
Abstract
Nursing home (NH) managers and staff are continually seeking ways to improve care provided to their residents. One strategy reported to be successful is the empowerment of direct care workers (DCWs). Typically, these workers are certified nurse aides (CNAs), including those trained to serve as hydration aides, medical aides, and restorative aides. DCWs are more familiar with the daily needs and desires of residents than any other NH employees. Consequently, allowing them to participate in decisions about the residents can result in decisions that improve the health and satisfaction of residents. Conversely, the task-oriented assembly-line approach to NH care has been reported to “get in the way” of delivering the best care. This includes forcing DCWs to do things residents do not want such as waking them up much earlier than desired or bathing them at a time they do not want to be bathed (Koren, 2009). The purpose of this study is to identify factors associated with employee empowerment (EE) in NHs.
The advantages of empowering DCWs have been identified by a variety of researchers examining resident care. For example, Barry, Brannon, and Mor (2005) found CNA empowerment to be associated with a reduction in resident pressure ulcers (see also Anderson & McDaniel, 1999). Scotti, Harmon, and Behson (2007) found that empowering health care workers resulted in higher customer satisfaction. Armstrong, Laschinger, and Wong (2009) found workplace empowerment to be a significant predictor of patient safety (see also Lundmark & Hickey, 2006). Yeatts and Cready (2007), in their quasi-experiment examining the effects of empowered CNA teams, found positive effects on resident care. And more recently, Shield et al. (2013) surveyed employees and family members of NH residents in 33 NHs and concluded that empowering the DCWs was associated with higher service quality (see also Barden, Quinn, Donabue, & Fitzpatrick, 2011; Bowers & Nolet, 2014; Hamann, 2013; Koberg, Boss, Senjem, & Goodman, 1999). Still other studies have found positive effects on the employees themselves including the ability to be more flexible and implement their own ideas (Wichitchanya, 2013).
These many positive results have led to the incorporation of DCW empowerment into numerous “culture change” programs that are attempting to have a “patient-centered” focus of care (Shield et al., 2013). For example, the Eden Alternative (W. H. Thomas, 1994), the Green House Project (The Green House Project, n.d.), LEAP (Learn, Empower, Achieve, Produce; Hollinger-Smith et al., 2002), and the Wellspring Model (Fagan, 2003; Reinhardt & Stone, 2001) incorporate empowered DCWs into their programs. While much has been learned about the positive effects of empowering DCWs, less empirical study has examined the factors that lead to DCW empowerment, defined as shared decision-making (SDM) between DCWs and nurse managers. The purpose of this study is to assist in reducing this lack of knowledge by identifying factors that are associated with SDM.
Defining EE
There are at least three theoretical approaches to EE and each defines EE somewhat differently. The first theoretical approach to consider EE came primarily from management and organizational scholars who have defined EE as an employee’s ability to make her or his own decisions regarding the work. Major contributors have included McGregor (1960), Herzberg (1966), Deming (1982), Lawler (1986), Hackman and Oldham (1980), and Kanter (1986). Factors believed to contribute to EE have typically included “structural” or organizational and work design characteristics such as training, the reward system, availability of resources to DCWs, and work procedures. A second theoretical approach is typically referred to as “psychological” EE. Major contributors have included Bandura (1997), Conger and Kanungo (1988), K. W. Thomas and Velthouse (1990), Spreitzer (1995, 1996), and Kirkman and Rosen (1999). This approach defines EE at the individual level as a state of mind—if the employee believes she or he is empowered then empowerment exists (Kuokkanen & Leino-Kilpi, 2000). Factors contributing to psychological EE include a belief that one has the appropriate knowledge and skills to make decisions, that one has autonomy in the workplace, and the belief that the decisions being made are meaningful and have important impacts. A third and more recent theoretical approach has been presented primarily by health care researchers and defines EE as a “sharing” of decision-making. From this perspective, EE exists when DCWs and management are working together to make decisions. Major contributors to this perspective include Anthony (2004), Kramer et al. (2008), and Laschinger, Gilbert, Smith, and Leslie (2010). Factors believed to be particularly important to SDM include interpersonal characteristics such as information exchange, trust of management, and coworker support. Our research highlights this third definition of EE. That is, we have treated EE as SDM between DCWs and nurse managers.
Theoretical Approach Explaining SDM
The purpose of this study is to identify factors associated with SDM between DCWs and nurse managers in NHs using the three theoretical approaches noted above. We have placed structural, psychological, and interpersonal characteristics into four categories: organizational context, work design, interpersonal process, and personal characteristics. Each is reviewed below.
Organizational Context
Training, the reward system, and the availability of resources appear to have received the most attention among those examining organizational characteristics. Training has been viewed as having at least two major focuses, one on providing employees with the knowledge and skills needed to provide high-quality health care (Beck, Ortigara, Mercer, & Shue, 1999; McAiney, 1998; Owens, 2006) and the second on instilling within employees the interpersonal skills important to working with others (King, 2009; Kramer et al., 2008; Laschinger, Leiter, Day, Gilin-Oore, & Mackinnon, 2012; McPhee, Skelton-Green, Bouthillette, & Suryaprakash, 2011). Training has been found to be associated with a broad array of factors including EE (Coogle, Parham, Jablonski, & Rachel, 2007; Kirkman & Rosen, 1999; Yeatts, Cready, Swan, & Shen, 2010).
The reward system within a NH has been reported to enhance employee decision-making if it is designed to reward personal competencies, including participation in decision-making (Spreitzer, 1995; Wang, Zhang, & Jackson, 2013). Research suggests that compensation systems that reward employee responsibility, creativity, and initiative will also be rewarding employee characteristics important to decision-making (Laschinger et al., 2010). Wichitchanya (2013) has noted the importance of both intrinsic rewards such as praise and approval as well as extrinsic rewards such as pay increases (see also Kanter, 1979; Kramer et al., 2008). In addition, Koberg et al. (1999) have noted the ability of reward systems to point out the expectations that management has of its employees which can include their participation in decision-making.
Finally, access/availability to resources has been reported to be important to the decision-making process (Kanter, 1986, 1993). Making good decisions requires that the decision-makers have the specific kinds of materials, time, and space needed to develop an informed decision (Laschinger et al., 2010; Spreitzer, 1996). As Spreitzer (1996) has noted “a lack of access to critical organizational resources contributes to powerlessness and dependency” (p. 489; see also Davies, Wong, & Laschinger, 2011; Trus, Razbadauskas, Doran, & Suominen, 2012).
Work Design
Less research has examined the effects of work design on SDM. Work design characteristics include work procedures, feedback, resident assignments, and workload. Kirkman and Rosen (1997, 2000) have noted the need for work procedures to be effective for employees to be involved in decision-making. Work procedures that lack effective coordination and communication among nonmanagement employees make it difficult for them to make good decisions. Feedback to employees has been reported to affect EE through its ability to provide a variety of information useful for decision-making (Lucas et al., 2008; Wang et al., 2013; Wichitchanya, 2013). Furthermore, Conger and Kanungo (1988) have suggested that supportive, nonblaming feedback can encourage employees to believe in their capabilities and to subsequently participate in decision-making. McAiney (1998) has described the importance of resident assignments to the decision-making process. She has observed that the assignment of residents to DCWs is sometimes rotated frequently. This gives DCWs the advantage of knowing something about many different residents. It is a disadvantage because the DCWs have less knowledge about any one resident. McAiney has suggested that the better approach for making good decisions may be to reduce such rotations by making permanent assignments. Beck et al. (1999) has emphasized the negative effects of work overload. They have noted that DCW burnout can result as the workload increases and the DCW becomes more emotionally attached to the residents served. In this case, work overload might reduce DCW time given to SDM because of the large amounts of time needed for resident care and the subsequent DCW burnout.
Interpersonal Process
At least four interpersonal attributes have been identified as affecting SDM: support by management, trust of management, information exchange, and coworker support. Shield, Looze, Tyler, Lepore, and Miller (2013) have noted that management support for employees is shown by being receptive to their ideas, flexible, and a willing partner. Koberg et al. (1999) have described management support as providing employees with the means, ability, and authority to achieve success (see also King, 2009; Randolph, 1995; Wang et al., 2013; Campbell, 2003). Laschinger et al. (2010) noted that support by management is crucial to creating an empowered work environment for DCWs (see also Laschinger & Finegan, 2005; Williamson, 2008; Ejaz et al., 2008). Management trust is closely tied to support and has been studied extensively. Barton and Barton (2011) have reported that management support lays the foundation for employees to trust their managers. In a study of nine public schools, Myrick, Greer, and Melvin (1994) found a similar relationship—teachers reported high levels of empowerment when school principals had created an environment of trust between themselves and their teachers (see also Koberg et al., 1999). Kanter (1989) summarized the effects of trust by noting, “It is trust that makes partnerships work” (p. 89).
Information exchange is also important to EE. DCWs cannot be effective partners in decision-making if they lack essential information related to the decisions to be made (Anthony, 2004; Williamson, 2008). This information is sometimes available to nurse managers but not DCWs unless it is shared by the managers. Kanter (1989) has noted that managers must “make more information more available” for employees to make effective decisions (p. 5). Lawler (1986) has clarified that “without considerable information moving downward, employee participation and involvement become impractical and even dangerous” (p. 24; see also Laschinger et al., 2010). Hamann (2013) has noted that CNAs have valuable information that can be shared with nurse managers during the decision-making process. This includes information that can only be obtained from daily interactions with residents and their families from the time residents wake up in the morning to the time they prepare for bed in the evening. Thus, effective SDM is able to occur when NH management and CNAs share the information they possess and then use it when making decisions (Davies et al., 2011).
Coworker support has been described as a group of peers who work together, are committed to one another, are interdependent, and have a sense of camaraderie (Kirkman & Rosen, 1999; Koberg et al., 1999; Larkin, Cierpial, Stack, Morrison, & Griffith, 2008). While coworker support has received attention in the literature, there has been relatively little focus on coworker support and SDM. Sieloff (2004) has observed that coworker support among nurses can result in increased empowerment (see also Larkin et al., 2008; Laschinger et al., 2010). Unfortunately, no studies were uncovered that focused directly on the effects of coworker support on SDM when considering DCWs. However, it is reasonable to suspect that such support fosters an environment where DCWs encourage each other to participate in SDM with nurse management.
Personal Characteristics
Skills and knowledge, formal education, gender, and race are personal characteristics that have received attention from researchers studying EE. Employees who have a high level of work skills and knowledge have been reported to have the expertise needed to participate in decision-making (Chaudhuri, Yeatts, & Cready, 2013; Conger & Kanungo, 1988; Kirkman & Rosen, 2000; Williamson, 2008). A similar conclusion has been reached with regard to formal education (Koberg et al., 1999; Myrick et al., 1994; Shield et al., 2013). Conger and Kanungo (1988) have highlighted the effects of gender and race by noting an historical, cultural belief within the United States that White males are most suited to participate in decision-making (Chaudhuri et al., 2013). Such a belief can result in females and non-Whites deferring to their male counterparts, expecting more participation from White males during the decision-making process (Kanter, 1979; Koberg et al., 1999). This belief is reinforced by the overabundance of women occupying less powerful positions in the workplace, as is found within NHs (Chaudhuri et al., 2013; Kanter, 1979). Finally, there are a variety of other personal characteristics that have received attention as furthering empowerment in the workplace. These include self-esteem (Bradbury-Jones, Sambrook, & Irvine, 2008; Trus et al., 2012; Wang et al., 2013), maturity (Kirkman & Rosen, 2000), and an array of personality characteristics such as extroversion, ambition, sociability, high growth needs, preferences for empowerment, tolerance for flexibility and compromise, and an internal locus of control (Kirkman & Rosen, 2000; Yeatts & Hyten, 1998).
Design and Method
The purpose of this study is to identify factors associated with SDM between DCWs and nurse managers. Provided below is a description of the data collection procedures and the DCW participants, followed by a description of the questionnaire items, concepts, indices created, and data analysis techniques.
Data Collection and DCW Characteristics
The data come from a larger study focused on the empowerment of DCWs in NHs. A self-administered survey instrument was completed by 372 DCWs working within 11 NHs in the north Texas region. These questionnaires were typically distributed and collected by the research team at an “all-staff” meeting. Absentees were later contacted by a member of the research team and invited to participate. The 11 NHs were surveyed between 2002 and 2005. NHs were selected to allow for variation in size, private versus nonprofit status, location (urban, suburban, rural), and income level (percent of residents receiving Medicaid). The response rate was 78%. A complete description of the data collection procedures is provided by Yeatts and Cready (2007). The DCW respondents can be characterized as women, in their 30’s, having a high school education, and more than half were non-White. More specifically, 88% of the DCWs were women with an average age of 36, average years of education 11.9, and 52% non-White (Table 1).
Means and Standard Deviations for Organizational, Work Design, Interpersonal, and Personal Characteristics.
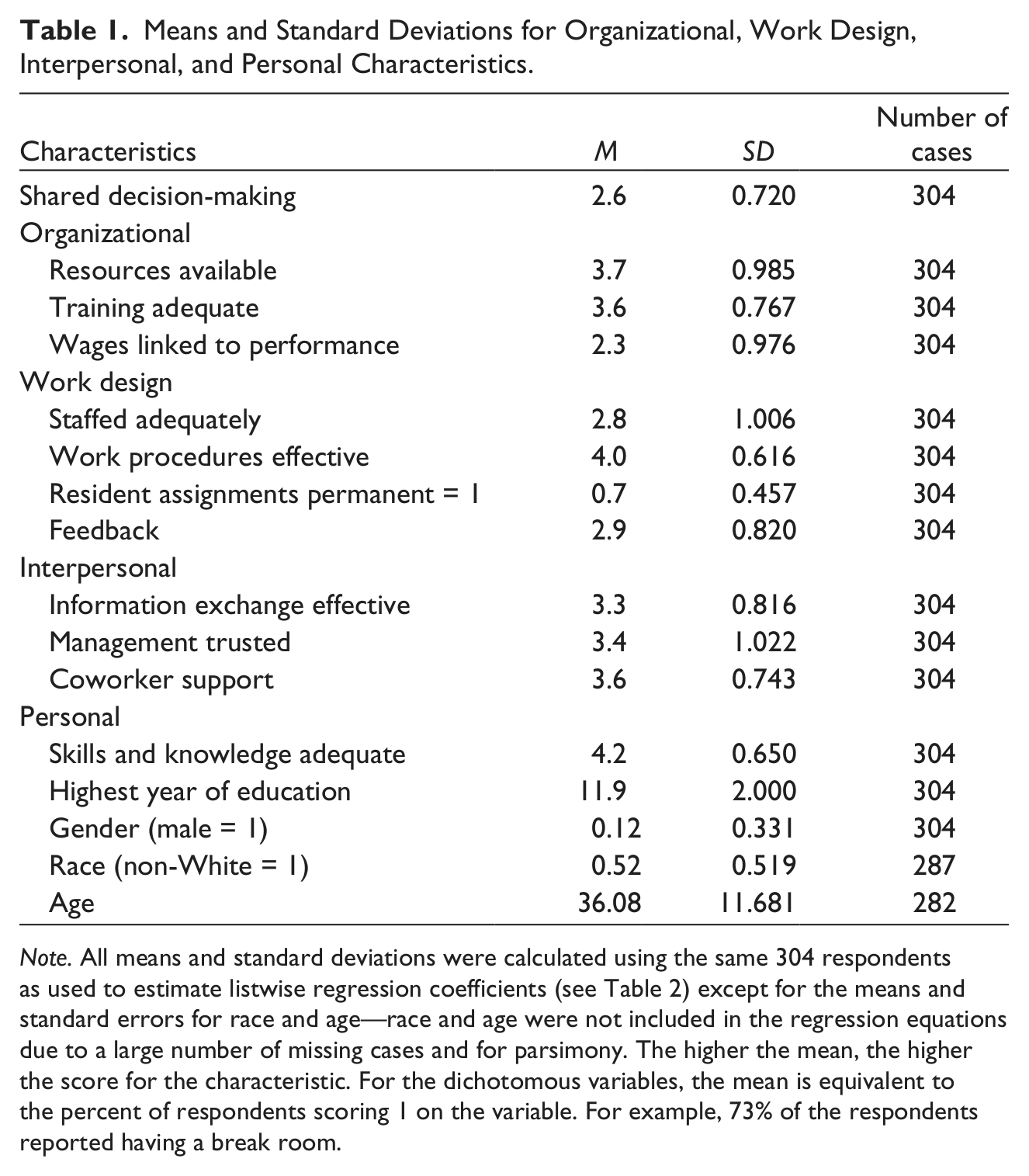
Note. All means and standard deviations were calculated using the same 304 respondents as used to estimate listwise regression coefficients (see Table 2) except for the means and standard errors for race and age—race and age were not included in the regression equations due to a large number of missing cases and for parsimony. The higher the mean, the higher the score for the characteristic. For the dichotomous variables, the mean is equivalent to the percent of respondents scoring 1 on the variable. For example, 73% of the respondents reported having a break room.
Questionnaire Items, Concepts, and Indices
The DCWs responded to a series of statements by using a 5-point Likert-type scale ranging from 1 for strongly disagree to 5 for strongly agree. Many of these items were drawn from existing instruments that measure the concepts of interest, including those developed by Cook, Hepworth, Wall, and Warr (1979); Hackman and Oldham (1980); Quinn and Staines (1979); Spreitzer (1995); and Yeatts and Hyten (1998). When necessary, statements were modified to reflect the uniqueness of the NH environment. When measures could not be found in previous studies, items were developed and pretested.
For most concepts of interest, at least three questionnaire items were used to create indices to represent them (see Appendix A for all statements used). The dependent variable (DV), SDM, was based on statements such as “I work with management staff in making decisions about my work.” Organizational characteristics included training, the reward system, and available resources. A variety of statements were used. For example, availability of resources was measured by statements such as the following: “When working, I usually have all the supplies and work materials I need to do a good job (such as towels, gowns, etc.).” Three of the four work design variables were also measured by a variety of statements for each. For example, one of the statements for workload states as follows: “There are usually enough CNAs working to do a good job.” The work design variable, “resident assignments permanent,” was measured by a single question and coded zero (0) where resident assignments were not permanent and one (1) where assignments were permanent. The interpersonal characteristics were similarly measured by a variety of statements for each. For example, coworker support was measured by statements such as the following: “I can trust the other nurse aides I work with to lend me a hand if I need it.” Finally, personal characteristics were obtained by asking respondents to provide their gender, age, race, and highest grade level completed. Skill and knowledge level was obtained with the following statement: “I have all the skills and knowledge I need to do a good job and I use them.” Appendix A provides the concepts measured, items used for each concept, and the Cronbach’s alpha for each. Appendix B provides the bivariate correlations for all the variables considered.
Exploratory and confirmatory factor analyses were used to identify and confirm the ability of the items to reflect a particular concept. The standardized Cronbach’s alphas for the indices ranged from .68 to .88 with most above .70 (see Appendix A). Once the items for an index were determined, the individual scores on each item were added together and divided by the number of items. This calculation allowed the index score to remain in the original range of the individual items (i.e., 1 to 5 or strongly disagree to strongly agree).
Data Analysis
A variety of checks for outliers were performed on the data. Given the length of the questionnaire (113 items), there was some concern that some DCWs may not have read all statements carefully. To test for this problem, three pairs of statements were included in the questionnaire with each statement in a pair identical or with one of the two worded in the opposite direction (positive statement vs. negative statement). If the respondent was not consistent in his or her responses for at least two of the three pairs of questions, the case was removed from the analysis. As a result, nine cases were removed. Furthermore, multivariate outliers were checked by examining Mahalanobis distance measures and box plots. The most extreme cases were examined for possible typing errors or cases in which the respondent did not follow the instructions. Subsequently, two cases were removed. Finally, listwise removal of missing cases was used for the regression analyses, resulting in 305 DCWs being included in all analyses. Race and age were not included because of the relatively large number of missing responses for each.
Analytical strategy
The DCWs were working at 1 of 11 NHs (i.e., 11 clusters). Therefore, tests were run to determine whether a multilevel, cluster analysis was most appropriate. Peugh (2010) and others recommend ignoring the cluster variable if the model’s design effect (DEFF) is 2.0 or less (DEFF equals the standard error with nested random effects divided by the standard error without random effects). Hox and Maas (2002), Muthen and Satorra (1995), and others have taken a more conservative approach that a DEFF less than 1.1 indicates little to no effect of the cluster variable so that there is no need to adjust for it. Our analyses found the DEFFs of the 11 NHs to range from .8 to 1.1 indicating that a single-level analysis is most appropriate with no need to adjust for the cluster variable. We chose to use Stata’s “svy” command (a widely accepted procedure) to adjust for any potential cluster effect and thus reduce the chances of underestimating the standard errors (Huang, 2014, p. 4). An underestimated standard error can lead to underestimating uncertainty in the results, leading to confidence intervals that are too small, and thus spuriously statistically significant results (i.e., inflated Type 1 error rates; Hox, 2010; Lai & Kwok, 2014; Snijders & Bosker, 2012). Furthermore, Lai and Kwok (2014) in their simulation studies concluded that adjusting for clustering in single-level analyses may be the more preferable option when there are 20 or fewer clusters even when DEFF is small and very close to 1.
Unfortunately, adjusting for cluster effects makes problematic the calculation of beta scores. The standardized regression coefficients, or beta scores, are typically used in ordinary least squares (OLS) regression to examine the relative effects of the independent variables (IVs). A beta score refers to how many standard deviations the DV will change, per standard deviation increase in the IV, controlling for the other IVs in the model. There are a number of other statistical procedures for calculating relative effects while adjusting for clustering, such as standardizing respondent scores, but each appears to have shortcomings and no one procedure is widely accepted by the social science statistics community. Therefore, to obtain some insight into the relative effects, we present betas calculated from the unadjusted OLS regressions. This procedure should be followed only when unadjusted regressions and regressions adjusted for clustering are minimally different with regard to their standard errors and p values. An examination of the results found this to be true. This finding came as no surprise based on our earlier analysis of DEFFs. Thus, in Table 2, we report the unadjusted OLS betas as we have confidence in these, and we report the p values from regressions adjusted for clustering as these are expected to be the most accurate p values. However, for dummy-coded dichotomous variables, Fox (1997) and others have noted that the usual interpretation of standardized estimates (βs) does not apply as they cannot be increased by one standard deviation. Consequently, the dummy variables “permanent resident assignments” and “gender” were included in the regression equations but beta estimates were not calculated for them.
Regression Models Adjusted for Clustering Examining the Effects of Organizational, Work Design, Interpersonal, and Personal Characteristics on Shared Decision-Making.
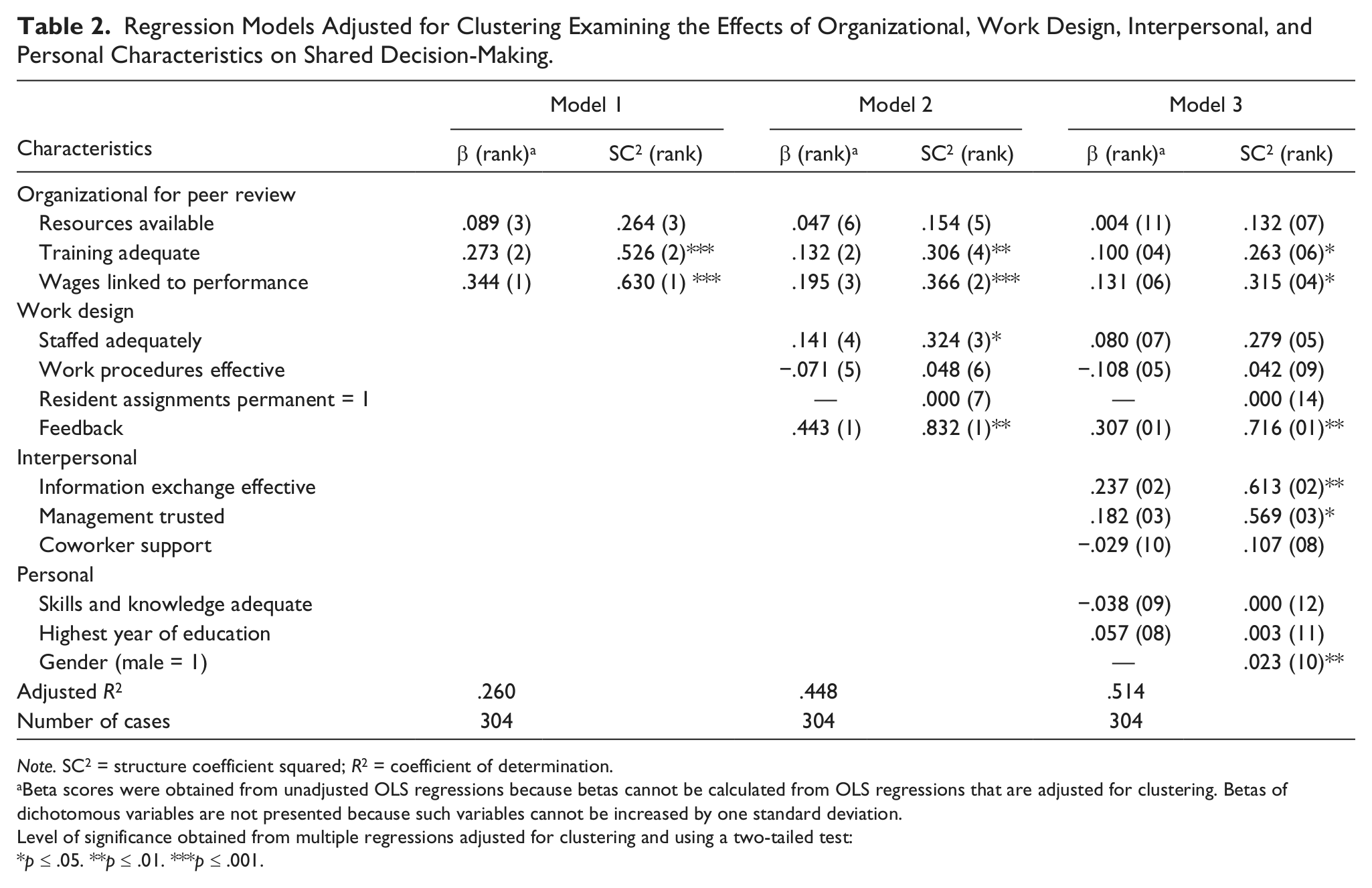
Note. SC2 = structure coefficient squared; R2 = coefficient of determination.
Beta scores were obtained from unadjusted OLS regressions because betas cannot be calculated from OLS regressions that are adjusted for clustering. Betas of dichotomous variables are not presented because such variables cannot be increased by one standard deviation.
Level of significance obtained from multiple regressions adjusted for clustering and using a two-tailed test:
p ≤ .05. **p ≤ .01. ***p ≤ .001.
Also reported are structure coefficients squared (SCs2; Table 2). Beta weights can lead to erroneous conclusions when even a small amount of multicollinearity exists between one or more IVs. In these cases, the shared explanatory power for the variation in the DV is assigned to only one of the two correlated IVs. Consequently, among two correlated IVs, one can appear to have a significant effect and high correlation with the DV, while the second can appear to have no significant effect and little correlation with the DV. As Courville and Thompson (2001) have noted, “a predictor (IV) may have a large absolute correlation with Y (DV) but have a zero beta weight, if one or more other correlated predictors (IVs) are assigned credit for that predictor’s shared explanatory ability” (p. 231). SCs avoid this shortcoming by providing the correlation between an IV and DV that is not reduced by any multicollinearity or shared association with one or more other IVs. If there is no multicollinearity between IVs, then the beta scores and the SCs will be ranked identically with regard to level of association with the DV. On the contrary, if an IV is correlated with one or more other IVs, then its SC ranking may differ substantially from its beta ranking. Tolerance checks of the data revealed no substantial levels of multicollinearity among the IVs. Nevertheless, SCs can help to identify cases where the association between an IV and the DV are hidden by the IVs correlation with one or more other IVs. Therefore, we chose to include SCs in the analysis. Squaring the SC of an IV provides more intuitive understanding of the relationship between the IV and DV. A squared SC is directly related to the total variation explained by the IV. More specifically, a squared SC provides an IV’s contribution to the total variation explained. For example, if an IV’s SC2 equals .50, this would indicate that the IV accounts for 50% of the total variation explained by all the IVs. Of course, some, all, or none of this contribution could be shared with the other IVs depending on the level of multicollinearity between IVs.
Table 2, Model 1 examines the effects of organizational characteristics, Model 2 adds work design, and Model 3 adds interpersonal and personal characteristics. The adjusted coefficient of determination or adjusted R2 provides a measure of “goodness of fit” of a model to the actual data after adjusting for the number of variables in the regression model (a large number of variables in the regression model can artificially inflate the R2). The adjusted R2 represents the total amount or percentage of variance in SDM explained by the IVs included in the model. The three models are compared to determine which model provides the best fit to the data, that is, provides the most explanation for the variation in SDM.
Results and Discussion
The first theoretical approach to EE focused on the structure or organizational systems within the organization, including training, rewards, and the decentralization of resources to employees (Hackman & Oldham, 1980; Kanter, 1989; Lawler, 1986). An examination of the DCW responses provides strong support for this theoretical perspective. When only the three organizational characteristics are considered (Table 2, Model 1), two of the three were found to be significant with 27% of the variation in SDM explained. When controlling for the work design, interpersonal and personal variables (Table 2, Model 3), these two organizational characteristics remained significant. Those DCWs who reported having training available whenever it was needed were more likely to be participating in SDM after holding all other variables constant. This was expected as workers with training were believed to garner the support of nurse managers and have the expertise and confidence needed to participate in decision-making (Laschinger et al., 2012; McAiney, 1998). Similarly, “wages linked to performance” had a significant positive association in all three models (Table 2) and was ranked fourth among the SCs2 in level of association with SDM. This supports the conclusions of Lawler (1986), Spreitzer (1995), and others that when wages are linked to performance, employees seek ways of improving their performance such as by participating in decision-making.
The second theoretical approach to EE led to the study of work designs within the organization including examinations of feedback, work procedures, adequate staffing, and resident assignments. Our findings suggest that work design is important to SDM, with an additional 19% of the variation explained beyond that of the organizational characteristics. Two of the four work design characteristics were significant when considering only organizational and work design variables (Table 2, Model 2). Feedback was found to have the strongest association with SDM, after controlling for the other IVs (Table 2, Models 2 and 3). Feedback was measured by whether nurse management listens to DCWs and provides DCWs with explanations when DCW suggestions are not used (Appendix A). When DCWs received this type of feedback, they were more likely to report participation in SDM, supporting previous research (Wang et al., 2013; Wichitchanya, 2013).
Adequate staffing was found to be positively associated with SDM before interpersonal and personal characteristics were added to the model (Table 2, Model 2) but no longer significant once these additional variables were added (Table 2, Model 3). Unlike the conclusions in previous research (Beck et al., 1999), this suggests that the lack of adequate staffing did not prevent the DCWs from participating in SDM. Resident assignment (i.e., ranging from no permanent assignments to all residents being permanently assigned to DCWs) also showed no association with SDM. This does not support the proposition that knowing more about a smaller number of residents (i.e., permanent assignments) is more conducive to SDM (McAiney, 1998).
Most recently researchers have turned their attention to psychological empowerment, emphasizing the importance of interpersonal characteristics to SDM (Anthony, 2004; Kanter, 1989). The data strongly support this perspective with two of the three interpersonal characteristics significantly associated with SDM (Table 2, Model 3). Findings show that effective information exchange, such as DCWs obtaining resident information directly from nurses rather than relying on the “grapevine,” was the variable with the second highest beta and second highest SC2. When nurse management was providing DCWs with the information that was requested or needed by DCWs then DCWs were more likely to report their involvement in decision-making. Conversely, where there was a lack of effective information exchange, that is, information was not easily available from nurse managers, DCWs were less likely to report participation in SDM.
Trust in management has also been reported as essential to EE (Kanter, 1989; Myrick et al., 1994). It has been hypothesized that DCWs will not participate in decision-making if they do not feel they can trust management to support them in their efforts. The data again support this view (Table 2, Model 3). Trust in management was ranked third when examining beta scores and SCs2. A third interpersonal characteristic, coworker support, was not found to be associated with SDM. This suggests that SDM between nurse management and the DCW did not depend on whether the DCW could rely on and/or trust her coworkers.
A review of the literature showed that personal characteristics have also been associated with SDM. It has been reported that nonmanagement employees, as well as managers, have traditionally been socialized to believe that men should be a part of the decision-making process while women “take a back seat” (Conger & Kanungo, 1988; Kanter, 1979). The data support this view. Males were more likely to report participating in SDM than females. However, the SCs2 indicate that this significant association was relatively small with gender accounting for only 2% of the total variation explained by the IVs and a SC2 ranking of 10 among the 13 IVs. Surprisingly, skills and knowledge were not found to have an association with SDM (Table 2, Model 3). This does not support the work of others who have suggested otherwise (Conger & Kanungo, 1988). Perhaps the skills and knowledge “needed to do a good job” as stated in the questionnaire (Appendix A) are not the same as those needed for SDM.
The IVs collectively explained 51% of the variation in SDM, which is high. The most important variables identified were feedback (β = .307; SC2 = .716), information exchange (β = .237; SC2 = .613), and management trust (β = .182; SC2 = .569). This suggests that it was the work design and interpersonal relationships between nurse management and DCWs that were most important to SDM. However, organizational characteristics were also important, including having wages linked to performance (β = .131; SC2 = .315) and the availability of training (β = .100; SC2 = .263). Personal characteristics appeared to be less important for SDM, with gender having a small relative association with SDM (SC2 = .023) and education and skills and knowledge having no significant effect.
Limitations
Financial resources did not allow for a national random sample of DCWs. Consequently, the validity of generalizations from the 304 DCWs working in North Texas to the DCWs throughout the United States may be limited. Furthermore, the DCWs provided their perceptions of the variables measured. Consequently, to the extent that they were uninformed on any particular variable, their perceptions may have been less than accurate. Ideally, we would have had additional measures of the variables, such as “adequate skills and knowledge” to verify the DCWs’ perceptions.
Because the analysis is cross-sectional (one point in time), the associations between the IVs and SDM cannot be assumed to be causal in nature. In addition, when relevant IVs are left out of a regression model, the beta coefficients of those IVs included in the model will be affected (i.e., specification error). Consequently, the reported beta coefficients must be viewed tentatively. Fortunately, studies have demonstrated that OLS regression is robust (able to accommodate some violation of regression assumptions).
Conclusion
Numerous studies have demonstrated the positive effects of SDM on employee performance (Armstrong et al., 2009; Barden et al., 2011; Barry et al., 2005; Wichitchanya, 2013). This has encouraged NH managers to search for means of empowering their workers through SDM and has resulted in a variety of management strategies (e.g., the Eden Alternative, LEAP, and The Greenhouse Project). Results from this study suggest that the factors having the highest association with SDM include nurse management feedback to DCWs, the routine provision of information to DCWs, and a trusting relationship between nurse management and DCWs. In other words, DCWs may be more likely to participate in SDM when nurse management shares relevant information, listens to DCW ideas, and discusses the ideas with the DCWs. Furthermore, when DCW suggestions are not used, it is important that the DCWs be provided with reasons for why they were not used in a way that demonstrates nurse management respect for the DCWs. The results also indicate that organizational characteristics are important to the empowerment of DCWs including a training program that emphasizes the value and importance of SDM and DCW wages that are linked to their performance.
Footnotes
Appendix A
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Commonwealth Fund 10.13039/100000905.