
Abstract
Social connections benefit cognitive, emotional, and physical health (e.g., Berkman & Syme, 1979; Boden-Albala, Litwak, Elkind, Rundek, & Saco, 2005; Cohen, Doyle, Skoner, Rabin, & Gwaltney, 1997; Cruwys et al., 2013; Holt-Lunstad, Smith, Baker, Harris, & Stephenson, 2015; House, Landis, & Umberson, 1988). Aging can contribute to social isolation and increase vulnerability to its negative effects (e.g., Hawkley, Masi, Berry, & Cacioppo, 2006; Ong, Rothstein, & Uchino, 2012). Because of this, finding ways to support the social relationships of older adults should be a priority for those concerned with their well-being (Hawkley & Cacioppo, 2007). Internet connectivity offers a creative way to increase older adults’ social connectivity, and through this to support their well-being (e.g., Mason, Sinclair, & Berry, 2012). Yet, evidence for the effectiveness of this strategy is inconclusive, perhaps due to an insufficient focus on the social uses of technology, and on the challenges involved in supporting older adults to access these. The current study targets these challenges.
Internet Use, Health, and Well-Being Among Older Adults
Longitudinal data link older adult’s Internet use to reduced depression, improved cognitive capacity, and better health behavior (Cotten, Ford, Ford, & Hale, 2014; Xavier et al., 2013, 2014). But, other research finds limited benefits of online compared with face-to-face interaction (Helliwell & Huang, 2013), and that increased online social activity can predict subsequently reduced well-being (Kross et al., 2013), raising the concern that online social interaction might come at the expense of more important offline interactions. However, the depression-reducing benefits of older adults’ Internet use amplify among those in smaller versus larger households (Cotten et al., 2014), suggesting that Internet use can compensate, rather than detract from, offline networks.
A similarly mixed pattern is evident in the experimental literature. Inducing online social activity might reduce younger adults’ loneliness (Deters & Mehl, 2013). However, interventions that introduce older adults to computers and online networking suggest few reliable consequences. Although early studies of this kind were promising (McConatha, McConatha, Deaner, & Dermigny, 1995), larger scale, better controlled, studies have found no discernible benefits for cognitive and mental well-being or social engagement (e.g., Slegers, van Boxtel, & Jolles, 2008; White et al., 2002; Woodward et al., 2011).
When interpreting this evidence, it should also be noted that the majority of interventions targeting older adults were conducted prior to (McConatha et al., 1995; White et al., 2002), or only on the cusp of (Slegers et al., 2008), the expansion of online social networking capabilities (i.e., “Web 2.0”). Their methods also suggest that training was directed toward proficiency in computer use, rather than using computers as social tools (Woodward et al., 2011, is an exception). Computers have also become increasingly customizable to different needs and capacities, including those of older adults. In light of these issues, further investigation of the benefits of socially focused, “age-friendly,” Internet and computer training seems warranted. This was the primary aim of the current study.
Interventions Targeting Social Participation Among Older Adults
The current study was informed by a growing body of research, inspired by prominent social-psychological theories of group membership, which attests to the value of socially targeted interventions among older populations (Jetten, Haslam, Haslam, Dingle, & Jones, 2014). Recent studies show that the well-being benefits of a range of ordinary activities (e.g., Gleibs, Haslam, Haslam, & Jones, 2011; Haslam et al., 2014; Knight, Haslam, & Haslam, 2010) are enhanced when activities are group-based rather than individualized (see Jetten, Haslam, & Haslam, 2012), thereby allowing the development of meaningful social connections. This work particularly points to the role of group participation in supporting individual identity (i.e., knowing “who I am”) as a key mechanism through which positive health effects flow (e.g., Jetten, Haslam, Pugliese, Tonks, & Haslam, 2010; Jones et al., 2011).
Similarly, we expected effects of Internet provision and training to be maximized when these focused on social engagement, rather than the mere acquisition of computer skills—although, consistent with other theories of the self and psychological functioning, we expected that increased competencies, as well as connectedness, would contribute positively to well-being (in line with self-determination theory; for example, Reis, Sheldon, Gable, Roscoe, & Ryan, 2000). In addition to these mechanisms, we anticipated that the sense of identity that social participation supports might also be important for explaining well-being benefits. Testing these possible mediating pathways was the second aim of this research.
The Current Research
We tested the potential for age-friendly computer and Internet provision, and training on its use for social purposes, to enhance the well-being of older adults. In spite of the weak evidence from previous studies, we expected to find benefits of training not just on indicators of individual skills acquisition and competency but also on social engagement, identity, and, through these, individual well-being outcomes.
We were also interested in the degree to which benefits might differ depending on the individual’s immediate social context (i.e., following Cotten et al., 2014). All participants were recruited through a care organization, but approximately half were in residential care, whereas the other half were supported in the community. We expected the benefits of the intervention to be most evident among those who were previously most isolated, and we reasoned that those receiving care in their own home might display greater risk of this. Although those living in residential care should be worse off in terms of individual health (reflecting their enhanced care needs), they also have easier access to a community of others and structured social activity to facilitate connections with these.
Method
Participants
One hundred twenty-one clients of a large not-for-profit care organization (78 female, aged 60 to 95 years) agreed to take part in the study. Participants were receiving care in their own home/supported housing in the community (henceforth “domiciliary care”), or residential care in one of the organization’s 26 care homes.
Care staff identified potential participants who were (a) willing to be engaged for a period of 4 months, (b) had the space and infrastructure for Internet use (i.e., a phone connection and a table that could accommodate the computer package), and (c) had sufficient cognitive ability to engage with the training. The latter was initially based on a six-item screener (Callahan, Unverzagt, Hui, Perkins, & Hendrie, 2002), subsequently confirmed by the Mini-Mental State Examination (Folstein, Folstein, & McHugh, 1975), on which potential participants were required to score ≥ 19 out of 30. 1 We limited participation to individuals who did not currently have Internet access. The only advertised rewards for participation were receiving temporary use of a computer and training package (experimental group), or going into a lottery to win one of two computer packages (control group).
Following initial recruitment, 22 participants withdrew before baseline assessment. A further 23 withdrew before follow-up assessment. Participant flow is summarized in Figure 1. Seventy-six participants completed baseline and follow-up assessments. The majority (50) were women (M age = 80.71; SD = 8.77) and were widowed (60%), single (15%), or divorced (9%), with only 15% being currently married. The mean age at leaving full-time education was 15.34 years. Participants were distributed across residential (n = 32) and domiciliary care (n = 44; mean approximate length of care = 5.68 years; SD = 8.71). The majority (75%) of the latter lived alone.
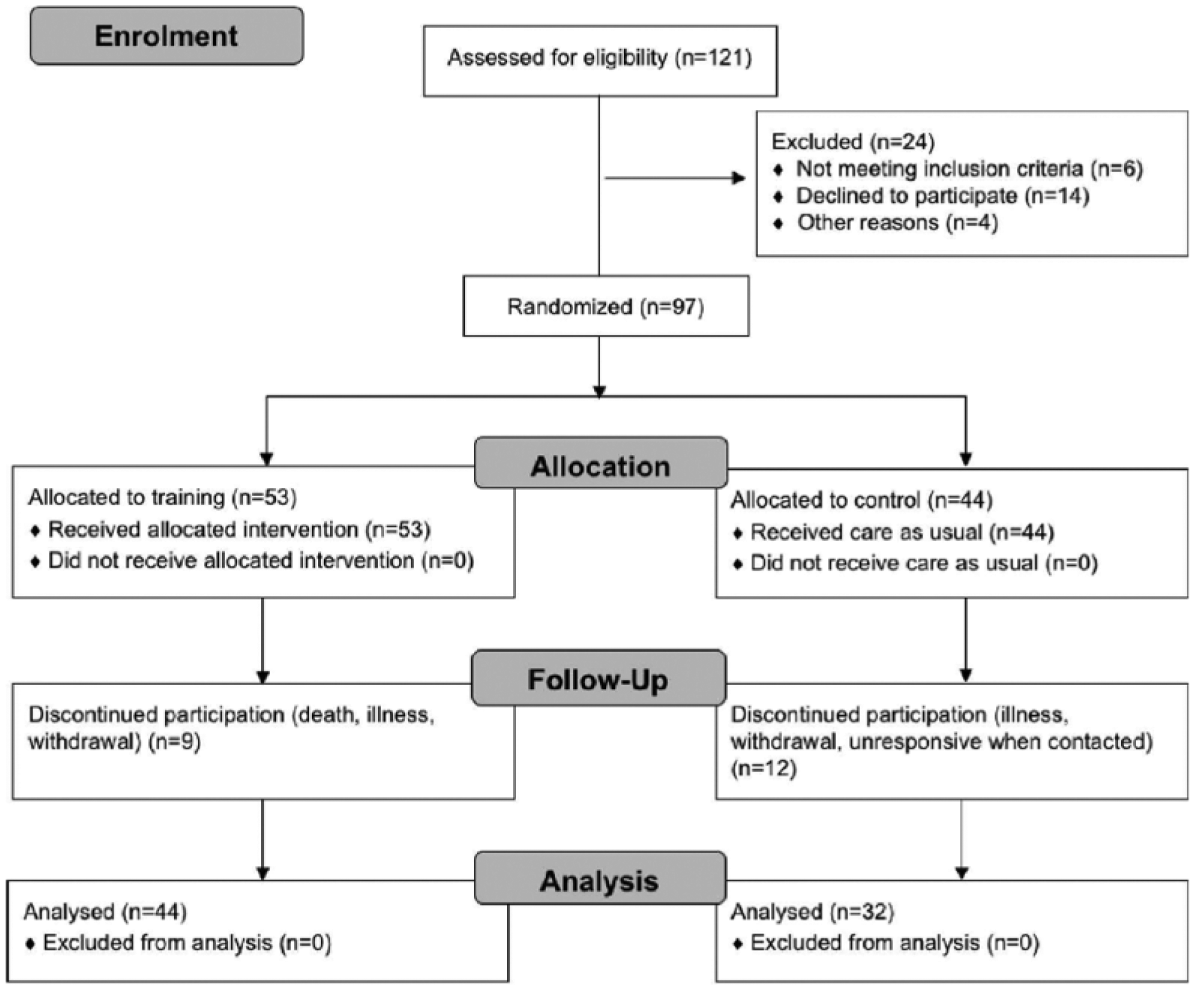
CONSORT diagram summarizing recruitment, allocation, and drop-out numbers and reasons.
Design
The study followed a 2 (condition: training, control) × 2 (population: domiciliary, residential) × 2 (time: baseline, follow-up) design. After baseline assessment, participants were randomly assigned to either a training or care-as-usual control group. Stratified randomization was used within domiciliary and residential participants to ensure balanced allocation to condition. Trained research assistants verbally administered assessments. Ethical approval was given by the University of Exeter.
The Training Package
The training group received a customized computer platform with a simplified touch-screen interface (“EasyPC”) and any necessary broadband infrastructure (i.e., modem, cables, etc.). Participants kept this for 12 months, which included the training period, after which they could choose to buy the package at a reduced rate and to take on broadband costs.
Three “Care Technologists” administered the training. These were qualified carers employed by the organization who were trained to deliver computer training for the current project. The training schedule was manualized, and participants were also provided with a user manual to support their training, including homework tasks to consolidate learning in between sessions. Training was stepped-down across 3 months and involved the following:
Within the defined schedule, Care Technologists were flexible with training and responsive to the needs and interests of their client. If participants were not interested in a specific application (e.g., Facebook) they were not required to persist with it, provided they had received the basic training in how to use that application should they wish. In this way, we aimed to instill competencies with computer use, and specifically in social networking applications, rather than to force participants to use things that did not meet their needs or interests.
Procedure
A member of the research team scheduled baseline assessments with potential participants. The researcher ensured that these were fully informed and understood the random nature of group assignment. If consent was given, demographic details were taken and all measures were administered. Assessments typically took between 1 and 2 hours.
Randomization followed the T1 interview. This was achieved via an online randomization program that occurred monthly to include all participants who had completed a baseline interview in that time. Participants allocated to the control condition received care-as-usual (also involving regular carer visits). They were sent a letter and small gift (e.g., a pen) expressing gratitude for their involvement and inviting them to participate in a follow-up interview and were informed that on completing the second interview they would be entered into the lottery for one of two computer packages. Those who were allocated to the training group had infrastructure installed and were assigned a Care Technologist.
Follow-up assessment was scheduled after training was complete or after an equivalent period for control participants. This was targeted to occur within a 4-week period post-training (i.e., 4 months since baseline). Due to health or delays in training, this time frame varied for some participants. Once all measures had been administered, participation was complete and participants were thanked.
Measures
1. Cognitive and mental health.
The Addenbrooke’s Cognitive Examination–Revised (ACE-R; Mioshi, Dawson, Mitchell, Arnold, & Hodges, 2006) was used to assess general cognitive ability across multiple domains, including attention/orientation, memory, verbal fluency, language, and visuo-spatial abilities. In accordance with standard scoring procedures for this instrument, participants received a total score out of 100, with higher scores indicative of better cognitive functioning across domains.
Mental health was assessed using several indicators. The 12-item General Health Questionnaire (GHQ-12; Goldberg & Williams, 1988) assessed the frequency of negative mental health symptoms “in the past few weeks” (αs = .87 and .85); the eight-item Center for Epidemiologic Studies–Depression Scale (CES-D; Radloff, 1977) assessed the frequency of depressive symptoms in the last week (αs = .82 and .81); and the Geriatric Anxiety Inventory–Short Form (GAI-SF; Byrne & Pachana, 2011), assessed the experience of five anxiety symptoms, also in the last week. GHQ and CES-D items were assessed on a 4-point Likert-type scale (1 = rare or no symptoms, 4 = frequent symptoms; exact wording depended on scale and item), and responses were averaged to give indices on which higher scores indicated more frequent negative mental health symptoms within the specified time frame. GAI items were responded to in a binary agree/disagree format, and number of agreements were summed to give an indication of the degree of anxiety experienced by the person in the last week. General well-being was indexed via the five-item Satisfaction With Life Scale (SWL; for example, “In most ways my life is close to ideal”; Diener, Emmons, Larsen, & Griffin, 1985). Responses to these items were given on a 5-point scale (1 = not at all true, 5 = very true), and individual items were averaged to form an index on which higher scores indicated greater SWL (αs = .85 and .81).
2. Sense of self and social relationships.
We assessed the autonomy and competence subscales from self-determination theory’s basic needs satisfaction questionnaire (Gagné, 2003; the third need, relatedness, is covered elsewhere). This included 13 statements (e.g., “I generally feel free to express my ideas and opinions,” “Often I do not feel very competent”) and participants indicated the degree to which each was true for them (1 = not at all true, 5 = very true). Responses were averaged, with higher scores indicating stronger feelings of autonomy (αs = .71 and .74) and competence (αs = .42 and .73). 2
Personal identity strength was assessed by six items (from Baray, Postmes, & Jetten, 2009; Campbell et al., 1996; for example, “I know what I want from life,” “I have a clear picture of who I am and what I am”; αs = .68 and .77). Responses were given on a 5-point scale (1 = not at all true, 5 = very true) and were averaged so higher scores indicated a stronger sense of one’s self.
A social network activity index (Cohen et al., 1997) asked participants to report (yes, no) whether they had been in contact with each of 10 different targets (e.g., spouse, children, grandchildren, other family, friends, close neighbors, people in my local community) at least once every 2 weeks. Responses were summed. Separately, participants indicated their satisfaction with the amount of contact they had with each of these targets (1 = very dissatisfied, 5 = very satisfied). Responses were averaged to provide a general index of social network satisfaction. Subjective loneliness was also assessed with eight items (αs = .86 and .84) from the University of California, Los Angeles (UCLA) Loneliness Scale (Russell, 1996) on which participants indicated the extent to which various statements applied to them (e.g., “How often do you feel that you lack companionship?”; 1 = never, 4 = always).
3. Computer attitudes.
These were assessed using 13 items from Jay and Willis’ (1992) questionnaire (e.g., “I feel comfortable with computers”). Responses were made using a 5-point scale (1 = strongly disagree, 5 = strongly agree) and averaged such that higher scores indicated more positive attitudes (αs = .81 and .90).
Results
Initial Checks
Analyzing all the data collected at Time 1 (n = 97), conditions did not differ in age, t < 1, p = .70, gender, χ2 = .20, p = .67, or any measure at baseline, ts < 1.60, ps > .11. There were no baseline differences between those who had dropped out by Time 2 and those who did not, neither overall, ts < 1.39, ps > .17, nor within each condition, all ts < 1.75, ps > .08, and no indication of different drop-out rates across conditions, χ2 = 1.50, p = .22. This suggests that randomization was successful and attrition not systematic. That said, in the analyses conducted on the sample of completers (n = 76), reported below, small baseline differences are apparent on certain indices (computer attitudes, CES-D, and GHQ). This suggests some possible effects of attrition, an issue we return to in the “Discussion” section. To address the robustness of the findings from these analyses, we also report intention-to-treat analyses based on the full sample of participants assigned to conditions, irrespective of whether they completed the study.
There were also (predictable) differences between residential and domiciliary populations. Participants in residential (vs. domiciliary) care were significantly older, t = 3.00, p = .004, performed worse on the ACE-R, t = −4.22, p < .001, felt less autonomous, t = −2.28, p = .02, and slightly less competent, t = −1.96, p = .053. Residential participants also reported a less active social network, t = −5.51, p < .001. No other baseline differences between groups emerged, |t|s < 1.33, ps > .019. There was, therefore, no evidence for our assumption that domiciliary (vs. residential) care participants would be at greater risk for social isolation—if anything, the pattern was the reverse.
Effects on Computer Attitudes, Sense of Self, and Social Relationships
Descriptive statistics are presented in Table 1. The impact of the intervention was assessed via a series of 2 (condition: training, control) × 2 (population: residential, domiciliary) × 2 (time: 1, 2) mixed ANOVAs. Statistics are reported in Table 2.
Estimated Means (and Standard Errors) for All Variables According to Time, Condition, and Population Group.
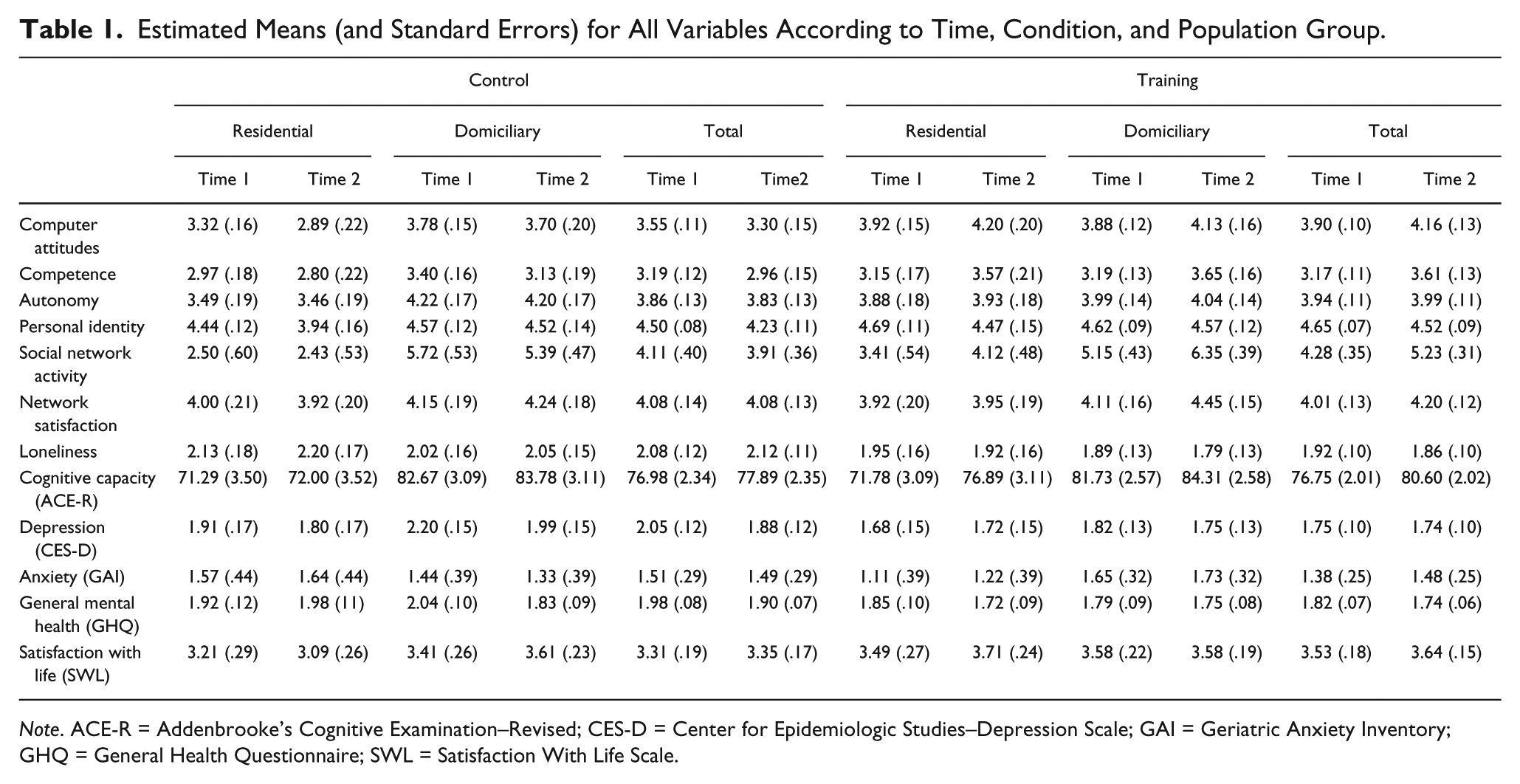
Note. ACE-R = Addenbrooke’s Cognitive Examination–Revised; CES-D = Center for Epidemiologic Studies–Depression Scale; GAI = Geriatric Anxiety Inventory; GHQ = General Health Questionnaire; SWL = Satisfaction With Life Scale.
ANOVA Statistics From Main Analyses for All Outcome Variables.
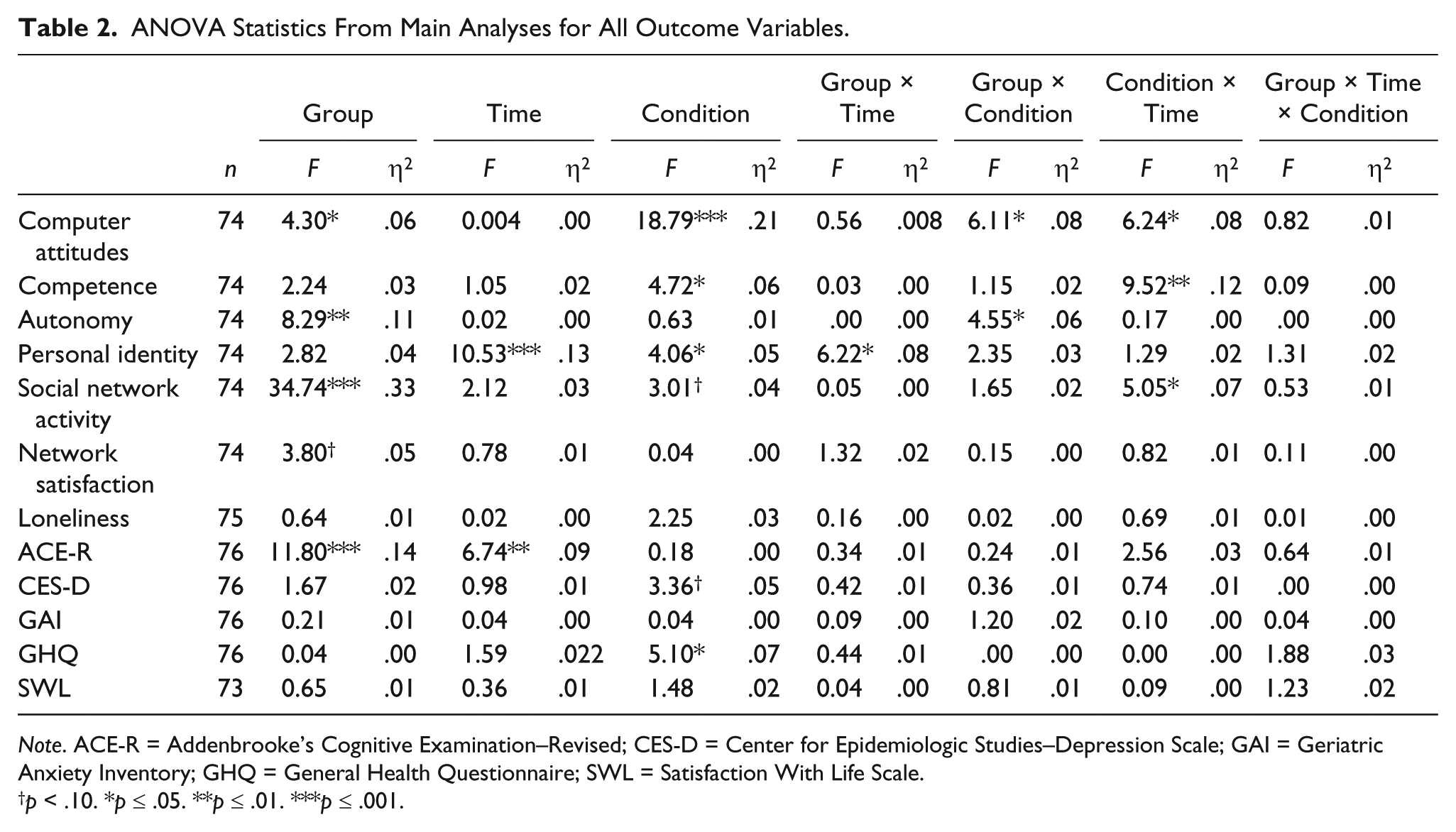
Note. ACE-R = Addenbrooke’s Cognitive Examination–Revised; CES-D = Center for Epidemiologic Studies–Depression Scale; GAI = Geriatric Anxiety Inventory; GHQ = General Health Questionnaire; SWL = Satisfaction With Life Scale.
p < .10. *p ≤ .05. **p ≤ .01. ***p ≤ .001.
Computer attitudes
This analysis revealed a significant effect of condition qualified by a significant Condition × Time interaction. Follow-up tests confirmed that although there was a small difference between training and control groups at Time 1, F(1, 70) = 5.68, p = .02, ηp2 = .08, this difference was considerably larger at Time 2, F(1, 70) = 19.11, p < .001, ηp2 = .21. Moreover, trainees reported improved attitudes about computers across time, F(1, 70) = 3.83, p = .054, ηp2 = .05, whereas attitudes in the control group did not change, F(1, 70) = 2.59, p = .11, ηp2 = .04.
Beyond this, there was a significant effect of population, and a significant Condition × Population interaction. Follow-up tests revealed a difference between training and control participants in the residential care group, F(1, 70) = 20.23, p < .001, ηp2 = .22, but not in the domiciliary care group, F(1, 70) = 2.03, p = .16, ηp2 = .03. Residential trainees had more positive attitudes than residential controls. Although the three-way interaction was not significant, further probing revealed that the Condition × Time interaction was more apparent in residential, F(1, 29) = 3.83, p = .06, ηp2 = .12, than domiciliary participants, F(1, 41) = 1.92, p = .17, ηp2 = .05. Thus, the intervention improved computer attitudes, but especially among those living in a care home rather than their own home.
Sense of self
On feelings of competence, there was a significant effect of condition, qualified by a significant Condition × Time interaction. Although there were no differences between groups at Time 1, F < 1, by Time 2 trainees were experiencing heightened feelings of competence relative to the control group, F(1, 70) = 10.86, p = .002, ηp2 = .13. Moreover, trainees reported improved feelings of competence across time, F(1, 70) = 9.52, p = .003, ηp2 = .12, whereas self-competence in the control group did not change, F(1, 70) = 1.91, p = .17, ηp2 = .03.
This pattern did not extend to feelings of autonomy. For this variable, there was a significant difference between residential and domiciliary groups, qualified by a significant Condition × Population interaction, indicating that the baseline population difference was more apparent in the control group than the training group. However, as this interaction was not modified by time of measurement, the pattern is difficult to attribute to the training itself.
The analysis of personal identity strength revealed significant main effects of time and condition: Personal identity strength declined across time and was higher in the training versus control group. A significant Time × Population interaction further indicated that the decline in personal identity strength was more evident among those in residential care, F(1, 71) = 14.17, p < .001, ηp2 = .17, than domiciliary care, F < 1. Although no other effects were significant, given the emerging pattern we probed the condition and time effects further. This revealed that the apparent decline in personal identity strength was limited to the control group, F(1, 71) = 8.47, p = .005, ηp2 = .11, and was not apparent in the training group, F(1, 71) = 2.56, p = .11, ηp2 = .04. This accelerated decline resulted in a significant difference between training and control groups at Time 2, F(1, 71) = 4.23, p = .04, ηp2 = .06, that was not apparent at Time 1, F(1, 71) = 1.92, p = .17, ηp2 = .03. This pattern was especially evident among participants receiving residential rather than domiciliary care. Among the former, decline was more pronounced in the control, F(1, 71) = 12.61, p = .001, ηp2 = .15, than training group, F(1, 71) = 2.85, p = .10, ηp2 = .04. Among the latter, there was no evidence of decline in either group, Fs < 1.
Social relationships
The analysis of social network activity revealed a marginal effect of condition qualified by a significant Condition × Time interaction. Although there were no differences between training and control groups at Time 1, F < 1, at Time 2 there was a significant difference, F(1,71) = 7.88, p = .006, ηp2 = .10. Trainees reported increased social network activity across time, F(1, 71) = 7.91, p = .006, ηp2 = .10, whereas the control group did not change, F < 1. The effect of training on indicators of social connectedness was confined to the measure of network activity rather than satisfaction or subjective feelings of loneliness.
Summary
The above analyses provide evidence that the intervention did what it was designed to do: Across time, participants who received the training developed more positive attitudes about computers, felt more competent as a person, and were engaged more actively with their social network relative to those who did not receive the training. There was also some evidence that training contributed to the maintenance of personal identity over time. Contrary to initial expectations, to the extent that there were different effects across population groups, these favored the residential care, who in fact were more socially restricted at the outset.
Effects on Cognitive and Mental Health
Cognitive health
The analyses of ACE-R scores revealed a significant effect of time, indicating that cognitive performance improved from baseline to follow-up. Although the interaction with condition did not reach significance (p = .11), given the general expectation of cognitive decline in this population, and the unusual nature of improvement, we explored the apparent time effect further. Follow-up tests revealed that the effect of time was confined to the training group, F(1, 72) = 10.34, p = .002, ηp2 = .13, and was not at all apparent in the control group, F(1, 72) = .43, p = .51, ηp2 = .006.
Mental health
The only effects to emerge on mental health outcomes were a marginal effect of training on CES-D, and a significant effect of training on GHQ scores. Trainees experienced slightly better mental health than control participants. However, these effects were independent of time of measurement and therefore hard to attribute to the training. There were no other main or interactive effects of the variables on any of these measures.
Intention-to-Treat Analysis
To check the robustness of the effects reported above, and to partly address any problems of attrition, we conducted an intention-to-treat analysis including all allocated participants. Given the short period of assessment, and the general pattern of limited change in the control group in the main analyses, we assumed no change among those who withdrew or were lost to follow-up. The last measurement (i.e., Time 1) was carried forward to represent Time 2 for these participants. The observed patterns on computer attitudes, competence, social network activity, personal identity strength, and cognitive capacity held in these analyses (see Table 3), as did the absence of any effects on mental health outcomes.
ANOVA Statistics From Intention-to-Treat Analyses on Key Outcomes (No Change Assumed for Participants Lost to Time 2).
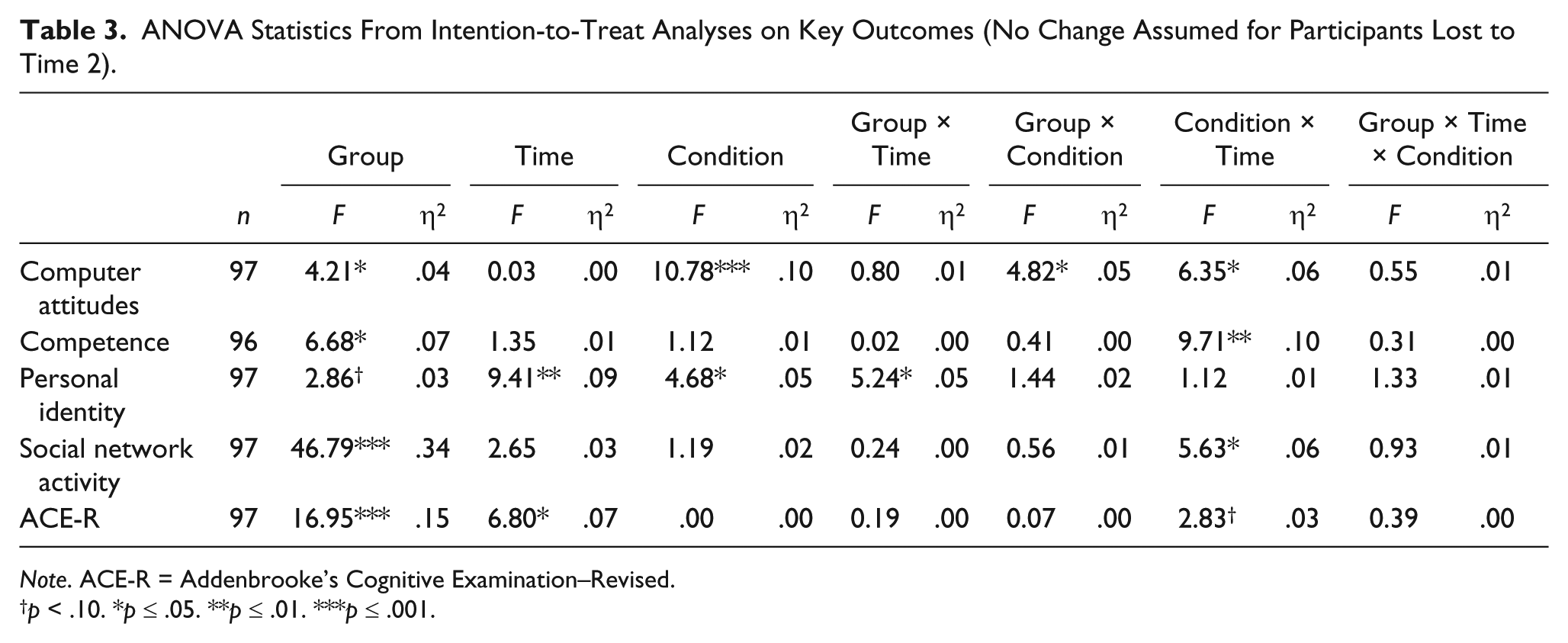
Note. ACE-R = Addenbrooke’s Cognitive Examination–Revised.
p < .10. *p ≤ .05. **p ≤ .01. ***p ≤ .001.
Indirect Effects on Cognitive and Mental Health
We also explored the possibility of indirect effects on cognitive and mental health outcomes via the observed impacts on the suggested mediators. Specifically, we specified a series of models (PROCESS, Model 6; Hayes, 2013) in which maintained personal identity strength was positioned as a proximal mediator of any indirect effects of training (coded: training = 1, control = 2) on improved cognitive and mental health outcomes (i.e., controlling for baseline); and improved competence and expanded social networks were (separately) specified as mediators of any effects of training on personal identity strength and outcomes (again controlling for baseline). This general model is depicted graphically in Figure 2. Model statistics are reported in Tables 4 and 5.

Schematic model of indirect effects analysis.
Regression Statistics for Indirect Effects Between Training and Cognitive and Mental Health Outcomes via Increased Competence and Social Network Activity, and Maintained Personal Identity.
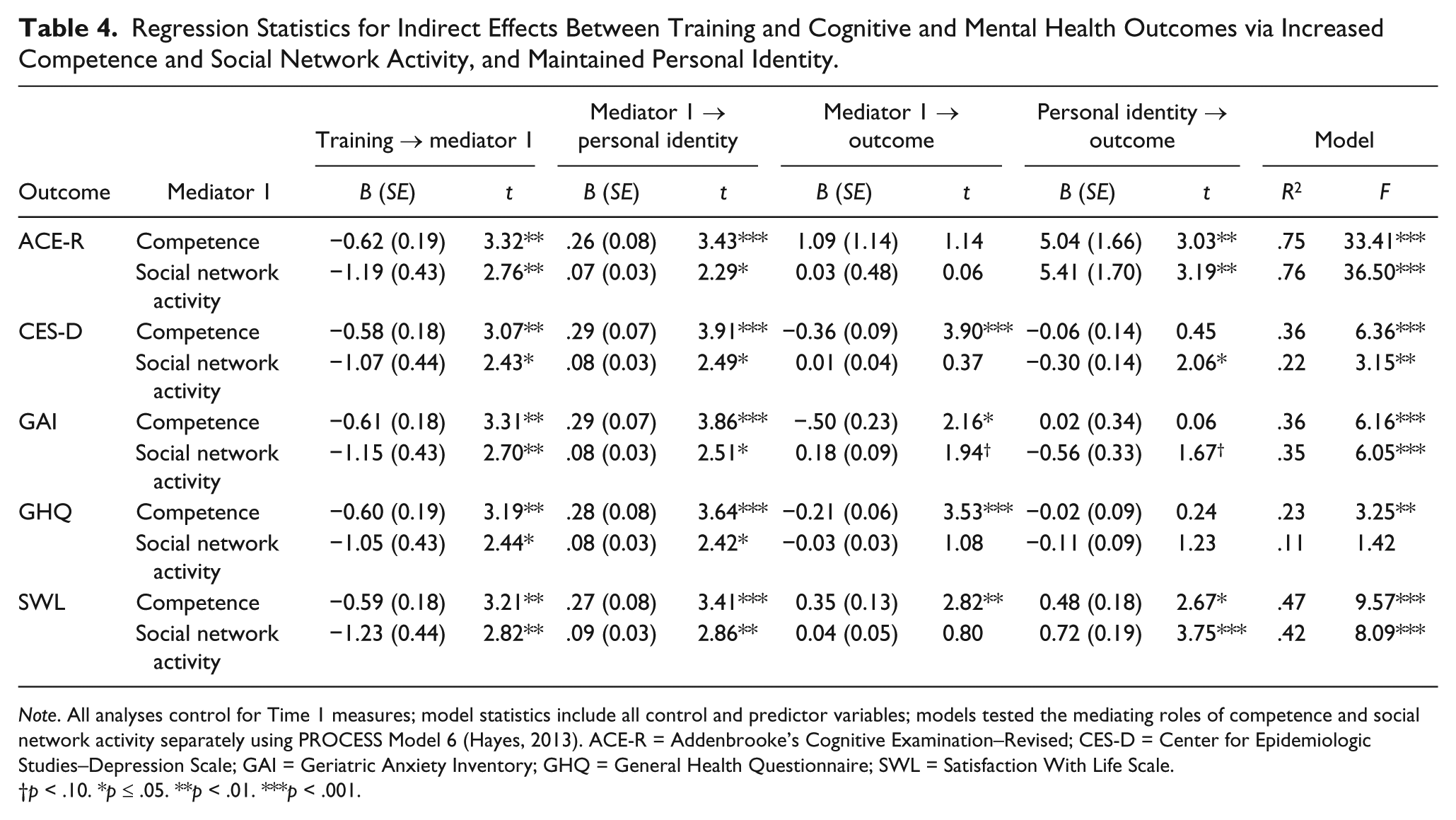
Note. All analyses control for Time 1 measures; model statistics include all control and predictor variables; models tested the mediating roles of competence and social network activity separately using PROCESS Model 6 (Hayes, 2013). ACE-R = Addenbrooke’s Cognitive Examination–Revised; CES-D = Center for Epidemiologic Studies–Depression Scale; GAI = Geriatric Anxiety Inventory; GHQ = General Health Questionnaire; SWL = Satisfaction With Life Scale.
p < .10. *p ≤ .05. **p < .01. ***p < .001.
Tests of Indirect Effects Between Training and Cognitive and Mental Health Outcomes via Increased Competence (C) and SNA, and maintained PI.
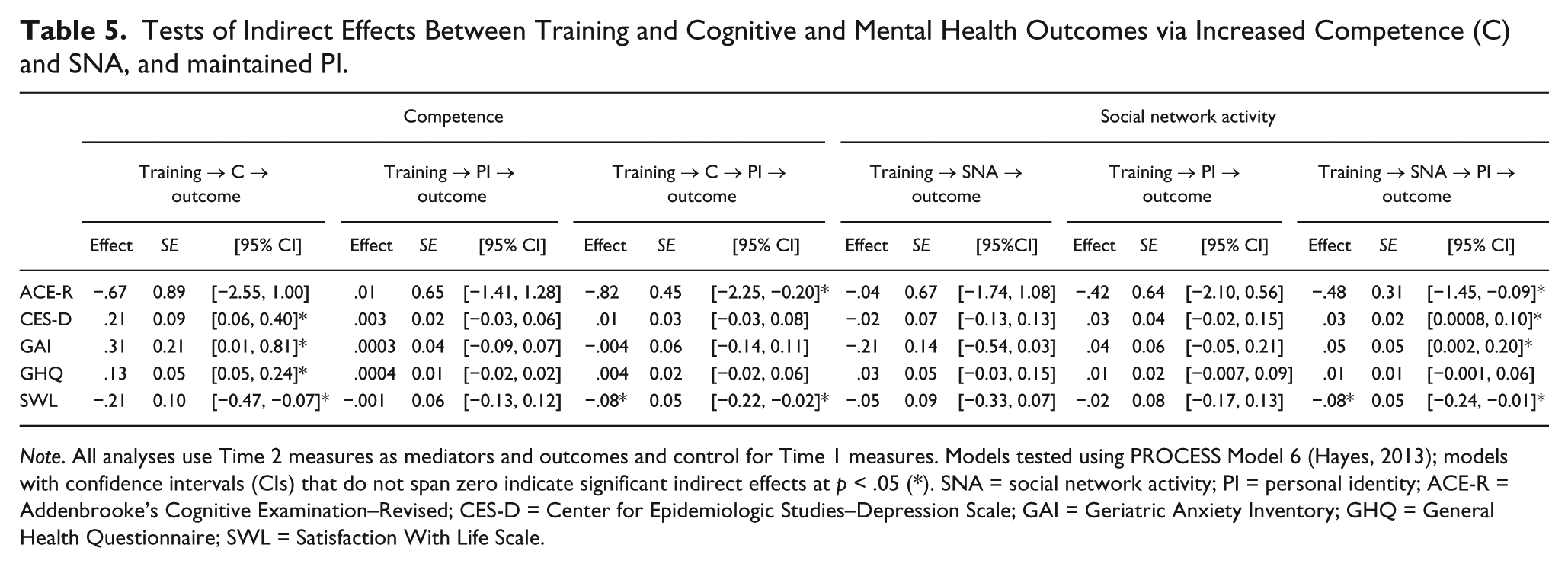
Note. All analyses use Time 2 measures as mediators and outcomes and control for Time 1 measures. Models tested using PROCESS Model 6 (Hayes, 2013); models with confidence intervals (CIs) that do not span zero indicate significant indirect effects at p < .05 (*). SNA = social network activity; PI = personal identity; ACE-R = Addenbrooke’s Cognitive Examination–Revised; CES-D = Center for Epidemiologic Studies–Depression Scale; GAI = Geriatric Anxiety Inventory; GHQ = General Health Questionnaire; SWL = Satisfaction With Life Scale.
Indirect effects on cognitive improvement
The model testing the serial links between training, increased competence, maintained personal identity strength, and improved ACE-R scores revealed 95% confidence intervals for the two-step meditational path that did not include zero, suggesting a significant indirect effect. Similarly, the model testing the serial links between training, expanded social networks, maintained personal identity strength, and improved ACE-R scores revealed confidence intervals for the two-step path did not span zero, suggesting a significant indirect effect.
Indirect effects on mental health
The models run on mental health indicators produced slightly different patterns for each mediator. The model testing sequential effects via increased competence revealed support for a single-step meditational model linking training to reduced depression (CES-D), anxiety (GAI), and improved general mental health (GHQ) via increased competence alone (i.e., not further mediated through maintained personal identity strength). The analysis of SWL revealed the two-step meditational path via competence and personal identity strength. The model testing sequential effects on these outcomes via increased social network activity revealed support for the two-step meditational pathway for CES-D, GAI, and SWL, but not for GHQ.
Discussion
Participants who were randomly assigned to a training group (vs. a control), who received computers, Internet connections, and supportive training in the use of these for social purposes, displayed progressively more positive attitudes about computers and enhanced feelings of self-competence. Consistent with the intention of the training, this group also displayed increased social network activity across time, as well as a maintained sense of self (i.e., personal identity). Finally, the training had cognitive benefits. Notably, these changes were intertwined: Analyses of indirect effects showed that the improved cognitive capacities of trainees were in part explained through their maintenance of self (consistent with Jetten et al., 2010; Jones et al., 2011), and that this, in turn, was partly explained by the twin processes of improved self-competence and increased social engagement.
There were similar indirect pathways to improved mental health, but direct effects of training on these mental health outcomes were not observed. This could suggest that the mental health benefits of receiving the training were offset by additional unexamined processes (e.g., frustration), or that these effects are more complex or simply require more time to develop and unfold. Similarly, the fact that we observed significant effects of the intervention on the amount of reported social activity, but not on participants’ subjective satisfaction with their social relationships or reductions in felt loneliness, could suggest that these more qualitative features of social networks are harder to affect, or take longer to percolate, than quantity of contact alone. To clarify this picture, future research should seek to extend these findings by exploring the longer term impact of computer and Internet use on the social worlds and emotional well-being of older adults who receive such training.
Implications
The present findings provide a positive signal for technology-based interventions to support the well-being of vulnerable older adults. Informed by theory, and a growing literature on socially based interventions (see Jetten et al., 2012; Jetten et al., 2014), the current investigation prioritized the social use of technology, rather than technology per se. That is, we did not just give trainees computers and teach them how to use them as computers. Rather, training specifically focused on the use of computers as social tools, in addition to ensuring basic skills. This, perhaps, explains the broader range of effects observed relative to past work, in which skills acquisition was the primary focus (e.g., Slegers et al., 2008; White et al., 2002).
Along these lines, and in keeping with our general theoretical framework, we do not believe that computers themselves were responsible for any benefits that accrued. Indeed, based on our experiences in this project, we echo the critical warning that to properly address the social isolation of older adults one should not mistake “broadband connections for social ones” (e.g., Coward, 2014). For computer and Internet provision to become viable components of intervention to address the social and psychological needs of older people, our results suggest that these should be accompanied by supportive training in how to use these as tools of social engagement, an analysis supported by the observed meditational roles of increased social network activity and maintained sense of self in addition to improved feelings of competence.
Extending this point further, we also do not believe that technology is the only intervention that should be considered in this space. Although our participants generally experienced the training positively, feedback from carers suggested that some individuals did not find this a positive and enhancing experience, and preferred not to engage with the computer they were given. While we do not know what factors determined this experience, it is clear that computers are not for everyone. Alternative interventions may be needed to address this group. But, again, the mechanisms we observed in our study are useful for informing such alternatives. Consistent with social-psychological theories, our study found that feelings of self-competence, social engagement (e.g., Reis et al., 2000), and maintenance of identity (Jetten et al., 2010; Jones et al., 2011) were critical to the intervention’s success. On this basis, we suggest that alternative interventions should also try to maximize the likelihood of these processes being activated.
Limitations
Further larger scale experimental investigations are still clearly necessary and our findings suggest value in pursuing this line of enquiry. A key limitation of the present study (and comparable previous ones: Slegers et al., 2008; White et al., 2002; Woodward et al., 2011) is the inability to disentangle the effects of training from the trainer. Regular visits from a trainer could, arguably, account for the increased social engagement observed. However, several points speak against this interpretation. First, all participants were receiving care. Attentive visits were not new or novel to our participants, irrespective of condition. Second, increased social activity was carried mostly by changes in reported contact with grandchildren and children rather than relationship categories that could plausibly contain carers. 3 Finally, training ended at least 1 month prior to follow-up assessment, and the last month of training was delivered remotely on an ad hoc basis. Contact with trainers was neither recent nor regular by the time of the follow-up assessment. Nonetheless, future investigations should control for this possibility more rigorously, for example, via a second control group receiving visits of similar regularity and duration to those in the training group.
A further important limitation of the present study is that of attrition. Although the level of attrition itself was not surprising, especially given the population being studied (i.e., vulnerable older adults receiving care), attrition inevitably creates the possibility that any effects observed might be due to differences between those who completed and those who did not, either alone or in combination with the intervention given. While we cannot rule out this as a source of bias in our data, baseline checks did not detect any significant differences between those who remained in the study and those who dropped out, and patterns of dropout were not confounded with condition. Furthermore, intention-to-treat analyses, in which no change was assumed for those who dropped out, confirmed the robustness of the observed patterns. It is, of course, still possible that those who dropped out differed from those who did not on some dimension that was not measured in the study, or that dropout was related to some condition that developed over the course of the intervention but was not apparent at baseline (e.g., an emerging mental or physical health condition resulting in withdrawal). Unfortunately, without any Time 2 data from those who dropped out, this issue cannot be resolved.
A final potential limitation of this work is the enduring relevance of the issues we have raised. Specifically, it could be argued that the importance of providing older adults with supportive training in the social use of Internet technology might wane as current generations, who are more accustomed to living their lives online, grow older and enter care. While it is true that computer literacy is likely to increase with each generation, technology itself is not static and also changes across time. As such, we do believe that there will always be an important place for technological support within the care environment, and that this will remain true even with improved technological competency among the clients of care providers. Irrespective of what the future holds in terms of computer literacy, it is also the case that right now technological access and support to clients is relatively low in the care sector. For example, one recent report estimated that only ~20% of care homes in the United Kingdom routinely provide Internet access to their residents (McCardle, 2013). Based on our findings, we would suggest that this might be a missed opportunity for improving the quality of life of residents and something that needs to change in the present, rather than waiting for the future to change around it.
Conclusion
Interventions that support older individuals to maintain their social connections are vitally needed. Internet technology is an often-suggested basis for such interventions; however, past research suggests only limited benefits of this for older adults. In contrast, our experimental study revealed that the combination of a user-friendly computer interface with supportive training (a) significantly improved the cognitive capacity of trainees, (b) did so through supporting the self and activating social connections, and (c) indirectly flowed through the same processes to improve indicators of mental health and well-being. Thus, we highlight the utility of socially guided technological interventions to support and empower older adults to build their social connections, participate in meaningful social networks, and through this experience better health and well-being.
Footnotes
Acknowledgements
The larger project involved data collection in Italy. Due to logistical challenges, the Italian study was not experimental precluding comparison across countries. This article focuses on the U.K. data only. For more details of the project and partners, see ![]() . We acknowledge the support of the Italian team in the larger project, particularly Lucia di Furia and Angela Genova. In the United Kingdom, access to participants, the recruitment and training of care technologists, and the provision of training were all coordinated by Somerset Care Ltd. We are particularly thankful to Julie Cullis, Sarah Scott, Jason Shaw, Katherine Alexander, Emma Green, and Tina Wells. We are also grateful to Antonio Dell’Atti and Ben Neild for project management.
. We acknowledge the support of the Italian team in the larger project, particularly Lucia di Furia and Angela Genova. In the United Kingdom, access to participants, the recruitment and training of care technologists, and the provision of training were all coordinated by Somerset Care Ltd. We are particularly thankful to Julie Cullis, Sarah Scott, Jason Shaw, Katherine Alexander, Emma Green, and Tina Wells. We are also grateful to Antonio Dell’Atti and Ben Neild for project management.
Author Contributions
The research was designed by C.H. and T.A.M. Data were collected and collated by M.B., R.K., L.-G.M., and N.W. Analyses were performed by T.A.M. and N.W. The article was written by T.A.M., N.W., and C.H.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the European Commission’s Programme for Employment, Social Affairs, and Inclusion (PROGRESS: 2007-2013; grant number: VS/2012/0346).