
Abstract
Keywords
The growing body of evidence documenting broad-spectrum associations of early life adversity with adulthood health is building an increasingly persuasive case for safeguarding health attentive to early life as well as continuing patterns of adversity exposure. Well, over half of U.S. adolescents and adults experience at least one significant form of adverse childhood experience (ACE) before their 18th birthday (Kessler et al., 2010; McLaughlin et al., 2012). The majority of those report more than one adversity, with at-risk youth and adults report considerably higher exposure levels (e.g., Baglivio, Epps, Swartz, Huq, & Hardt, 2014). Commonly assessed ACEs include exposure to violence and instability or dysfunction among caregivers (e.g., substance abuse, mental illness, or criminality). Population-based studies indicate that these exposures are strongly associated with onset of physical health problems in children, ranging from autoimmune conditions (e.g., asthma) to chronic pain as well as chronic disease outcomes in adulthood even after accounting for other relevant risk factors (Felitti et al., 1998; Scott et al., 2013).
Allied arenas of research are providing insights regarding developmental and health outcomes associated with early life adversity and of mechanisms including neurobiological, cognitive, emotional, and social pathways that unfold in dynamic ways over time (Shonkoff & Garner, 2012; Taylor, Way, & Seeman, 2011). Attention to stress embodiment pathways builds on findings that chronic activation of stress responsive systems can cause “wear and tear” on regulatory systems (McEwen & Seeman, 1999), resulting in a gradual deterioration of health owing to repeated adaptation to stressors (Geronimus, Hicken, Keene, & Bound, 2006). More recent work (Ellis & Del Giudice, 2014; Miller, Chen, & Parker, 2011) theorizes that early life stress may be of particular importance because of its influence on the developing stress response system, particularly immune function, and thus the individual’s response to future encounters with stress (Slopen, McLaughlin, Dunn, & Koenen, 2013). The hypothalamic–pituitary–adrenal (HPA) axis, and its primary adrenal end-product cortisol, appears especially sensitive to social information, calibrating its activity to both social risk factors and socially supportive protective experiences—and the lack thereof (Del Giudice, Ellis, & Shirtcliff, 2011; Miller et al., 2011).
Stress responses to adversities evoke psychological (e.g., anxiety, depression) as well as physical (e.g., increased heart rate and blood pressure) arousal to which, over time, individuals may undertake health-affecting behaviors to blunt or manage that arousal (Ensel & Lin, 2004). For example, smoking, substance use, overeating, and sedentary habits are all behaviors that may help to reduce aversive arousal and to regulate mood state, at least temporarily (Kassel, Stroud, & Paronis, 2003), yet in the long run are associated with morbidity, disability, and mortality (Mokdad, Marks, Stroup, & Gerberding, 2004). Although adherence to health-promotive behaviors has a sustained positive effect on successful aging, there is considerable heterogeneity in these practices and relationships to adult outcomes (Pruchno & Wilson-Genderson, 2012).
Life course stress process models also point to processes of stress proliferation (Pearlin, Aneshensel, & LeBlanc, 1997). That is, early adversity increases the likelihood of subsequent stress exposures and secondary stress effects such as limited developmental success and attainment of various forms of human capital and the capacity to acquire and maintain supporting social relationships (Umberson, Williams, Thomas, Liu, & Thomeer, 2014). These sequences collectively result in deeper trajectories of cumulative adversity and poorer health (O’Rand & Hamil-Luker, 2005). In addition to biological consequences, ongoing stress promulgated through a range of problematic conditions such as low socioeconomic status, and life insults undermine people’s adaptive capacities (Pearlin, Schieman, Fazio, & Meersman, 2005). The social contexts and consequences of early and later adversities and the biological processes of embodiment both accumulate and interact (Blane, Kelly-Irving, d’Errico, Bartley, & Montgomery, 2013) with ACEs both undermining development and health in earlier life stages as well as increasing the rate and range by which health functioning is compromised in later life periods.
Yet these stacked experiences of proliferative stress are commonly underrecognized and, thus, often unaddressed in health care settings. The links between precipitating adversities and their lifelong consequences can thus remain hidden for years, which reduce opportunities for early intervention and prevent cascading damage. Taken together, the extant literature is sufficiently compelling that the American Academy of Pediatrics has issued evidence summaries and policy statements arguing that early life adversity functionally constitutes the roots of later health and functioning disparities and advocating for assessment, reduction, and efforts to mitigate the long-term negative consequences on health (Knudsen, Heckman, Cameron, & Shonkoff, 2006; Shonkoff & Fisher, 2013).
The Present Study
This article addresses the relevance of early life adversity for adult health with several features that extend research to date. We use structural equation modeling (SEM) to test multiple hypothesized pathways, which allows testing the significance of indirect as well as direct effects, thereby allowing for assessment of effect mediation. We are unaware of any published articles applying SEM analysis to test ACEs within multivariate explanation of adult health. Some articles have used more restrictive predictors (e.g., child abuse), with results that support the value of a stress framework (Hager & Runtz, 2012). Rather than focus on specific health conditions (e.g., chronic pain, Lampe et al., 2003), we use a latent construct that includes clinical indicators (number of chronic conditions) as well as subjective and functional indicators (perceived health and days of poor health that interfere with life functioning). This combination may reduce the odds of underdetection of health erosion among individuals who have not yet been diagnosed with health conditions but are experiencing negative health effects.
Our primary goal is to determine whether a cumulative adversity model that captures stress proliferation theorizing achieves good fit. Within this framework, we hypothesize that ACEs will be significantly associated with adult social contexts (low income, adult adversity, social support) as well as health behaviors, each of which will be significantly associated with poorer health. We anticipate that ACEs will achieve significant indirect effects through these variables, indicating mediated pathways to adult health. We anticipate that the model overall will be reasonably robust across sex and age, achieving acceptable model fit, although some variation in effect sizes may be evident. We use age 45 as a cut point for age groups as it represents a life stage beyond young adulthood but not yet into advanced age wherein poorer health is more common, and broader self-reported health may be less reflective of disease progression.
Method
Sample
Data come from the 2011 Washington State Behavioral Risk Factor Surveillance System (BRFSS) survey conducted in collaboration with the Centers for Disease Control (CDC) by health departments in all U.S. states and protectorates. Respondents were obtained via random-digit-dialing and a disproportionate stratified random sampling of households wherein one adult per household was randomly selected for participation in a telephone interview. Respondents missing valid responses to demographic questions (age, sex, race, and education) and ACEs items were excluded from the analyses, for a final sample size of 12,549. Respondents included English and Spanish-speaking adults, aged 18 years or older, who resided in a household with a working landline phone through which they participated in the study.
Measures
ACEs score
ACEs score (R = 0-8) was assessed as an index of “yes” responses to eight dichotomous categories of adverse experiences while below age 18: living with someone with serious mental illness, who has substance abuse issues, who had been incarcerated; parents were divorced or separated, physically hurt one another; or who physically, sexually, or verbally abused the respondent.
Low income
Low Income was assessed as an index of four dichotomous items (R = 0-4): an annual household income under US$25,000, unemployed or otherwise unable to work, unable to see a health care provider due to cost, and being food insecure.
Social support
Social Support (R = 0-4) is an index summing the number of people (0-3) respondents reported that they can count on to help with practical problems plus an additional value of 1 if married or partnered.
Adult adversity
Adult Adversity (R = 0-6) is a summed index of adulthood adverse experiences dichotomously coded including being incarcerated, experiencing domestic violence, sexual assault, or homelessness; having health problems that require special equipment; and care burden (provided regular care to others with illness or disability or to unrelated child lacking parental care).
Health Behaviors
Health Behaviors (R = 0-3) is an index of being overweight or obese (body mass index [BMI] of 25 or greater), a current tobacco user, and being sedentary (dichotomously coded). Sedentariness is a CDC calculated variable identifying individuals who do not meet recommended minimums of 150 min (or vigorous equivalent) per week of physical activity.
Poor Physical Health
Poor Physical Health is a latent variable comprising three items. General Health is the respondent’s subjective rating of their own overall physical health, with Likert-type response options of 0 (excellent) to 5 (poor). Poor Health Days is the number of days out of the past 30 the respondent felt their physical health was not good. Chronic Health Conditions is a summed index of nine health conditions that respondents reported “yes” to having a doctor, nurse, or other health professional tell them they had the following: prediabetes, diabetes, asthma, cancer, heart attack or coronary heart disease, stroke, chronic obstructive pulmonary disease (COPD) or emphysema, and kidney disease.
Control variables
Analyses control for race, ethnicity, and education, with mutually exclusive categories of race/ethnicity including White or Caucasian, Black or African American, Hispanic, other race, and multiracial and education represented as dichotomous variables indicating completion of high school or attainment of a GED (General Educational Development) diploma.
Groups
For purposes of analysis, respondents were grouped into four categories based on reported sex and age: females 45 years old or below, males 45 years old or below, females above 45 years old, and males above 45 years old. We chose age 45 as an age that might reasonably represent early onset of poor health and which previous studies have shown that there is already evidence of an association between ACEs and elevated risk of chronic disease reflecting biological processes (Winning, Glymour, McCormick, Gilsanz, & Kubzansky, 2016).
Analysis Plan
The current study assesses the relationships among study variables and both direct and indirect pathways toward Poor Physical Health through a two-step SEM. Analyses begin with confirmatory factor analysis to confirm the construct validity of the Poor Physical Health latent factor. Path analyses then assess the relationships among each of the six manifest (directly measured) and one latent variable. Path models not only assess the direct effect of ACEs on Poor Physical Health but also mediated pathways through the other model predictors. Given the longitudinal association of earlier life and adult income statuses (Duncan, Ziol-Guest, & Kalil, 2010), and thus likely prelude to more proximal adult experiences, Low Income was allowed to serve as a predictor of each of the other mediators. Among these mediators, Adult Adversity and Health Behaviors were allowed to correlate, given the expected high association between these constructs. Path analyses were conducted using a multigroup format, with models examined within each of four groups defined by both age (45 or below/above 45) and sex.
All analyses were conducted with MPlus 7.4 (Muthén & Muthén, 1998-2015). As the analyses included categorical endogenous variables, models were estimated with weighted least squares mean and variance djusted (WLSMV) and a pairwise present approach to missing data to maximize the utility of the available data during estimation. Results presented are the standardized estimates relative to both independent and dependent variables. Analyses were adjusted for sample stratification and weighted by gender and age to provide estimates representative of the population of the State of Washington, using weights provided by the Washington State Department of Health. Given the stratified nature of the sample, analyses adjusted for respondent strata to provide more accurate standard errors.
Results
Weighted demographic characteristics and descriptive statistics for each of the five manifest variables and the three variables that constitute the latent outcome are listed in Table 1 for each sex and age groups, as well as for the full sample. Respondents in the full study sample are identified primarily as Caucasian or White (77.3%), with 2.5% as African American or Black, 11.6% as Hispanic/Latino/a, 6.5% as another race/ethnicity, and 2.1% as multiracial. More respondents below the age of 45 years reported of being Hispanic heritage than those above 45.
Weighted Demographic Characteristics and Mean Estimates by Group.
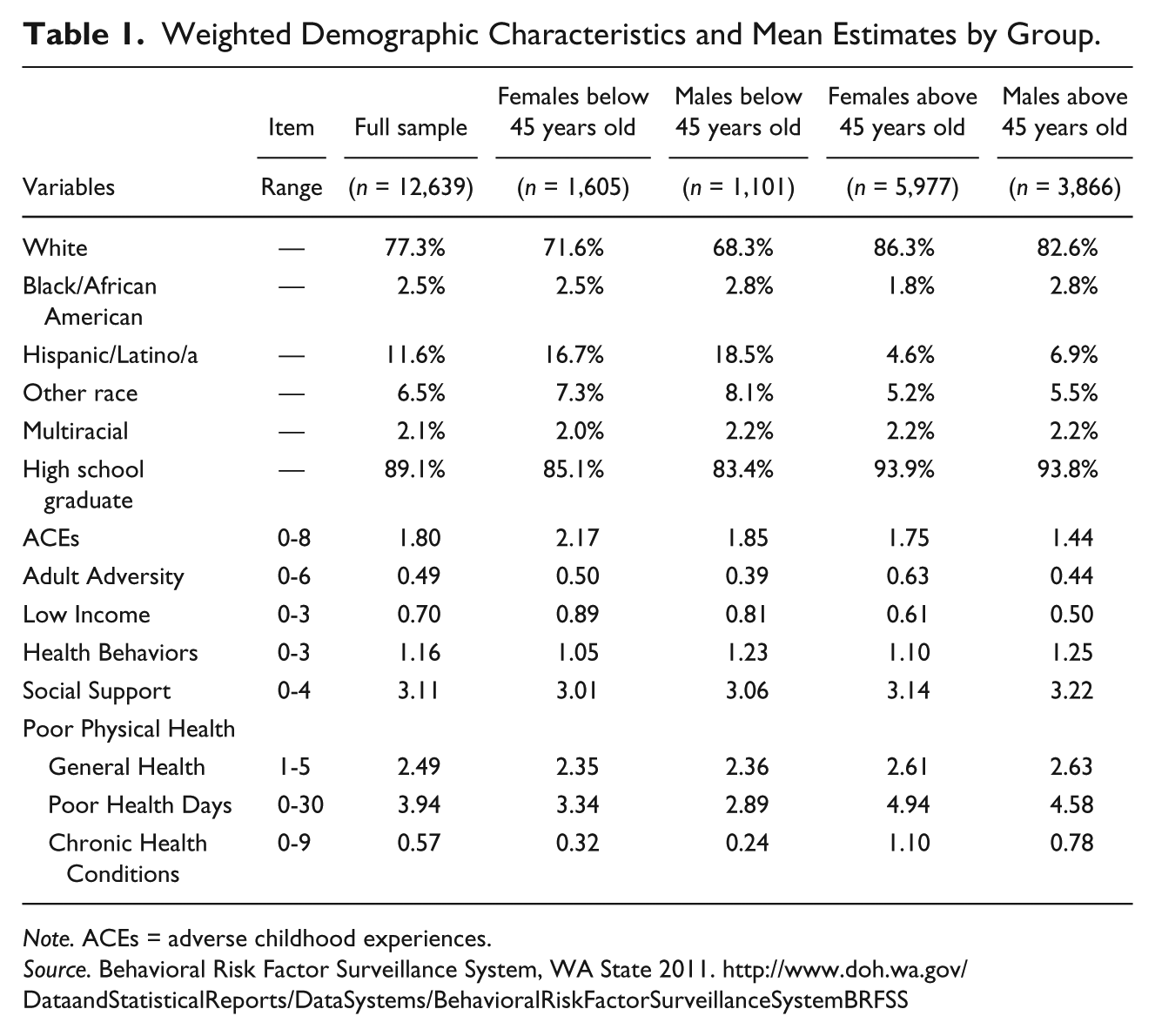
Note. ACEs = adverse childhood experiences.
Source. Behavioral Risk Factor Surveillance System, WA State 2011. http://www.doh.wa.gov/DataandStatisticalReports/DataSystems/BehavioralRiskFactorSurveillanceSystemBRFSS
Compared with males in their same age groups, females, on average, reported higher rates of ACEs, Adult Adversity, Low Income, Poor Health Days, Chronic Health Conditions, and Social Support but lower rates of Health Behaviors. Compared with males and females below 45 years old, respondents above 45 years old reported lower rates of ACEs and being Low Income, as well as higher rates of Poor Health Days and Chronic Health Conditions.
Model Results
The confirmatory factor analysis for the Poor Physical Health latent variable indicated an appropriate factor structure with strong model fit (comparative fit index [CFI] = 0.95; root mean square error of approximation [RMSEA] = 0.03) and satisfactory factor loadings for each of the indicators (General Health, Poor Health Days, Chronic Health Conditions). When accounting for other study variables in the path analyses, factor loadings for the latent variable remained satisfactory (see Figures 1 and 2), with some expected variability across the younger and older age groups.
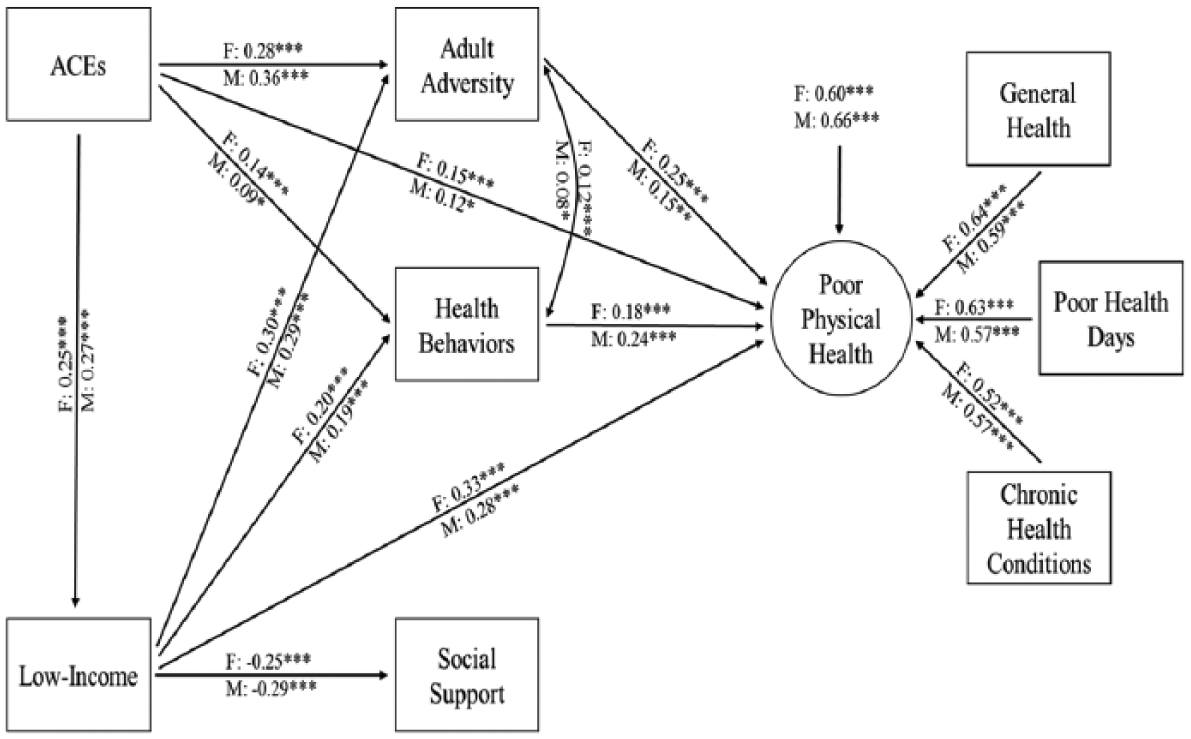
Path analyses estimates among females and males below 45 years old.
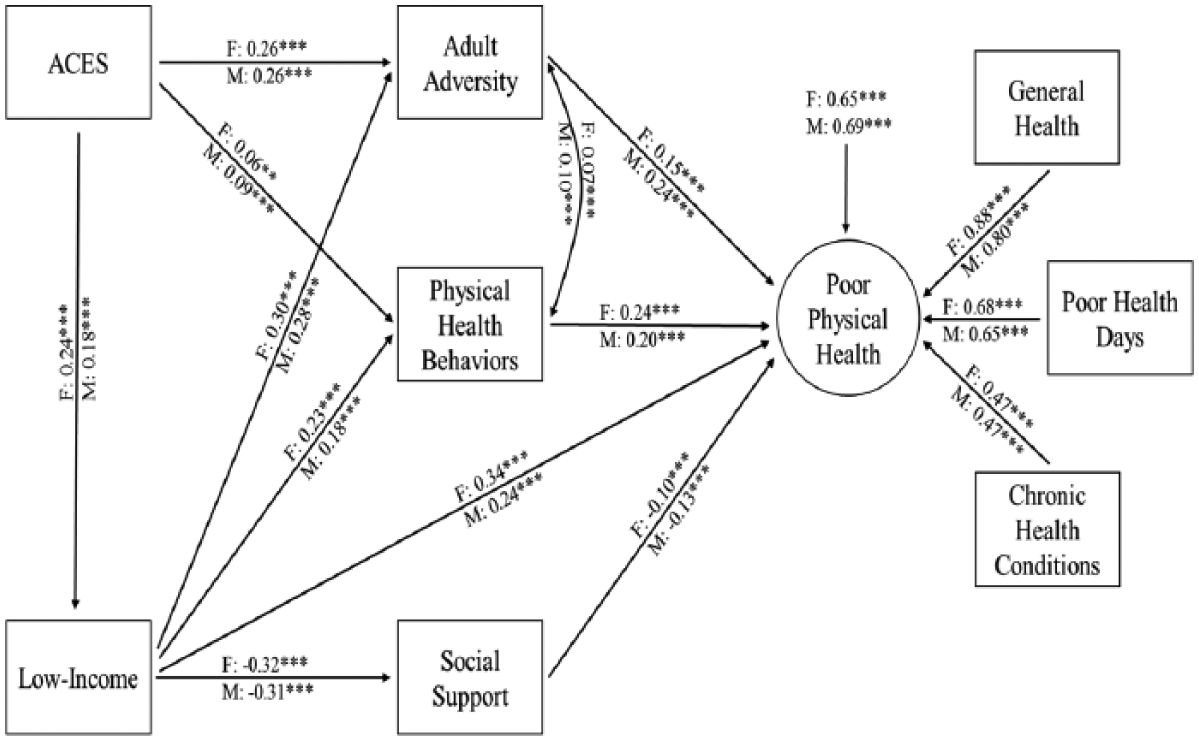
Path analyses estimates among females and males above 45 years old.
Fit statistics for the path analyses were strong, with CFI values of 0.95 or higher and RMSEA values of 0.04 or lower for the full sample and for all four groups (see Figures 1 and 2 for more details). The model estimates among groups were generally more similar by age than by sex; as such, Figure 1 shows the path analysis model results for males and females below 45 years old and Figure 2 shows the estimates for males and females above 45 years old. All estimated paths are displayed along with standardized estimates. For clarity, control variable estimates and estimates of nonsignificant paths are not shown.
Models demonstrated hypothesized findings across all four groups, with significant direct pathways from ACEs to Adult Adversity, Health Behaviors, and Low Income, from Low-Income Households to Adult Adversity, Health Behaviors, and Poor Physical Health, and from Adult Adversity and Health Behaviors to Poor Physical Health. In addition, across groups, the bidirectional correlative association between Adult Adversity and Health Behaviors is slightly positive and significant. Low Income held a substantial, negative association with Social Support across all models. The ACEs direct pathway to Social Support did not achieve significance in any model.
Generally, effect sizes and directionality among estimates were consistent across each of the four groups, with a few age group differences observed. The inverse path from Social Support to Poor Physical Health achieved significance for older (above 45 years old) but not younger adults. The direct path from ACEs to Poor Physical Health achieved significance only for younger males and females (below 45 years old).
Indirect and total effect estimates from ACEs and Low Income to Poor Physical Health are shown in Table 2. For the paths between ACEs and Poor Physical Health, most indirect effects across groups are significant, with relatively modest individual effects. However, this confirms the presence of multiple pathways from childhood trauma to physical health far into adulthood. The exceptions are those pathways through Social Support, which achieved significance only through Low Income and Social Support for older males and females. Most clear from these pathways is that direct effects of ACEs to Poor Physical Health are substantial and significant in younger adulthood where direct combines with indirect effects and that multiple indirect pathways from ACEs sustain into older adulthood.
Indirect, Direct, and Total Path Estimates by Group.

Note. ACEs = adverse childhood experiences; LowInc = Low Income; AdltAd = Adult Adversity; SocSupp = Social Support; HBeh = Health Behaviors; PH=Poor Physical Health.
Source. Behavioral Risk Factor Surveillance System, WA State 2011.
p < .05. **p < .01. ***p < .001.
The mediational pathways from Low Income to Poor Physical Health present similarly, in that the direct path held the strongest effect, with more modest significant indirect effects through Adult Adversity and Health Behaviors. The pathway through Social Support was significant among both male and female older adults. Total effects were similar across all four groups.
Discussion
The current study extends the current research base through testing for both direct and indirect effects of early life adversity on physical health in both younger and older adulthood, thereby distinguishing multiple pathways through which ACE effects appear to be carried within a multivariate structural model. Findings establish good fit of the hypothesized model that was stable across gender as well as adult age periods (before and after age 45). The models confirm our hypotheses that ACEs significantly compromise physical health, as measured by complementary indicators (number of chronic conditions, subjective feeling of health, and number of days health has been poor). Findings elucidate direct effects in younger adulthood, consistent with stress embodiment, as well as mediated pathways through lower economic status, adulthood adversity, poor health behaviors, and, to a more limited extent, lower social support, each of which also lead to poorer physical health.
ACEs, Age, and Physical Health
Younger adults (below 45 years old) indicate a significant direct pathway from ACEs to poor health. This result adds to a growing body of evidence of the role of childhood experience in adult health (Shonkoff, Boyce, & McEwen, 2009) and is consistent with predictions of developmental origins of health and disease models (Gluckman & Hanson, 2004) that postulate stress effects from in utero through full childhood. Childhood stress experience may calibrate the immune system to promote chronic inflammation, which in turn increases risk of diseases of a number of body systems (Miller et al., 2011).
The direct pathway from ACEs does not sustain significance among older adults, suggesting that effects of childhood traumatic experiences on physical health become more diffuse and mediated by other factors. Although ACEs may affect physiology across the life span, and continue to impact health at later ages, the effects captured here suggest that ACEs are accelerating disease processes so that ACEs may be associated with earlier onset of common physical maladies that ultimately appear in a large proportion of the population. Miller et al. (2011) predict that early life stress alters the immune response system throughout the life span which subsequently advances various mechanisms of pathogenesis. As such, this and similar models predict that ACEs increase the risk of faster progression toward the most common causes of poor physical health in this population. We would expect that associations between ACEs and poor health may persist throughout the life span but that these effects may be more difficult to detect at later ages without fine-grained data describing the severity and progression of disease. Moreover, among older individuals, lasting effects of early adversity on physical health are indirectly manifested through other adulthood outcomes, such as increasing the risk of negative health behaviors, which then relate to a higher risk of poor health.
Age also appears to moderate the protective relationship of social support to health with that direct pathway achieving significance only for respondents under 45 years old. Social support here captures availability of helping persons (number of people can turn to for practical help, being partnered). Older adulthood involves greater trends of losing partners (separation, divorce, widowhood) and access to extended family, thereby losing important sources of social support during a life period that often carries greater need for emotional and instrumental supports. Conditions of low income tend to amplify challenges of acquiring and sustaining an engaged support network, which carries implications for health. The presence of both significant direct and indirect effects (from ACEs and low income status) through social support signals a developmental pathway of special note in older adulthood.
In general, sex appears a weaker moderator of model relationships than age. Though some differences in levels across study variables are evident (such as higher cumulative ACEs among females), the set of pathways through which ACEs impact physical health appear to be similar for males and females with no consistent pattern of model differences. This suggests a robustness of theorizing regarding the stress process model applying to both males and females. Although sex differences may be evident in the patterning of intervening factors (e.g., greater sexual assault and interpersonal violence victimization among females, greater incarceration and tobacco use among males), the current findings indicate that a cumulative adversity path model should be applicable to general population males and females.
Stress Proliferation
Results are also consistent with continuity of life stress and secondary stressors implicated as intervening mechanisms within stress proliferation theorizing (Turner, Thomas, & Brown, 2016). That is, some early life adversity may stem from stable or repeated contexts such as socioeconomic disadvantage or family or neighborhood turmoil or dysfunction that exposes individuals to ongoing cumulative risk (Evans & Kim, 2010; Pearlin et al., 2005). Early life adversities are also associated with curtailed opportunities and success, such as lower educational and occupational achievement, less effective social supports, and trajectories of stress-related health behaviors (Umberson, Liu, & Reczek, 2008; Zielinski, 2009).
Indeed, for respondents in all four models, ACEs showed direct predictive effects toward lower current income status, greater adult adversity exposure, and more health compromising behaviors, as well as significantly mediated effects through each of these variables to poorer health. This theory base views early adversity as a risk factor for chains or trajectories of risk, with greater accumulation leading to greater health erosion (Hertzman, Power, Matthews, & Manor, 2001; Kuh & Shlomo, 2004). The pathway from ACEs to low income adult statuses is particularly noteworthy as this spawns multiple subsequent pathways carrying both ACEs and poverty effects toward poor health.
Socioeconomic status holds broad implications regarding the conditions of people’s lives, including the likelihood of encountering a range of adversities as well as having fewer resources to buffer or deal with life stressors. This stacking of stressors accelerates weathering or wear and tear on the body’s physiological regulatory systems, leading to earlier aging, particularly among the poor (Crimmins, Kim, & Seeman, 2009; McEwen & Seeman, 1999). Study of biological risk profiles via biomarkers reveal powerful and sustained implications of low income across cardiovascular, metabolic, and inflammatory risks. Such results also point to the interruptive potential of early investments in higher education and income to curb early adversity effects (cf. Cohen, Janicki-Deverts, Chen, & Matthews, 2010).
Early adversity combines with poverty toward elevating risk of both continuing stress through significant adversities in adulthood as well as health compromising behaviors. Both pathways are likely to influence the types of environments that individuals inhabit which may carry multiple and often inescapable forms of stress, shape individuals’ perceptions of and reactions to adversity that heighten distress and exacerbate stressful circumstances (Holahan, Moos, Holahan, Brennan, & Schutte, 2005; Matthews & Gallo, 2011), and foster coping patterns that undermine health (Felitti et al., 1998; Turner & Lloyd, 1995).
One advantage of SEM model testing relative to regression approaches is the ability to test for indirect effects through multiple pathways. These findings document the importance of adult social contexts and experiences as well as behavioral habits in mediating effects from early adversity exposures. This life course infusion of effects suggest early life adversity to carry a metamechanism function, that of a fundamental risk factor that spreads through a range of subsequent mechanisms that carry health jeopardy—thereby compounding health risk, particularly among those with histories of adversity (Link & Phelan, 1995).
Implications of a Life Course Perspective
The sustained long reach of early adversities on health far into adulthood substantiates childhood as a sensitive life period (Lynch & Smith, 2005) and the value of life course perspective on health that urges consideration of pathways as prevention venues. The mediating pathways observed here promote confidence in the value of interventions across the life course to strengthen ACE-affected individuals’ contexts, choices, and resources toward disease avoidance and resilience promotion. Schafer and Ferraro (2012, p. 118) offer the metaphor of an athletic tournament, noting that individuals with the burden of early adversities or misfortunes “may not be eliminated in the initial round of competition” but are unlikely to advance to “the elite stages of the game” represented by relative disease freedom and well-being. At the same time, social and biological trajectories are intertwined across the life course, with protective resources offering the potential of redirecting trajectories (Hatch, 2005), supporting our metaphoric athletes in advancing with vigor to the finals.
The presence of robust effects among ACEs, low income, adult adversities, and poor health behaviors is notable among younger respondents as these ages constitute parenting years of younger children. Evidence is accumulating that stress exposure health effects can span more than one generation through an array of biological processes (Bowers & Yehuda, 2016; Haussmann & Heidinger, 2015). In addition, those with greater ACEs are at greater jeopardy of carrying a range of distal and proximal risks into the family households and their parenting capacities such as risk of lower income, greater adversity, lesser support, and poorer health behaviors and conditions as indicated here. These conditions, in turn, constitute early adversity risks for their children. Although the current study does not provide direct results regarding parenting or intergenerational transmission, related evidence indicates these conditions and parental ACE exposure are associated with disrupted developmental transitions and poorer health at earlier ages among offspring (Evans, Li, & Whipple, 2013; Wickrama, Conger, & Abraham, 2005). In addition to health supports, parenting and family supports are likely to hold promise for interrupting cross-generational impairments, particularly for ACE-affected and underresourced parents (Lengua et al., 2014; Steele et al., 2016).
Limitations
A number of limitations should be noted. These data are cross-sectional and based upon one U.S. state with race/ethnicity characteristics that may not be representative of other regions. The analysis controls for race and ethnicity to partially address this issue. The measures constructed here from available data are limited in their capacity to fully capture full dimensionality of the constructs. In particular, social support is a broadly applicable construct that would benefit from inclusion of features such as quality of one’s social support structure and perceived support satisfaction. Use of multiple health status indicators (diagnosed, self-assessed, days of health impairment) in the health status latent variable allows a more balanced, comprehensive assessment of health relative to singular disease assessment. However, measurement of additional aspects of health, ideally including more detailed health information that better reflects biological processes and disease progression as well as environmental factors may yield more information about how stress pathways function to produce negative physical health outcomes. The exclusion of individuals who are not home-based (e.g., in residential, medical or other system settings) and those for whom ACEs and demographic data were not available may lead to an underestimation of ACEs and, thus, of some relationships in pathways to poorer health. Although mean comparisons of study variables between those with missing data and the study sample identified only minimal variation, it is possible that excluded individuals may represent adults with greater adversity exposure.
Conclusion
The current findings argue the value of including both early life and adult adversity as routine aspects of health histories. Ideally, preventing and reducing early life adversity exposure is a primary aim not only for early life benefits but also an important element to addressing preventable adult health disparities. Attention to issues such as health care access and quality problems is clearly relevant. Yet evidence is mounting that tackling early life adversity origins of life course health disorders may be a powerful strategy for reducing enduring effects and, thus, reducing the population-level burden of premature and complex health erosion (Schafer & Ferraro, 2013; Shonkoff et al., 2009). Medically, awareness of cumulative adversity profiles offers opportunities for patient education about stress effects as well as strategies to promote health enhancing behaviors and conditions. Proactivity oriented models of healthy aging find evidence for the value of anticipatory adaptations (e.g., exercise, marshaling support) toward maintaining quality of life among older adults within a stress paradigm (Kahana, Kelley-Moore, & Kahana, 2012). The current findings suggest the extended value of this kind of intentionality—of building and invoking internal and external resources across the life course to buffer stress, foster resilience, and safeguard health.
This study was able to document multiple important pathways that connect childhood experiences to adulthood outcomes within a population representative sample. Use of routinely collected health surveillance data for these purposes encourages extended research across other states and regions and, potentially, other administrative data. These observed pathways illuminate the potential of multiple settings and opportunities for education about life course adversity, interrupting stress proliferation, and strengthening protective factors to offset adversity effects. In addition to health care, community and system supports that address education, workplace, economic insecurity, child and family needs, criminal justice, social isolation, and related aspects of functioning and well-being will encounter individuals with cumulative risk histories and can be part of a network of forces to curb adversity effects on health.
Footnotes
Authors’ Note
This research was supported in part by a grant from the Eunice Kennedy Shriver National Institute of Child Health and Human Development research infrastructure grant, R24 HD042828, to the Center for Studies in Demography & Ecology at the University of Washington as well as a grant from the Gates Foundation to the Foundation for Healthy Generations.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported in part by a grant from the Eunice Kennedy Shriver National Institute of Child Health and Human Development research infrastructure grant, R24 HD042828, to the Center for Studies in Demography & Ecology at the University of Washington.