
Abstract
Introduction
The ability to predict decrements in performance of everyday tasks has great salience for community-dwelling older adults, their families, caregivers, and health care providers. Older adults who report difficulty or have modified the way that they perform everyday tasks are at high risk for disability (Fried, Young, Rubin, & Bandeen-Roche, 2001; Wolinsky et al., 2007). Disability is defined as dependency in mobility, activities of daily living (ADLs), and instrumental activities of daily living (IADLs) necessary for living independently (Fried, Ferrucci, Darer, Williamson, & Anderson, 2004). Disability in older adults is associated with adverse outcomes such as higher health care costs and higher rates of institutionalization and mortality (Fried & Guralnik, 1997; Guralnik, Alecxih, Branch, & Weiner, 2002). In older adults with chronic health conditions, the onset of disability is often a subtle yet progressive process that may go unrecognized until the disability is severe (Fried et al., 1996). Adverse outcomes can potentially be reduced through early identification and interventions for disability (Gill, Robison, & Tinetti, 1997).
For many older adults with chronic health conditions, the quality of performance in mobility, ADL, or IADL tasks may decline prior to the actual onset of disability. Fried, Herdman, Kuhn, Rubin, and Turano (1991) proposed that subtle changes in task performance precede the onset of disability; these subtle changes may represent an intermediate phase prior to loss of function termed “preclinical disability.” Individuals who demonstrate preclinical disability are more likely to experience future loss of functional independence (Fried, Bandeen-Roche, Chaves, & Johnson, 2000). Independence in task performance can be described as the performance and completion of a task “in the manner or within the range considered for a normal human being” (World Health Organization, 2001, p. 28). To maintain independence, older adults who experience preclinical disability may change the frequency and/or the way in which they complete ADL/IADL. These changes, frequently described as compensatory and adaptive strategies, reflect the quality of task performance. Increased understanding of mobility, ADL, and IADL performance quality at the preclinical disability phase will enhance preventive interventions to delay or minimize disability.
The objective of the current investigation was to explore baseline motor and cognitive performance-based measures as predictors of mobility, ADL, and IADL performance quality in a sample of community-dwelling older women. In addition, we explored the capability of the predictors to discriminate between individuals with greater or lesser performance quality. Our investigation is unique in two ways. First, we focused on quality of performance rather than independence of performance in mobility, ADLs, and IADLs. Next, we used performance-based measures as our predictors and our outcomes. Prior prediction studies of basic ADL and IADL performance have focused on task independence rather than quality and have used self-report measures to predict disability rather than performance-based measures (Gill et al., 1997; Johnson, Lui, & Yaffe, 2007; Stuck et al., 1999). However, evidence suggests that individuals at the preclinical disability stage will not self-report disability if they are only experiencing change in task quality (Fried et al., 1996). Thus, identification of performance quality predictors using performance-based measures may lead to early identification and referral for intervention to reduce adverse outcomes related to disability in older adults.
Method
Design
This was a secondary analysis of data of 256 community-dwelling older adult women with complete data (18 women with missing data were excluded from the analysis). The primary study collected data from 274 older adult females receiving health care at the UPMC Senior Care—Benedum Geriatric Center (Rogers et al., 2003; Rogers, Holm, Beach, Schulz, & Starz, 2001). Data were collected at two time points in the primary study: baseline and 6 months later. Performance-based impairment measures were administered in the clinic at baseline, and performance-based ADL/IADL outcome measures were administered in the home 6 months later, providing a real-world setting for data collection. All activities of the parent study were approved by the University of Pittsburgh’s Institutional Review Board.
Participants
In the primary study, participants were adjudicated by a physician board certified in geriatrics into the following primary diagnostic categories, with no secondary diagnosis in any other category: well (no primary diagnosis), osteoarthritis of the knee, depression, mild dementia, congestive heart failure, or macular degeneration. Inclusion criteria were (a) community-dwelling female; (b) ≥70 years of age; (c) be medically stable (i.e., not actively or terminally ill); (d) have a Mini-Mental State Examination (MMSE) ≥24 for all groups except dementia, which required an MMSE <24 (Folstein, Folstein, & McHugh, 1975); (e) have a history of successful performance of ADLs based on the Older Americans Resources and Services (OARS) Multidimensional Functional Assessment BADL (basic activity of daily living) and IADL items (Fillenbaum & Smyer, 1980); and (f) have no hearing or visual impairments that would prevent them from participating in the interviews or performance-based measures.
Measures
Outcomes
The Performance Assessment of Self-Care Skills (PASS), home version (Chisholm, Toto, Raina, Holm, & Rogers, 2014; Raina, Rogers, & Holm, 2007; Rogers & Holm, 1989; Rogers et al., 2001), was used to measure quality of task performance for daily living tasks. Table 1 shows the breakdown of the PASS outcomes that were assessed: mobility, BADLs, cognitive instrumental activities of daily living (CIADLs), and physical activities of daily living (PIADLs). Quality of task performance is the frequency of which the individual demonstrates quality or process issues (adequacy) with the task scored using a 4-point ordinal scale that ranged from 0 (no issues) to 3 (many issues). To compute outcomes of mobility, ADL, CIADL, and PIADL, quality scores were averaged across tasks for each individual. Each outcome was then dichotomized into greater (1) and lesser (0) disability using a median split. This approach was selected based on the absence of a prior cut-point. We were interested in which baseline variables were most predictive of lower performance quality at the 6-month assessment; therefore, our reference group was comprised of individuals categorized as lesser performance quality.
Outcomes.
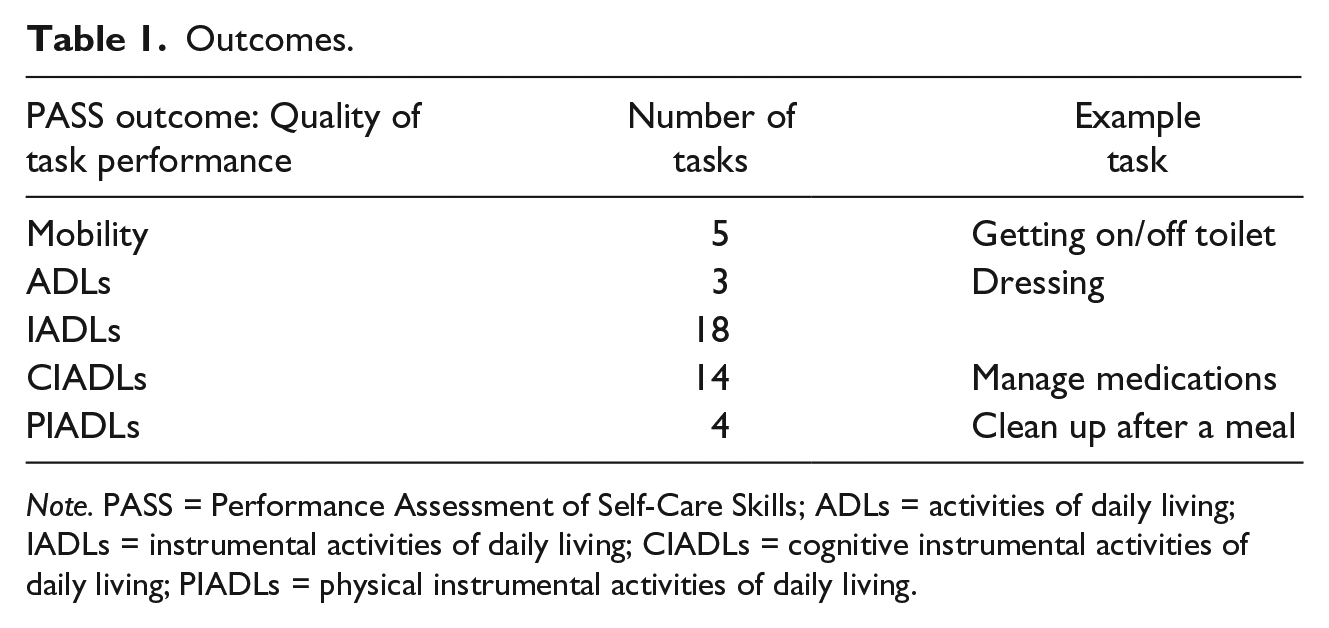
Note. PASS = Performance Assessment of Self-Care Skills; ADLs = activities of daily living; IADLs = instrumental activities of daily living; CIADLs = cognitive instrumental activities of daily living; PIADLs = physical instrumental activities of daily living.
Predictors
Covariates were classified as demographic or diagnostic whereas impairment predictors of interest were performance-based and categorized as motor or cognitive. Demographic variables included age, education level, marital status, and income. Diagnostic variables were primary diagnosis and number of medical conditions (Cumulative Illness Rating Scale for Geriatrics [CIRS-G], Miller et al., 1992; and the Geriatric Depression Scale [GDS], Yesavage et al., 1983). We also controlled for the corresponding baseline PASS score to account for confounding of prior performance quality. Table 2 provides a list of the motor and cognitive impairment predictors. The Trailmaking Parts A and B (Trails) score was computed as the ratio of Trails B/Trails A.
Potential Predictors of Preclinical Disability.
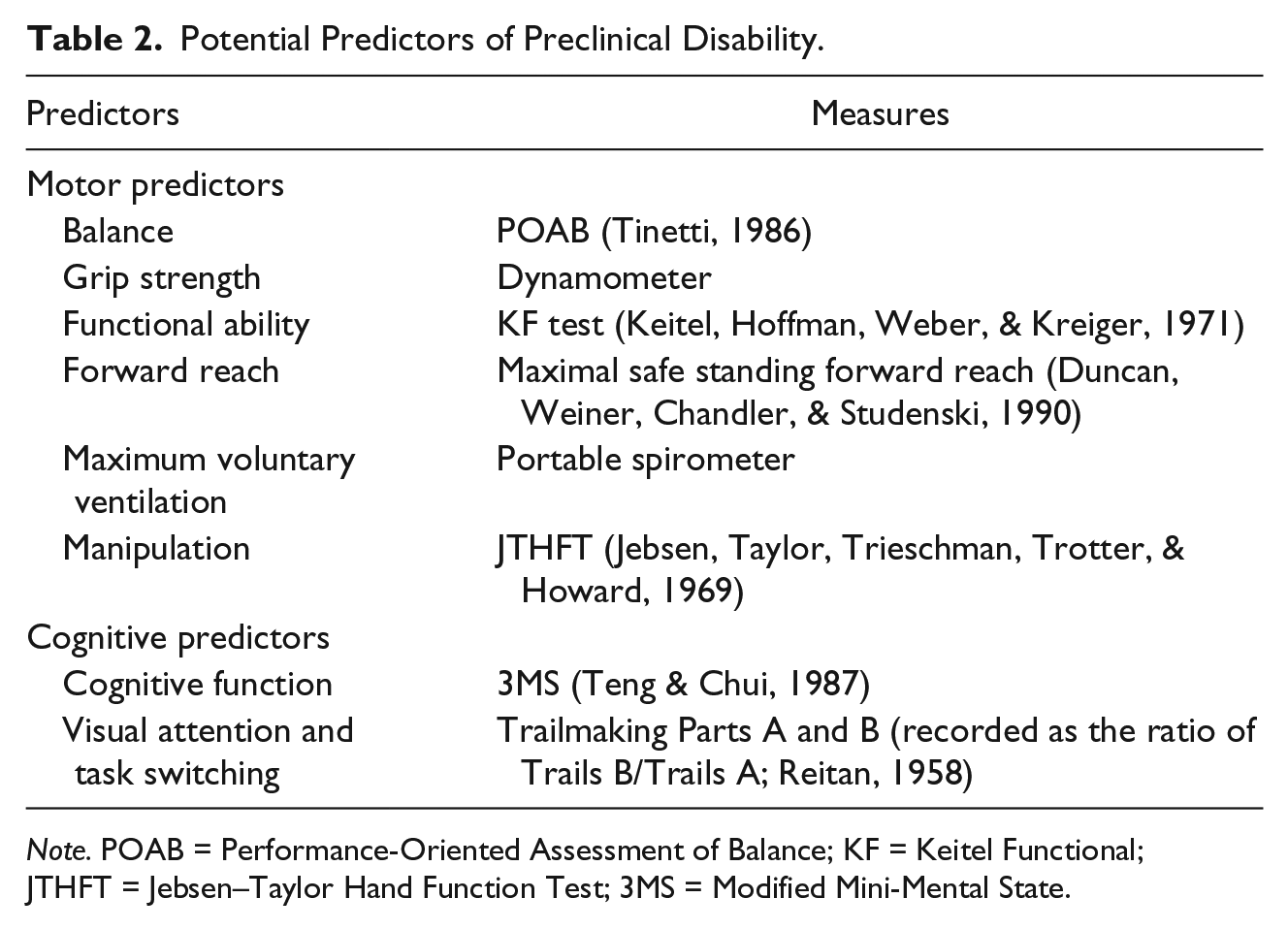
Note. POAB = Performance-Oriented Assessment of Balance; KF = Keitel Functional; JTHFT = Jebsen–Taylor Hand Function Test; 3MS = Modified Mini-Mental State.
Statistical Analysis
All statistical analyses were performed using SPSS (IBM Corp., Released 2012, IBM SPSS Statistics for Windows, Version 22.0) with alpha set to .05. Logistic regression analyses were performed using a stepwise method, with demographic, diagnostic, and baseline outcome variables force entered in Step 1, and potential motor/cognitive variables were explored together with backward elimination in Step 2 (Hosmer, Lemeshow, & Sturdivant, 2013). Separate models were created for 6-month mobility, ADL, CIADL, and PIADL outcomes. Parameter estimates, standard errors, and odds ratios with 95% confidence intervals were examined to determine which variables had the best odds of predicting declines in task performance. We further explored significant predictors by constructing receiver operating characteristic (ROC) curves. For each outcome, a logistic regression model containing only significant performance-based motor and cognitive predictors was created. Accuracies were computed as the area under the curve (AUC), allowing us to examine the discriminative strength of the overall models and individual motor or cognitive predictors (McNeil & Hanley, 1984).
Results
Demographic information for the 256 participants is reported in Table 3. Participants had a mean age of 79, primarily were White (85.5%), many had post–high school education (47.7%), and most were single, widowed, separated, or divorced (80.5%) with an income of US$30,000 or less (82.4%). All participants were female. Participants had one of six primary diagnoses: well (no diagnosis, 21.5%), osteoarthritis of the knee (19.9%), depression (21.9%), dementia (4.3%), congestive heart failure (20.7%), or macular degeneration (11.7%). Table 4 reports the means, medians, and ranges for mobility, ADL, CIADL, and PIADL task adequacy.
Demographics.

Descriptive Information for Outcomes.
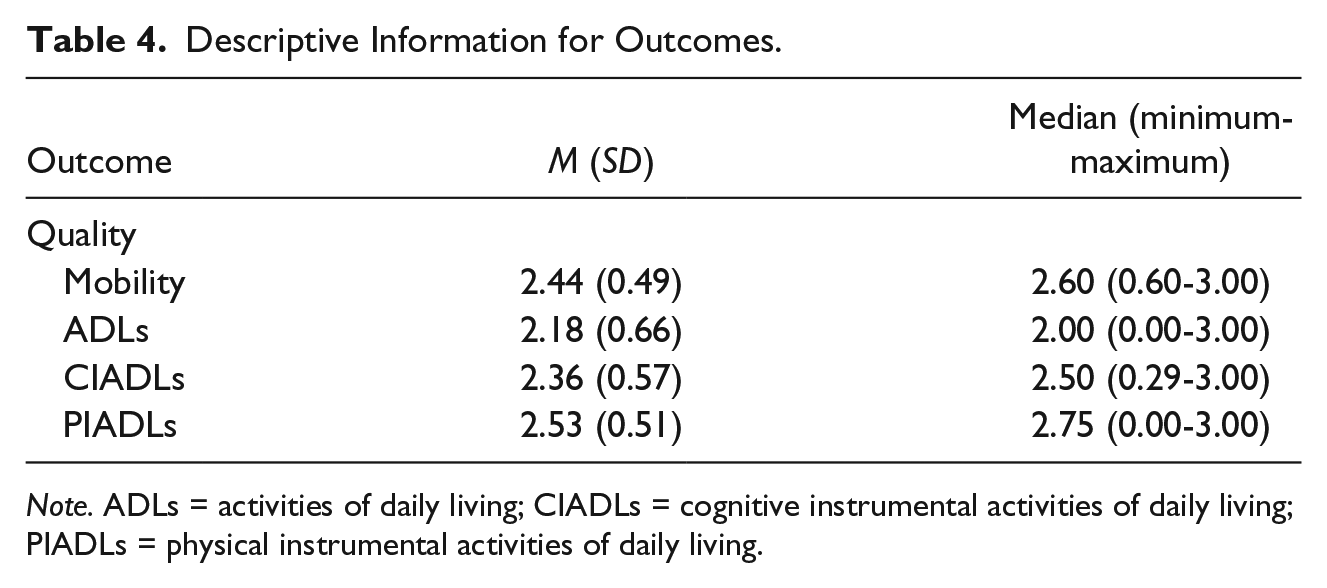
Note. ADLs = activities of daily living; CIADLs = cognitive instrumental activities of daily living; PIADLs = physical instrumental activities of daily living.
Table 5 reports the parameter estimates, standard errors, and odds ratios with 95% confidence intervals for the significant motor and cognitive predictors after controlling for covariates. The odds ratios of the cognitive predictors (1.76-2.32) were generally stronger than the odds ratios of the motor predictors (1.02-1.80). Forward reach (p = .049) and the Modified Mini-Mental State (3MS; p = .012) were predictive of mobility performance quality, whereas the Performance-Oriented Assessment of Balance (POAB; p = .007) and the Keitel Function (p = .005) were predictive of ADL performance quality. Manipulation, as measured by the Jebsen–Taylor Hand Function Test (JTHFT; p = .030) and the 3MS were predictive of CIADL (p = .017), and the Trails (p < .001), 3MS (p = .050), and JTHFT (p = .050) were predictive of PIADL performance quality.
Logistic Regression and ROC Curve Results.
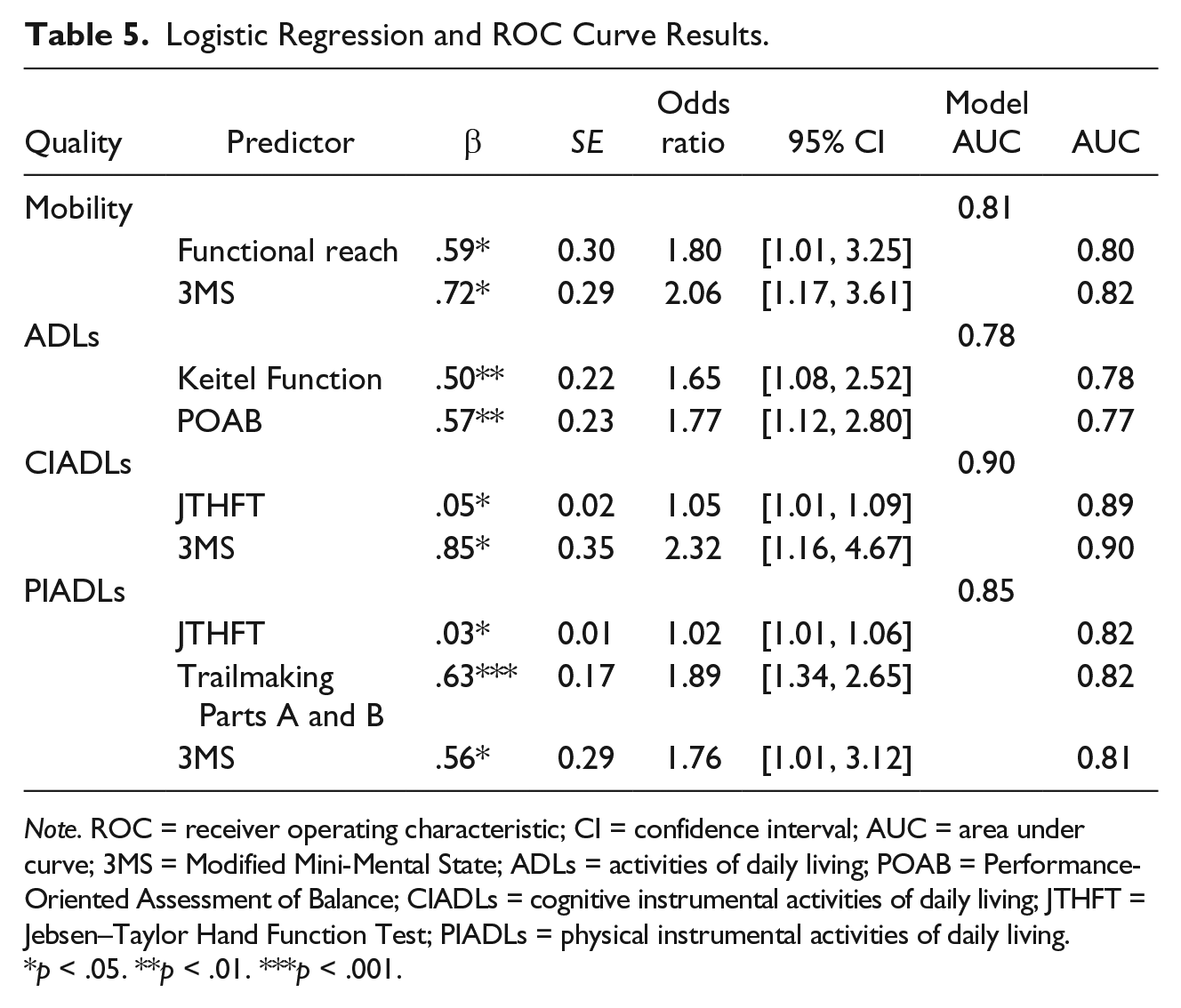
Note. ROC = receiver operating characteristic; CI = confidence interval; AUC = area under curve; 3MS = Modified Mini-Mental State; ADLs = activities of daily living; POAB = Performance-Oriented Assessment of Balance; CIADLs = cognitive instrumental activities of daily living; JTHFT = Jebsen–Taylor Hand Function Test; PIADLs = physical instrumental activities of daily living.
p < .05. **p < .01. ***p < .001.
Next, we determined the ability of significant predictors (in combination and as single measures) to classify individuals as having greater or lesser performance quality using ROC curves after controlling for covariates. The model including the cognitive predictor 3MS and manipulation (JTHFT) as predictors of CIADL performance quality provided the most accurate classification (c = .90). Table 4 displays the combinations and single AUC values for all significant predictors. All AUCs were ≥.77, indicating that cognitive and motor impairment measures accurately classified individuals into greater or lesser performance quality categories whether in the model together or as individual predictors.
Discussion
The current investigation sought to determine early-warning indicators of performance-based preclinical disability in a sample of 256 older adult females. Motor and cognitive impairment measures were found to predict mobility, ADL, and IADL quality performance after controlling for baseline covariates. The 3MS was predictive of mobility, CIADL, and PIADL performance, suggesting that this cognitive impairment measure may be useful to predict declines in quality of performance. Our results provided evidence that individual performance-based motor and cognitive impairment measures were accurate discriminators between greater and lesser performance quality.
Our results are similar to prior studies of predictors of task performance. Grimmer, Beaton, and Hendry (2013) found that declines in IADLs were associated with self-report measures of mental and physical quality of life scores. This is similar to our finding that motor and cognitive measures are both associated with declines in IADLs; however, our study focused on performance-based measures rather than self-report measures. We found that balance was an indicator of lower ADL performance, which aligns with the findings of a systematic review of physical indicators of ADL disability (Vermeulen, Neyens, van Rossum, Spreeuwenberg, & de Witte, 2011). However, the systematic review focused on frail older adults whereas our older study was not completed with older adults who were not considered frail.
The main characteristic of the preclinical disability phase is that individuals use compensation to cope with impairments prior to the onset of disability (Fried et al., 1991). There is a dearth of studies that explore the role of compensatory behaviors in activity and participation limitations (Higgins, Janelle, & Manini, 2014). The concept of a progression from a preclinical phase to disability has been well documented in the literature (Fried et al., 2001; Wolinsky et al., 2007); however, more studies have focused on the second phase of disability, where a loss of functional independence has occurred (Gill et al., 1997; Johnson et al., 2007; Stuck et al., 1999). By examining the relationships between motor and cognitive impairment and performance quality of mobility, ADLs, and IADLs using the PASS, we were able to explore potential indicators of early decline.
The AUC values obtained for our overall and individual predictors were good to excellent (McNeil & Hanley, 1984), suggesting that motor and cognitive impairment predictors accurately classified individuals into the greater or lesser performance quality categories. AUCs for the overall models were slightly stronger than individual predictors, indicating that observing a combination of motor and cognitive performances could be important for early detection of lesser performance quality in older adults. However, prior studies have suggested that physical and cognitive measures are independent predictors of disability (Gill, Williams, Richardson, & Tinetti, 1996; Grimmer et al., 2013). In addition, we recognize the value of using one measure as a quick screen to refer individuals to services that may delay the onset of disability.
When comparing the odds ratios and AUC values, the 3MS was a strong predictor of three of our four outcomes. This provides evidence that the 3MS could stand alone as a screen for preclinical disability. Interestingly, ADL adequacy was predicted by two motor impairment measures, forward reach and the POAB. Although the AUC was good (c = .78), it was lower than the three models that contained the 3MS cognitive measure (c = .81-.90). This suggests other factors may explain differences in ADL performance such as personal or environmental factors. Prior literature suggests that low physical activity and hospitalizations contribute to declines in ADLs (Boyd et al., 2009; Vermeulen et al., 2011). Although our findings suggest that the 3MS could act as a quick screen for preclinical disability, the limitations of our study require future investigations to confirm.
Limitations
There were a number of limitations in the current investigation. Our sample was comprised of females who were primarily White. A more diverse sample of older adults would allow for greater generalizability of results. In addition, there were several limitations due to the secondary nature of the analyses. The small numbers within the diagnostic conditions did not allow for subgroup analyses to focus on particular medical diagnoses. The use of the median splits to dichotomize the outcomes may have led to a loss of information; however, the data were not collected in the parent study to facilitate cut-point calculations. This limitation is also present in our AUC analyses, as we lacked sufficient information in the data set to calculate cut-points for prediction of quality.
Suggestions for Future Research
Our suggestions for future research are primarily based on the limitations of our current investigation. We used a homogeneous sample; therefore, future studies using a diverse sample are needed. Future studies should be designed to identify the best performance-based indictors of preclinical disability, with the intent to establish cut-points for diagnostic purposes.
Conclusion
Our findings imply that performance-based impairment measures have diagnostic value in clinical practice for the purpose of early identification, screening, and referral of community-dwelling older adults. Further investigation of performance-based impairment measures as diagnostic screens for preclinical disability is warranted.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.