
Abstract
Introduction
Hearing deficits are common in older adults; however, the prevalence of hearing loss doubles with every age decade, such that by the age of 70, two-thirds of adults are hearing impaired (Lin, Niparko, & Ferrucci, 2011; Lin, Thorpe, Gordon-Salant, & Ferrucci, 2011). Individuals with hearing loss have been shown to have poorer health outcomes, including decreased cognitive function (Lin, Ferrucci, et al., 2011; Lin et al., 2013; Valentijn et al., 2005), quality of life (Ciorba, Bianchini, Pelucchi, & Pastore, 2012; Wallhagen, Strawbridge, Shema, Kurata, & Kaplan, 2001), and mobility (Chen, Genther, Betz, & Lin, 2014).
Mental health is a key component of healthy aging. The estimated prevalence of anxiety disorders ranges from 9.2% to 28.7% with the highest rates in older adults (Somers, Goldner, Waraich, & Hsu, 2006). Limited research has examined how hearing loss may affect anxiety (Chung, Hung, Lin, & Sheu, 2015; Fellinger, Holzinger, Gerich, & Goldberg, 2007; Nachtegaal et al., 2009; Tambs, 2004). Hearing impairment (HI) could plausibly contribute to anxiety and poor mental health outcomes through mediating pathways of cognitive impairment (Lin, Ferrucci, et al., 2011; Lin et al., 2013; Valentijn et al., 2005), social isolation (Mick, Kawachi, & Lin, 2014), or disability (Chen et al., 2014). Sensory deprivation has also been proposed as a possible cause for anxiety and mood disturbances (Gilmartin, Grota, & Sousa, 2013; Heine & Browning, 2002). Alternatively, shared common etiologic factors such as age, cardiovascular disease (Gates, Cobb, Dagostino, & Wolf, 1993), or other demographic factors (Agrawal, Platz, & Niparko, 2008) could underlie any observed association between HI and anxiety.
In this study, we investigated whether HI, objectively measured with audiometry, was associated with anxiety symptoms in a population of U.S. community-dwelling older adults followed in the Health, Aging and Body Composition (Health ABC) study. Self-reported measures, derived from a validated screening tool (Bech, Bille, Moller, Hellstrom, & Ostergaard, 2014) were used to assess anxiety. We hypothesized that greater HI is associated with greater anxiety symptoms, independent of demographic and cardiovascular risk factors.
Method
Study Design and Population
We conducted a cross-sectional analysis of data from the Health ABC study, a prospective observational study that enrolled 3,075 well-functioning, community-dwelling older adults aged 70 to 79 from 1997 to 1998 (aged 76-85 years at Study Year 6; Simonsick et al., 2001). Study participants were recruited from a random sample of White and Black Medicare beneficiaries living in Pittsburgh, Pennsylvania and Memphis, Tennessee. Only White and Black individuals were recruited because one of the original study objectives was to examine race-related differences in body composition parameters, and resources were insufficient to include other races. To be eligible, participants had to report no difficulty walking a quarter of a mile, climbing 10 steps without resting, or performing basic activities of daily living. Our analytic cohort was composed of individuals who completed audiometric testing administered in Year 5 and anxiety assessments measured in Year 6 (n = 1,732). Participants were excluded from our analysis for various causes (evidence of cognitive impairment indicated by Modified Mini-Mental State examination [3MS] score < 80 at study enrollment [n = 149; Teng & Chui, 1987], inability to complete hearing testing [n = 500], death prior to Year 6 [n = 378], withdrawal from study prior to Year 6 [n = 12], missed anxiety measures in Year 6 [n = 273], or missing covariates [n = 31]). Compared with the individuals excluded from our analytic cohort, study participants were more likely to be younger, White, higher educated, and former smokers. All participants provided written informed consent, and the institutional review boards of both sites approved this study.
Audiometry
Air conduction thresholds were obtained in each ear from 0.25 to 8 kHz with supra-aural headphones (TDH 39; Telephonics Corporation) using an audiometer (MA40; Maico Diagnostics) in a sound-proof booth and calibrated to American National Standards Institute standards (ANSI/ASA S3.6-1996). We calculated a speech-frequency pure tone average (PTA) using audiometric thresholds at 0.5, 1, 2, and 4 kHz in the better-hearing ear in accordance with the World Health Organization-established cutoffs for clinically significant hearing loss (i.e., none < 25 dB HL, mild 25-40 dB HL, moderate or greater > 40 dB HL; World Health Organization, 2014).
Anxiety
Anxiety symptom measurements were derived from the validated Hopkins Symptom Checklist (Parloff, Kelman, & Frank, 1954). Three questions addressing anxiety were used: “During the past week: (a) have you felt fearful; (b) have you felt nervous/shaky inside; and (c) have you felt tense/keyed up?” These questions were answered on a 4-level ordinal scale: no, a little, quite a bit, or a lot. Previous research has demonstrated the utility of the abbreviated Hopkins Symptom Checklist, varying between three to four questions, as a screening tool for anxiety symptoms (Brenes, Guralnik, Williamson, Fried, & Penninx, 2005; Mehta et al., 2007; Tambs 2004). Based on previous studies (Kasper & Simonsick 1995; Mehta et al., 2003; Simonsick, Guralnik, & Fried, 1999), we defined individuals as having anxiety symptoms if they rated any two symptoms as at least “a little” or any one symptom as at least “quite a bit.”
Covariates
At enrollment (Year 1), participants reported their age, sex, race, and educational history. Participants were also identified at enrollment as having hypertension or diabetes if they reported ever being told so by a physician, if diagnosed during the clinical visit, or if they recorded taking medications for either condition (Lin et al., 2013). Stroke history was assessed by the question, “Has the doctor ever told you that you had a stroke, CVA, cerebrovascular accident, TIA, transient ischemic attack or mini-stroke?” Smoking status, defined as current, former, or never, was based on an interviewer-administered questionnaire. These cardiovascular risk factors and demographic characteristics are known to be associated with HI (Linssen, van Boxtel, Joore, & Anteunis, 2014) and were included as covariates in our analytic model to adjust for potential confounding. At Year 5, participants’ hearing aid use was assessed by the interviewer-administered question, “Do you wear a hearing aid?” with potential answers, “yes, no, or don’t know.” Depressive symptomatology was measured in Year 6 and defined as a score >15 on the validated 20-item Center for Epidemiologic Studies Depression Scale (CES-D; Radloff, 1977).
Statistical Analysis
Baseline characteristics of participants were compared using the Kruskal–Wallis test and Fisher’s exact test where appropriate. The relationship between HI and anxiety was analyzed using logistic regression. Models were sequentially adjusted for demographic characteristics (age, sex, race, and education) and cardiovascular risk factors (smoking status, hypertension, diabetes, and stroke). As a sensitivity analysis, depression (CES-D) was added as a covariate to our final model. This is because previous studies have suggested an association between HI and depression (Li et al., 2014; Mener, Betz, Genther, Chen, & Lin, 2013), and anxiety and depression can overlap in their clinical presentation; hence, it is unclear whether depression is truly a confounder of the association between HI and anxiety. Effect modification was evaluated through stratification by sex, as women are 70% more likely than men to experience an anxiety disorder and may be more susceptible to the effects of HI on anxiety (McLean, Asnaani, Litz, & Hofmann, 2011). As a secondary analysis, hearing threshold was treated as a continuous variable. A threshold of two-tailed p value < .05 was considered statistically significant. All analyses were conducted in Stata SE 12 (StataCorp, College Station, Texas).
Results
Our analytic cohort comprised 1,732 adults characterized in Table 1. Participants with mild HI (n = 649) and moderate or greater HI (n = 352) were more likely to be older, male, White, less educated, enrolled at the Memphis site, and have a history of smoking than participants with no HI (n = 731). There was no difference in history of hypertension, diabetes, or stroke between individuals with and without HI.
Baseline Characteristics of Analytic Cohort.
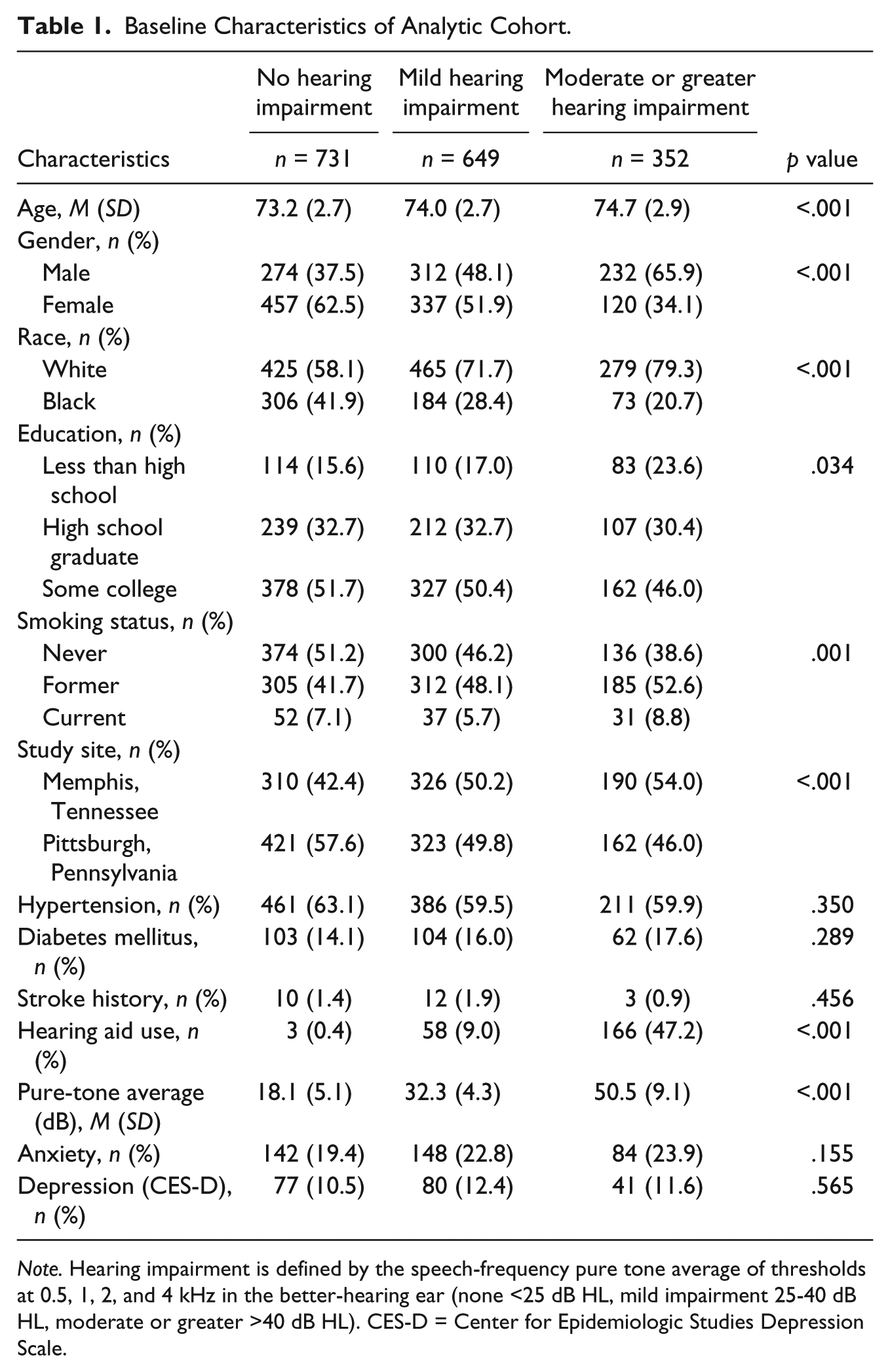
Note. Hearing impairment is defined by the speech-frequency pure tone average of thresholds at 0.5, 1, 2, and 4 kHz in the better-hearing ear (none <25 dB HL, mild impairment 25-40 dB HL, moderate or greater >40 dB HL). CES-D = Center for Epidemiologic Studies Depression Scale.
The association between HI and anxiety was investigated through logistic regression models adjusted for demographic (age, sex, race, and education) and cardiovascular risk factors (history of stroke, smoking, diabetes, and hypertension; Table 2). In the fully adjusted model, we observed that the odds of anxiety were higher among individuals with mild HI (OR = 1.32, 95% CI = [1.01, 1.73]) and with moderate or greater HI (OR = 1.59, 95% CI = [1.14, 2.22]) compared with individuals with no HI. Secondary analysis of hearing threshold as a continuous variable yielded similar results—each 10 dB increase in PTA was associated with a 12% higher odds of prevalent anxiety (OR = 1.12, 95% CI = [1.02, 1.23]). Additional analyses stratified by sex yielded similar results in men and women (women: mild HI OR = 1.26, 95% CI = [0.91, 1.75], moderate or greater HI OR = 1.68, 95% CI = [1.07, 2.62]; men: mild HI OR = 1.51, 95% CI = [0.92, 2.51], moderate or greater HI OR = 1.65, 95% CI = [0.96, 2.84], compared with no HI). Our results were not substantially attenuated by adjustment for depression (mild HI OR = 1.28, 95% CI = [0.96, 1.70]; moderate or greater HI OR = 1.6, 95% CI = [1.12, 2.27]).
Odds of Anxiety by Hearing Impairment Category.
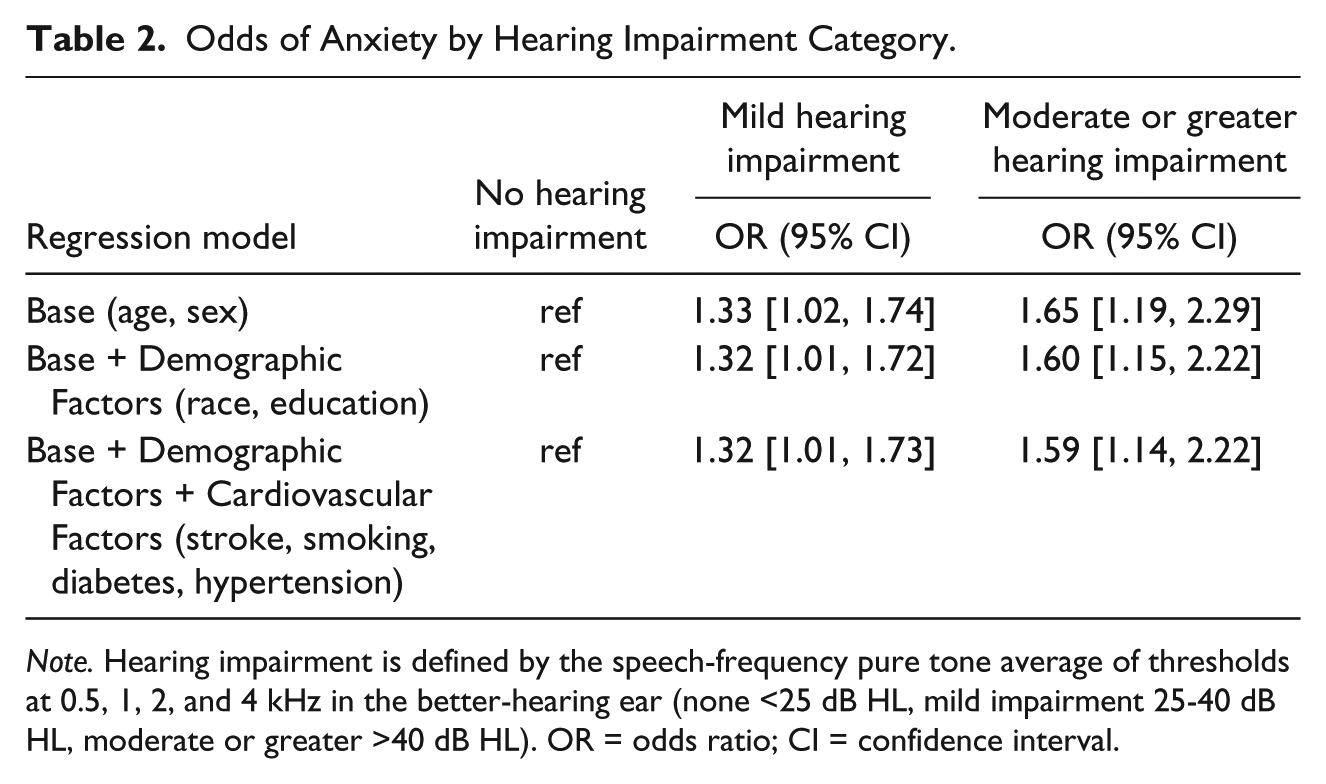
Note. Hearing impairment is defined by the speech-frequency pure tone average of thresholds at 0.5, 1, 2, and 4 kHz in the better-hearing ear (none <25 dB HL, mild impairment 25-40 dB HL, moderate or greater >40 dB HL). OR = odds ratio; CI = confidence interval.
To explore whether hearing aid use was associated with lower anxiety, we included hearing aid use as a variable in a model restricted to individuals with HI (n = 1,001, 22.4% reporting hearing aid use [Table 1]). Among individuals with mild HI (n = 649) and moderate or greater HI (n = 352), hearing aid use was not significantly associated with a lower odds of anxiety (mild HI OR = 0.86, 95% CI = [0.48, 1.56]; moderate or greater HI OR = 0.85, 95% CI = [0.50, 1.43]; all HI OR = 0.93, 95% CI = [0.66, 1.31]).
Conclusion
Our results demonstrate that HI is independently associated with anxiety in community-dwelling older adults with individuals with mild HI having 32% higher odds of anxiety, and individuals with moderate or greater HI having 59% higher odds of anxiety compared with individuals with no HI. Our results were robust to adjustment for multiple potential confounders.
Although several studies have explored an association between HI and depression (Li et al., 2014; Mener et al., 2013), few have examined other mental health outcomes. In a large survey of Norwegian adults aged 20 to 101 years, Tambs (2004) identified a moderate association of HI with anxiety only in adults 20 to 64 years of age, but did not find an association with adults >65 years of age. This cross-sectional study also utilized the Hopkins Symptom Checklist but did not identify a significant association of hearing and anxiety in adults aged >64 years. This lack of association may be secondary to survey non-response bias (response rate of 69%), treatment of positively skewed anxiety score as a continuous variable, or differences in cross-cultural factors that may influence the association between HI and anxiety in older adults.
A Dutch study examining the association of HI, identified by an online speech-in-noise screening test, and anxiety in 1,511 adults 18 to 70 years of age suggested a potential link, but failed to reach the threshold for statistical significance (Nachtegaal et al., 2009). This may be a result of a contrast between hearing loss in younger adults (often congenital) versus older adults (often age-related). A population-based study in Taiwan compared the prevalence of anxiety disorder in 3,522 adults diagnosed with sudden sensorineural hearing loss with 10,566 matched controls (Chung et al., 2015). They found that individuals with sudden sensorineural hearing loss were 1.49 times more likely than controls to have been diagnosed with anxiety disorder. This is consistent with our ORs, although it is likely that both hearing loss and anxiety disorders were under diagnosed in this population. These studies suggest that the etiology of the hearing loss may be important to the impact on anxiety symptoms, with post-lingual hearing loss seeming to have a greater association with anxiety.
A cross-sectional study from Ireland found that HI was associated with clinically diagnosed “depressive-anxiety syndrome” in adults aged 75 years or greater (Bernabei et al., 2011). However, this study, as well as several others assessing mental health (Gomaa, Elmagd, Elbadry, & Kader, 2014; Jones, Victor, & Vetter, 1984), used subjective self-reported measures of hearing loss, which have low sensitivity for identifying HI (Kamil, Genther, & Lin, 2014). Audiometrically measured HI is particularly important in studying anxiety because individuals who subjectively report anxiety symptoms may be more likely to report a concern for hearing loss (Tambs, 2004).
Several mechanisms could explain the observed association between HI and anxiety. Microvascular disease has been associated with both hearing loss (Gates et al., 1993) and poorer mental health (Taylor, Aizenstein, & Alexopoulos, 2013), suggesting its possibility as a confounder. Likewise, demographic factors, such as age, sex, and education, could underlie the association. However, our results were adjusted for multiple demographic characteristics and cardiovascular risk factors (i.e., stroke, smoking, diabetes, and hypertension). Alternatively, the association of HI with poorer anxiety outcomes could be mediated through other mental health factors, such as social isolation and sensory deprivation. The role of depression in the association between HI and anxiety is uncertain. Although depression and anxiety are correlated among older adults (Mehta et al., 2003), there is minimal evidence to suggest depression serves as an intermediate or confounder of the relationship. Notably, the addition of depressive symptoms as a covariate in our final model did not mitigate the association between HI and anxiety.
In the present study, we observed that individuals using hearing aids had 15% lower odds of anxiety compared with individuals with HI who did not use a hearing aid, although these results were not statistically significant. Our cohort was likely underpowered to detect a statistically significant association. Furthermore, hearing aid use was reported as a binary variable and did not include key mediators (e.g., hours worn/day, years of use, communication strategies used) that could influence the strength of association (Knudsen, Oberg, Nielsen, Naylor, & Kramer, 2010). Longitudinal studies with a more precise measurement of hearing aid use would be necessary to determine whether hearing rehabilitation could affect anxiety among older adults with HI.
Our study has limitations. We cannot establish the temporal relationship between hearing loss and anxiety based on our cross-sectional results, and further longitudinal research is warranted. Three items from the validated Hopkins Symptom Checklist were used for anxiety symptomatology versus a clinical diagnosis or a more comprehensive screening questionnaire. Still, this method is comparable with numerous studies analyzing anxiety in older adult populations (Brenes et al., 2005; Kasper & Simonsick, 1995; Mehta et al., 2003; Mehta et al., 2007; Simonsick et al., 1999). Covariates (Year 1) and audiometry (Year 5) were recorded prior to the anxiety measurement in Year 6, although these factors are unlikely to significantly change over the course of several years. Our analytic cohort made up 56% of the original study population. The age range of the participants was fairly narrow (76-85 years), potentially limiting the generalizability of this study to all adults. Residual confounding by unmeasured factors (e.g., socioeconomic factors, work status, lifestyle factors, or other comorbidities) is also plausible.
In conclusion, our results demonstrate that HI, a highly prevalent condition in older adults, is associated with greater anxiety, independent of demographic characteristics and cardiovascular risk factors. As greater attention is focused on the mental health of an aging population, future research is necessary to elucidate the mechanistic pathways between HI and anxiety, and to determine whether outcomes are improved with hearing rehabilitative therapies.
Footnotes
Authors’ Note
The contents of the article are solely the responsibility of the authors.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Frank Lin reports being a consultant to Cochlear, on the scientific advisory board for Autifony and Pfizer, and a speaker for Med El and Amplifon.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This article was supported in part by the Eleanor Schwartz Charitable Foundation; a Triological Society/American College of Surgeons Clinician Scientist Award; the Johns Hopkins Institute for Clinical and Translational Research; the National Institutes of Health (NIH; Grant Numbers K23DC011279, TL1 TR001078); the National Institute on Aging (NIA; Grant Number R01-AG028050, and Contract Numbers N01-AG-6-2101, N01-AG-6-2103, and N01-AG-6-2106); National Institute of Nursing Research (Grant Number R01-NR012459); and the NIH Intramural Research Program.