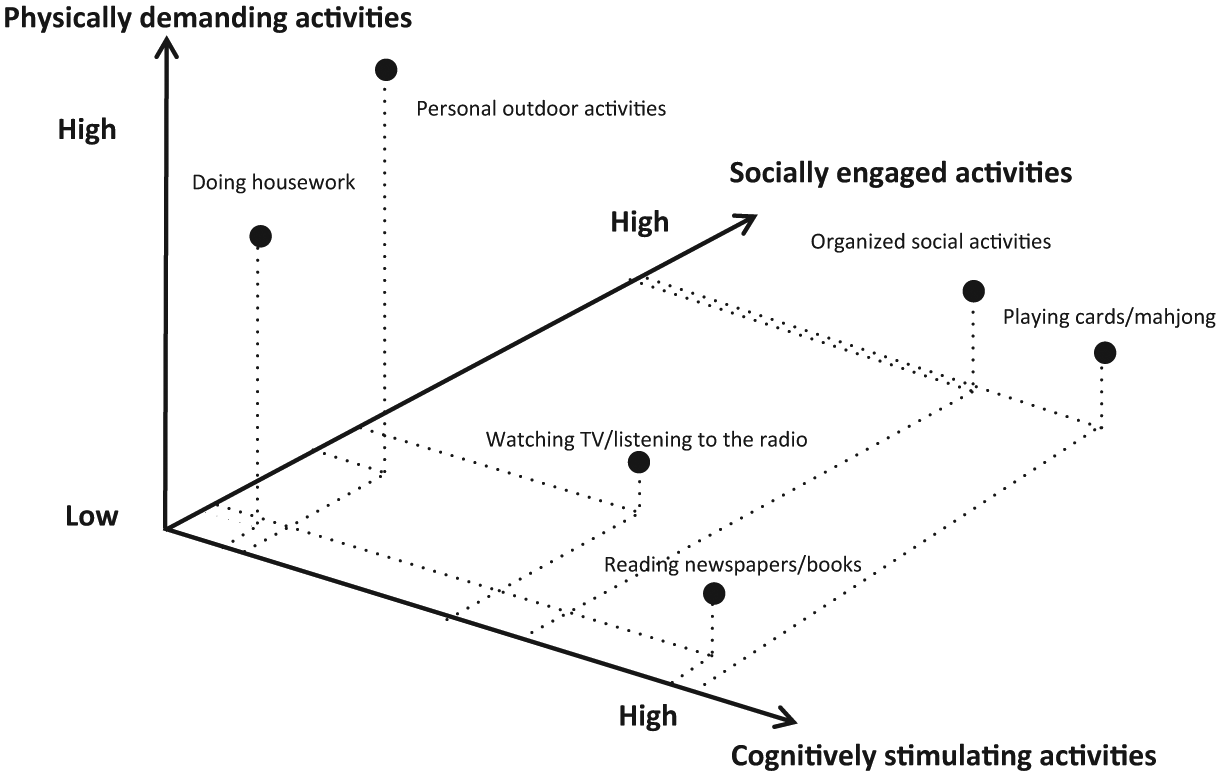
Health lifestyle indicated by a three-dimensional framework of leisure-time activities.
Better-educated older adults may engage in activities that are physically active/demanding, cognitively stimulating, and socially engaged, which in turn, may benefit their mental health through physiological pathways. We argue that those activities engaged in by older Chinese tend to fall in a three-dimensional system. Activities that fall along a certain dimension are relatively stronger in that dimension and weaker in other two dimensions in comparison with other activities. For instance, as an indicator of the cognitively stimulating activity index, reading newspapers/books is higher in the cognitively stimulating dimension, but relatively lower in the socially engaged and physically active dimensions in comparison with other activities. Primarily based on face validity, we simplified the three dimensions of activities as below: The first dimension contains activities that are largely socially engaged such as attending organized social activities and playing cards/mahjong. The second dimension incorporates activities that are largely cognitively stimulating such as watching TV/listening to the radio and reading newspapers/books. The third dimension includes activities that are physically active such as doing housework and engaging in personal outdoor activities.
Taken together, the second aim of our study is to examine whether a healthy lifestyle indicated by participating in leisure-time activities explains the association between education and distress over and above those well-established mediators such as physical health, economic conditions, and social relations such as marital status and living arrangements.
Education and Health: Subgroup Variations
As Walsemann, Gee, and Ro (2013) summarized in their recent review article on education and health, the relationship between education and health is not uniform across social groups. In other words, “The effects of educational attainment [tend to] intersect with multiple forms of stratification” (Walsemann et al., 2013, p. 1084) to benefit some social groups more than others. Whether educational gradients in health are stronger or weaker for the socially disadvantaged groups than for those socially advantaged groups? Findings remain mixed in American society. Kessler (1982) revealed that, among indicators of SES, education is the strongest predictor of distress for women in the labor force. Ross and Mirowsky (2006) found that education reduces depression more for women than for men. For physical health, self-rated health, and mortality, findings are inconsistent, with some studies suggesting that education has a larger effect on women’s health than on men’s (Ross, Masters, & Hummer, 2012; Ross & Mirowsky, 2010; Thurston, Kubzansky, Kawachi, & Berkman, 2005), others revealing inconclusive (Matthews, Manor, & Power, 1999) and opposite findings especially when mortality was examined (Ross et al., 2012). When race is considered, a recent study (Montez et al., 2012) suggests that each year of schooling before getting a high school diploma is associated with smaller mortality risk reduction for Blacks than for Whites.
In China, gender and rural/urban residence are two typical forms of social stratification. Compared with old Chinese men, old Chinese women have worse health and fewer health-related resources. Pearson (1995) reviewed the traditions of gender discrimination in China and described that women in China have been historically discriminated against. The status of women, however, has been substantially improved after the Communist revolution when Mao Zedong advocated that “women should hold up half the sky.” Although significant gender discrimination remains in China nowadays, access to education and the labor force has started to become more equal for both gender groups compared with previous era. However, it should be noted that most Chinese elderly had already passed their schooling age before these fundamental social changes. A paucity of studies that examined gender differences in health found that both the suicide rates and depression rates are much higher for women than for men in China (Pearson, 1995; L. Zhang et al., 2011) and women are more likely to be functionally dependent compared with men in late life (Kaneda et al., 2009). And the socioeconomic and health disadvantages could be particularly evident for Chinese women of older age (Zeng, Liu, & George, 2003).
In addition to gender differences in health, another primary delineation distinguishing individuals across various domains in China is the urban/rural residence. The official hukou system established in early 1950 legally divides individuals into agricultural and nonagricultural populations. Individuals belonging to different populations are subject to different socioeconomic and health policies (Chan & Zhang, 1999). One study conducted in Beijing (Zimmer, Kaneda, Tang, & Fang, 2010) found that older Chinese living in urban areas show advantage in mortality and functional independence over their rural counterparts largely because they enjoy better SES and are more likely to have health insurance. Other studies on functional health and mortality among older Chinese revealed that urban residents are less likely to have a functional limitation at 2 or 3 years follow-up (Liang et al., 2001; Zimmer, Wen, & Kaneda, 2010) and are less likely to die over a 2-year study period (Zimmer et al., 2010) compared with their rural counterparts. Dong and Simon (2010) found that older Chinese in rural areas, in comparison with their urban counterparts, are more likely to have lower education, income, lower overall health, lower quality of life, and worse change in recent health, and more depressive symptoms. Similarly, some studies published in Chinese also suggested that rural residents exhibit higher rates of depression than urban residents (A. M. Guo & Lai, 2011; L. Zhang et al., 2011).
Old age may also suggest a disadvantaged social position because it is usually associated with death of loved ones, fewer socioeconomic resources due to retirement, more physical and chronic conditions, and lower levels of psychological well-being. Collectively, the third aim of our study is to examine subgroup variations with regard to age, gender, and rural/urban residence within the association between education and distress. The conceptual framework guiding our study is presented in Figure 2.

Conceptual model linking education, mediators, moderators, and distress.
Method
Sample
We use data from the 2002, 2005, 2008, and 2011 waves of the Chinese Longitudinal Healthy Longevity Survey (CLHLS). Six waves of the CLHLS have been collected since 1998. We excluded the 1998 and 2000 waves because they only surveyed the oldest-old population (80+) in China. Information on young-old population (65-79) has been collected since wave 2002, the starting point of our investigation. The CLHLS was conducted in randomly selected half of the counties/cities in 22 provinces in China. To avoid errors of random fluctuation due to small sample size at more advanced ages, especially for males, CLHLS did not follow the procedure of proportional sampling design in the selected 22 provinces in 2002 and 2005. Instead, the CLHLS made an attempt to interview all centenarians in the sampled counties/cities and for each centenarian, one nearby elder from each of four age groups 65-69, 70-79, 80-89, and 90-99 with a predesignated age and sex was interviewed on a random basis. As a result, the oldest-old groups were oversampled.
All participants of the CLHLS were tracked in the following waves unless they were dead or lost to follow-up. Respondents who were dead or lost to follow-up will be replaced with new cases with the same age, gender, and residence type within the same county. All information in the CLHLS has been obtained through face-to-face in-home interviews. The systematic assessments on data quality of the CLHLS is high regarding accuracy of age-reporting, reliability, validity, and the consistency of numerous measures and the randomness of attrition (Gu, 2008). Our longitudinal data contain a total of 54,405 valid observations, with 13,560; 13,073; 13,156; and 7,910 observations in the waves of 2002, 2005, 2008, and 2011, respectively. The 2011 data only tracked participants from the previous wave without new recruitment, resulting in a reduction in sample size.
Measurement
Psychological distress, the opposite of psychological well-being on a mental health continuum (Mirowsky & Ross 2002, 2003), was measured by a four-item index (ranging from 0 to 16) to capture individual differences in the severity of the depression and anxiety symptoms. Specifically, the CLHLS asked participants to report how often they feel anxious or fearful, feel lonely, feel useless when getting old, and feel not as happy as younger age. A score was assigned to each question with 4 as “always,” 3 as “often,” 2 as “sometimes,” 1 as “seldom,’ and 0 as “never.” A sum index was then created with higher scores reflecting higher levels of psychological distress. All items load on one and only one factor above 0.73, and the Cronbach’s alpha of the distress index is above .85 across waves. Ross and Zhang (2008) used the same items to construct the psychological distress scale. Other scholars (Z. Wu & Schimmele, 2006; W. Zhang & Liu, 2007) applied similar measures in the CLHLS to construct the psychological well-being and psychological disposition scales. These studies have confirmed that those items are good measures to gauge mental health of older Chinese.
Education was measured by four categories: the illiterate category (including respondents with no years of schooling), elementary school category (including respondents with 1-6 years of schooling), middle school category (including respondents with 7-9 years of schooling), and high school or above category (including respondents with ≥10 years of schooling). This classification is appropriate in consideration of the extremely low proportion of college-educated elderly in China, which is lower than 5% according to the estimation of the CLHLS.
We included covariates such as age (in years), gender (female = 1), ethnicity (minority = 1), rural/urban residence (rural = 1), marital status (currently married = 1), and living arrangements (living with family members = 1). Survey wave was measured as a categorical variable with values of 2002, 2005, 2008, and 2011 to control for the temporal trends of distress. For our analysis using Heckman selection model, we added two additional covariates: whether the respondent suffered serious illness in past 2 years (yes/no) and whether the current age/death age of the respondent’s mother is above 80 years old (yes/no). Both covariates are related to the likelihood of being deceased or lost to follow-up, the dependent variable used in the selection equation.
We examined three sets of mediators to evaluate the impact of education on distress. We first included the physical health factors such as self-reported health (bad/fair/good), disability in activities of daily life (ADL; yes/no, measured by any dependency in bathing, dressing, going to the toilet, indoor transferring, feeding, and continence), and disability in the instrumental ADL (IADL; yes/no, measured by any difficulty in visiting neighbor, shopping, cooking, laundering, using public transportation, walking for 2 km, lifting 5 kg, and crouch for 3 times). Economic mediators, the second set of mediators, include self-evaluated economic condition (bad/fair/good) and economic independence (yes/no, measured by whether the respondent’s life depends on his or her own financial resources or on others). Finally, a three-dimensional framework of leisure-time activities was incorporated. For each activity mentioned, a score to indicate its frequency was assigned with 4 as “almost every day,” 3 as “at least once a week,” 2 as “at least once a month,” 1 as “seldom,” and 0 as “never.” Three sum indices (socially engaged activity index, cognitively stimulating activity index, and physical demanding activity index) were created.
Analysis
Weight was applied in descriptive statistics (in Table 1) to adjust for the survey design of the CLHLS. The weighting variable was based on the census-informed age, gender, rural/urban residence distributions of the entire Chinese elderly population in the survey year (CLHLS Research Team 2000). We then used pooled data to estimate the crude effect of education on distress by age, gender, and residence in Table 2. The random-effect panel model was used to estimate the impact of education on distress adjusting for demographics, living arrangements, and survey waves because the longitudinal data contain multiple observations for a single respondent across waves. The model introduced a random intercept for each respondent to control for the intraperson variance. To assure that there is no major bias due to mortality selection in the model, we examined the association between education and the subsequent status of being lost to follow-up for the periods of 2002 to 2005, 2005 to 2008, and 2008 to 2011, respectively. The results (available upon request) showed no significant associations. Collectively, the major purposes of using pooled data and random-effect panel model is to (a) increase the sample size for a better estimation of the effect of education and (b) control for the unobserved heterogeneity among individuals by introducing a random intercept for individuals. We additionally examined the interactions of education with gender, urban/rural residence, and age in Table 3.
Weighted Descriptive Statistics Across Four Data Waves (2002, 2005, 2008, and 2011).

Note. Socially engaged activity index is composed of organized social activities and playing cards/mahjong. Cognitively stimulating activity index consists of reading newspapers/books and watching TV/listening to the radio. Physically demanding activity index includes personal outdoor activities and doing housework. ADL = activities of daily life; IADL = instrumental activities of daily life.
Effects of Education on Distress by Age Groups, Gender, and Rural/Urban Residence in Random-Effect Panel Models.

Note. Reference categories are in parentheses.
p< .10. *p< .05. **p< .01. ***p< .001.
Effects of Education on Psychological Distress in Random-Effect Panel Models for Whole Samples in 2002, 2005, 2008, and 2011.

Note. Reference categories are in parentheses.
p< .10. *p< .05. **p< .01. ***p< .001.
To further explore the effect of education by different subgroups, we conducted longitudinal analyses by gender, residence, and age groups in Tables 4 and 5 to examine the longitudinal effect of education on the changing status of distress separately in the following four periods, that is, from 2002 to 2005, 2005 to 2008, 2008 to 2011, and finally 2002 to 2011. Due to similar concerns as above that sample attrition between waves may bring bias in estimation, Heckman selection model was applied with two equations in Tables 4 and 5: In the outcome equation using ordinary least squares (OLS) regressions, distress at the later wave is the dependent variable, education is the independent variable, and covariates include age, gender, residence, minority status, marital status, and living arrangements; in the selection equation using Probit regressions, the likelihood of being deceased or lost to follow-up is the dependent variable, and covariates include education, those covariates used in the outcome equation, distress at the baseline, and two additional variables as whether the respondent suffered serious illness in the past 2 years and whether the current age/death age of the respondent’s mother is above 80 years old. These two variables are not in the outcome equation, thus take the role of “exclusion restriction” to avoid substantial collinearity between the predicted inverse Mills ratio term and the remaining covariates in the outcome equation in Heckman selection model.
Effects of Education on the Changing Status of Distress by Gender and Rural/Urban Residence in Heckman Selection Models.

Note. Reference categories are in parentheses. In the outcome equation, dependent variable is “distress at the later wave.” Covariates including age, gender, rural/urban residence, minority status, marital status, and living arrangement were not listed, but available upon request. In the selection equation, the dependent variable is “whether respondent is deceased or lost to follow-up at the later wave.” Covariates including age, gender, rural/urban residence, minority status, marital status, living arrangement, and distress at baseline were not listed, but available upon request. The coefficient associated with “middle school (elementary school)” was omitted because there was no sample aged 90+ whose education level was middle school and survived from 2002 to 2011.
p< .10. *p< .05. **p< .01. ***p< .001.
Effects of Education on the Changing Status of Distress by Age Groups in Heckman Selection Models.

Note. Reference categories are in parentheses. In the outcome equation, dependent variable is “distress at the later wave.” Covariates including age, gender, rural/urban residence, minority status, marital status, and living arrangement were not listed, but available upon request. In the selection equation, the dependent variable is “whether respondent is deceased or lost to follow-up at the later wave.” Covariates including age, gender, rural/urban residence, minority status, marital status, living arrangement, and distress at baseline were not listed, but available upon request. The coefficient associated with “middle school (elementary school)” was omitted because there was no sample aged 90+ whose education level was middle school and survived from 2002 to 2011.
p< .10. *p< .05. **p< .01. ***p< .001.
Finally, we used four nested models to explore how the effect of education on distress is mediated by health lifestyle as indicated by leisure-time activities while controlling for other widely used mediators and covariates. Model I included basic demographics, living arrangements, and survey waves; Model II added physical health variables such as ADL disability, IADL disability, and self-rated health; Model III incorporated economic variables such as self-evaluated economic condition and status of economic independence; Model IV added our focal mediating variables—those leisure-time activities that are socially engaged, cognitively stimulating, and physically demanding. Variables on leisure-time activities were lagged to avoid potential reverse causation with distress. All analyses were performed using Stata/SE 12.0.
Results
Results from Table 1 show that the mean scores of distress range from 4.89 to 5.49, which are relatively stable across waves. The educational level of the elderly was generally low in China: Almost half of survey respondents did not have any schooling, and approximately 40% of the respondents only received elementary level of education. In addition, education was negatively associated with distress (Figure 3): The mean level of distress declined from 5.74 for the illiterate to 3.86 for those with high school or above level of education. This pattern is consistent for different gender-rural/urban groups except for rural females. Figure 3 also shows that rural females reported the highest mean level of distress, followed by urban females and rural males who share similar level of distress. Urban males reported the lowest mean level of distress.
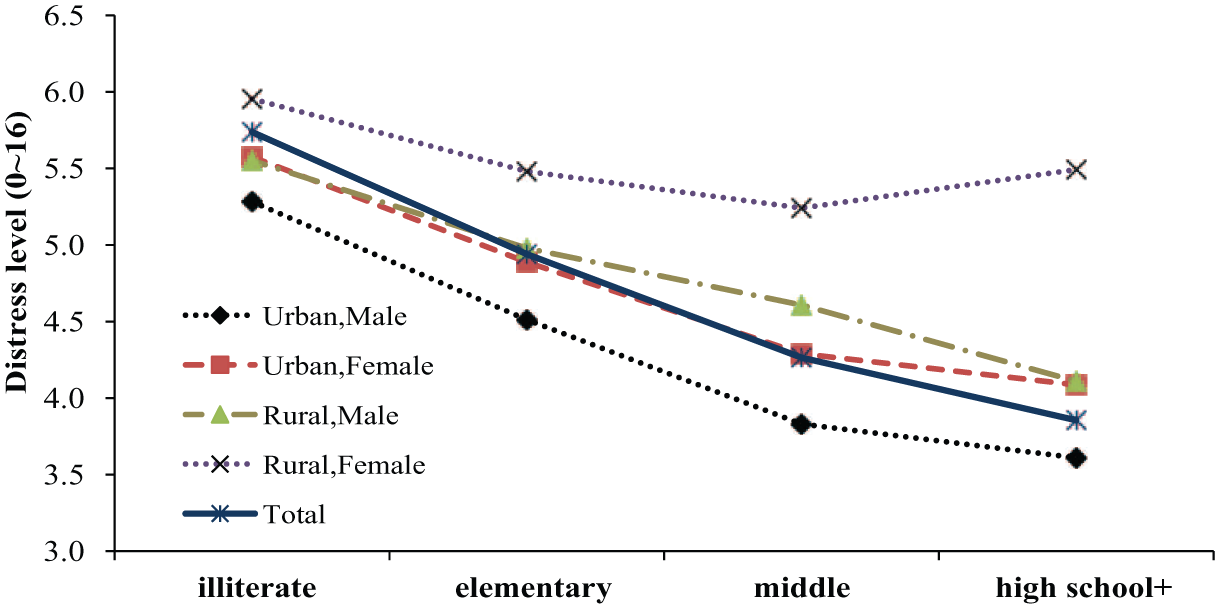
Distress at different levels of education by gender and rural/urban residence (weighted).
Other variables in the analysis are also described in Table 1. For instance, the mean age of respondents across waves was about 73.0 with a standard deviation of about 6.0. The percentage of rural respondents declined from 64.6% to 52.1% from 2002 to 2011. Most respondents were currently married and living with their family members. About half of the survey respondents reported their health as good, the prevalence of ADL disability was generally lower than 10%, and the prevalence of IADL disability was about 35% across waves. Although nearly half of the respondents reported enjoying economic independence, less than one fifth of them reported having good economic conditions.
The crude impact of education on distress is summarized in Table 2. Results display that, compared with those having elementary level of education (the reference group), the illiterate reported a higher score of distress by 0.37, whereas those with a middle school level of education and high school or above level of education reported lower scores of distress by 0.48 and 0.74, respectively (see the last column in Table 2). And the significant relationship between education and distress remains consistent and substantial across different age, gender, and rural/urban groups.
To disclose the subgroup variations in the education–distress association, we introduced interactions between education levels and covariates in the full model of Table 2. Results (summarized in Table 3) reveal that some interaction terms are significant at the level of .05 or .10. It is worth noting that disadvantage of being illiterate was significantly less for females than for males, and for older age groups than for younger age groups. In other words, the effect of education is significantly more salient for males and for the young-old.
While examining the coefficients of waves in Tables 2 and 3, it is worth noting that the trends discontinued after 2008: The coefficients of the 2005 and 2008 waves were positive, whereas the coefficients of the 2011 wave became negative. We speculate that this discontinued trend may reflect the impact of the ongoing health care reform on population health in China. Since 2003, China has started to adopt a new health insurance system called New Cooperative Medical Scheme (NCMS) in rural area and its coverage has expanded to the majority of rural counties by the end of 2007. Some studies examined the impact of the NCMS and revealed that participating in the NCMS increases the utilization of preventive care (Lei & Lin, 2009) and activities of daily living, and improve cognitive functioning for the elderly enrollees in rural areas (Cheng, Liu, Zhang, Shen, & Zeng, 2014). This policy change at the macro level may partially contribute to the discontinued trend identified in the findings.
As Table 3 shows that the interactions between levels of education and some covariates are significant or borderline significant in the pooled analysis, we stratified our sample by gender, residence, and age groups in the longitudinal analysis using Heckman selection model. Results are summarized in Tables 4 and 5. Similar to our findings in the cross-sectional analysis, results of the longitudinal analyses revealed that a higher level of education at the baseline was always associated with a lower level of distress in a later wave, although some results are not significant at the .05 level. It is interesting to note that the effect of high school or above level of education on subsequent level of distress always maintained significant for certain subgroups such as males, urban residents, and the 65-79 age group. These findings indicate that a high level of education predicts distress over time, and this is particularly true for males, urban residents, and the young-old. The reliability and robustness of the effect of education on the changing status of distress should also be highlighted. In Tables 4 and 5, when compared with the elementary level of education, the effect of the illiterate level of education on the subsequent level of distress was always positive (except for those 90+) and the effects of middle school and above levels of education on distress were always negative (except for those 80+). These findings indicate that higher levels of education lead to lower levels of subsequent distress, and these patterns are persistent across various periods and for most subgroups.
Although variables on health lifestyles are our focal mediators, those widely examined mediators such as physical health and economic factors were also introduced into the baseline model in Table 6 to facilitate comparisons. When adding physical health variables into the baseline model, the effect of education on distress was reduced by 17.8%, 27.5%, and 6.3%, respectively, for the illiterate, the middle school category, and the high school or above category in comparison with the elementary school category (Model II). Economic factors further mediated the effect of education as shown in Model III: The effect of education was additionally explained away by 37.6%, 38.0%, and 44.3%, respectively. The effect of education was further reduced when leisure-time activities were added in Model IV. In this model, the effects of education were additionally reduced by 44.8%, 36.5%, and 38.2%, respectively, and differences of the illiterate group and the middle school group in comparison with the reference group became insignificant at the .05 level. These findings indicate that education is associated with better mental health largely because those well-educated (compared with their poorly educated counterparts) enjoy better physical health and economic conditions, and engage in more leisure-time activities that are socially engaged and cognitively stimulating. The effect of physically demanding activity index on distress is insignificant.
Effects of Education on Distress via Mediators in Random-Effect Panel Models.
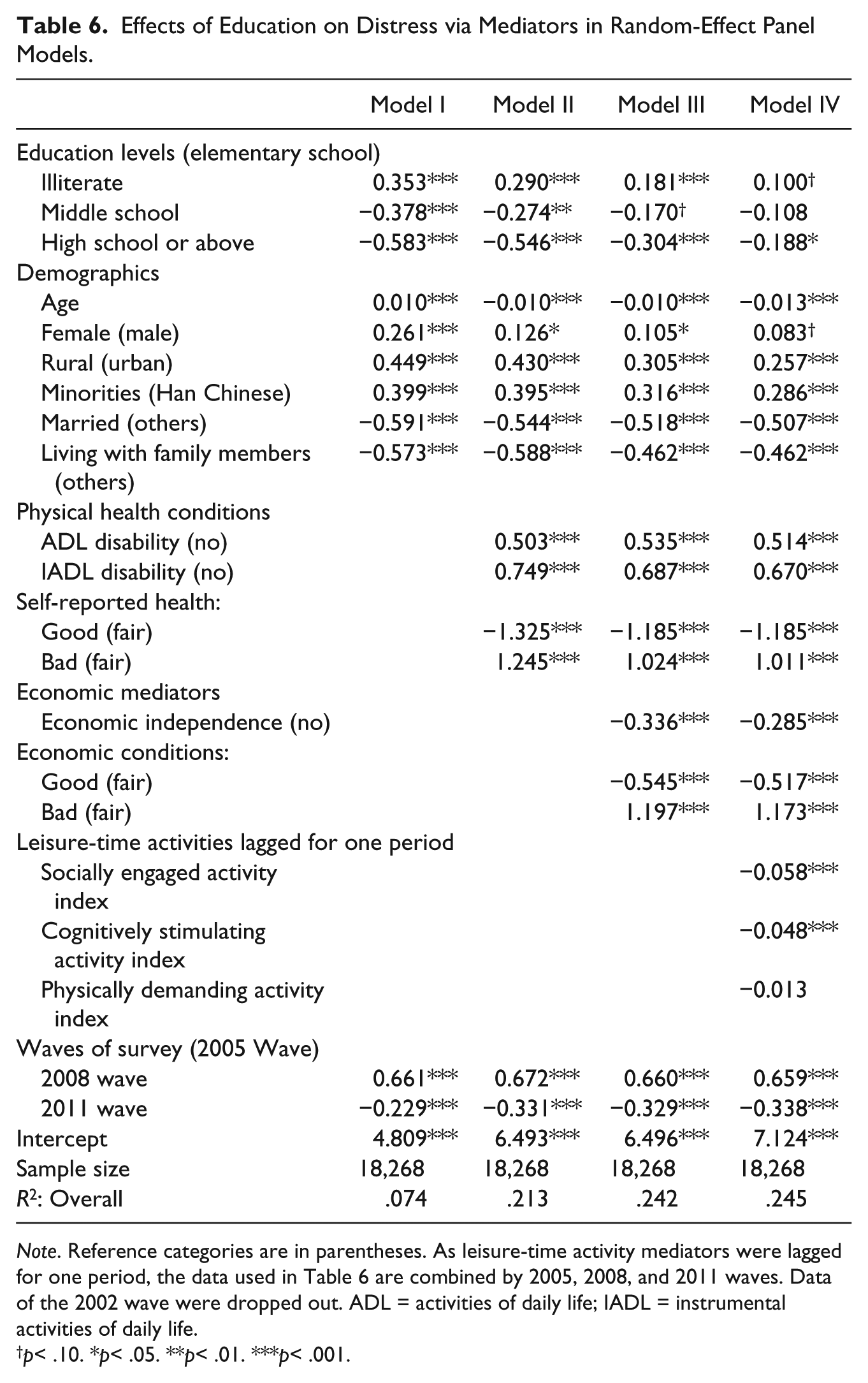
Note. Reference categories are in parentheses. As leisure-time activity mediators were lagged for one period, the data used in Table 6 are combined by 2005, 2008, and 2011 waves. Data of the 2002 wave were dropped out. ADL = activities of daily life; IADL = instrumental activities of daily life.
p< .10. *p< .05. **p< .01. ***p< .001.
Discussion
Although many studies have examined the relationship between education and distress, a few significant gaps remain in the literature. Questions such as whether and how education predicts distress for the elderly over time and whether this association varies by demographics like age, gender, and residence are still not fully answered. Using four waves of data across 10 years from the CLHLS and applying the random-effect panel model and Heckman selection model, we found the following: (a) There is a persistent and negative association between education and distress among older Chinese using pooled data across survey waves; (b) high levels of education predicts low levels of distress over time and this is particularly the case for males, urban residents, and the young-old (aged 65-79); and (c) the effect of education on distress is partially explained by leisure-time activities, physical health, and economic conditions.
Pooled analysis comprising the young-old, the old-old, and the oldest-old Chinese suggests that education has a persistent, stable, and long-term protective effect on the mental health in China among the elderly. This finding greatly enhances the external validity of the well-established relationship between education and health in Western societies. In general, current Chinese elderly cohorts were not well-educated due to historical reasons. According to our results, only less than 20% of the respondents had education higher than middle school, and very few had college level of education. Despite the general low levels of education among older Chinese, the reliable and robust association between education and mental health remains with each additional level of increase in education suggests a mental health advantage. The types of education received by older Chinese many decades ago may be very different from those in Western society, but the strong effect of education on health is still identified in our study. This indicates that education, no matter what forms it takes, is able to translate into abilities, skills, a lifelong learning habit, and various psychosocial resources that are essential to promote individual health. Education remains a root cause of psychological well-being within the Chinese cultural context.
Consistent with prior research on other health outcomes such as self-rated health (Goesling, 2007; Lynch, 2003; Mirowsky & Ross, 2008) and mortality (Feldman, Makuc, Kleinman, & Cornoni-Huntley, 1989; Lauderdale, 2001) in the United States, our findings on mental health revealed that the effect of education on distress is more substantial and significant for the young-old than for the old-old. This indicates that the importance of education on mental health is likely to increase over time in China. Results from our supplementary analysis (available upon request) by age groups also show that younger cohorts, in comparison with their older counterparts, reported significant lower levels of distress, enjoyed much higher levels of education, a better physical health, and more economic independence, and engaged in leisure-time activities more frequently. These supplementary findings further suggest that the gap in mental health between the well-educated and the poorly educated is projected to be widening across more recent birth cohorts. Reasons that account for the widening gap may include (a) the increasing relevance of schooling to public health knowledge and to the practice of healthy lifestyles, (b) the increasing importance of the health-enhancing roles of mediators linking education and health (Lynch, 2003), and (c) the increasing unequal access to health care between the rich and poor as a result of the increased out-of-pocket cost due to the privatization and market-based financing reform in the Chinese health care system (Hsiao, 1995; Kaneda et al., 2009). Even for the newly adopted NCMS, there is no evidence showing that it decreases the out-of-pocket expenditure for the enrollees (Cheng et al., 2014; Lei & Lin, 2009). Taken together, all these changes taking place in the contemporary Chinese society tend to boost the significance of education, making it more important to the health for the younger generations.
This study also contributes to the literature by examining population differences in the strength of the educational gradient in health. Our findings point out that education is likely to intersect with multiple forms of stratification in the Chinese society such that the advantaged social groups (i.e., males, urban residents, and the young-old) tend to enjoy more mental health benefits from education than their disadvantaged counterparts. Different from some findings in the United States (Kessler, 1982; Ross et al., 2012; Ross & Mirowsky, 2006, 2010), our results may support resource amplification view (i.e., resources work together to multiply their advantage) rather than resource substitution theory (i.e., the presence of one resource such as education makes the lack of other resources less harmful). A weaker mental health effect of education for those disadvantaged social groups may suggest that they experience smaller economic returns from schooling than the advantaged social groups. For instance, compared with their urban counterparts, rural Chinese tend to have limited pension support (Zeng et al., 2002) and health services (Y. Liu, 2004) so that various advantages associated with education may not be fully realized for them because of policy differences and institutional discrimination.
However, a closer examination of Figure 3 suggests other possible explanations. As illustrated by the top dotted line in Figure 3, an increased level of education does not seem to make a significant difference in the mental health of rural women whose initial level of distress is the highest among all four groups. In this sense, our findings on subgroup variations may be more outcome-driven than resource-driven. That is, women, rural residents, and the old-old are at risk of higher levels of distress, which might make education less useful for them to deal with distress. Our supplementary analysis also showed that, although education partially explains gender and rural/urban differences in distress, the disparities remain significant and substantial. This suggests that higher levels of distress for females and for rural residents are resulted not only from their poorer individual educational attainment but also from some structural factors in further upstream such as place of education and the hukou registration system that greatly differentiate the educational opportunity as well as quality among various social groups. Taken together, our findings may not be able to either support or dispute resource multiplication or resource substitution theory without eliminating other possible explanations. Moreover, we have to keep in mind that there are high percentages of women and rural residents are illiterate or do not have formal education (Zeng et al., 2003; Zeng et al., 2002). As a result, we may not have sufficient cases of highly educated women and rural residents in the data to make valid comparisons.
The better-educated older Chinese enjoy better psychological well-being in late life than do their less-educated counterparts in part because they enjoy better physical health and better economic conditions, and engage in more leisure activities. Based on prior theoretical and empirical research (Cockerham, 2000; Glass, Leon, Marottoli, & Berkman, 1999; Ross & Zhang, 2008; Sun & Liu, 2006), we theorized a three-dimensional system of leisure-time activities that goes beyond the previous categorization along two broad dimensions: physical versus sedentary and social versus solitary (Jacobs, Hammerman-Rozenberg, Cohen, & Stessman, 2008). Studies have started to show that some nonstrenuous and solitary leisure activities such as watching TV or reading daily are significantly related to a better mental health (Ross & Zhang, 2008) and a reduced mortality risk among older adults (Jacobs et al., 2008; Sun & Liu, 2006). Their findings suggest that “a broader definition of leisure activities may be useful when considering the impact of these activities among older people” as remaining active in any aspect is related to a successful aging (Jacobs et al., 2008, p. S73). Our results indicate that, among three dimensions of leisure-time activities, the index of activities that are socially engaged (including attending organized social activities and playing cards/mahjong), that require perhaps the most social and cognitive skills and abilities derived from education, has the greatest impact on distress, followed by activities that are cognitively stimulating but solitary. These two sets of activities greatly mediate the effect of education on distress, suggesting that education, as a “learned effectiveness” can benefit mental health through weaving a healthy lifestyle that goes beyond the widely examined behavioral mediators such as exercise, drinking, and smoking in prior research. Our findings also suggest that, within the Chinese cultural context, socially engaged activity is likely to form a pathway that is most relevant in the education–health association for the elderly who greatly value collectivism.
Although our study has addressed a number of important issues in the field of education and health, several limitations need to be noted. First, although we considered several important pathways linking education and health in China, we did not include other psychosocial mediators such as a sense of personal control, self-esteem, and social support in the analysis. These variables are not systematically measured in the CLHLS. Second, besides the urban/rural differential, other regional differences such as eastern versus western difference should be closely examined to comprehensively disclose the regional disparities in the education–health association in China. Last but not least, to confirm the subgroup variations identified in this work, future studies need to include younger generations who enjoy more equal access to education that is more or less similar in the quality and content.
Conclusion
Despite these limitations, our study’s main advantages include the use of a nationally representative sample, the application of sophisticated statistical analyses using longitudinal data, an examination of subgroup variations, and the theorization of a three-dimensional framework of leisure-time activities. Our findings help to strengthen the external validity of the education–health association, identify the culturally sensitive pathways linking the two, and suggest the dynamic patterns on the subgroup variations within this association in a non-Western context.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by grants from the Humanity and Social Science Foundation of Ministry of Education, China (Grant 10YJC790021), and the Natural Science Foundation of Hunan, China (Grant 11JJ3093).