
Abstract
Introduction
Chronic illness is a worldwide public health concern. As populations live longer, chronic non-communicable diseases (NCDs) now constitute the major cause of death and disability around the world. (Di Cesare et al., 2013). Low- and middle-income countries (LMICs) are disproportionally affected by the morbidity and mortality from NCDs. Latin American countries have had an especially fast pace of population aging (Palloni, Pinto-Aguirre, & Pelaez, 2002) and are expected to have the highest NCD growth rates in the world in the next decades (Wagner & Brath, 2012). Limited health infrastructures are often insufficient to care for the needs of LMICs’ aging and chronically ill populations. These countries face a multiple burden from NCDs and other conditions such as infectious diseases, injuries, and maternal-child health issues (Di Cesare et al., 2013).
The burden from NCDs may have a toll on cognitive ability of aging individuals (Lipnicki et al., 2013). Impaired cognition, in turn, may impair older adults’ quality of life and independent living (Hendrie et al., 2006). In later life, impaired cognition is linked to lower adherence to medical treatments (Fang, Nicholas, & Silverman, 2010; McArdle, Smith, & Willis, 2009), worse health, poor decision making, higher medical expenditures, and worse economic outcomes (Fang et al., 2010; McArdle et al., 2009; Smith, McArdle, & Willis, 2010). There are no current medical technologies or interventions capable of significantly and sustainably revert cognitive loss once a deficit is established. Preventing cognitive impairment is therefore a matter of great public health interest. Understanding the determinants of cognitive impairment is an important step to identify targets for preventive strategies.
Cognition in later life is influenced by factors across the life span. Genetic predisposition, childhood health, nutritional, and economic circumstances (Borenstein, Copenhaver, & Mortimer, 2006; Case & Paxson, 2008), and educational attainment (Banks & Mazzonna, 2012; Case & Paxson, 2009) are among the early-life factors associated with late-life cognitive ability. Labor market and earning opportunities (Reuser, Willekens, & Bonneux, 2011) and other lifestyle factors and behaviors (Nguyen, Couture, Alvarado, & Zunzunegui, 2008; Salthouse, 2013) are midlife factors that also play important roles. In healthy individuals, cognitive ability begins to decline as early as in young adulthood, and seems to occur with little variability across individuals of a same-age range (Salthouse, 2004).
NCDs may affect cognitive ability through diverse and potentially simultaneous mechanisms. Some NCDs may directly impair brain function, such as in the case of neurologic (Langa, Foster, & Larson, 2004) and mental health conditions (Sáez-Fonseca, Lee, & Walker, 2007). NCDs may indirectly affect brain function through imbalances in circulation, oxygenation, and metabolic homeostasis (Breteler, Claus, Grobbee, & Hofman, 1994; Chang-Quan et al., 2011; Incalzi et al., 1993). Pharmaceuticals frequently used to treat NCDs may have adverse effects that affect cognition (Cancelli, Beltrame, Gigli, & Valente, 2009). Scarcity and resource depletion that may result from the loss of productivity and income of living with an NCD may negatively affect cognition (Shah, Mullainathan, & Shafir, 2012). Finally, the experience of living with a NCD and engaging in its long-term management may impair cognition through increased stress and depression (Barnett et al., 2012; Korczyn & Halperin, 2009; Sáez-Fonseca et al., 2007).
In this study, we aim to (a) identify whether there is a link between NCDs and cognitive function among older adults in Latin America. We investigate if this association differs across gender, and if it is more pronounced among those individuals in the bottom of the cognition distribution; (b) explore whether there is evidence supporting a dose-response type of association with the number of comorbidities; (c) evaluate whether there is evidence supporting a differential association across specific NCDs or disease groups.
We specifically hypothesize that the underlying physiopathological mechanisms may influence the association between specific NCDs and cognitive scores. If our hypothesis holds, NCDs that directly impair brain function, such as neurologic and mental health conditions, would have the greatest association with lower cognitive scores among all NCDs, because their mechanisms of action might almost necessarily affect cognition. NCDs that may potentially indirectly affect brain function through imbalances in circulation, oxygenation, and metabolic homeostasis, such as heart disease, lung disease, hypertension, and diabetes, would also be associated with lower cognition but at a smaller magnitude than diseases with direct brain effects. NCDs with unlikely direct or indirect impact on brain function, such as arthritis, osteoporosis, and cancer, would have the lowest association with cognitive scores, but this association might still be present because of the effect on brain function from factors such as the effect of pharmaceuticals, stress, and resource depletion, as described above.
Data
SABE Survey: Health, Well-Being, and Aging (Salud, Bienestar y Envejecimiento) in Latin America and the Caribbean
We use publicly available data from the SABE database, a household survey of non-institutionalized individuals aged 60 years and above from major metropolitan areas of seven Latin American countries (Argentina, Barbados, Brazil, Chile, Cuba, Mexico, and Uruguay). SABE was implemented between 1999 and 2000 through a partnership between the Pan-American Health Organization (PAHO), the U.S. National Institute on Aging (NIA), the Center for Demography and Ecology of the University of Wisconsin–Madison, and academic institutions from participating countries (Albala et al., 2005).
The SABE survey was modeled after the U.S. Health and Retirement Study. SABE used standardized questionnaires especially designed to allow for cross-country comparisons (Wong, Pelaez, Palloni, & Markides, 2006). SABE collected comprehensive data on demographic characteristics, socio-economic conditions, and current and past health. In addition, biometric (height, knee height) and cognitive measurements (Mini-Mental State Examination [MMSE]) were objectively ascertained (Wong et al., 2006). SABE used a multistage census-based cluster sampling methodology that has been described in detail elsewhere (Albala et al., 2005).
We pooled data from individuals aged 60 years and above from four of the SABE survey sites: Brazil (São Paulo), Chile (Santiago), Mexico (Mexico City), and Uruguay (Montevideo). We chose these countries a priori because of their similarities in terms of health systems, geography, and population, aiming to obtain the most homogeneous pooled dataset as possible. Information from Argentina was not included because of the lack of a key covariate (knee height) which proxies for accumulate health during first years of life. Data from Cuba (Havana) and Barbados (Bridgetown) were not included because these two island countries have marked structural differences to the countries we studied, including population size and health systems characteristics.
Measurement of Cognition
Cognitive ability was the main dependent variable in this study. SABE measured cognitive ability through a modified version of the MMSE, intended to minimize low literacy bias (Quiroga, Albala, & Klaasen, 2004). Modified-MMSE scores ranged from 0 to 19, with higher scores indicating better cognitive ability (Quiroga et al., 2004). In general, cognitive ability can be understood as a combination of two main systems: fluid and crystallized intelligence. Fluid intelligence is characterized by the capacity to solve new problems, whereas crystallized intelligence reflects accumulated knowledge (Cattell, 1967; McArdle, Ferrer-Caja, Hamagami, & Woodcock, 2002). Measures of fluid intelligence decline fast with age, whereas crystallized intelligence tends to increase in early life and decline after middle age (Park & Gutchess, 2006). The MMSE does not primarily measure fluid intelligence, because this test does not present novel problem-solving situations (McArdle, 2011). The MMSE involves a series of questions about orientation, memory, and executive functioning, and relies heavily on language skills, therefore being mostly a test of crystallized intelligence.
Cognitive scores from 40 individuals from the Chile (Santiago) survey site could not be included in our analysis. Following other studies that utilized the same data, we treated these observations as missing values (Maurer, 2010).
A cutoff score of 12 points has been proposed to divide cognitively impaired (MMSE score: 0-12) from unimpaired (MMSE score: 13-19) individuals in previous investigations of the SABE survey (see, for example, Nguyen et al., 2008). We used both the total and the dichotomized MMSE scores in our analysis. In our robustness checks, we explored an alternative classification based on the observed distribution of MMSE scores in our sample. Our alternative classification kept the same cutoff point for unimpaired cognition (MMSE scores: 13-19), but cognitive impairment was divided between mild/moderate (MMSE scores: 7-12) and severe (MMSE scores: 0-6).
Measurement of Chronic Conditions
The number and type of chronic conditions were the main independent variables in the present study. SABE collected information on NCDs via self-report (Barcelo, Pelaez, Rodriguez-Wong, & Pastor-Valero, 2006; Palloni & McEniry, 2007; Wong et al., 2006). Individuals were asked whether a physician or a nurse had ever diagnosed them with any of the following: hypertension, diabetes, heart disease, lung disease, stroke, psychiatric conditions, cancer, arthritis, and osteoporosis (Ostbye et al., 2005). Individuals with any diseases were classified as having “one” or “two or more” NCDs. An individual was classified as having no disease, if he or she replied negatively to all NCDs. Individuals with no diseases were utilized as the reference group throughout this study.
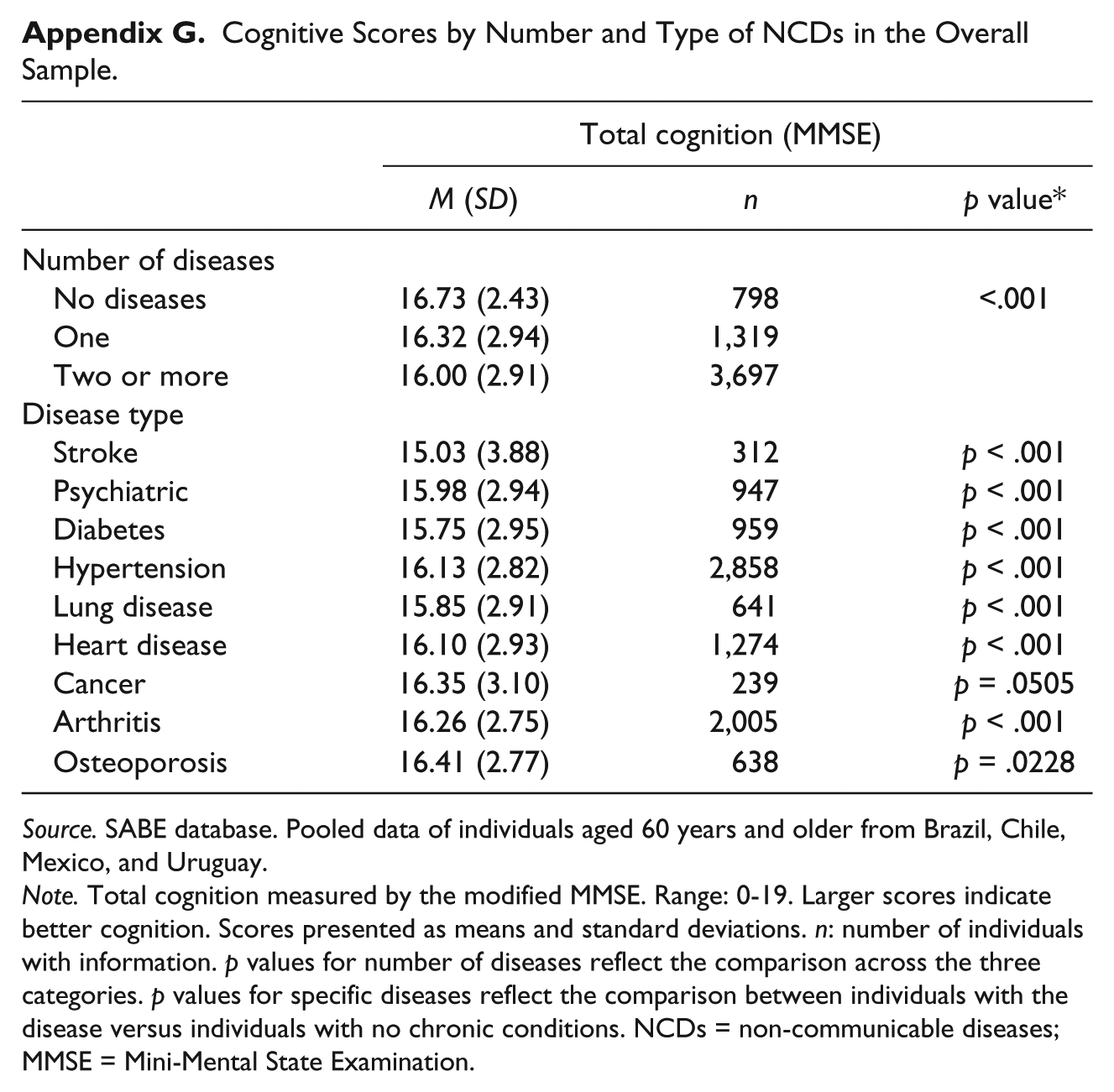
Specific NCDs (stroke, neuropsychiatric conditions, hypertension, diabetes, heart disease, lung disease, cancer, arthritis, and osteoporosis) were analyzed individually, one at a time. When interpreting the results, we considered three different groups of NCDs according to their potential effect on brain function, as follows: Group 1—NCDs with potential direct effect over brain functions: stroke and neuropsychiatric disorders; Group 2—NCDs with potential indirect effect on brain function through impairments of the body’s circulation, oxygenation, or metabolic homeostasis: hypertension, heart disease, lung disease, and diabetes; Group 3—NCDs with no direct effect and none or minimal indirect effect on brain functions via impairments in circulation, oxygenation, or metabolic homeostasis: arthritis, osteoporosis, and cancer. Appendix F shows the prevanlence of chronic conditions in each site. Appendix G shows the cognitive scores by number and type of chronic condition.
Measurement of Control Variables
SABE collected extensive information on demographic, economic, and early-life characteristics, which composed the main control variables in our analytical models. The selection of covariates was driven by existing work in the literature (Case & Paxson, 2008; Huang, Lei, Ridder, Strauss, & Zhao, 2013; Maurer, 2010), and included only exogenous variables. All our control variables are described below.
Age
Age was measured as a continuous variable in years. A quadratic term for age was included in the regression models to allow changes in the effect on cognition to be identified across the various age ranges.
Marital status
Marital status was classified as “married” if individuals were currently married or in a civil union, and “not married” otherwise.
Education level
Education level was defined as the highest completed educational degree. To accommodate for the different education systems across countries, SABE included different degrees that ultimately represented equivalent education categories. For simplification, we aggregated the education categories in four major groups: elementary/middle school, high school, technical school, and college/graduate school. The multiple-choice question on the highest completed educational degree did not have an option corresponding to “incomplete or no school attendance.” Therefore, we suspected that missing values corresponded to “no education/incomplete degree.” To check this assumption, we compared missing values with the number of people who responded “no” to the question of whether they were able to read or write, and we found that the two groups were equivalent. As we implemented reduced-form models, we only included level of education in the model specification. Among seniors, it is safe to assume that education is exogenous and a good proxy for individual socio-economic level. We did not control for occupation, income, or type of job even though these variables were available because these controls are individual choices even among older population. It is important to highlight that we run specifications (These results are not reported) with full controls and the fundamental results do not change.
Early-life health conditions
Health status before age 15 years was categorized as “excellent” or otherwise. The family’s economic circumstances before age 15 years were categorized as “good” or otherwise. Nutrition scarcity was categorized as “never hungry” (never having had a period of lack of food resulting in hunger between age 0 and 15 years) or otherwise. These variables were based on self-reports and provided in the original scale.
Knee height
Knee height can be considered an objectively obtained proxy for early-life conditions. Early-life circumstances affect both the physical and cognitive development of an individual, and manifestations of both these mechanisms, such as height and cognition, are highly associated (Case & Paxson, 2008; Maurer, 2010; Stowasser, Heiss, McFadden, & Winter, 2014). In later life, body height is susceptible to the influence of shrinkage, fractures, and frailty. Because late-life conditions affecting body height may also affect cognitive ability, studies of the determinants of late-life cognition have used knee height as an instrument for body height to reduce endogeneity (Huang et al., 2013; Lei, Hu, McArdle, Smith, & Zhao, 2012; Maurer, 2010).
Survey site
Indicator variables were added to identify the individual’s place of residence: Chile (Santiago), Mexico (Mexico City), and Uruguay (Montevideo). Brazil (Sao Paulo) was the reference group in all the analyses.
Empirical Strategy
Conceptual Framework
Figure 1 illustrates the conceptual framework linking NCDs and cognition, and displays the inter-relationships between the various early-, mid-, and late-life factors. NCDs may directly affect cognition through biological mechanisms such as brain damage and neurochemical imbalance, or act through biosocial, behavioral, and economic pathways such as stress from disease management, impairment of quality of life, and others. NCDs may also mediate the effect of early-life circumstances, education, and mid/late-life factors on late-life cognition.
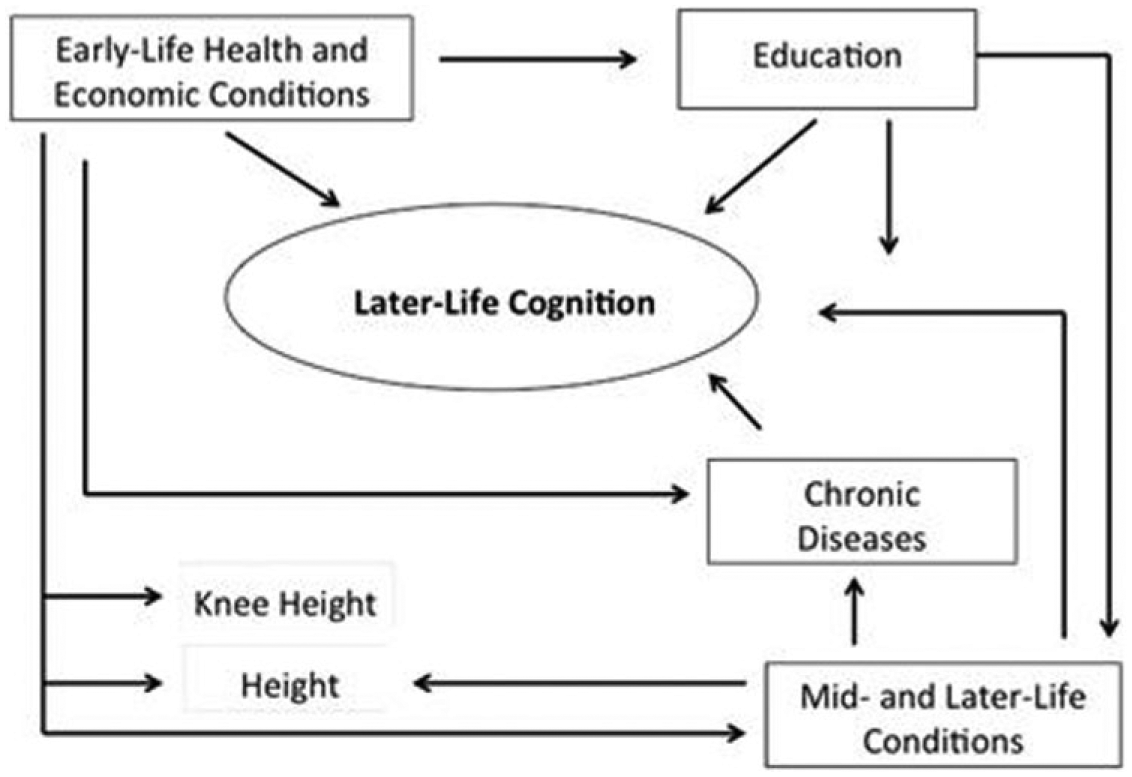
Conceptual model of the determinants of late-life cognition and the role of chronic diseases.
Cognitive ability can, in turn, affect NCD outcomes through poorer self-management, lower disease awareness, impaired interpersonal communication, and others. Although not depicted, non-cognitive (character) skills may influence the inter-relationships between the various factors and cognitive ability. For example, non-cognitive skills have been found to mitigate the decline of cognitive ability observed with age (Salthouse, 2013).
Analytical Model
The following model was used to estimate the proposed conceptual framework:

In this model
Without including the control variables, β1 captures the raw correlation between NCDs and cognitive ability (Aim 1). Including the control variables will remove from this raw correlation the effect of other characteristics influencing cognitive ability in early-, mid-, and late-life conditions. Notice that coding the chronic condition indicator as dummy variables to capture number of chronic conditions allows us to investigating if cognition declines with number of conditions (Aim 2). Finally, using relevant dummies according to the groups of chronic conditions described in the introduction allow us to explore Aim 3.
The orthogonal assumption about the error term may be difficult to hold in a cross-sectional setting, as the error term may capture unobservable factors that may simultaneously affect cognitive ability and NCD status. For example, differences in past cognitive abilities that helped individuals produce better health over life span, or differences in past illness severity that influenced current cognitive ability and current propensity to NCDs. The error term may also capture unobserved systematic individual differences, such as differences in non-cognitive skills or in the ability to access better care.
Main Analytical Approach
The equation of interest was estimated using ordinary least squares (OLS) and Tobit regression models, to account for the right-censored nature of the cognitive measurement (Amemiya, 1984). The two models were estimated first in a reduced-form controlling for age, squared term for age, and survey site fixed effects (Model 1). Models were then extended to add all control variables: marital status, education, knee height, and health, economic conditions and nutrition scarcity before age 15 years (Model 2).
Cases with incomplete information on early-life health conditions (0.95% of females, n = 34; and 0.72% of males, n = 16) were excluded from the extended analyses. Cases with missing information on knee height (8.8% of females, n = 314; and 11.3% of males, n = 252) were input the gender-specific average and were identified in the extended regression models by an indicator variable for missingness.
In the first set of regressions, the main independent variable was the number of NCDs, classified as one, or two or more, NCDs (reference group: no NCDs). In the second set of regressions, the main independent variable was each specific NCD (reference group: no NCDs). Models were implemented for each NCD, one at a time. The third set of regressions consisted of linear probability models implemented to differentiate between cognitively impaired (MMSE score: 0-12) from unimpaired (MMSE score: 13-19) individuals. This is important to test whether the effect of having one chronic condition or multiple conditions will reflect in reducing cognitive ability at the margin of being impaired.
Analytical models were implemented separately for females and males. The distribution of MMSE scores and control variables differed significantly between these two groups. Also, females and males have different trajectories in cognition determinants such as nutritional, educational and occupational opportunities (including earnings), self-care, and other behavior choices. Furthermore, the relationship between the multiple determinants and cognitive abilities may vary between females and males.
The statistical analysis was implemented using Stata Statistical Software: Release 12 (StataCorp. 2011, College Station, Texas).
Sensitivity Analysis
The initial models were complemented with a series of robustness checks. First, because stroke and psychiatric diseases were strongly associated with MMSE scores, it could be argued that their mechanisms of action might almost necessarily affect cognition. To explore the possibility that NCDs with direct effects on brain function might be the largest drivers of the association between NCDs and cognition, OLS and Tobit models were repeated after excluding all cases of stroke and psychiatric diseases from the sample.
Second, non-parametric specifications on age were implemented in the OLS models to explore whether the observed association between NCDs and cognitive score was an artifact of mortality selection. Third, a quantile regression model was implemented to evaluate whether the effect of NCDs was different across the distribution of cognitive scores. Finally, ordinal probit models were implemented to evaluate differences in the probability of being severely impaired (MMSE scores: 0-6), mild/moderately impaired (MMSE scores: 7-12), or unimpaired (MMSE scores: 13-19). With the exception of the non-parametric specification on age, which also looked at type of NCDs, all other robustness checks used the number of NCDs as the main independent variable.
Results
Sample Characteristics
A summary and description of key variables is displayed in Table 1. The final sample totalized 5,814 individuals from four survey sites: Brazil (n = 1,967), Chile (n = 1,265), Mexico (n = 1,133), and Uruguay (n = 1,449). Our sample was composed of a higher percentage of women (61.5%, n = 3,578) than men (38.5%, n = 2,236). Females and males were significantly different in all characteristics except for age (Table 1).
Description and Summary Statistics for Key Variables.

Source. SABE Database. Pooled data of individuals aged 60 years and older from Brazil, Chile, Mexico and Uruguay.
Note. MMSE is obtained by direct measurement. Lower MMSE scores indicate worse cognition. Chronic diseases: self-report of having ever been diagnosed with the condition by a doctor or nurse. Numbers in parentheses after each of the chronic diseases correspond to the total number of individuals who answered the question, by gender (female, males). Married: individuals presently married or in a civil union, reference: otherwise. Education: highest degree completed, reference: otherwise. Early-life conditions: self-reported conditions between age 0 and 15 years: excellent health (reference: good or poor health), good economic conditions (reference: average or poor), never hungry: never having had a period of hunger between age 0 and 15 years (reference: having experienced hunger). Place of residence: indicator variables identifying the metropolitan area where the individual resides. p value: calculated by chi-square test for categorical variables (education category and place of residence), and by t test for continuous variables and proportions (other variables). NS = non-significant (p > .05). MMSE = Mini-Mental State Examination.
Females were more likely to have two or more NCDs (71% vs. 52%, p < .0001), and less likely to have one (19% vs. 28.6%, p < .0001) or no NCDs (10% vs. 19%, p < .0001). Females were more likely than men to have any of the NCDs of interest (p < .0001 for all of the conditions). Females were less likely to be married (p < .0001), less likely to have had excellent health during childhood (p = .032), and tended to have lower education attainment (p < .0001) than men. Nonetheless, females were more likely to have had good economic conditions and no periods of hunger during childhood (p < .0001 for both).
Figure 2 shows the distribution of cognitive scores in our sample. Females tended to have lower cognitive scores (MMSE = 16.05 ± 2.97) than males (MMSE = 16.3 ± 2.69, p < .0001). In both cases, the distribution of MMSE scores was skewed to the left, with most of the scores concentrating in the upper limit.

Distribution of cognitive scores among older adults in our sample of four Latin American countries.
Table 2 presents a comparison of key variables between individuals with and without NCDs separately for females and males. Overall, individuals with one or more NCDs tended to have lower cognitive scores when compared to those with no NCDs (MMSE = 16.0 ± 2.99 vs.16.7 ± 2.68, p < .0001 among females and MMSE = 16.26 ± 2.79 vs. 16.79 ± 2.79, p = .0004 among males) and tended to be older (71.4 ± 7.85 vs.69.4 ± 7.74 years, p < .0001 among females and 71.6 ± 7.75 vs. 69.6 ± 7.02 years, p < .0001 among males). Females with one or more NCDs had significantly lower educational attainment, and significantly worse early-life health, economic and nutritional conditions than females with no NCDs. Males with and without NCDs, however, did not significantly differ in terms of these characteristics.
Descriptive Statistics of Individuals With and Without NCDs.

Source. SABE Database. Pooled data of individuals aged 60 years and older from Brazil, Chile, Mexico and Uruguay.
Note. NCDs: self-report of having ever been diagnosed by a doctor or nurse with stroke, psychiatric condition, hypertension, heart disease, diabetes, lung disease, cancer, arthritis, or osteoporosis. Total cognition measured by MMSE score (range: 0-19). Lower MMSE scores indicate worse cognition. Married: individuals presently married or in a civil union, reference: otherwise. Education: highest degree completed, reference: otherwise. Early-life conditions: self-reported conditions between age 0 and 15 years: excellent health (reference: good or poor health), good economic conditions (reference: average or poor), never hungry: never having had a period of hunger between age 0 and 15 years (reference: having experienced hunger). Place of residence: indicator variables identifying the metropolitan area where the individual resides. p = p value: calculated by chi-square test for categorical variables (education category and place of residence), and by t test for continuous variables and proportions (other variables). NS = non-significant (p > .05). NCDs = non-communicable diseases; MMSE = Mini-Mental State Examination.
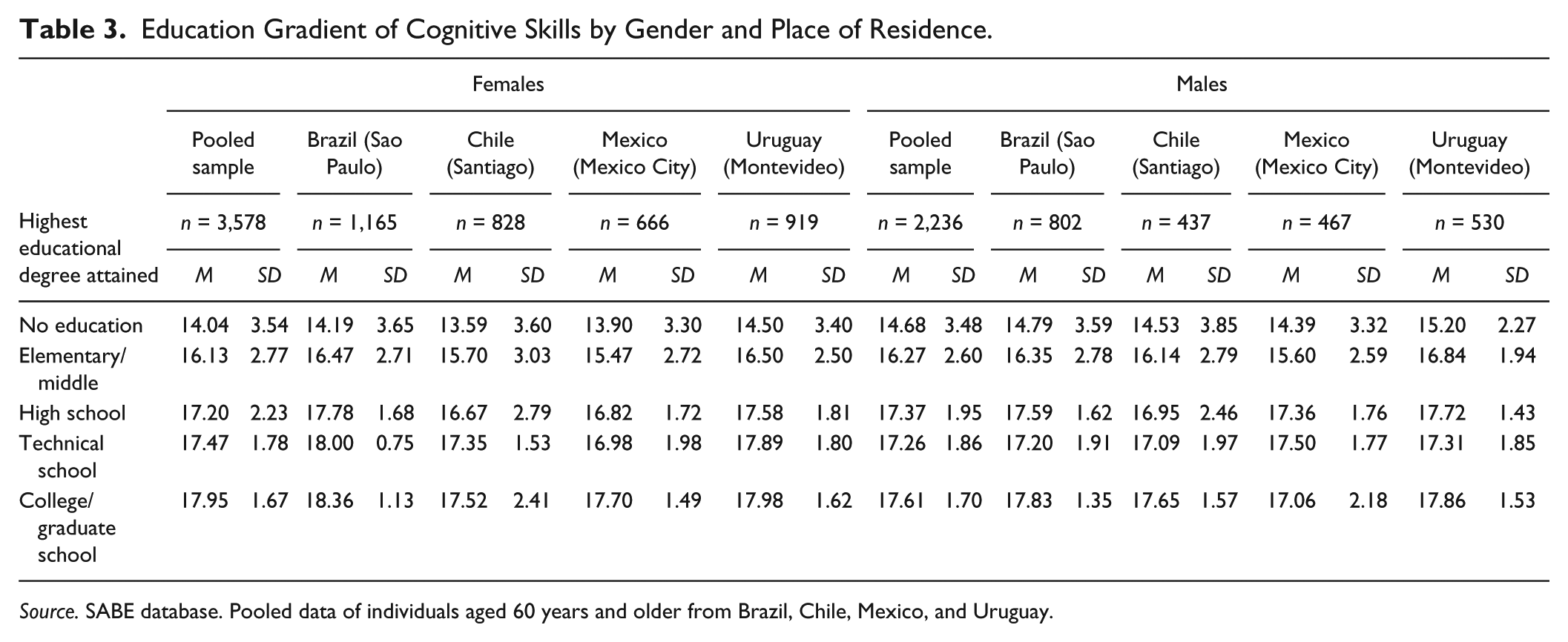
Table 3 displays the distribution of cognitive scores according to education levels. Between individuals of the same gender, MMSE scores tended to be lower for persons with lower education (p < .0001 for the trend in all survey sites). Among those with no education, MMSE scores were significantly lower among females than males (MMSE = 14.04 ± 3.54 vs. 14.68 ± 3.48, p = .011). Conversely, among those with college or graduate degrees, MMSE scores tended to be higher among females than males (MMSE = 17.95 ± 1.67 vs. 17.61. ± 1.70, p = .085). MMSE scores were not significantly different across genders for those with elementary/middle, high school, or technical school degrees.
Education Gradient of Cognitive Skills by Gender and Place of Residence.
Source. SABE database. Pooled data of individuals aged 60 years and older from Brazil, Chile, Mexico, and Uruguay.
General Determinants of Cognitive Skills in Later Life
Table 4 shows the estimates of the association between the control variables and cognitive ability as obtained from OLS and Tobit reduced and extended models. These results are briefly reviewed here to demonstrate that the estimates are consistent with models of human capital production of cognitive skills over the life span previously reported in the literature.
OLS and Tobit Estimates of the Association Between Number of NCDs and Cognitive Skills.

Source. SABE database. Pooled data of individuals aged 60 years and older from Brazil, Chile, Mexico, and Uruguay.
Note. Estimates presented as regression coefficients and robust standard errors in parentheses. Tobit estimates presented as marginal effects. Standard errors account for clustering at each survey site primary sampling units. All models include indicator variable for survey site (reference: Sao Paulo). Age sq.: squared term for age, divided by 100. Married: presently married or in a civil union, reference: otherwise. Education: highest educational degree completed, reference: no completed educational degree. Early-life conditions: self-reported conditions between age 0 and 15 years: excellent health (reference: good or poor health), good economic conditions (reference: average or poor). Never hungry: never having had a period of hunger between age 0 and 15 years, reference: having experienced hunger. Knee height: cases with missing information were input the gender-specific average. An indicator variable indicating missing knee height was included in the regressions. Cases with incomplete information on other early-life health conditions were excluded from the analysis Cons.: constant term of the regression analysis. F test: p value of global F-statistic of the regression analysis. Cases with incomplete data on early-life conditions were excluded from the analysis. Pseudo R2 shown for Tobit models. OLS = ordinary least squares; NCDs = non-communicable diseases.
p < .1. **p < .05. ***p < .01.
Age was significantly associated with cognitive scores among both women and men. A positive coefficient for the effect of age and a negative coefficient for the squared term for age (both statistically significant) indicate that the association between age and cognitive ability has a “concave” form, that is, that the association is initially positive but becomes negative as age increases. Being presently married and being more educated were positively associated with cognitive scores in both genders. Being married was associated with an average increase in 0.286 ± 0.080 points in the MMSE score among females and 0.276 ± 0.126 points among males, all other things being equal. On average, as expected, higher education has a positive and statistically significant effect on cognitive skills for both males and females.
Among the early-life characteristics, excellent health before age 15 years was associated with an average 0.161 ± 0.093 points higher MMSE scores (p = .064), and knee height was associated with an average of 0.033 ± 0.014 higher MMSE scores (for each additional cm, p = .014) among females). None of the early-life health characteristics was statistically significantly associated with cognitive ability among males. In sum, as expected, married, education, and good early-life conditions seem to be protective of cognitive capital for both male and female. Cognitive capital depreciates rapidly with age for both genders.
Links Between Number of NCDs and Cognitive Ability
Figure 3 shows the unadjusted decline of cognitive ability with age for individuals with and without NCDs in our sample using locally weighted regression. Cognitive scores decline permanently after age 60 years for both males and females. Without controlling for other covariates that may influence the relationship between NCDs and cognition, having one or more NCDs was associated with a lower cognitive score at each age, as compared with same-age individuals without NCDs, for both genders.
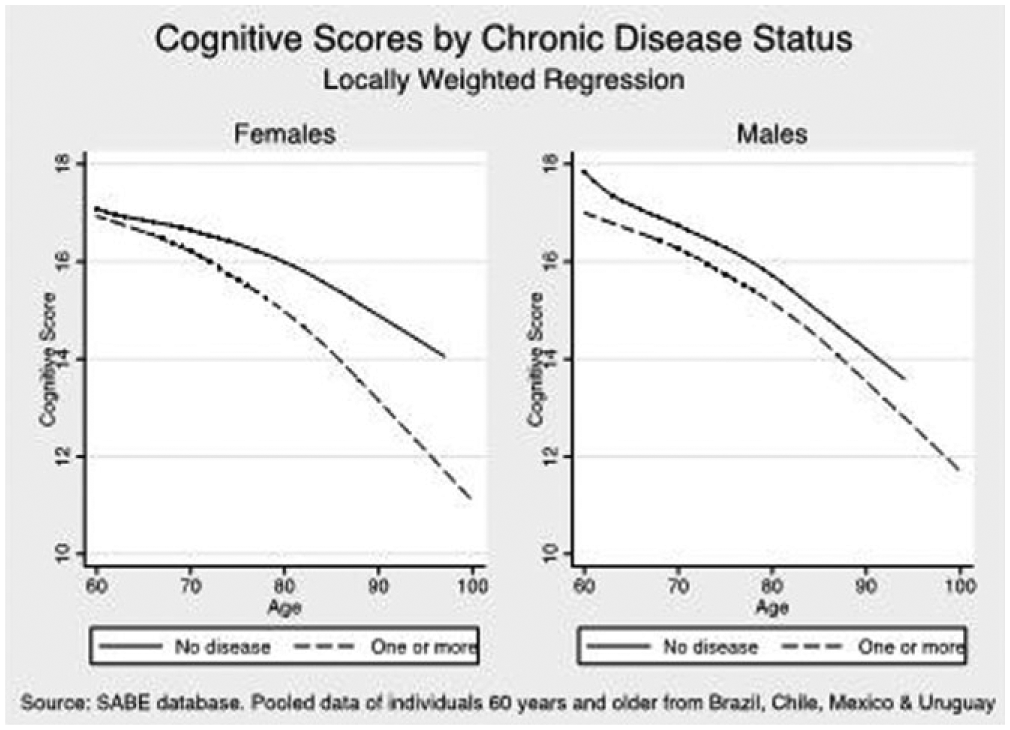
Cognitive scores according to NCD status in our sample of older adults from four Latin American countries.
Table 4 displays the estimates of the association between the number of NCDs and cognitive scores as obtained from the OLS and Tobit reduced and extended models. Among females, the reduced models demonstrate a significant association between the presence of NCDs and lower cognitive scores (OLS estimates ± standard errors: one NCD = −0.434 ± 0.175, p = .014; two or more NCDs: −0.494 ± 0.158, p = .002) as compared with those with no disease. Even though the coefficient for two or more conditions is larger (suggesting a dose-response), the confidence intervals overlap. This result provides a weaker evidence to conclude that individuals with a larger number of chronic conditions show lower cognition. The pattern was different among males, where the reduced models found a significant association among those with two or more NCDs, but not for those with one NCD (OLS estimates ± standard errors: one NCD = −0.040 ± 0.141, p = not significant; two or more NCDs: −0.535 ± 0.125, p < .0001), as compared with those with no disease, all other things being equal.
The full set of control variables (socio-demographic and early-life health characteristics) implemented in the extended models did not offset the association between NCDs and cognitive ability found with the reduced forms. Even though some reduction in the magnitude of the estimates was seen in the extended models, there was no change in the direction of the associations and no loss of statistical significance.
In the OLS extended models, the presence of one NCD among females was associated with lower MMSE scores by an average of −0.346 ± 0.172 points (p = .045), and the presence of two or more NCDs was associated with an average of −0.292 ± 0.151 points (p = .054) when compared with those with no disease, all other things being equal. Among males, the presence of one NCD was associated with lower MMSE scores of, on average, −0.133 ± 0.140 points when compared with those with no disease, but this difference was not statistically significant. The presence of two or more NCDs, however, was associated with lower MMSE scores of, on average, −0.542 ± 0.127 points (p < .0001).
The negative direction of the associations was consistent across the OLS and the Tobit models, but the magnitude of the estimates tended to be higher with Tobit. The 95% confidence intervals for the OLS coefficients invariably included the Tobit estimates, suggesting that there was no statistically significant difference between the results from these two models, and that right censoring did not significantly impact our results.
To improve the understanding of the relationships between NCDs and cognitive scores, the magnitude of this association can be compared with other factors. For example, being married was associated with around 0.28 points higher MMSE scores (around 1.8% of the average value), than the scores of those not married, in both genders. Among females, the negative association between two or more NCDs and cognitive scores was comparable with this magnitude, and the negative association between having one NCD and cognitive scores was slightly larger than that. In the case of males, however, the negative association between MMSE scores and having two or more NCDs was almost double the magnitude of the positive association of being married (men with two or more NCDs had around 0.54 lower cognitive scores than those with no disease; which is around 3% of the current average value of cognitive skills for men). Having one NCD had much lower magnitude of association, of around 0.133 lower scores than those with no disease.
Links Between Type of NCDs and Cognitive Skills
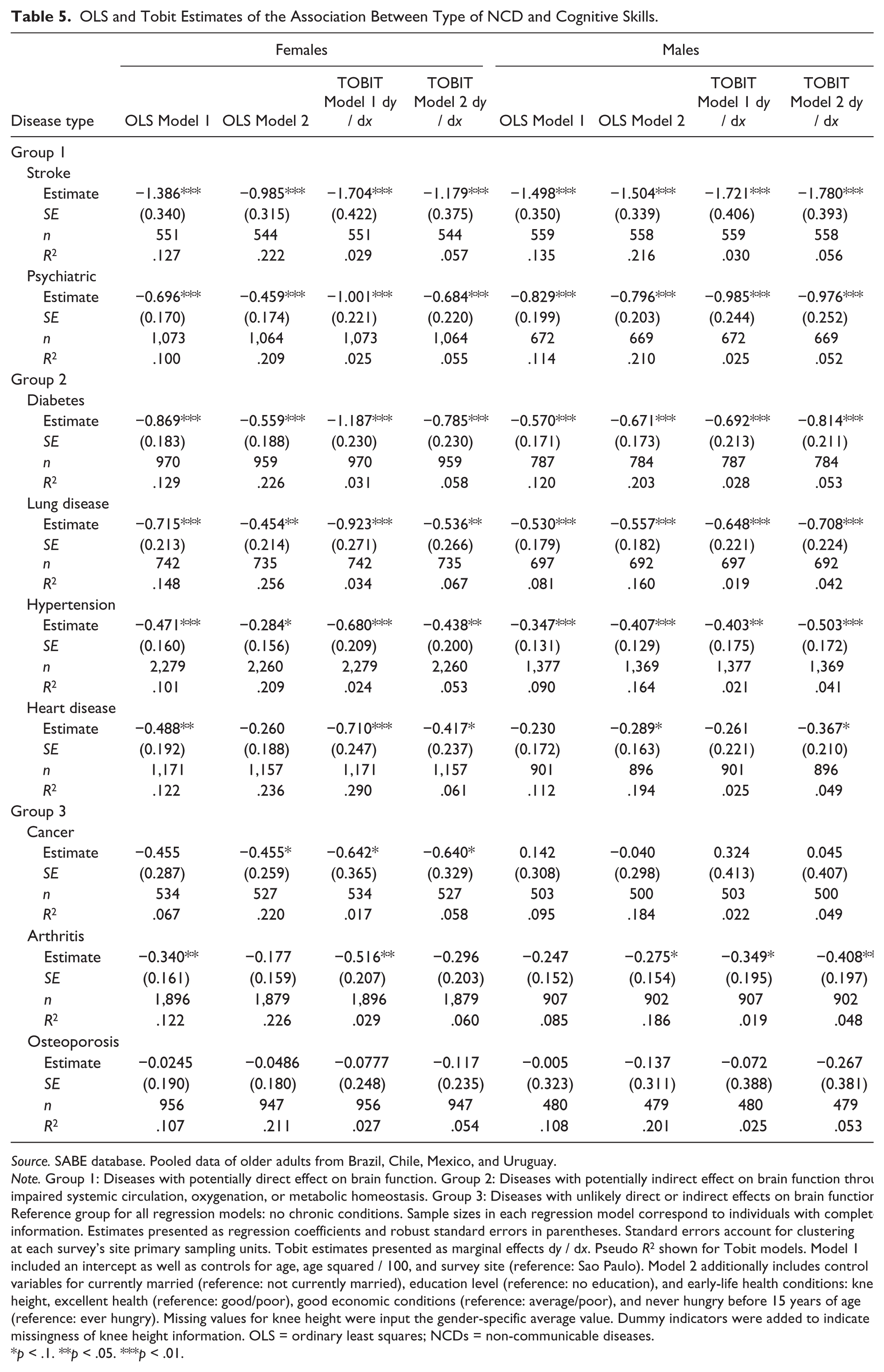
Table 5 displays the results of the reduced and extended OLS and Tobit models exploring the association between the multiple NCDs of interest (stroke, psychiatric conditions, diabetes, lung disease, hypertension, heart disease, cancer, arthritis, and osteoporosis) and MMSE scores. Only the NCD-related coefficients are shown. Full sets of results are available upon request.
OLS and Tobit Estimates of the Association Between Type of NCD and Cognitive Skills.
Source. SABE database. Pooled data of older adults from Brazil, Chile, Mexico, and Uruguay.
Note. Group 1: Diseases with potentially direct effect on brain function. Group 2: Diseases with potentially indirect effect on brain function through impaired systemic circulation, oxygenation, or metabolic homeostasis. Group 3: Diseases with unlikely direct or indirect effects on brain function. Reference group for all regression models: no chronic conditions. Sample sizes in each regression model correspond to individuals with complete information. Estimates presented as regression coefficients and robust standard errors in parentheses. Standard errors account for clustering at each survey’s site primary sampling units. Tobit estimates presented as marginal effects dy / dx. Pseudo R2 shown for Tobit models. Model 1 included an intercept as well as controls for age, age squared / 100, and survey site (reference: Sao Paulo). Model 2 additionally includes control variables for currently married (reference: not currently married), education level (reference: no education), and early-life health conditions: knee height, excellent health (reference: good/poor), good economic conditions (reference: average/poor), and never hungry before 15 years of age (reference: ever hungry). Missing values for knee height were input the gender-specific average value. Dummy indicators were added to indicate missingness of knee height information. OLS = ordinary least squares; NCDs = non-communicable diseases.
p < .1. **p < .05. ***p < .01.
With the exception of osteoporosis, all NCDs were statistically significantly associated with lower MMSE scores. When compared with individuals with no NCDs, and adjusted for all control variables, diseases in Group 1 (stroke and neuropsychiatric conditions) tended to have the highest association with decreased cognitive scores. Stroke was the condition with the greatest magnitude of association with MMSE scores, as it remained larger than one point difference in MMSE scores, on average, even when adjusted to all our control variables of interest (extended OLS estimates ± standard errors: females = −1.027 ± 0.314, p = .01; males = −1.504 ± 0.339, p < .0001, as compared with individuals with no NCDs). In addition, the association between stroke and MMSE scores was the second largest in our analysis, only behind the positive association between education levels and MMSE scores. Neuropsychiatric disorders also had large associations with low MMSE scores, especially among males, where it was larger than any other disease except for stroke (extended OLS estimates = females: −0.475 ± 0.169, p = .005; males = −0.826 ± 0.204, p < .0001, reference: no NCDs).
Diseases in Group 2 (diabetes, lung disease, hypertension, and heart disease) were also statistically significantly associated with lower cognitive scores among both males and females. These associations remained after controlling for the full set of covariates, and tended to be lower than that of diseases in Group 1. Heart disease was the exception, as in the fully adjusted models, its statistical significance was effaced among women, but accentuated among men.
Diseases in Group 3 (cancer, arthritis, and osteoporosis) tended to have the smallest associations with MMSE scores that also varied more extensively by gender. Cancer had similar magnitudes of association in both genders but achieved borderline statistical significance among females (extended OLS estimate = −0.458 ± 0.260, p = .079). Among males, there is no statistically significant association between MMSE scores and cancer (extended OLS estimate = −0.046 ± 0.302, p = .879). Arthritis was the opposite, reaching borderline statistical significance among males (extended OLS estimate = −0.258 ± 0.151, p = .090) but not among females (extended OLS estimate= −0.189 ± 0.157, p = .228).
Figure 4 graphically displays the OLS estimates using full model for the association between the various NCDs and cognitive ability, separately for males and females (coefficients are shown in Table 5, Model 2). Whereas there is some overlap of confidence intervals across the multiple diseases, a pattern where diseases in Group 1 have largest association, followed by diseases in Group 2 and diseases in Group 3 can be seen, especially among men. With the sole exception of cancer, the association of all other NCDs with cognitive scores was larger among men than among women.
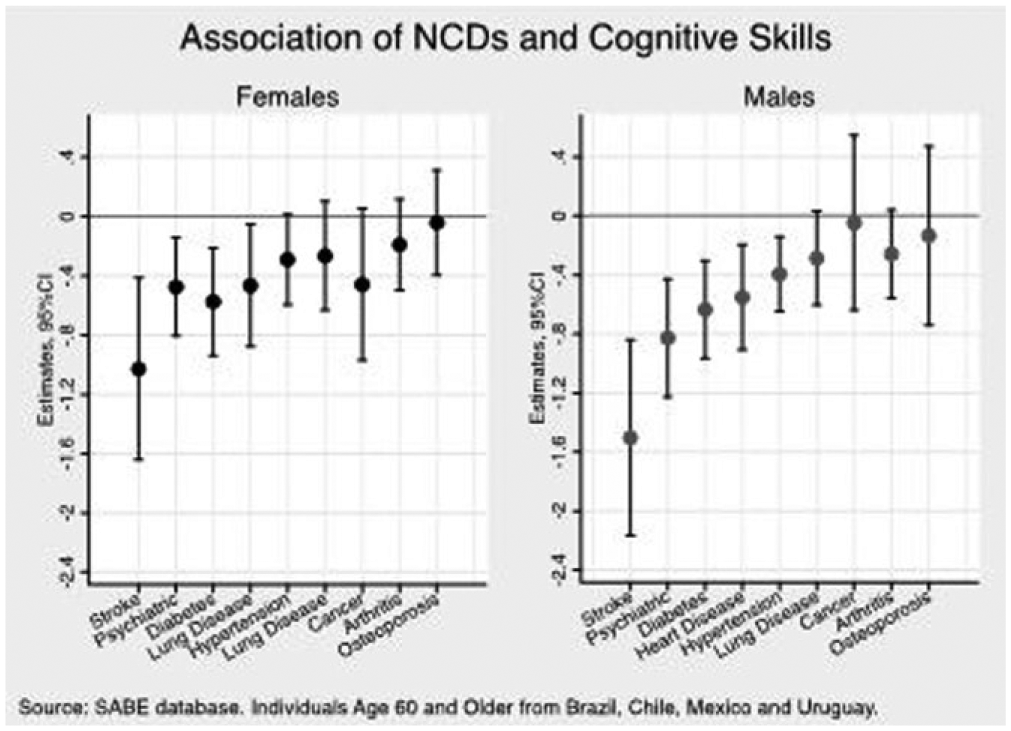
OLS estimates of type of NCD on cognitive skills in our sample of older adults from four Latin American countries (results from full Model 2, Table 5).
Links Between NCDs and Cognitive Impairment
Table 6 shows the results of linear probability models investigating the association between NCDs and cognitive impairment (MMSE score: 0-12). Reduced and extended analytical models were implemented using the number and the type of NCDs as the main independent variable, and using individuals with no NCDs as the reference group. Only the NCD-related coefficients are shown. The full set of results is available upon request.
Linear Probability Models Exploring The Association Between Number of NCDs and the Probability of Being Cognitively Impaired (MMSE: 0-12).

Source. SABE database. Pooled data of individuals aged 60 years and older from Brazil, Chile, Mexico, and Uruguay.
Note. Outcome: cognitive impairment (MMSE: 0-12). Reference: unimpaired (MMSE 13-19). Group 1: Diseases with potential direct effect on brain function. Group 2: Diseases with potential indirect effect on brain function through impaired systemic circulation, oxygenation, or metabolic homeostasis. Group 3: Diseases with unlikely direct or indirect effects on brain function. Reference group for all regression models: no chronic conditions. Sample sizes in each regression model correspond to individuals with complete information. Estimates presented as regression coefficients and robust standard errors in parentheses. Standard errors account for clustering at each survey site’s primary sampling units. Model 1 includes an intercept and controls for age, age squared / 100, and survey site (reference: Sao Paulo). Model 2 additionally includes control variables for being currently married (reference: not currently married), education level (reference: no education), life conditions before age 15 years: excellent health (reference: good/poor), good economic conditions (reference: average/poor) and never hungry (reference: ever hungry), knee height, and an indicator variable for missing knee height data. Missing values for knee height were input the gender-specific average. Individuals with missing values for other early-life conditions were excluded from the analysis. NCDs = non-communicable diseases; MMSE = Mini-Mental State Examination; OLS = ordinary least squares.
p < .1. **p < .05. ***p < .01.
Among females, having one NCD was associated with an average of 3.4% higher probability of having cognitive impairment as compared with those with no diseases, all other things being equal (extended model estimate: 0.034 ± 0.016, p = .038). Having two or more NCDs, however, was not statistically significantly associated with changes in the probability of being cognitively impaired.
Among males the relationships exhibited a dose-response pattern, where having one NCD was not statistically significantly associated with changes in the probability of being cognitively impaired, but having two or more NCDs was associated with an almost 5% higher probability of having cognitive impairment, on average, as compared with those with no diseases (estimate: 0.049 ± 0.011, p < .0001).
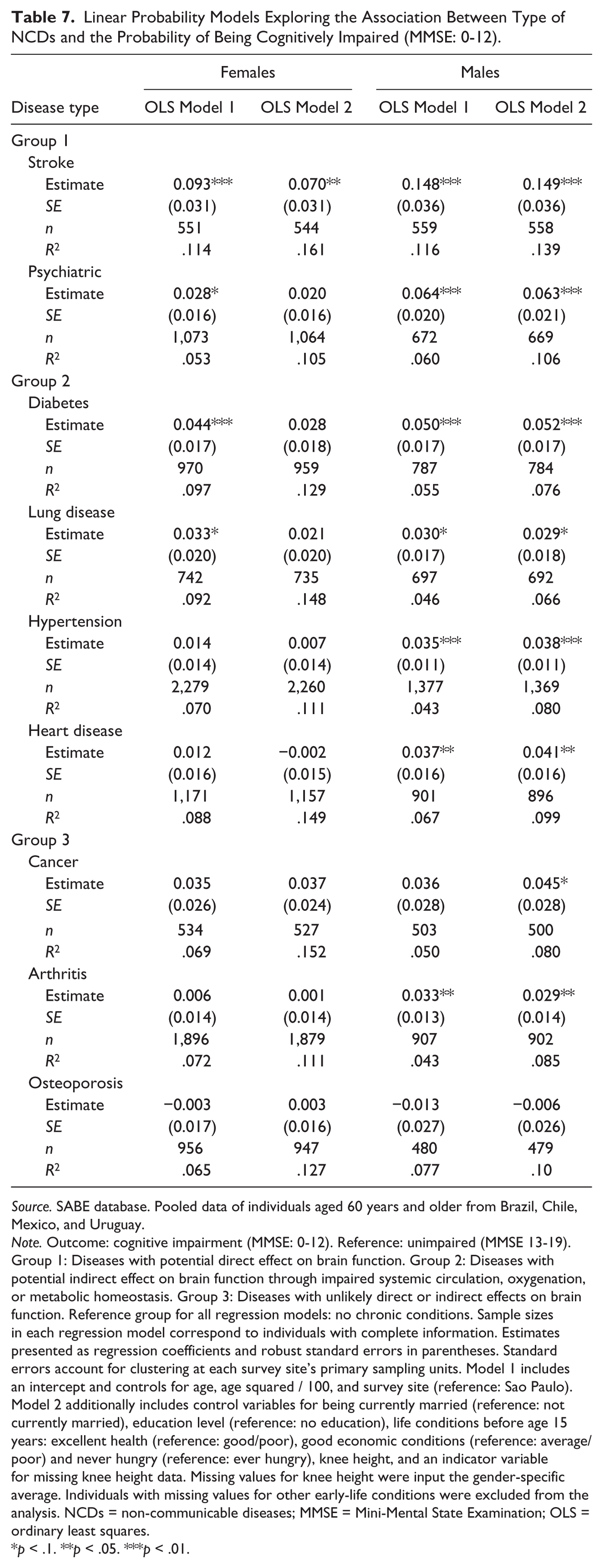
Stroke was the NCD with the largest magnitude of association among both genders, being associated with an average of 7% greater probability of cognitive impairment among females and 14.9% among males, as compared with individuals with no diseases (Table 7). Among females, none of the other NCDs had statistically significant associations with cognitive impairment. Among males, diseases in Group 1 (stroke and psychiatric disease) had the largest association, followed by diseases in Group 2 (hypertension, diabetes, heart disease, and lung disease) and diseases in Group 3 (cancer, arthritis and osteoporosis). Among males, all other NCDs but osteoporosis had positive and statistically significant associations with the probability of being cognitively impaired, varying from 2.9% (in the case of lung disease and arthritis) to 6.3% (psychiatric conditions) and 14.9% (stroke) higher probability of cognitive impairment.
Linear Probability Models Exploring the Association Between Type of NCDs and the Probability of Being Cognitively Impaired (MMSE: 0-12).
Source. SABE database. Pooled data of individuals aged 60 years and older from Brazil, Chile, Mexico, and Uruguay.
Note. Outcome: cognitive impairment (MMSE: 0-12). Reference: unimpaired (MMSE 13-19). Group 1: Diseases with potential direct effect on brain function. Group 2: Diseases with potential indirect effect on brain function through impaired systemic circulation, oxygenation, or metabolic homeostasis. Group 3: Diseases with unlikely direct or indirect effects on brain function. Reference group for all regression models: no chronic conditions. Sample sizes in each regression model correspond to individuals with complete information. Estimates presented as regression coefficients and robust standard errors in parentheses. Standard errors account for clustering at each survey site’s primary sampling units. Model 1 includes an intercept and controls for age, age squared / 100, and survey site (reference: Sao Paulo). Model 2 additionally includes control variables for being currently married (reference: not currently married), education level (reference: no education), life conditions before age 15 years: excellent health (reference: good/poor), good economic conditions (reference: average/poor) and never hungry (reference: ever hungry), knee height, and an indicator variable for missing knee height data. Missing values for knee height were input the gender-specific average. Individuals with missing values for other early-life conditions were excluded from the analysis. NCDs = non-communicable diseases; MMSE = Mini-Mental State Examination; OLS = ordinary least squares.
p < .1. **p < .05. ***p < .01.
Robustness Checks
Appendix A displays the results of the analytical models excluding stroke and psychiatric disease and redefining the number of NCDs exclusively in terms of diabetes, lung disease, hypertension, heart disease, cancer, arthritis, and osteoporosis. The magnitude of associations was generally reduced, but the redefined NCD categories yielded results qualitatively identical to those obtained in the main analysis. Among women having one NCD, but not two or more, was statistically significantly associated with lower cognitive scores as compared with those with no diseases. Among men, having one NCD was not significantly associated with cognitive scores, but having two or more was statistically significantly associated with lower cognitive scores as compared with those with no disease, all other things being equal.
Appendix B displays the results of non-parametric specifications on age. As found in previous models, having a NCD was associated with lower MMSE scores among females (extended OLS estimate ± standard error: = −0.365 ± 0.172, p = .034) but not among males (estimate: = −0.151 ± 0.143, p = .292). Having two or more NCDs was associated with statistically significantly lower MMSE scores in both genders (females= −0.313 ± 0.152, p = .40; Males = −0.544 ± 0.129, p < .0001). The results for each type of NCD from models with non-parametric specifications on age are comparable with those obtained from the reduced and extended OLS models and are also reported in Appendix B.
Appendix D displays the results of the quantile regressions. The negative association between NCDs and cognitive skills was larger among those in the bottom of the cognitive distribution for males, but higher for those at the top of the cognitive distribution for females. The results were statistically significant only for those with two or more NCDs. Full set of results are available from the authors upon request.
Appendix E displays the results of ordinal probit models. These results largely corroborated previous findings. Having one NCD was associated with larger probability of having severe cognitive impairment (extended model estimates: females: 0.0069 ± 0.0038, p = .065; males: 0.0040 ± 0.0023, p = .084) or moderate to mild cognitive impairment (females: 0.0258 ± 0.0145, p = .075; males: 0.197 ± 0.0113, p = .081), and with lower probabilities of having no cognitive impairment (females: −0.0327 ± 0.0181, p = .070; males: −0.0237 ± 0.0134, p = .077). Having two or more NCDs was statistically significantly associated with probability of cognitive impairment only among males (severe cognitive impairment: 0.0089 ± 0.0022, p < .0001; moderate to mild cognitive impairment: 0.0388 ± 0.0097, p < .0001), and lower probability of having no cognitive impairment (estimates: −0.0476 ± 0.0110, p < .0001).
In sum, the comprehensive sensitivity analysis affirmed the direction and size of the associations between NCDs and cognitive ability found in the main analytical models.
Discussion
In this study, we found that the negative association between NCDs and cognition varied significantly across genders. Among women, the relationship was similar at any level of NCDs: women with one or with two or more NCDs had statistically significant lower cognitive scores as compared with women without NCDs, all other things being equal. Among men, however, having only one NCD was not associated with significant differences in cognition, while having multiple NCDs was associated with a large and statistically significant decrease in cognitive scores that exceeded the differences found among women. The negative association between NCDs and cognition was comparable in magnitude with the positive association of being married among women. Among men, the negative association of having two or more NCDs was twice as large. Interestingly, the positive association between marriage and cognition was similar in magnitude across both gender groups.
At the margin, the presence of NCDs was associated with an increased probability of being cognitively impaired in the case of males, but not females. It is possible that, while females exhibit lower cognitive scores associated with the presence of NCDs, this association may not be large enough to result in clinically relevant impairment.
Our hypothesis that differences in physiopathological mechanisms might underlie the relationship between NCDs and cognitive scores did, in general, hold, in the sense that NCDs with direct impact on brain function (Group 1) tended to have greater effect than NCDs with potential indirect impact on brain function via imbalances in circulation and metabolism (Group 2), and these conditions, in turn, tended to have greater effects on cognitive scores than diseases without direct or indirect effect on brain function (Group 3). These results are of relevance for future inquiry, especially as they support a differential effect according to the degree of brain involvement. Also, the results indicate that even diseases with no direct or indirect brain involvement may still be associated with lower cognitive scores. However, there was some degree of heterogeneity among diseases of a same group, indicating that the biological mechanism of the disease may explain some but not the full association between NCDs and cognition in later life. Further research is needed to clarify the extent to which NCDs may affect cognition through pathways such as medication, stress, depression, resource depletion, and intensive management. Stroke was the NCD with the greatest association with lower cognitive scores, but repeating the analysis without cases of stroke and psychiatric conditions did not change the results. A series of robustness checks supported the findings.
Our findings were in line with results previously reported in Latin America and the Caribbean and elsewhere (Lei et al., 2012; Maurer, 2011; Nguyen et al., 2008), in that, on average, cognitive scores tended to be lower among women as compared with men, and women also tended to have lower levels of schooling, and more NCDs. However, women with greater schooling in our sample had, on average, greater cognitive scores than men, and the association between number of NCDs and cognitive scores was stronger at the bottom of the cognitive distribution for men but at the top of the cognitive distribution for women.
Another limitation of the study was the use of cross-sectional data, which did not allow for establishing the causal direction of the observed associations. Changes within individuals can only be measured by using longitudinal data. However, maturation effects (environmental changes, adaptation over time, learning with the practice of repeated cognitive testing) may be difficult to measure and control in longitudinal studies. Understanding cognitive decline requires that both types of studies complement each other. The use of cross-sectional data allows the identification of differences in cognition between individuals, as it assumes that the experience of two individuals of different ages was the same when they had the same age, as long as relevant covariates are controlled for. The richness of the SABE dataset allowed this analysis to control for all the correlates of cognitive aging that have been previously used in the literature. Nevertheless, important correlations between unobservable factors that may affect both aging and health, as well as cognitive ability may remain (Stowasser et al., 2014). Even though the present study was not able to explore the causal effect of NCDs on cognitive abilities, the proposed approach may help lay out the foundation for future research aiming to assess causality in the effect of NCDs on cognitive skills.
By combining data from individuals from four different countries, the generalizability of the results was expanded and the replication of the methodology in other settings was greatly facilitated. The use of data with comprehensive life-course information from four different countries helped reduce the limitations of cross-sectional data. Differences in the effect of characteristics across the life span may play a role in variations of cognition, especially in the differences observed across genders. In the present study, early-life characteristics such as knee height and excellent health before age 15 years were associated with higher cognitive skills among females, but not among males. These results were similar to previous analyses of the same datasets (Maurer, 2010). Differently from previous analyses, however, economic circumstances and nutritional scarcity before age 15 years were not significantly associated with cognitive abilities in later life for either gender. The associations previously found might have been effaced in light of the additional variables included in our study, namely, the presence of NCDs and marital status.
The reasons underlying the differences in the association between NCDs and cognition across genders are not completely understood. Unobserved differences in factors across the life span, such as nutritional, educational, and occupational opportunities, behaviors, and attitudes could help explain this finding. Or, there may be differences across genders in how these factors affect cognition. Unobserved differences in the severity of illness, management of the conditions, quality of care, and frequency and type of comorbidities may also play a role.
It is also possible that some gender differences could be explained by better care-seeking behavior, because the interview asked specifically for diagnoses given by a physician or nurse, and women are more likely than men to seek professional and preventive care services (Miilunpalo, Vuori, Oja, Pasanen, & Urponen, 1997). Older women tend to report a larger number of chronic conditions than men in self-reported questionnaires (Miilunpalo et al., 1997). An alternative explanation would be that individuals show persistent heterogeneity in past cognitive skills either between or within each gender, and this affects their production of health over their life span. The general heterogeneity observed in the coefficients also suggests that the endogeneity problems may be different for males and females.
Part of the gender differences may also be due to cohort effect—as women live longer, they represent a larger proportion of older cohort—not age, and the corresponding availability of technologies in these cohorts for the treatment and management of chronic conditions. Two possible channels may explain these findings. First, fertility declines in Latin America (particularly in Brazil and Mexico) occurred among the younger cohorts included in the analysis (those born around 1940 who were aged 60 in the year 2000). So these cohorts had, on average, fewer children, whereas the children they had more likely occurred in a hospital (rather than with a midwife). Thus, younger cohorts could have reached older age in better health than their older-cohort counterparts. Second, the availability of medical technology for the treatment and management of chronic diseases has only been available in Latin America in the last two decades or so. This means that older cohorts were unlikely to benefit from these medical innovations (e.g., anti-hypertensive medication, lipid-lowering drugs, etc). 1
The assessment of cognitive ability was also one of the study’s limitations. In general, cognitive ability can be understood as a combination of two main systems: fluid and crystallized intelligence. Fluid intelligence is characterized by the capacity to solve new problems, whereas crystallized intelligence reflects accumulated knowledge (Cattell, 1967; McArdle et al., 2002). Measures of fluid intelligence decline fast with age, whereas crystallized intelligence tends to accumulate from early life and decline after middle age (Park & Gutchess, 2006). The test utilized to measure cognitive ability in this study, the MMSE, is primarily a test of crystallized intelligence, and is largely dependent on verbal skills (McArdle, 2011). Therefore, fluid intelligence and some aspects of crystallized intelligence were not assessed. Nevertheless, our findings have a large clinical relevance because changes in cognitive scores as measured by the MMSE are correlated with clinical and functional outcomes as well as health prognosis (Fan, Batmanghelich, Clark, & Davatzikos, 2008; Fang et al., 2010; McArdle et al., 2009; Royall, Palmer, Chiodo, & Polk, 2004). The distribution of scores in the MMSE tended to be left-skewed, with most of the scores concentrating in the upper limit. This may also hinder the test’s ability to differentiate across individuals with unimpaired cognition. Yet, we implemented analytical models that account for the right censoring of the data and that did not significantly change our results, suggesting that right censoring did not affect our analysis in a significant way.
Even though our study did not provide causal effect parameters, the replication of our approach with data from four different settings provides further evidence that lead us to propose general principles for policy implications.
First, investigations of the effect of policies and interventions aimed at reducing the burden from NCDs should include an analysis of cognitive measurements, because these policies may yield benefits that extend beyond physical health outcomes. Because better cognitive skills are associated with better decision making, better self-management, and better social and financial outcomes in older ages (Agarwal, Gabaix, Driscoll, & Laibson, 2009; Smith et al., 2010), policies to reduce the burden from NCDs might influence cognitive abilities and potentially its effects on quality of life and independency during the senior years. The potential expanded effects of NCD treatments mediated by cognition should be incorporated in cost/benefit analyses to justify public investment in programs to reduce the burden from NCDs.
Second, the effectiveness of policies aimed at reducing the negative effect of cognitive decline in later life should be investigated among individuals with NCDs, and potentially target these groups specifically (Agarwal et al., 2009). The marginal returns from policies to prevent cognitive decline could be enhanced if they were implemented in aging individuals before the development of NCDs, as the negative impact from multiple established comorbidities may be associated with a cognitive decline that may be too steep to be reversed.
Third, cognitive impairment should be taken into consideration when treating patients with conditions that require complex protocols. In these cases, a negative feedback loop may arise because low cognitive skills may lead to poor self-management of NCDs (Trujillo & Fleisher, 2013).
Finally, the findings indicate that further research aimed at clarifying or modifying the relationship between NCDs and cognition should consider each gender and each disease groups separately.
Footnotes
Appendix
Cognitive Scores by Number and Type of NCDs in the Overall Sample.
| Total cognition (MMSE) | |||
|---|---|---|---|
| M (SD) | n | p value* | |
| Number of diseases | |||
| No diseases | 16.73 (2.43) | 798 | <.001 |
| One | 16.32 (2.94) | 1,319 | |
| Two or more | 16.00 (2.91) | 3,697 | |
| Disease type | |||
| Stroke | 15.03 (3.88) | 312 | p < .001 |
| Psychiatric | 15.98 (2.94) | 947 | p < .001 |
| Diabetes | 15.75 (2.95) | 959 | p < .001 |
| Hypertension | 16.13 (2.82) | 2,858 | p < .001 |
| Lung disease | 15.85 (2.91) | 641 | p < .001 |
| Heart disease | 16.10 (2.93) | 1,274 | p < .001 |
| Cancer | 16.35 (3.10) | 239 | p = .0505 |
| Arthritis | 16.26 (2.75) | 2,005 | p < .001 |
| Osteoporosis | 16.41 (2.77) | 638 | p = .0228 |
Source. SABE database. Pooled data of individuals aged 60 years and older from Brazil, Chile, Mexico, and Uruguay.
Note. Total cognition measured by the modified MMSE. Range: 0-19. Larger scores indicate better cognition. Scores presented as means and standard deviations. n: number of individuals with information. p values for number of diseases reflect the comparison across the three categories. p values for specific diseases reflect the comparison between individuals with the disease versus individuals with no chronic conditions. NCDs = non-communicable diseases; MMSE = Mini-Mental State Examination.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.