
Abstract
Introduction
The 2012 U.S. Census Bureau estimates that 53 million Hispanics/Latinos live in the United States, accounting for 16.9% of the U.S. total population. Hispanics/Latinos are predicted to comprise nearly 29% by 2050 (Ennis, Ríos-Vargas, & Albert, 2011; Ortman & Guarneri, 2009). Hispanics/Latinos will contribute to the growing older adult population in the United States (aged 65 years and older) (Federal Interagency Forum on Aging-Related Statistics, 2010). The U.S. Census Bureau expects that the older population in the United States will experience considerable growth in the next four decades, and that the proportion of older adults who are Hispanic/Latino will increase rapidly over the next four decades, increasing from 7.3% in 2012 to a projected 18.4% by 2050 (Ortman, Velkoff, & Hogan, 2014). The dramatic increase in the Hispanic/Latino population, particularly among older Hispanic/Latino adults, suggests an urgent need to address their mental and physical health needs and associated health disparities. Previous studies show that Hispanics/Latinos experience racial/ethnic health disparities across numerous emotional and physical metrics (Sadule-Rios, 2012), are more prone to experience racism and acculturative stress (Lara, Gamboa, Kahramanian, Morales, & Bautista, 2005), and often display lower socioeconomic status (SES) and educational attainment (Rodriguez-Galan & Falcón, 2009), all of which are risk factors leading to chronic stress and symptoms of depression.
A meta-analysis examining rates of depression among Hispanics/Latinos found that they experience significantly higher levels of depressive symptoms compared with non-Hispanic White peers (Menselson, Rehkopf, & Kubzansky, 2008); depression is documented at 11.4% for older Hispanic/Latino adults compared with 6.8% in Whites (Strine et al., 2008). This holds true across the life span into older age (González, Haan, & Hinton, 2001; Yuri, Chiriboga, Giyeon, & Phillips, 2008). In turn, depression is associated with delays in seeking medical care, resulting in late diagnosis and treatment among older Hispanics (Rodriguez-Galan & Falcón, 2009), and high rates of suicide attempts among Puerto Ricans (Oquendo, Lizardi, Greenwald, Weissman, & Mann, 2004). Further compounding existing health disparities, older Hispanic/Latino adults are less likely to access adequate mental health care resources (Unützer et al., 2003). Contributing factors for this limited access consists of medical antecedents (Zimmerman, Mast, Miles, & Markides, 2009), socioeconomic, as well as, cultural factors—including stigmatization of mental health and perceptions/engagement within urban and inner-city communities (Kawachi & Berkman, 2003; Kim, 2008; Mair, Diez Roux, & Galea, 2008; Paczkowski & Galea, 2010; Walters et al., 2004). Although U.S. Hispanics/Latinos are a very heterogeneous group, and those in Los Angeles are more likely to be from Central America than some of the studies cited here, this body of work shows that as a whole, depression is an important problem for Hispanics/Latinos warranting further investigation.
Clinically diagnosed depression and subclinical presentation of symptoms have been associated with a number of deleterious health related effects including decreased physical activity, decreased quality of life, increased morbidity/mortality, and increased health care expenditure (Beekman, Deeg, Braam, Smit, & Van Tilburg, 1997; Meeks, Vahia, Lavretsky, Kulkarni, & Jeste, 2011; Schulz et al., 2000). Despite increasing evidence linking negative affective states to compromised physical health, the impact of depressive symptoms on cognitive functioning among older Hispanic/Latino adults remain largely unstudied with the limited evidence often conflicting. Hispanic/Latino older adults in the United States may be particularly vulnerable to the comorbid experience of depressive symptoms and cognitive impairments given documentation of financial constraints, language-related barriers, reduced educational attainment, and overrepresentation within inner-city neighborhoods (Black et al., 1999; Espino, Lichtenstein, Palmer, & Hazuda, 2001; Perrino, Mason, Brown, Spokane, & Szapocznik, 2008).
Measured by multiple distinct previously tested instruments (e.g., Geriatric Depression Scale [GDS], Hoyl et al., 1999; Center for Epidemiologic Studies Depression Scale, Haringsma, Engels, Beekman, & Spinhoven, 2004; Radloff, 1977), some studies identify depressive symptoms as a risk factor for global cognitive impairment among African American and Hispanic/Latino populations (Angel, Frisco, Angel, & Chiriboga, 2003; Downer, Vickers, Al Snih, Raji, & Markides, 2016; O’Bryant et al., 2013; Perrino et al., 2008), with further indication that persistent depressive symptoms may be prospectively linked with later onset cognitive decline (Perrino et al., 2008). Elevated symptoms of depression in this cohort are also linked to poor episodic memory (memory associated with autobiographical events) and impairments in executive function (Bauermeister & Bunce, 2015), processing speed, visual recognition and simple reaction time (Bunce, Batterham, Christensen, & MacKinnon, 2014), and subsequent amplified risk of Alzheimer’s disease in later life (Håkansson, Soininen, Winblad, & Kivipelto, 2015). Providing conflicting evidence, a subset of studies document no association between depressive symptom and cognitive functioning in later life (Comijs, van den Kommer, Minnaar, Penninx, & Deeg, 2011; Petersen, McGue, Tan, Christensen, & Christiansen, 2016). Divergent findings are often attributed to the selection of clinical versus community samples, ethnic/racial subgroupings, incongruent follow-up periods across studies, and different assessment tools to capture depressive symptoms and cognitive function (Perrino et al., 2008).
Given current gaps in the field, the primary aim of the current study is to explore the cross-sectional and prospective associations of depressive symptoms and cognitive functioning in a large sample of older Hispanic/Latino adults enrolled in an exercise intervention. We hypothesized that compromised profiles of cognitive functioning, independent of sociodemographic factors and medical comorbidities, would be evident in older Hispanic/Latino adults experiencing elevated symptoms of depression, when compared to peers with low to no symptoms. The current study seeks to address gaps in the current literature on the association of depressive symptoms and cognitive function by specifically dealing with two major shortcomings: (a) minimal to no inclusion of minority or underserved older adult populations (i.e., Hispanics/Latinos) and (b) absence of longitudinal designs capturing measures of psychological ill-being and cognition across multiple waves. We additionally adjust for medical comorbidities that may serve as confounders but are generally overlooked. Findings from the current study may also elucidate implications for health professionals to better understand and deliver interventions to address the unique physical and mental health needs of older Hispanic/Latino adults.
Method
Study Population and Data Source
The current dataset (N = 572) comes from a randomized trial whose aim was to examine the efficacy of a multifaceted exercise intervention (¡Caminemos!; clinicaltrials.gov #NCT00183014) in increasing physical activity levels and reducing behavioral sedentarism in older Hispanics/Latinos (Hernandez et al., 2015; Hernandez, Prohaska, Wang, & Sarkisian, 2013). Analyses for the current study involved baseline, 1-year, and 2-year in-person interview data collected from older Hispanic/Latino adults (aged ≥ 60 years) participating in the ¡Caminemos! Trial.
Briefly, original study enrollment occurred between August 2005 and 2009 across 27 senior centers in the greater Los Angeles region. Hispanic/Latino adults were eligible to participate in the trial if they met the following criteria: self-report of Hispanic/Latino heritage, aged 60 years or older, English or Spanish fluency, and sufficient cognitive functioning (measured using a six-item cognitive screening test, Callahan, Unverzagt, Hui, Perkins, & Hendrie, 2002). Older adults reporting active participation in 20 min or more of physical activity at least 3 days a week (n = 164) were excluded from enrollment in the trial.
Eligible participants were randomly assigned to either the intervention group—consisting of 4 weekly 1-hr group sessions teaching attribution retraining techniques to raise expectations for aging—or the control group who instead received 4 weekly 1-hr health education lectures. As part of attribution retraining, participants were taught that sedenterism is not an inevitable consequence of the aging process, but rather can be attributed to mutable conditions associated with but not caused by aging. Each week, after attending their randomly assigned 1-hr group sessions (i.e., attribution retraining vs. health education), participants in both arms of the study participated in a 1-hr exercise class taught by a certified instructor. Exercise classes began 15 min after group discussion sessions concluded and involved strength, flexibility, and endurance training from the LifetimeFitnessProgram© (LFP) (now called EnhanceFitness®) and were conducted by trained and certified LFP instructors. The four weekly sessions making up the “core intervention” were followed by monthly follow-up reinforcement (maintenance) sessions for 11 additional months, and sessions every 2 months for the following 12 months (total intervention duration = 24 months). Treatment and control groups received the in-person lectures and exercise sessions separately.
To minimize attrition and improve overall adherence to intervention activities, multiple protocol driven institutional review board (IRB)-approved strategies were implemented including substantial staff effort to obtain outcome data from participants who missed data collection sessions. With these extensive efforts to curtail attrition, the 24-month attrition rate was slightly under 30% for both arms of the intervention; 76% completion rate for intervention arm at 2-year follow-up versus 71% in control arm. Approval for the study was obtained through the Institutional Review Board of the University of California at Los Angeles, and written informed consent was provided by all enrolled participants.
Study Measures
Depressive symptoms
The five-item GDS was used as a screener for depressive symptoms. The five-item scale consists of dichotomous (yes/no) response options to items such as, “Are you basically satisfied with your life?” Acceptable psychometric properties have been shown for the GDS among community-dwelling older adults without overreliance on somatic complaints which are more appropriate for younger populations (e.g., weight loss) (Hoyl et al., 1999). Displaying a sensitivity of 0.97 and a specificity of 0.85, the GDS has good convergent validity when measured against clinically diagnosed depression as per a health care specialist (Hoyl et al., 1999). Older adults who endorse two or more items on the GDS are classified as screening positive for depression. The GDS has been previously used with older Hispanic/Latino adults (Ortega Orcos, Salinero Fort, Kazemzadeh Khajoui, Vidal Aparicio, & de Dios del Valle, 2007; Reuland et al., 2009).
Cognitive function
The Modified Mini-Mental State (3MS) Examination was used to assess cognitive functioning with possible scores in the range of 0 to100 (Teng & Chui, 1987). Lower scores are indicative of greater cognitive impairment. The 3MS test has shown adequate psychometric properties in older adult populations with high-level specificity (0.95) and sensitivity (0.94) (Teng & Chui, 1987). Scores <80 indicate clinically significant cognitive impairment. All participants were administered the 3MS at baseline, Year 1, and Year 2. The 3MS was the only measure included in the parent study to assess cognitive function.
Covariates
Covariates included baseline age (in years), sex, educational attainment (≤ eighth grade; some high school [HS]; HS/Graduate Equivalency Degree [GED] or more), income (<US$5,000; US$5,000 to <US$7,500; US$7,500 to <US$10,000; US$10,000 or more; not reported). We additionally considered self-reported diagnosis of the following chronic conditions: blood pressure, heart attack, congestive heart failure, stroke, diabetes, arthritis, hip fracture, fracture of wrist/arm/spine, asthma or chronic obstructive lung disease, psoriasis, cancer, and bypass surgery.
Statistical Analyses
Data analysis was performed through the use of SPSS version 23 statistical software (IBM SPSS 23 for Windows). Descriptive statistics summarizing baseline characteristics for the total sample are reported for sociodemographic factors, medical comorbidities, and cognitive function; these are presented as frequencies, percentages, and means as appropriate.
We conducted linear and logistic regressions to examine the association between depressive symptoms and cognitive impairment at baseline, with cognitive functioning scores for the 3MS as the outcome variable. Our model included baseline depression status—effect-coded: 0.5 = elevated symptoms of depression (2+ symptoms on the GDS), −0.50 = little to no depressive symptoms (< 2 symptoms on the GDS)—as well as terms for the following covariates: baseline age, sex, educational attainment, income, number of chronic conditions, and intervention group. All continuous variables were mean-centered and all categorical variables were effect-coded prior to analysis. We conducted both a linear regression presenting cognitive functioning as a continuous outcome (3MS scores ranging from 0 to 100) and a logistic regression with cognitive impairment status as a binary outcome—1 = cognitive impairment (3MS scores < 80) and 0 = no cognitive impairment (3MS scores > 80). Longitudinal growth models were used to examine changes in cognitive functioning across time to identify significant differences as a function of participants’ depression status. Specifically, we used longitudinal mixed-effect models (MIXED) (Singer & Willett, 2003) to examine cognitive functioning as a continuous outcome and generalized estimating equations (GEE) (Zeger, Liang, & Albert, 1988) to examine cognitive impairment as a binary outcome—1 = cognitive impairment (3MS scores < 80) and 0 = no cognitive impairment (3MS scores > 80). Longitudinal growth models offer several advantages over traditional analytic methods (e.g., repeated measures ANOVA) (Singer & Willett, 2003). Although traditional methods cannot accommodate incomplete data points, unbalanced data, or non-independence of observations, longitudinal growth models are able to accommodate missing data points, unbalanced data, and non-independence in observations. For all mixed-effects models, we included random effects for the intercept to allow individuals to vary in their initial levels of cognition. We tested whether to include random slopes to account for the variability in the rate of cognition change, but results based on R-squared, Bayesian information criterion (BIC), and Akaike’s information criterion (AIC) indicated no improvement of model fit. Our model included participants’ depression status—effect coded: 0.5 = elevated symptoms of depression (2+ symptoms on the GDS), −0.50 = little to no depressive symptoms (<2 symptoms on the GDS—time (baseline, 1 year, and 2 years), the interaction of depressive symptoms and time, as well as terms for our sociodemographic covariates: baseline age, sex, education, income, number of chronic conditions, and intervention group.
Results
Baseline Characteristics of the Study Sample
A total of 572 participants were included in the analyses (Mage = 73.13, SD = 6.76, 77.10% female). Table 1 provides participant characteristics. At baseline, older adults in this sample were 77% female, with a mean age of 73.13 years (SD = 6.76), 59% had less than an eighth grade education, 45% had income below US$10,000, and participants self-reported an average of two chronic conditions. A total of 77.6% self-identified as foreign-born, of which the majority reported Mexican ancestry (58.5%) with the remainder reporting country of birth as Central or South America (not shown). In addition, 73.4% of those enrolled in current study completed the survey battery in the Spanish language. Over the study period, mean cognitive functioning scores on the 3MS increased from 82.18 at baseline to 84.71 in Year 2. The percentage of participants with elevated depression decreased from 27.6% at baseline to 5.2% in Year 2. Compared to older adults not reporting elevated symptoms of depression at baseline, those with high levels of depression at baseline (2+ symptoms on the GDS) were more likely to report having a greater number of chronic conditions (Mdepressed = 2.56, SDdepressed = 1.47 vs. Mnotdepressed = 2.12, SDnotdepressed = 1.26, respectively, p < .001) and have incomes below US$10,000 (64% vs. 26.87%, p < .05). However, we found that older adults with elevated symptoms of depression at baseline did not differ from older adults not screening positive for depression at baseline in terms of their educational attainment, sex, or age.
Baseline Sample Demographics.
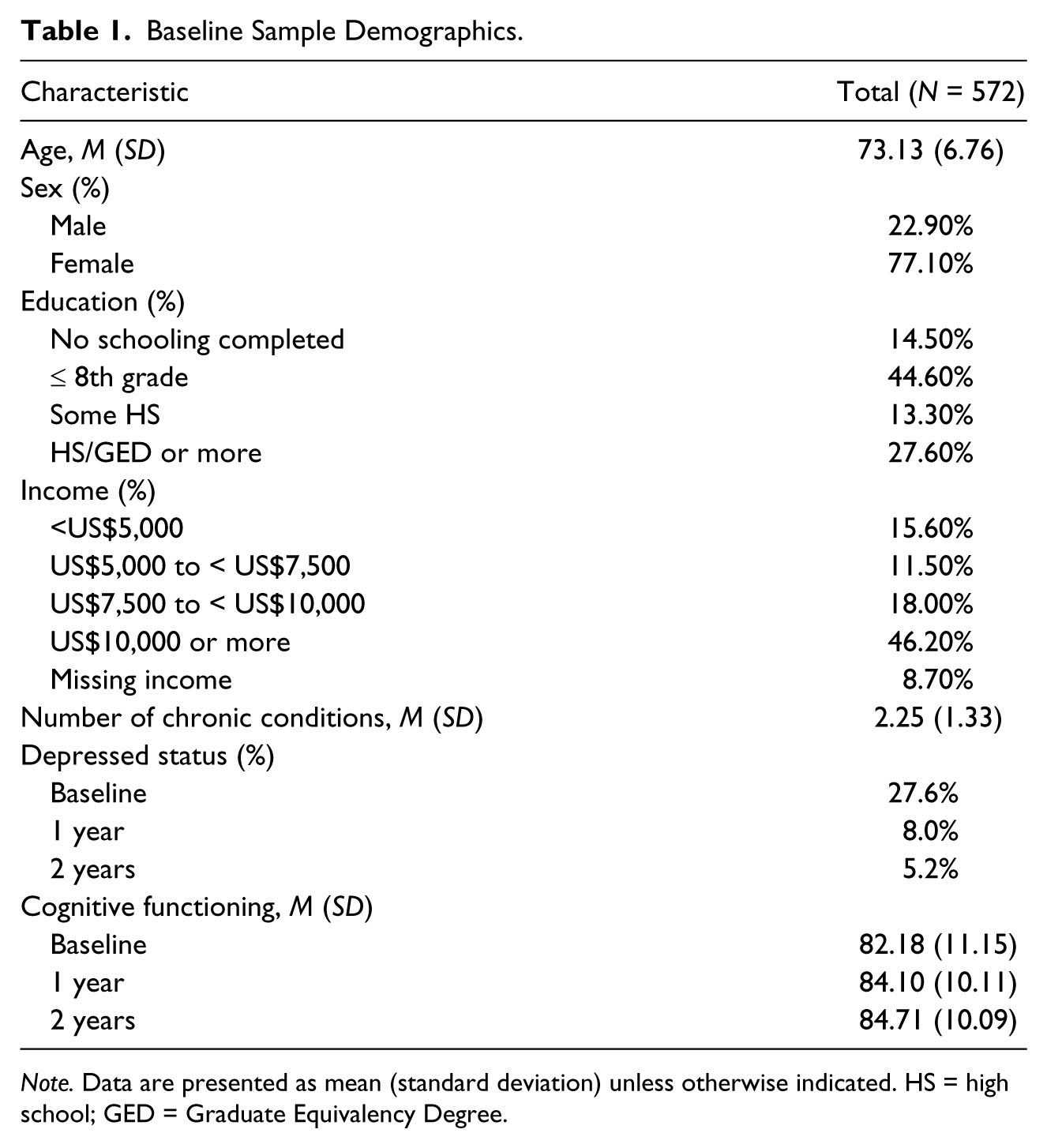
Note. Data are presented as mean (standard deviation) unless otherwise indicated. HS = high school; GED = Graduate Equivalency Degree.
Relationship Between Depressive Symptoms Cognitive Functioning at the Baseline Assessment
As seen in Table 2, at baseline, depressive symptoms were negatively associated with cognitive functioning, b = −3.09, t(558) = −3.09, p = .001, such that Hispanic/Latino older adults who screened positive for elevated depressive symptomatology had lower cognitive functioning scores on the 3MS (M = 78.82, SD = 12.75) relative to older adults who did not screen positive for depression (M = 83.47, SD = 10.21). In addition, depression at baseline was positively associated with our dichotomous measure of cognitive impairment, b = 0.46, χ(558) = 4.22, p = .04, such that Hispanic/Latino older adults who showed elevated symptoms of depression were 1.58 times more likely to demonstrate cognitive impairment (3MS < 80). Age, education, and income were all correlated with cognitive functioning and cognitive impairment in the expected direction of effects; namely, older age, lower levels of education, and lower income were all negatively associated with cognitive functioning and positively associated with cognitive impairment. Intervention group, gender, and the existence of chronic conditions were not associated with cognitive functioning or cognitive impairment at baseline.
Association of Depressive Symptoms and Cognitive Functioning at the Baseline Assessment (Using Linear and Logistic Regressions), Controlling for Sociodemographic Covariates.
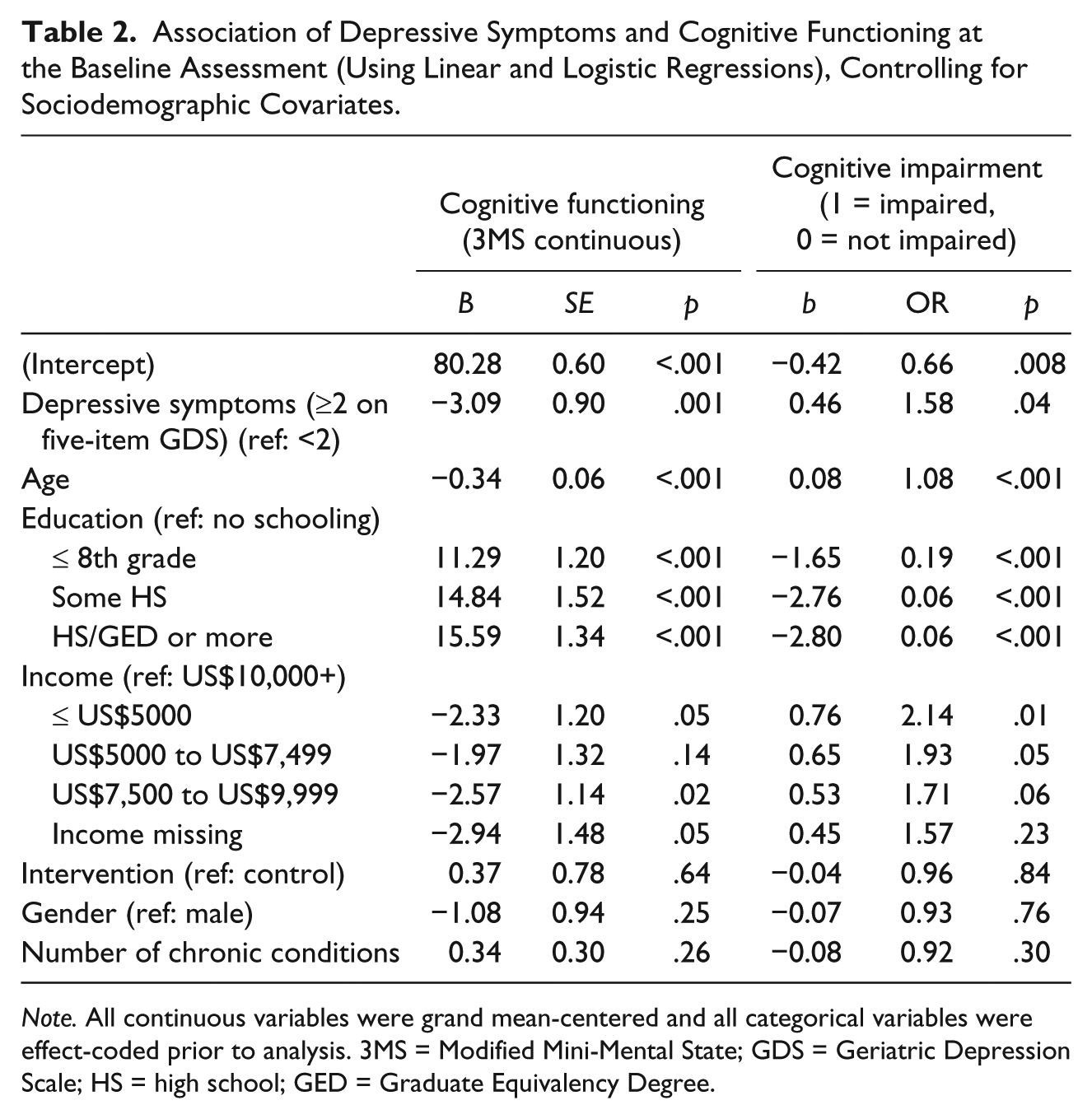
Note. All continuous variables were grand mean-centered and all categorical variables were effect-coded prior to analysis. 3MS = Modified Mini-Mental State; GDS = Geriatric Depression Scale; HS = high school; GED = Graduate Equivalency Degree.
Correlation Between Baseline Depressive Symptoms and Cognitive Functioning Over Time
As seen in Table 3, we found that the relationship between baseline depression and cognitive functioning was moderated by time. Specifically, we found significant baseline Depression × Time interactions for cognitive functioning at the 1-year and 2-year follow-up visits. Tests of simple effects revealed that whereas baseline depressive symptoms were associated with poorer cognitive functioning at the baseline assessment (p < .05), baseline depressive symptoms were not associated with cognitive functioning by the 1- and 2-year follow-ups (ps > .12) (see Figure 1). In addition, we found a similar, albeit weaker, pattern of effects for cognitive impairment (assessed as a binary outcome). Specifically, we found a significant baseline Depression × Time interaction for cognitive impairment at the 1-year follow-up (p = .05), but not the 2-year follow-up (p = .11). Tests of simple effects revealed that whereas baseline depressive symptoms were associated with cognitive impairment at the baseline assessment (p = .04), baseline depressive symptoms were not associated with cognitive impairment at either the 1-year or 2-year follow-up assessments (all ps > .63). Interestingly, older adults in this sample showed significant increases in cognitive functioning and significant decreases in cognitive impairment at each of the follow-up assessments (all ps < .001). Once again, age, education, and income were all associated with cognitive functioning and cognitive impairment in the expected direction of effects; namely, older age, lower levels of education, and lower income were all negatively associated with cognitive functioning and positively associated with cognitive impairment. Intervention group, gender, and the existence of chronic conditions were not associated with cognitive functioning or cognitive impairment at baseline.
Baseline Depression Status and Association With Longitudinal Changes in Cognitive Functioning (Using MIXED and GEE), Controlling for Sociodemographic Covariates.
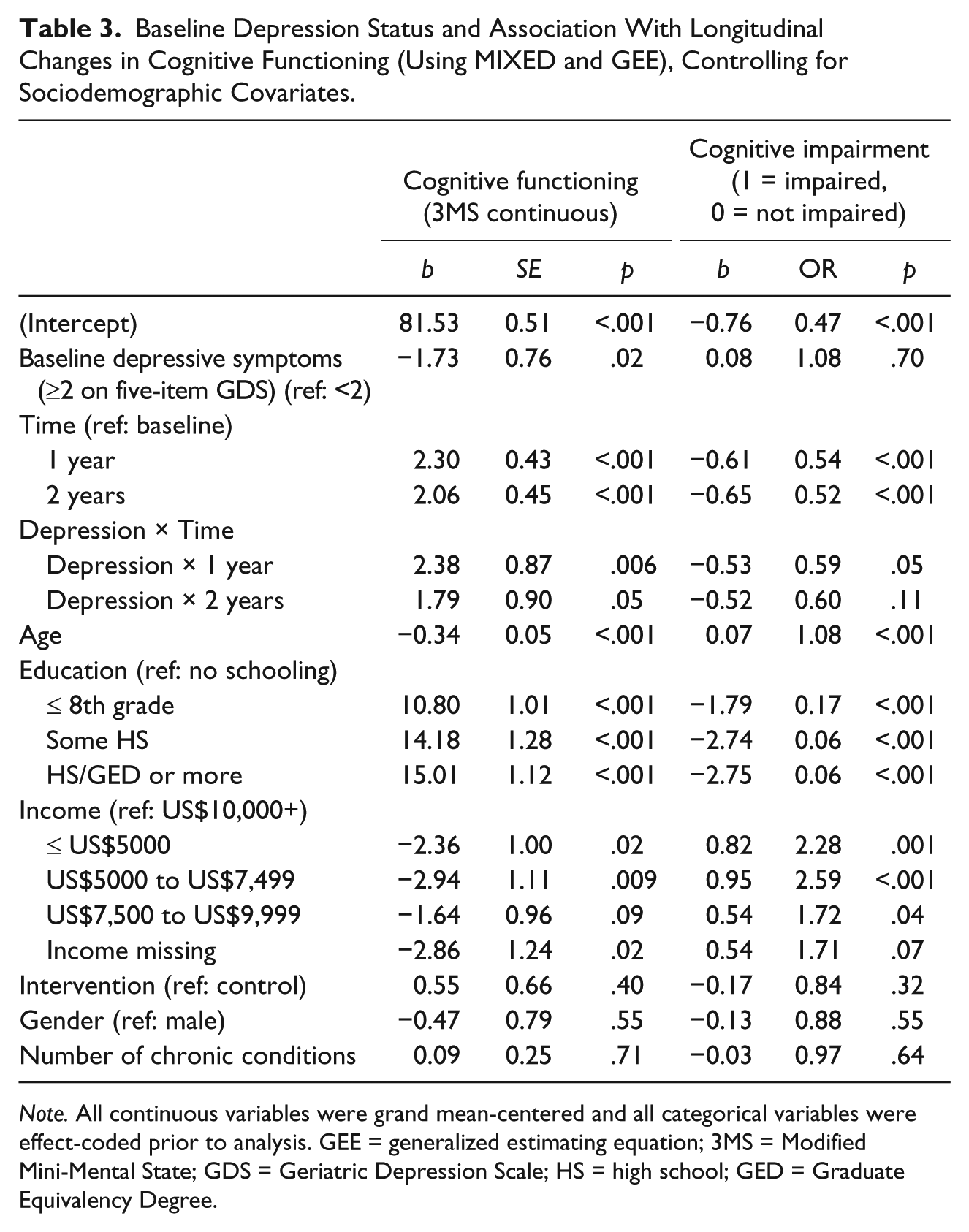
Note. All continuous variables were grand mean-centered and all categorical variables were effect-coded prior to analysis. GEE = generalized estimating equation; 3MS = Modified Mini-Mental State; GDS = Geriatric Depression Scale; HS = high school; GED = Graduate Equivalency Degree.
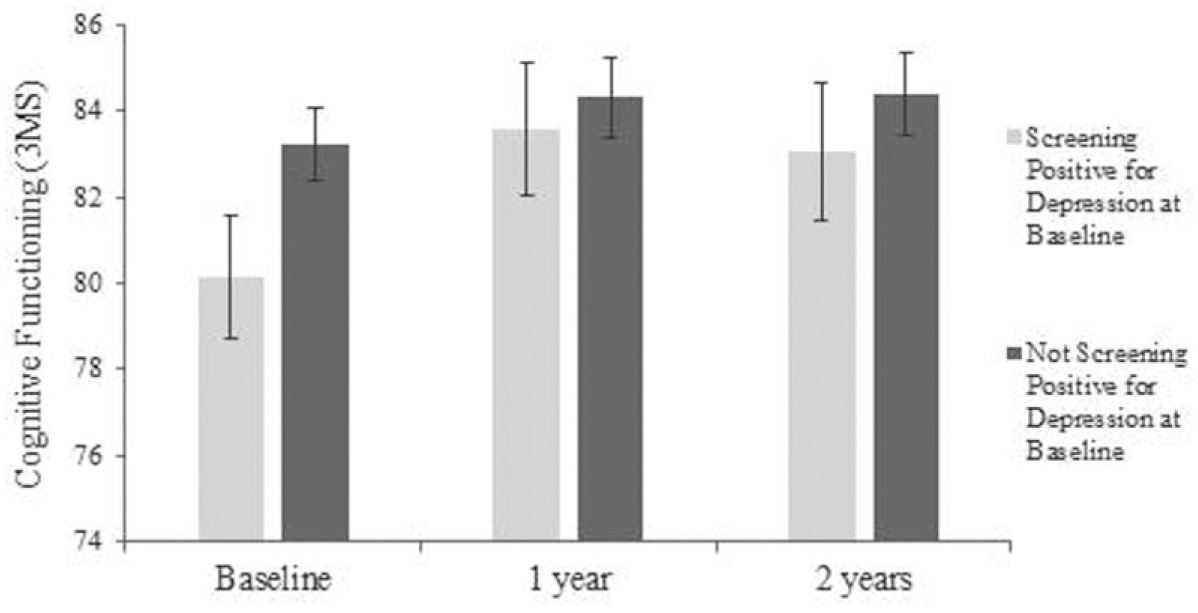
Baseline depression status and association with cognitive functioning over time, controlling for sociodemographic characteristics.
Association Between Depression Status and Cognitive Functioning at Each Assessment Point
As seen in Table 1, participants’ depression status was not stable L across time points; whereas 27.6% of the sample screened positive for depression at baseline, only 5.2% of the sample screened positive for depression by the 2-year follow-up. As such, we conducted additional longitudinal analyses examining whether participants’ depression status at the time of each assessment was associated with their cognitive functioning during that assessment. We found significant correlations between participants’ depression status at the time of each assessment and their cognitive functioning, b = −3.08, t(1267) = −4.48, p < .001, as well as cognitive impairment, b = 0.63, χ(1435) = 9.23, p = .002, at that assessment. Specifically, Hispanic/Latino older adults with elevated symptoms of depression had lower cognitive functioning scores on the 3MS during that assessment (M = 80.85, [79.56, 82.13]) relative to older adults who did not screen positive at that assessment (M = 83.88, [83.21, 84.55]). In addition, Hispanic/Latino older adults who screened positive for depression were more likely to experience cognitive impairment at that assessment (M = 0.36, [0.27, 0.46]) relative to older adults who did not screen positive at that assessment (M = 0.23, [0.20, 0.27]), such that Hispanic/Latino older adults who showed elevated symptoms of depression were 1.88 times more likely to experience cognitive impairment (3MS < 80) at that assessment. Participants’ depression status was not moderated by time for either their cognitive functioning and cognitive impairment scores (all Depression × Time interactions ps > .22) (see Figure 2).
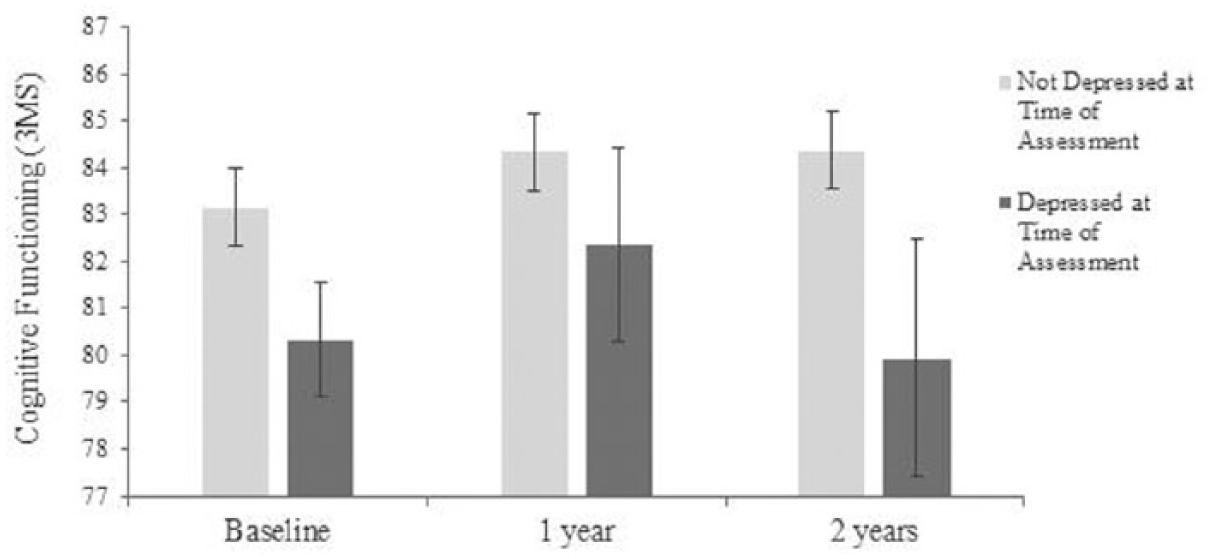
Association of depressive symptoms within each assessment and cognitive functioning over time, controlling for sociodemographic characteristics.
Discussion
In the current study of older Hispanic/Latinos recruited from senior centers and participating in an exercise intervention, 27.6% screened positive for depression at the baseline assessment, substantially higher than observed for the general U.S. population of older adults (Blazer, 2003; Hernandez et al., 2013). Findings suggest not only that elevated symptoms of depression are consistently associated with lower levels of cognitive functioning in older adults but also that the negative association between depressive symptoms and cognitive functioning is limited to the period of assessment, and depressive symptoms are not associated with cognitive functioning in future assessments. In other words, findings suggest that prevalent but not necessarily historic depressive symptoms are associated with impaired cognitive functioning at older ages for these participants in an exercise intervention.
Our findings of a significant link between depressive symptoms and cognitive functioning in older adults is consistent with the bulk of previous findings in this age cohort (Gatz, Tyas, John, & Montgomery, 2005; González et al., 2001; Menselson et al., 2008; Perrino et al., 2008). This finding is of clinical import as it suggests that interventions geared toward alleviating depressive symptoms may have a positive impact not only on emotional well-being but also on current cognitive function. This may be particularly challenging among Hispanic/Latino adults as this group is less likely to be diagnosed when experiencing psychological distress and often hold stigmatizing beliefs regarding mental health treatment which further prevents seeking of care (Lewis-Fernandez, Das, Alfonso, Weissman, & Olfson, 2005). Strength-based treatment approaches—that is, those that emphasize patients’ psychological assets—may be a promising avenue that is well aligned with Hispanic/Latino cultural scripts of interpersonal harmony and strong familial commitment (Hernandez et al., 2016). Given the non-experimental nature of our observational design, it is also plausible that a bidirectional relationship is evident whereby cognitive decline contributes to development and/or exacerbates poor mental health, or that something else entirely, such as poor physical health or social support, contributes to both depression and cognitive impairment. The current study documents a significant cross-sectional association between depressive symptoms and cognitive function across study waves in the presence of an exercise intervention. More robust designs that reduce threats to internal validity are needed, however, if we are to make inferences regarding causality.
A uniqueness of the current study is that it was embedded within a randomized trial testing an exercise intervention and only enrolled subjects who were sedentary at baseline. This uniqueness can also serve as a limitation given that exercise can incur mental and physical health benefits (Callaghan, 2004). Consequently, health trajectories seen for the current cohort may be atypical outside of the context of an exercise intervention. Absence of an association between baseline depressive symptoms and cognitive functioning across time may also be attributed to the relatively short follow-up period, low educational attainment of study participants (as a robust linked was evident in a cohort with higher education status) (Hollocks et al., 2015), and/or the inability to capture symptom chronicity (Perrino et al., 2008).
The present study has multiple strengths. It is one of the few studies examining psychological distress (i.e., depressive symptoms) in a large sample of community-dwelling urban older Hispanic/Latino adults. In addition, extensively tested instruments with excellent validity were used to capture both depressive symptoms and cognitive functioning. We do recognize, however, that analyses could have benefited from the availability of additional measures of cognition, including those assessing executive function and more objective clinical tests capable of detecting pathophysiologic alterations and changes in brain structure. Generalizability may also be limited as older adults in the current study were recruited from senior centers and may systematically differ from Hispanics/Latinos not attending such public institutions. Another strength is implementation of GEE, and advanced statistical method to examine the longitudinal relation between depressive symptoms and cognition. Despite numerous strengths, several study limitations should be considered when interpreting study findings. We did not examine clinically diagnosed depression as detailed in the Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5; American Psychiatric Association, 2013), but instead examined depressive symptoms using a previously tested screening tool with excellent diagnostic accuracy. Our findings may have differed had clinical diagnostic guidelines been used. Also, current use of pharmacotherapy (e.g., antidepressants) was not evaluated as this information was not collected as part of the original parent randomized control trial (RCT).
Future studies will want to address shortcomings of the literature. First, the underlying biological mechanism through which emotional health influences cognitive functioning remains largely unexplored. Potential avenues to explore include disruption of the vascular beds of the cortical and subcortical brain regions (Grool et al., 2012; Hollocks et al., 2015). In addition, as Hispanics/Latinos do not represent a homogeneous group (Daviglus et al., 2012; Sorlie et al., 2010), future studies will want to explore effect modification of the association of mental health and cognition in older Hispanics/Latinos of diverse heritage groups (e.g., Cuban vs. Mexican vs. Puerto Rican).
Taken together, these findings paint an optimistic portrait of cognitive aging across the life span. Although we found that elevated depressive symptoms were consistently associated with lower levels of cognitive functioning in cross-sectional analyses, the negative effects of depressive symptoms on cognitive functioning did not lead to future impairment in cognitive functioning. That is, participants’ depression status at the time of each assessment was significantly associated with their cognitive functioning during that assessment, but was not associated with their cognitive functioning in future assessments. Consistent with this flexible view of depression and cognitive decline, we found that older adults’ levels of depressive symptoms and their cognitive functioning were not fixed over time. Instead, we found that older adults in our sample showed lower magnitude of depressive symptoms across time as well as improved cognitive functioning, even controlling for sociodemographic variables and the effects of the intervention. This is of major clinical and public health significance given the rapidly growing segment in the United States comprised of older Hispanic/Latino adults. Knowledge garnered from the current study can be used to positively influence cognitive functioning in older Hispanic/Latino adults by promoting increased vigilance and screening efforts to identify and treat psychological ill-being (i.e., depressive symptoms). From a clinical perspective, medical professionals are urged to take a holistic approach to well-being and health that encompasses both physical and mental health metrics.
Footnotes
Acknowledgements
The authors thank the other investigators, the staff, and the participants of the “¡Caminemos!” study for their valuable contributions.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research reported in this publication was supported by the National Institute on Aging of the National Institutes of Health under Awards R01 AG024460 (C. Sarkisian, Principal Investigator [PI]), 1K24AG047899 (C. Sarkisian, PI), P30AG028748 (UCLA Claude D. Pepper Older Americans Independence Center, D. Reuben, PI); Resource Centers for Minority Aging Research Center for Health Improvement of Minority Elderly (RCMAR/CHIME) P30-AG021684 (C. Mangione, PI); and the National Heart, Lung, and Blood Institute (NHLBI) 1K01HL130712-01A1 (R. Hernandez, PI).