
Abstract
It is estimated that 8.5% of the estimated 43.2 million older adults (aged ≥65 years) in the United States smoke cigarettes and are at risk for various smoking-related health problems (Jamal et al., 2015; U.S. Census Bureau, 2016). Older smokers are a critical group for intervention because they are at heightened risk for cardiovascular disease (CVD), respiratory conditions, cancer, and other smoking-related conditions, such as visual impairment and other disabilities (Burns, 2000).
Fortunately, substantial health benefits from quitting smoking, such as CVD risk reduction, are realized within a few years. Heart attack and stroke risk is dramatically lowered within 1 to 5 years after cessation (Kawachi et al., 1993), even in older smokers (Burns, 2000; Hermanson, Omenn, Kronmal, Gersh, & Participants in the Coronary Artery Surgery Study, 1988). Smoking cessation also attenuates the rate of decline in lung function among people with smoking-related pulmonary dysfunction, such as chronic obstructive pulmonary disease (COPD; Anthonisen et al., 1994). Yet despite clear health benefits from smoking cessation in older adults, many do not receive evidence-based cessation treatments (Jonk et al., 2005; Thorndike, Rigotti, Stafford, & Singer, 1998). Older adults also are underrepresented in smoking cessation trials, and few intervention approaches have been tailored to them (Zbikowski, Magnusson, Pockey, Tindle, & Weaver, 2012).
Although there are fewer smokers among women aged 65 years and older compared with all women (7.5% vs. 14.8%, respectively), since 2005 there has been no significant reduction in smoking among women aged above 65 years, unlike the overall prevalence of smoking among adults (19.8% decline) and women, specifically (18.2% decline) (Jamal et al., 2015). Older women outnumber older men (23.4 million vs. 17.9 million, respectively), and the population of U.S. adults aged 65 years and above increased by 21% from 2002 to 2012, and is projected to increase to 79.7 million by 2040 (Administration on Aging, Administration for Community Living, U.S. Department of Health and Human Services, 2012). In addition, older women face sociodemographic vulnerabilities that could make it more difficult for them to quit smoking. For example, their average income of US$15,362 is about half that of older men, and almost half of women aged above 75 years live alone (Administration on Aging, Administration for Community Living, U.S. Department of Health and Human Services, 2012). To our knowledge, no prior studies have specifically queried older female smokers about their smoking cessation beliefs and preferences for treatment. This knowledge gap has hampered dissemination of proven interventions and/or development of tailored approaches to effectively address smoking cessation in this vulnerable subpopulation. Review of data from intervention studies in older smokers (>50 years) suggest that quit rates in this group are consistent with those of the general smoking population when effective interventions are provided (Zbikowski et al., 2012). However, barriers that hinder treatment in older smokers have not been well studied. To address these gaps, it is crucial to understand potential barriers to engaging older female smokers in cessation treatment and research.
The objective of this study was to inform development of tailored smoking cessation interventions by (a) characterizing older women smokers and those who quit smoking during their enrollment in the Women’s Health Initiative (WHI) study (Anderson et al., 2003), and (b) determining use and interest in cessation treatments, as well as interest in smoking cessation trials. As one of the largest cohorts of older women in the United States, the WHI offers a unique opportunity to identify and characterize many current and former female smokers aged 65 years and older and to assess the feasibility of recruiting older smokers into potential cessation trials conducted by the WHI and other groups. We also sought to preliminarily explore differences among female smokers of various racial/ethnic groups, with the future goal of designing culturally appropriate intervention strategies.
Method
Sample
Eligible women included those WHI participants who (a) were enrolled in WHI Extension 2 (Espeland et al., 2013) (beginning in 2010) and were contacted by the WHI Southeast Regional Center (SERC); (b) were English-speaking; and (c) reported currently smoking at their last available WHI assessment (i.e., during the enrollment and follow-up period from 1993 to 2005). All study procedures were approved by the WHI Ancillary Study Committee and Observational and Safety Monitory Board (OSMB) and the Wake Forest School of Medicine Institutional Review Board. WHI SERC staff mailed women an initial packet including an informational letter and the questionnaire; a second survey packet was mailed to nonrespondents approximately 4 weeks later. SERC staff attempted to contact nonrespondents by telephone, and called women who requested telephone rather than paper administration of general WHI assessments. Data were collected between August and November 2012.
Measures
Women were asked standardized questions from the Behavioral Risk Factor Surveillance System (Centers for Disease Control and Prevention [CDC], n.d.-a) to assess current smoking status (every day, some days, or not at all), average amount smoked in the last 30 days, and use of menthol cigarettes. We also assessed use of five quit aids (prescription medications, quit line, counseling, nicotine replacement products, and speaking with a doctor), including whether they were ever used and whether they were used during the most recent quit attempt.
Current smokers
Level of nicotine addiction was assessed using the time-to-first-cigarette question from the Fagerström (2003) Test of Nicotine Addiction. Motivation for quitting was assessed using two questions: (a) how concerned a participant was about the effects of cigarette smoking on current health (not, slightly, somewhat, or very concerned); and (b) intention to quit smoking, using the standard stages of change question (Velicer et al., 1995). Nine barriers to quitting smoking were assessed using questions adapted from the CDC Pregnancy Risk Assessment Monitoring Study (PRAMS) (CDC, n.d.-b), with three items added to address concerns that may be relevant to older women (e.g., lack of alternate pleasurable activities, problems with memory and thinking, and lack of motivation to quit). We also asked questions to guide future interventional study design, including likelihood of participating in a smoking cessation research study during the next year and preference for types of smoking cessation treatment (e.g., phone counseling, mail, computer/Internet, and medications).
Former smokers
Former smokers completed many of the same questions, but were asked to reflect back on the 12 months before they quit smoking cigarettes (following the format of the Tobacco Use Supplement to the Current Population Survey for former smokers) (National Cancer Institute, n.d.). They also rated the importance of 7 reasons for quitting smoking during their successful quit attempt: for example, cost, prohibitions in buildings, future health concern, present health concern, and effect on others, pressure from family and friends, and setting a good example for children/grandchildren.
Demographic variables
Date of birth, race/ethnicity, educational attainment, and marital status were collected at WHI baseline, and living arrangement (live alone or with someone else) was updated based on the last available assessment before the survey.
Health status variables
Self-reported health was assessed using a single item from the Medical Outcomes Study (categorized as excellent/very good/good vs. fair/poor) collected at the last WHI assessment available before the survey. History of CVD, cancer, hypertension, diabetes, and hypercholesterolemia was based on self-report and/or clinical adjudication during the WHI study from baseline through 2009. Alcohol use (categorized as none, <1 drink per day, or 1 or more drinks per day) and overweight/obese body mass index (BMI; defined as ≥ 25 kg/m2) were assessed at the last self-report available before the survey.
Psychosocial variables
Measures of depressive symptoms, stressful life events, social strain, social support, optimism/pessimism, cynical hostility, and health-related quality of life were expected to be related to smoking status. Depressive symptoms over the past week were measured with six items from the Centers for Epidemiological Studies Depression (CES-D) scale and two items from the Diagnostic Interview Schedule (DIS) (Radloff, 1977; Robins, Helzer, Croughan, & Ratcliff, 1981). Responses were scored according to the Burnam algorithm which computes a depression score from 0 to 1, with scores greater than 0.06 indicating greater probability of depressive symptoms (Burnam, Wells, Leake, & Landsverk, 1988). We dichotomized scores at this threshold and defined a group with evidence of depressive symptoms (score >0.06) and those without (score ≤0.06). The Burnam algorithm and dichotomization have been widely used within WHI. Optimism (positive future expectation) and pessimism (negative future expectation) are considered to be trait-like in the absence of intervention, and were associated with smoking status at baseline in the WHI (Tindle et al., 2009). Optimistic and pessimistic attitudes were measured using the Life Orientation Test–Revised (LOT-R; Scheier, Carver, & Bridges, 1994) and collected at the last available assessment before the survey. Scores range from 6 to 30, with higher scores indicating greater optimism and lower scores indicating greater pessimism.
Statistical Analysis
Results were summarized using means, standard deviations, interquartile ranges, counts, and percentages. Kruskal–Wallis, Pearson’s chi-square, and two-sample t tests were used for comparison across groups. Multiple logistic regression modeling and backward elimination were used to determine predictors of current smoking. Potential covariates were screened based on bivariate association with current smoking status; those with p < .20 were entered into the initial regression model. Covariates were then excluded using p < .10 to remain in the model. Exceptions were age, race/ethnicity, and education, which were included as covariates regardless of statistical significance for the screening and final model. Any p values less than .05 were considered statistically significant. In exploratory univariate analyses, we compared non-Hispanic White versus non-Hispanic African American current smokers; small samples of other minorities precluded comparisons. All analyses were performed using SAS Version 9.3 (SAS Institute, Cary, North Carolina).
Results
Sample Characteristics
We contacted 671 potentially eligible women by telephone (n = 61) or mail (n = 610), based on preferred modality; 10 women were deceased and five women identified themselves as lifetime never-smokers and were ineligible. Of the 656 eligible women, 411 completed the survey by mail or telephone (63% response rate). The mean age of respondents was 75.1 years. Restricting to surveys that indicated current smoking status, the analytic sample (n = 409) was comprised of 227 current and 182 former smokers. The majority were non-Hispanic White (81.7%), and about 80% reported attending at least some college. Respondents and nonrespondents varied significantly (p = .04) in educational level, with a greater proportion of nonrespondents reporting less than a high school diploma (26.1% vs. 18.3% for respondents) and a smaller proportion reporting some college (41.1% vs. 49.4%, respectively). There were no significant differences for age, race/ethnicity, and marital status. About 44% of ever smokers (i.e., current and former) reported that they currently or used to consume 15 or more cigarettes per day.
Comparison of Current and Former Smokers
Current and former smokers did not differ significantly on any sociodemographic or psychosocial characteristics (Table 1). They also reported similar health status, including self-reported health, history of cancer and CVD, and cardiovascular risk factors, except for BMI; current smokers were significantly more likely to be overweight or obese than former smokers. Current smokers were also more likely than former smokers (reported from past) to report that they smoked within 30 min of waking, and they endorsed more barriers to quitting, including cost of medicines/products/classes, loss of a way to handle stress, worsening anxiety and boredom, memory problems, and lack of motivation (Table 2). Former smokers were less likely to have used quit aids during their last quit attempt (possibly reflecting less of a need to use these aids to successfully quit smoking) and to report that they did not have a usual type of cigarette.
Sociodemographic and Health Characteristics of Current and Former Older Female Smokers Enrolled in the Women’s Health Initiative.
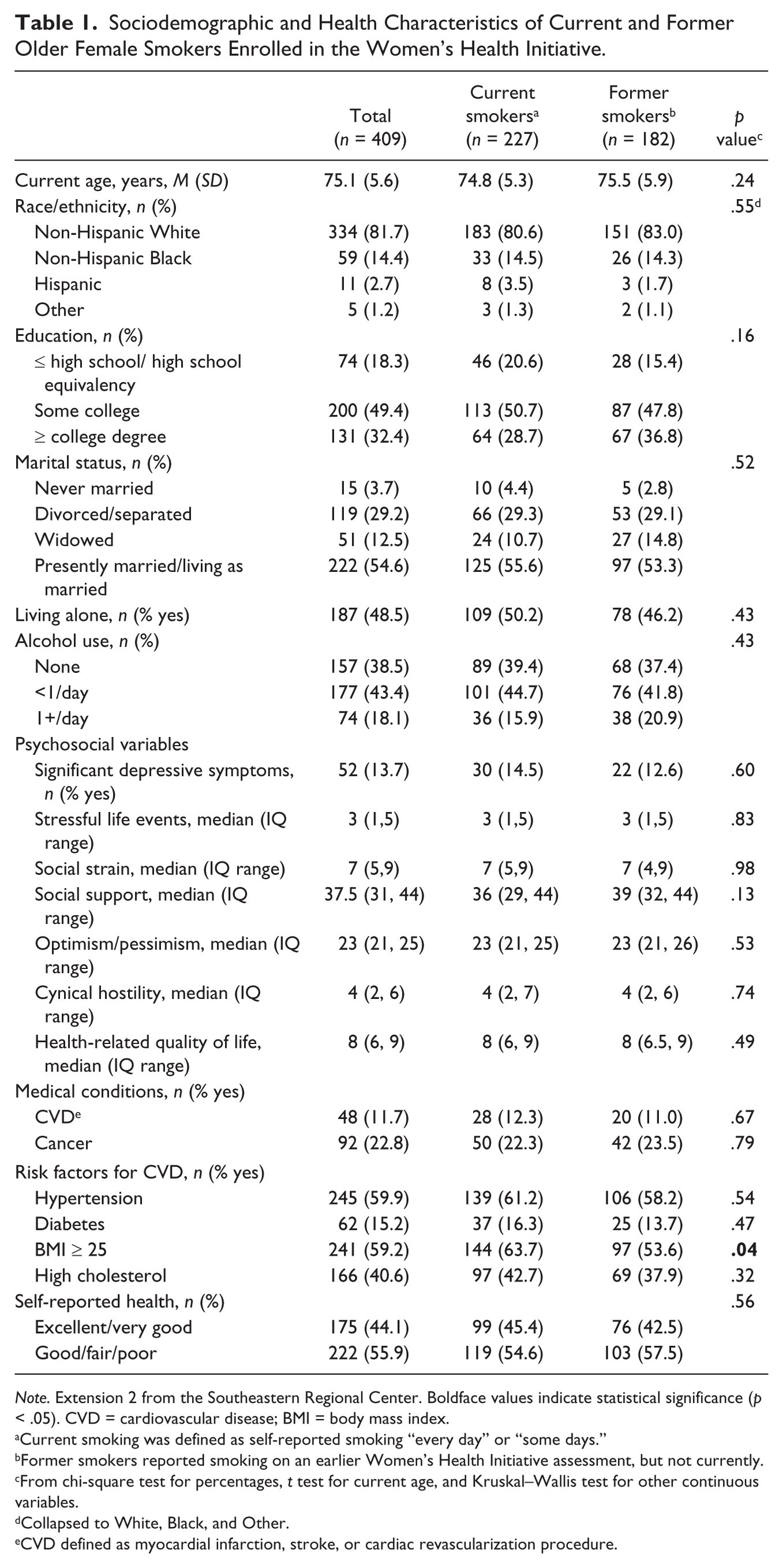
Note. Extension 2 from the Southeastern Regional Center. Boldface values indicate statistical significance (p < .05). CVD = cardiovascular disease; BMI = body mass index.
Current smoking was defined as self-reported smoking “every day” or “some days.”
Former smokers reported smoking on an earlier Women’s Health Initiative assessment, but not currently.
From chi-square test for percentages, t test for current age, and Kruskal–Wallis test for other continuous variables.
Collapsed to White, Black, and Other.
CVD defined as myocardial infarction, stroke, or cardiac revascularization procedure.
Smoking Characteristics of Older Current and Former Female Smokers Enrolled in the Women’s Health Initiative.
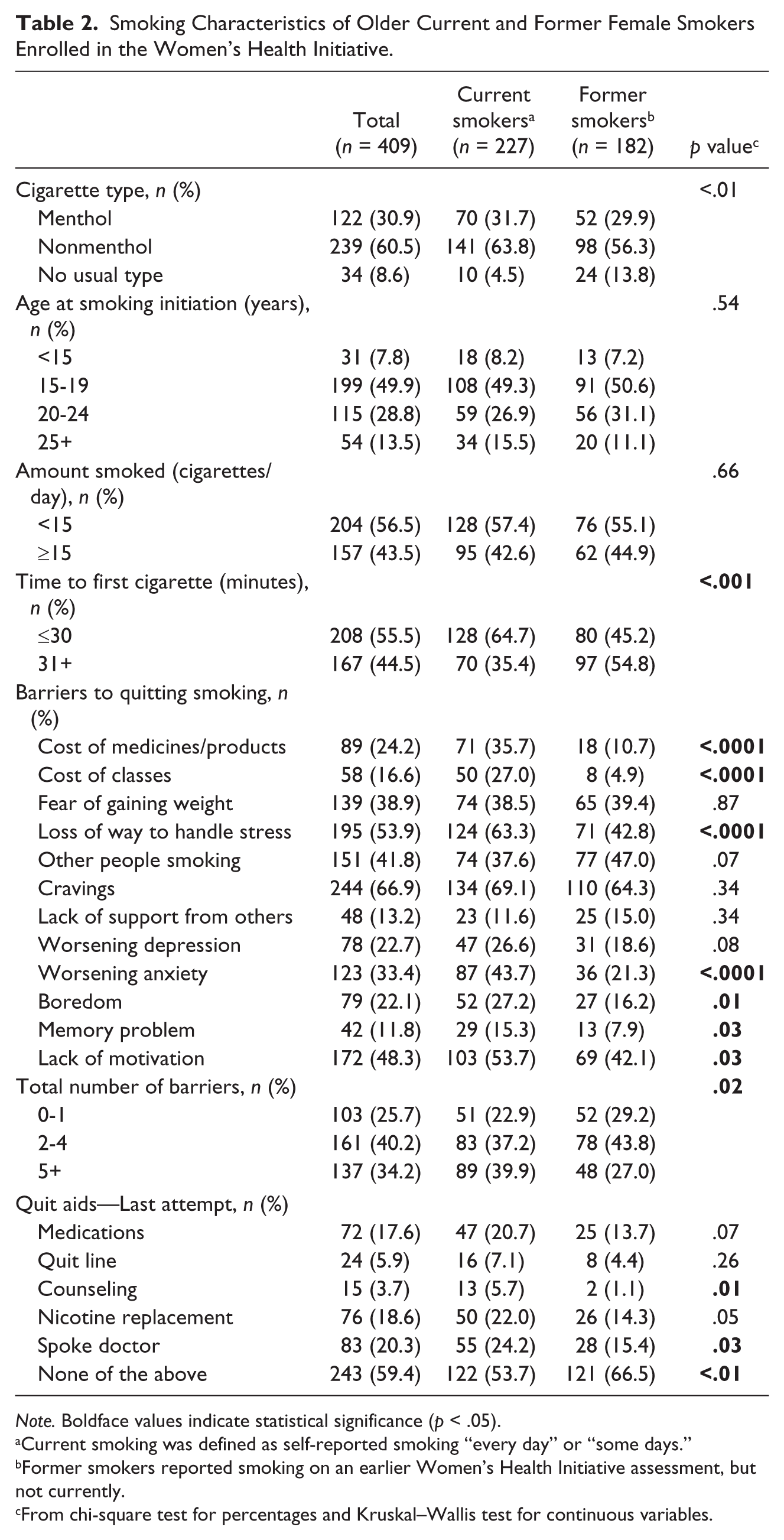
Note. Boldface values indicate statistical significance (p < .05).
Current smoking was defined as self-reported smoking “every day” or “some days.”
Former smokers reported smoking on an earlier Women’s Health Initiative assessment, but not currently.
From chi-square test for percentages and Kruskal–Wallis test for continuous variables.
In multivariable logistic regression models predicting the odds of being a current (vs. former) smoker, factors associated with lower odds of current smoking were having no regular type of cigarette (adjusted odds ratio [AOR] = 0.29, 95% confidence interval [CI] = [0.10, 0.88]) and endorsing other people smoking as a barrier to quitting (AOR = 0.36, 95% CI = [0.20, 0.66]). Factors associated with higher odds of current smoking were using nicotine replacement products during the last quit attempt (AOR = 2.09, 95% CI = [1.04, 4.21]) and endorsing cost of medicines/products as a barrier to quitting (AOR = 3.96, 95% CI = [1.86, 8.42]).
Past Cessation Treatment, Current Interest in Quitting, and Future Interest in Cessation Treatment
On average, current smokers reported that 3.0 years had elapsed since their last serious quit attempt, with 61% reported making a quit attempt in the past year. Less than half of the current smokers reported ever using any of the five different quit aids (Figure 1), while 36.6% reported that they had never used any quit aids. Just over a quarter of current smokers (27.1%) resided with another smoker, and most were concerned about the health effects of smoking (35.3% “very” and 36.7% “somewhat”). Regarding stage of change, 26.6% reported that they intended to quit smoking in the next 30 days, with another 30.9% reporting intention to quit within the next 6 months. Approximately 30% of the women reported no intention to quit smoking (29.8%). Regarding quit aids, women were most interested in cessation medications on a future attempt (Figure 1); approximately half also were interested in in-person classes, mailed materials, and phone counseling. Most reported that they were at least somewhat interested in joining a cessation study (67.5%).
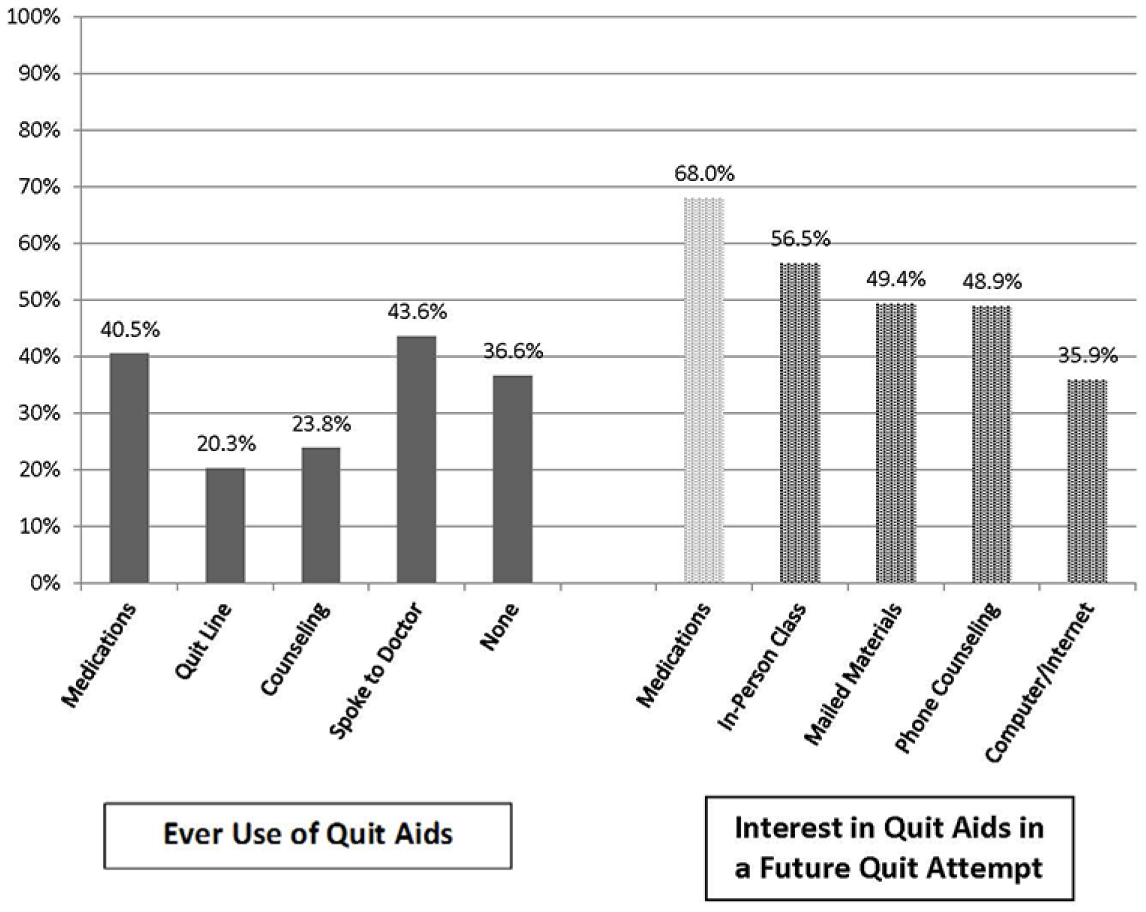
Ever use of cessation aids and interest (yes or maybe) in cessation aids among older female smokers enrolled in the Women’s Health Initiative (n = 227).
Differences Among Current Smokers by Race/Ethnicity
We preliminarily explored differences among the non-Hispanic White (n = 183) and non-Hispanic African American (n = 33) current smokers. There were not enough Hispanic smokers (n = 8) for formal statistical comparisons; descriptive statistics are reported in Supplementary Table 1. African American smokers were significantly more likely than White smokers to report smoking menthol cigarettes (66.7% vs. 23.7%, respectively); African American smokers also were more likely to smoke less than 15 cigarettes per day compared with White smokers and also were more likely to report waiting more than 30 min before their first cigarette of the day.
There were no significant differences between White and African Americans in use of quit aids ever or during the last quit attempts. Barriers to quitting were also similar; African American smokers were significantly more likely than White smokers to report boredom as a quit barrier. African American smokers were also more likely than White smokers to report high levels of concern about the health effects of smoking and risk factors for CVD. Three quarters of African American smokers reported their health as less than “very good,” compared with 42.3% of White smokers. African American smokers were more likely to express interest in joining a cessation study (83.3% vs. 64.5% of White and 27.1% of Hispanic smokers); a larger proportion of Hispanic smokers (42.9%) reported uncertainty about likelihood to join a cessation study. More African Americans reported interest in almost all the cessation treatments.
Discussion
In this cohort of older female smokers, just under one third reported an intention to quit in the next 30 days. This proportion is similar to low-income southern smokers in one recent study (Tseng et al., 2014), but substantially higher than U.S. and European population surveys (Thyrian et al., 2008; Wewers, Stillman, Hartman, & Shopland, 2003). More than 60% of respondents made a quit attempt in the last year but less than half used evidence-based quit aids, underscoring the profound undertreatment of smoking in this population. This is a critical shortcoming considering that combined medication and counseling can result in long term quit rates that are double or even triple those of unsupported quit attempts (Fiore et al., 2008). Because only about 24% of smokers reported speaking with a doctor during their last quit attempt, it is unclear whether providers fail to recommend or prescribe pharmacotherapy for older female smokers, or if other barriers prevent the use of such quit aids. Our results are consistent with studies showing under use of evidence-based cessation aids among female smokers (Sherman, Fu, Joseph, Lanto, & Yano, 2005). Collectively, these findings suggest that older female smokers are motivated, but may need extra support to make a successful quit attempt that is fully supported by proven therapies. Additional barriers that women report to quitting smoking, including difficulties with stress management and cravings, are also amenable to existing evidence-based therapies. Successful interventions also may need to address cost barriers to pharmacological cessation aids and counseling to address withdrawal symptoms, mood, weight gain, and motivation concerns common in female smokers (Allen, Oncken, & Hatsukami, 2014). Unlike prior studies of WHI participants, we did not observe a link between depressive symptoms and smoking cessation (Holahan et al., 2011), potentially because of the restriction of our sample to women who persisted in smoking for several years after WHI study entry.
Exploratory analyses focused on differences by race/ethnicity suggest that undertreatment of tobacco addiction is similar across racial and ethnic groups. African American smokers expressed a high level of interest in cessation treatment and joining a cessation study. Because African American smokers also experience poorer health and express more concern about the health effects of smoking, interventions and or clinical trials offered in the context of other health concerns (e.g., cardiovascular risk reduction) may be particularly appealing to older female African Americans.
Among older women, current smokers were more likely to be overweight and obese. Although smokers are generally thinner than nonsmokers (Albanes, Jones, Micozzi, & Mattson, 1987), this is not uniformly true. In one large study of more than 40,000 Scottish adults, smokers with a history of 20 or more pack-years were over 50% more likely than never-smokers to be overweight, and 25% more likely to be obese, even after adjusting for age (Mackay, Gray, & Pell, 2013). These findings perhaps reflect the comorbidity of poor health behaviors in certain populations (Chiolero, Faeh, Paccaud, & Cornuz, 2008). Cessation interventions that also limit weight gain would be particularly beneficial for older women, given data suggesting that substantial cessation-related weight gain may limit cardiovascular benefits of cessation (Allen et al., 2014).
Limitations
This study, one of the largest studies of older female smokers, capitalized on a large cohort of women followed for many years. Although the response to our survey was good, it was not as high as the response to annual WHI data collection mailings (generally 87%-92%). This discrepancy may reflect the more vulnerable population of current and former smokers that we targeted as compared with the larger WHI population. The overall WHI study was designed to be broadly representative of U.S. women (Hays et al., 2003), but as participants in an ongoing women’s health study, the sample of older female smokers in our study may not reflect the overall population of older female smokers in the United States. Compared with the baseline sample of smokers at entry in the overall WHI observational study (Holahan et al., 2011), our sample of current smokers contained roughly the same proportion of racial/ethnic minorities (80.6% White in current study +vs. 79.7% White in overall WHI observational study), more light smokers (<15 cigarettes per day: 57.4% vs. 52.9%), and a lower proportion with significant depressive symptoms (14.5% vs. 20.3%) which may be reflective of time trends or regional variation. We also could not confirm current smoking status via biochemical methods, although self-report is uniformly used to ascertain smoking status in large surveys. In addition, former smokers’ reports of smoking variables were retrospective, and thus possibly more likely to be influenced by recall bias. The small sample size for some racial/ethnic groups did not permit meaningful statistical comparisons among them; interesting exploratory trends emerged for the somewhat larger sample of African American female smokers, but should be interpreted with caution.
Conclusion
Interventions for smoking cessation are likely to be well received and feasible in older women, but to date, very few smoking cessation interventions have been designed specifically for them (Zbikowski et al., 2012). Existing evidence-based treatment strategies are clearly underused by these women, and interventions are critically needed to promote engagement of older female smokers in cessation attempts, support their specific vulnerabilities, and encourage their use of proven quit aids. Future studies designed to address tailoring and dissemination of effective smoking cessation aids among underrepresented older female smokers are needed.
Footnotes
Authors’ Note
Work on this article was performed while Kathryn Josephs was at the Wake Forest School of Medicine and Dr. Tindle was at the University of Pittsburgh. The WHI program is supported by contracts from the National Heart, Lung and Blood Institute, NIH. The authors thank the WHI investigators and staff for their dedication, and the study participants for making the program possible. A listing of WHI investigators can be found at ![]() .
.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Financial support provided by the Women’s Health Initiative Extension 2010-2015: The Southeast Regional Center (SERC) pilot grants program. The Women’s Health Initiative (WHI) program is funded by the National Heart, Lung and Blood Institute at the National Institutes of Health, U.S. Department of Health and Human Services (Contracts HHSN268201100046C, HHSN268201100001C, HHSN268201100002C, HHSN268201100003C, HHSN268201100004C, and HHSN271201100004C).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.