
Abstract
Successful aging (SA) is widely discussed in gerontology today as the world’s population ages and societies face growing resource demands created by these changing demographics. Rowe and Kahn (1987, 1997) were among the first scholars to propose a multidimensional model of SA with clear recommendations for its operationalization. Focused on objective indicators of good physical and cognitive health, high physical function, and productive and social engagement, theirs is a broad conceptual model of successful or healthy aging.
Despite extensive use of Rowe and Kahn’s model in recent decades and its emergence as “the gold standard” of SA definitions (Baker, Buchanan, Mingo, Roker, & Brown, 2015), it has drawn substantial criticism. Some critiques cite Rowe and Kahn’s disregard of individuals’ subjective assessments of their own functioning (Strawbridge, Wallhagen, & Cohen, 2002), while others voice concern about their emphasis on individual agency in achieving SA, at the neglect of social structural and institutional influences (Riley, 1998). Building on this latter criticism, Stowe and Cooney (2015) called for a broader life course examination of Rowe and Kahn’s model that moves beyond a static cross-sectional view of SA and includes structural and early life course influences, a suggestion recently promoted by Rowe and Kahn (2015).
In response, we draw on the life course perspective and nationally representative, longitudinal data to advance empirical testing of Rowe and Kahn’s SA model. Prior studies document a link between life course factors and aging outcomes; yet, most examine single later life health outcomes, rather than a multidimensional SA outcome as proposed by Rowe and Kahn (e.g., Luo & Waite, 2005; Montez & Hayward, 2014; Schafer & Ferraro, 2012). Still other studies use select samples (Pruchno, Hahn, & Wilson-Genderson, 2012; Pruchno & Wilson-Genderson, 2015; Pruchno, Wilson-Genderson, Rose, & Cartwright, 2010; Strawbridge et al., 2002), raising issues of generalizability. Although this literature is informative, an empirical analysis based on representative U.S. data with a broad set of life course predictors and Rowe and Kahn’s multidimensional SA formulation permits a stronger test of the life course critique of their specific model. In addition, assessing healthy aging outcomes across several critical dimensions of well-being simultaneously better informs public health planning. Identifying the portion of the population that has any of the risks to SA identified by Rowe and Kahn informs policy makers and program specialists of the need for some form of public intervention, whether that be, for example, enhanced medical care in response to disease or disability or social support in response to isolation. Estimates of overall need may be of value in resource planning.
We base our life course conceptualization for testing SA outcomes on the paradigmatic principles outlined by Elder, Johnson, and Crosnoe (2003). These principles emphasize aging as a lifelong process, contextually embedded in time and place, and shaped by both individual choices and social circumstances. This perspective also promotes a view of development and aging that captures the influence that significant others and their life course progress play in one’s life—known as the “linked lives” principle (Elder et al., 2003). The analytic approach we use to apply these tenets in analyses of SA transitions allows us to evaluate the relative influence of social structural factors, early childhood experiences, adult attainments, and later life health behaviors. By sequentially modeling these influences, we gain useful new insights into the potential modifiability of SA trajectories in later life—something Rowe and Kahn (1997) emphasized as possible through individual actions. If fixed structural factors and early childhood experiences have protracted effects on SA outcomes in later life, a different set of policy considerations and interventions are called for than if SA outcomes are primarily the result of adult attainments and experiences, and later life lifestyle behaviors. Thus, our findings may offer valuable new insights to inform discussion of the timing and focus of potential interventions.
Background
Rowe and Kahn’s (1997) SA model was intended to reflect “better than average” aging, with a goal of shifting discussions of aging away from decline and disease-oriented misconceptions of aging to the aging process itself. In their model, SA required individuals to be absent of chronic disease (recent studies add severe depression), display high physical (i.e., no limitations of daily living and few mobility restrictions) and cognitive function, and be socially and productively engaged (via work, volunteering, or care roles). Although Rowe and Kahn originally acknowledged genetic and other intrinsic influences on SA, the contribution of such factors and larger macrostructural forces was downplayed by their claim that “many of the predictors of risk and of both functional and activity levels appear to be potentially modifiable, either by individuals or changes in their immediate environments” (p. 439). Our application of a life course approach to predicting transitions from SA permits evaluation of such claims, which though highly criticized have been put to limited testing.
A Life Course Approach
The life course approach views development as unfolding over time, influenced by accumulating life experiences, changing historical conditions and events, and social institutions and policies. Both predictors of development and aging outcomes are considered fluid and ideally viewed over time and place. Therefore, we use longitudinal methods with both stable and time-varying predictors to assess influences on SA transitions over mid-to-late adulthood.
Two important studies of Rowe and Kahn’s SA model employ longitudinal data from nationally representative samples to establish the prevalence of SA at the national level and across recent time. Using Health and Retirement Study (HRS) data, McLaughlin, Connell, Heeringa, Li, and Roberts (2010) established that 12% of U.S. adults, 65 years and older, met Rowe and Kahn’s criteria (including a criterion of no serious depression) for SA. Furthermore, they reported that from 1998 to 2005, the odds of SA declined in the United States. Hank (2011) conducted a comparable study of European older adults using the Survey of Health, Ageing, and Retirement in Europe (SHARE) data, which includes samples from 14 European countries. His analysis provided a “place” contrast between the United States and Europe, as well as between the 14 SHARE nations, which differ in welfare state policies and income inequality. Hank revealed an overall SA rate of 8.5% in this European sample, though rates ranged from 1.6% in the Polish subsample to 21.1% for the subsample from Denmark. Both studies examined a limited set of predictors of SA outcomes as their main purpose was to establish national prevalence estimates of SA. Therefore, although the current study uses data from the HRS as did McLaughlin’s group (we employ eight waves of data—four more than McLaughlin et al.), our analysis of life course predictors of SA is much broader than theirs and that of other research with U.S. representative samples to date. Our approach has the advantage of testing the influence of fixed structural factors (as they did), as well as determining their relative importance once childhood experiences, adult attainments, and current lifestyle behaviors are examined. This approach provides greater insights into the modifiability of SA outcomes in adulthood.
Taking a long view of aging
Most samples used in SA research include persons aged 65 years and older (Hank, 2011; McLaughlin et al., 2010; Strawbridge et al., 2002). A limitation of this approach is that health-compromising processes already in progress prior to old age may be overlooked (Schafer & Ferraro, 2012). Yet, a recent study using HRS data from 2008 to 2014 included adults as young as age 51 and found that the prevalence of SA, based on criteria similar to those of Rowe and Kahn’s model, was already as low as 19% for persons aged 51 to 64 (Mejia, Ryan, Gonzalez, & Smith, 2017). This result is useful for considering the timing of SA interventions. However, that study’s main goal was to introduce a new formulation of SA, conceptualizing Rowe and Kahn’s SA components as resources predictive of alternative aging outcomes, such as life satisfaction. Thus, it did not present a broad analysis of predictors of the classic SA outcome for this wider age range of adults, which we argue is still warranted given the model’s widespread use, as well as substantial criticism of it. Moreover, the criteria cutoffs which Mejia et al. applied for SA status were stricter than those used in the current study and in McLaughlin et al.’s analyses. Hence, looking at SA outcomes and their predictors somewhat earlier in adulthood and using the standard Rowe and Kahn formulation is informative and adds evidence for weighing the value of the original SA model.
In addition, investigations into SA, whether applying Rowe and Kahn’s original model or a modified approach, rarely consider early childhood influences. Researchers typically focus on factors such as income and education—accomplishments achieved in adulthood (Hank, 2011; McLaughlin et al., 2010; Pruchno & Wilson-Genderson, 2015; Pruchno et al., 2010; Strawbridge et al., 2002). This emphasis on adulthood ignores the growing body of evidence that aging is “shaped by a host of factors that cumulate in individuals over decades of living” (Dannefer & Settersten, 2010, p. 3). For example, childhood health contributes to health outcomes in later life, in part due to its impact on education and income attainment in adulthood (Luo & Waite, 2005). Neglect of childhood conditions in studies of SA may result in overestimation of the significance of mid-to-late adulthood factors, erroneous causal conclusions, and suggested interventions that are unlikely to be fully effective. Thus, by including fixed social structural characteristics and factors that can be characterized as aspects of linked lives—some of which are present at birth or experienced in early childhood—this study better evaluates Rowe and Kahn’s (1997) initial claims regarding the modifiability of key risk factors for SA, and the importance of individual behaviors in achieving SA (Kahn, 2002).
Linked lives as an influence on aging
Acknowledging the interconnectedness of lives in how others influence one’s own development is a key aspect of the life course perspective. Life experiences often are based in one’s family and the product of family relationships or circumstances, especially those present in early childhood. Indeed, research reveals how such unfavorable early family experiences as parental loss or abuse (Schafer & Ferraro, 2012) or economic strain (Luo & Waite, 2005) predict health outcomes such as chronic disease (Schafer & Ferraro, 2012) and mortality (Montez & Hayward, 2014) in mid-to-late adulthood.
Beyond personal interactions and shared living circumstances, family influences also may be transmitted prior to birth, through genetics, and prenatal experiences and conditions (Ferraro, Pylypiv Shippee, & Schafer, 2009). Substantial family resemblance exists with regard to longevity (Glatt, Chayavichitsilp, Depp, Schork, & Jeste, 2007), for example, and genetics play a significant role in chronic disease (one component of SA) among older adults (Harris, Pedersen, McClearn, Plomin, & Nesselroade, 1992). Disease in later life also is associated with maternal health during pregnancy; Painter and colleagues (2006) revealed a significant link between malnutrition in pregnant Dutch women during World War II and coronary artery disease in their adult offspring decades later. Thus, a life course view of SA must include early childhood predictors, many of which result from family connections and circumstances.
Aging as influenced by social circumstances and individual choice
Another major tenet of the life course approach is that individuals make choices in their lives that actively shape their development, but these choices are influenced by socially structured constraints and opportunities—a process referred to as “agency within structure” (Settersten, 2003, p. 30). The key socially constructed categories that influence individual agency include sex, social class, race, and ethnicity. These structural factors are tested as predictors in most studies of SA (Hank, 2011; Kok, Aartsen, Deeg, & Huisman, 2017; McLaughlin et al., 2010; Mejia et al., 2017; Pruchno & Wilson-Genderson, 2015; Pruchno et al., 2010) and their influence is highly consistent. Generally, groups possessing lower social status (e.g., minorities, females) are disadvantaged in their pursuit of SA, just as Riley (1998) speculated in her critique of Rowe and Kahn’s model for ignoring social inequalities that jeopardize SA.
Despite inclusion of social circumstances and adult socioeconomic factors as predictors in most SA studies, research using longitudinal analyses of representative samples and applying Rowe and Kahn’s model is limited in examination of individual choices and lifestyle influences. Neither Hank (2011) nor McLaughlin et al. (2010) examined any prior adult or current behaviors, which limits the understanding of how individual actions are associated with social structural factors in predicting SA, as well as their relative influence on SA after considering social structural and childhood predictors. Strawbridge et al.’s (2002) analyses had similar shortcomings, failing to present any multivariate estimates of SA that included social structural predictors. Because Rowe and Kahn (1987, 1997) emphasized older adults’ behavior in their achievement of SA, it is critical to test such behaviors along with both social structural factors and early life course experiences.
Studies using alternative conceptualizations of SA find that aging outcomes are shaped by social structural factors as well as early life course experiences and current behaviors (Britton, Shipley, Singh-Manoux, & Marmot, 2008; Pruchno & Wilson-Genderson, 2015; Pruchno et al., 2010). Based on a large New Jersey sample, Pruchno’s group revealed that objective SA ratings were significantly influenced by structural factors like race, as well as such adult experiences as educational attainment and incarceration, and current behaviors including exercise, drinking (Pruchno & Wilson-Genderson, 2015; Pruchno et al., 2010), and smoking (Pruchno et al., 2012). One interesting result that speaks to the modifiability of risk comes from their 2012 study on smoking. Not surprisingly, they found a higher likelihood of SA (using a more relaxed definition than Rowe and Kahn’s) among nonsmokers than smokers, but no overall difference in likelihood of SA between current and past smokers. This offers some evidence of the importance of life course behaviors and the relative influence of structural factors in relation to early and concurrent experiences. Yet, their use of a single state sample and a less stringent definition of SA call for further empirical testing, which the current study provides.
Study Hypotheses
The current study advances research in several ways. First, it draws on eight waves (over 14 years) of U.S. nationally representative data for adults over age 50 to study transitions out of SA. Second, its inclusion of a broad set of early life course experiences and adult attainments as predictors, along with key social structural factors and later life behaviors, permits a stronger test of Rowe and Kahn’s SA formulation than what exists to date. Finally, sequentially modeling these sets of influences on transitions out of SA allows for clearer testing of the relative importance of each set, and stronger evaluation of the past debate concerning the role of individual versus structural factors in SA outcomes. Based on prior research, we pose the following hypotheses:
Method
Data
To examine transitions from SA to nonsuccessful aging (NSA), we used data from the HRS, conducted by the University of Michigan (grant number NIA U01AG009740). The HRS focuses extensively on retirement processes, economic issues, and health, with data collected approximately every 2 years, beginning in 1992, using a “multi-stage, area-clustered, stratified sample” probability design (Ofstedal, Weir, Chen, & Wagner, 2011, p. 3). Sampling weights make it possible to generalize from these data to noninstitutionalized individuals above age 50 who live in the contiguous United States.
This study used the raw HRS data for 1998-2012, merged with the cross-wave census region/division and mobility files (Final V6.1) and Version O of the streamlined, longitudinal HRS files prepared by RAND Corporation (Chien et al., 2015). We set 1998 as our baseline as it was the first survey year to include questions about respondents’ childhood conditions, which are key to our life course analysis. There also was more stability in inclusion and wording of key variables required for our analyses beginning with the 1998 wave. Survey response rates ranged from 81% in 2010 to 89% in 2012 (HRS Staff, 2017).
Our analytic sample drew from the population of HRS primary respondents (no proxy responses) who participated in the 1998 wave and were above age 50. A total of 12,108 respondents met these criteria and had full data required to construct our NSA outcome variable. The 1998 baseline analytic sample ranged from 51 to 105 years old, with an average age of 65.03. Females comprised 52.5% of the weighted sample; 6.1% of respondents reported Hispanic origin, and 10.4% reported race as Black. Table 1 presents descriptive statistics (using imputed data) on the analytic variables for respondents assessed as SA and NSA at the 1998 baseline.
Comparison of Respondents (N = 12,108) Assessed as Nonsuccessfully and Successfully Aging at Baseline (1998).

Note. Based on weighted imputed data, described by means (standard error) and percentiles. Percentiles may not equal 100 due to rounding error.
Variables
Dependent variable
Consistent with Rowe and Kahn’s (1997) SA conceptualization, we created a dichotomous variable to represent NSA based on seven criteria related to disease, disability, physical functioning, mental health, cognitive ability, social involvement, and productive engagement. This dependent variable iterated from 0 to 1 to indicate a transition out of SA to NSA, if and when over the course of the eight waves the respondent failed to meet any of the following seven required SA conditions. For disease, SA respondents could not report any of the following doctor-diagnosed major diseases: cancer, lung disease, stroke, diabetes, or heart problems. Regarding mental health, respondents had to report fewer than five of eight depressive symptoms from the short version of the Center for Epidemiologic Studies Depression Scale (Radloff, 1977) to meet SA status. Cognition was assessed using immediate and delayed recall tests of memory, a serial 7s subtraction test of working memory, and counting backward to assess attention and processing speed (Chien et al., 2015), resulting in a scale range of 0 to 27. Respondents who scored higher than 11 met the SA criterion for cognition. A SA classification for disability required that respondents reported no activities of daily living (ADL) limitations (e.g., difficulty bathing), and for the physical functioning component, they had to report no more than one mobility limitation (e.g., difficulty climbing a flight of stairs). For the SA social engagement dimension, respondents were required to report at least one of the following types of engagement: living with a spouse/partner, having good friends living nearby, or getting together with neighbors at least once a week for a chat. For the SA productive engagement criterion, respondents had to report at least one of these activities: formal volunteering in the past 12 months, current paid employment, providing care for grandchildren, or providing care for a parent.
Independent variables
We assessed life course predictors of SA in four domains.
Social structural characteristics
Several time- invariant social characteristics believed to shape respondents’ life course opportunities and experiences were included. Ethnicity was based on respondents’ reports of being Hispanic or Latino (1 = Hispanic, 0 = non-Hispanic). Race, dichotomized as Black–non-Black (1-0), referred to respondent’s reported primary racial identity. (Respondents not reporting either Black or White race were omitted due to small numbers.) Sex was coded as female–male (1-0). Age of the oldest parent (currently alive, or at death if no longer living at baseline) was used as an indicator of family longevity, given strong family resemblance in survival. We consider these factors to be “set” for respondents at birth, and thus largely beyond their control. The baseline model also included respondent’s age in years, calculated from the date of birth, and interview date for each wave.
Childhood experiences
Included among our indicators of childhood context and experiences were childhood health and economic adversity. Following studies of later life health outcomes using the HRS data (Luo & Waite, 2005; Montez & Hayward, 2014), we constructed a childhood health variable based on the following question: “Consider your health while you were growing up, before you were 16 years old. Would you say that your health during that time was excellent, very good, good, fair, or poor?” Like Montez and Hayward, we dichotomized responses into poor health (=1), including fair or poor responses, versus better health (=0), including responses of good to excellent health.
Childhood financial adversity represents an index also adopted from Montez and Hayward (2014). The original 0 to 6 index counts negative financial indicators in childhood reported by the respondent (father’s absence during childhood, mother’s education less than 8 years, father’s education less than 8 years, perception of the family as financially poor, experiencing financial difficulties that caused the family to move, receiving help from relatives because of financial difficulties). As others suggest (Luo & Waite, 2005; Montez & Hayward, 2014), missing data on parent education were recoded as less than 8 years. Also, using Montez and Hayward’s approach, we top-coded the index to a score of 5 due to few cases having scores of 6. These two childhood variables were modeled as time- invariant.
Adult attainments
Several variables depicted respondents’ socioeconomic attainments in adulthood. Education was dichotomized (1 = at least some college; 0 = less than high school, General Education Diploma, or high school graduate), and modeled as time- invariant predictor based on 1998 survey responses. The remaining indicators of adult attainments were time-varying and assessed at each wave. Household income consisted of all sources of income for both the respondent and spouse/partner for the past calendar year. Due to the nonlinear distribution of income and its skew even after transformation, an ordered categorical variable was created depicting income quartiles within the sample at each wave. A dummy variable reflecting negative assets (1-0) was also created to capture a form of economic hardship other than low income, as stress associated with debt may present added health risks (Thoits, 2010). Assets included the sum of all assets, excluding secondary residence, for the respondent and spouse/partner; cases with values below 0 were coded as having negative assets (=1).
Place of residence was determined from the respondent’s region of residence at each wave to capture context and environmental circumstances that shape health behaviors, health care access, and utilization (Waidmann & Rajan, 2000). Based on HRS supplied U.S. Census Bureau geographic divisions for place of residence, we created a dummy variable (1-0) reflecting residence in the South (=1) versus all other regions for each wave. The U.S. Census Bureau (2012) reports the Southern region to have the lowest median household income, and highest poverty rate and rate of uninsured individuals in the population. Others note poorer self-reported health and lower likelihood of an identified “usual” health care source for Southern residents (Waidmann & Rajan, 2000). Thus, we expected an elevated risk of NSA for respondents in the South.
Current lifestyle behaviors
The final component of our life course analysis focuses on current behavior, considered the most amenable to modification in later life. Body mass index (BMI) was computed by RAND Corporation using a formula based on respondent weight in kilograms divided by height in meters squared. Because health risk associated with BMI does not appear linear, we compare three groups: underweight and normal BMI (BMI < 25), overweight/obese (BMI ≥ 25 and <35), and severely obese (≥35). Among the benefits of being on the low end of overweight (i.e., middle group) are reduced ADL risk (Al Snih et al., 2007), and less incapacity and greater mobility (McClintock, Dale, Laumann, & Waite, 2016). BMI was assessed at each wave, as was smoking status. For the latter, respondents were asked about their current smoking status, as well as about prior smoking. We coded this time-varying smoking variable as never smoked (=0), previously smoked (=1), and currently smoke (=2). The analyses compared prior and current smoking with never smoking as a risk for NSA.
Missing Data
Missing data were assessed prior to modeling. Nearly all study variables had valid data for 99% of the cases. The variable depicting childhood financial adversity was missing data for 13% of the respondents, with those cases overrepresented by minority group respondents and those with lower adult attainments. We used STATA’s “mi impute” program to impute missing values for model covariates using the chained-equations method. Equations for each covariate included time- invariant baseline measures (plus two auxiliary measures—the Beale rural–urban continuum codes for place of residence and whether the respondent’s father was unemployed during childhood), as well as time-varying measures for all waves. The resulting 10 sets of complete data were combined to adjust for variance within and between imputed samples to calculate standard errors and coefficients (Acock, 2005).
Analytic Plan
We tested our hypotheses using discrete time event-history methods (Allison, 1984). These allow for the maximization of longitudinal data, incorporating both time- invariant and time-varying predictors. We estimated the dichotomous dependent variable, NSA, reflecting NSA status (1-0). The event-history analyses included all waves of relevant data for a respondent up to, and including, the wave in which that individual’s dependent variable value first indicated NSA = 1. For respondents lost to the survey over time, the estimated models included all waves of their completed data. Thus, each respondent contributed from one to eight waves of data. Each wave of data a respondent provided represented a case in the event-history data file, which included all of that respondent’s time- invariant data (e.g., race, sex), as well as the time-varying predictors (e.g., age, negative assets, BMI) for each specific wave, and the dependent variable, NSA, at that wave. The 12,108 eligible respondents at the 1998 baseline survey thus contributed 24,230 observations to the event-history data file.
A logit maximum-likelihood technique was used to estimate the models given a dichotomous dependent variable. We sequentially estimated three models of NSA to evaluate the significance of the various life course factors. Model 1 tested social structural conditions and childhood factors, addressing Hypotheses 1 and 2. To test Hypothesis 3, Model 2 examined how adult achievements contributed to NSA, and potentially mediated the early influences and social structural conditions previously tested. Model 3 examined how current lifestyle behaviors further shaped NSA, addressing Hypothesis 4. Furthermore, this final model provides evidence to test Hypothesis 5 regarding the continued influence of social structural factors once adult experiences and concurrent behaviors are controlled.
To assess the extent to which early childhood and fixed structural influences on transitions out of SA are mediated by adult experiences and attainments, and later life behaviors, these predictors of NSA require comparison across our nested models. However, coefficients in sequential logit models change from one model to another not only because of the original predictors’ association with newly introduced mediating variables—what Karlson, Holm, and Breen (2012) call confoundings—but also because of rescaling that occurs with the subsequent models due to differences in each model’s error variance (Karlson et al., 2012). Thus, to assess the extent to which early childhood experiences and structural factors are mediated by adult accomplishments and later life behaviors, we apply the KHB method developed by Karlson and colleagues, using their STATA add-on program (see Kohler, Karlson, & Holm, 2011). This approach results in logit coefficients that are measured on the same scale for the full (mediated) and reduced (prior) models. In addition, the procedure produces estimates of the percentage change in each coefficient from the reduced to the full model due to confounding, or the mediation of the newly introduced variables (Kohler et al., 2011). Our presentation of the multivariate results lists the logit coefficients and odds ratios (ORs) for the variables in each model, plus the percentage change in each predictor due to confounds (the variables added in the full model). In sum, this provides a means of assessing mediation by the subsequent life course factors that we introduce in sequential nested models.
The KHB program does not accommodate multiple imputed data sets, so we conducted the analysis on a subset of our 10 imputed data sets. We selected three data sets to analyze that represented low, average, and high estimates of our key independent variables (variation was extremely limited across these imputed datasets). The logistic regression results from the KHB program were highly comparable across the three datasets; in nearly all cases, coefficients for a given predictor variable were essentially the same, up to two decimal places, across datasets. Our multivariate table reports results from the dataset producing the most conservative estimates.
Results
To begin, we calculated the percentage of respondents at baseline that met SA status. This rate is important because our sample included a wider range of adults than past studies, and was based on nationally representative data. Weighted data revealed that 26.2% of the 1998 baseline sample, aged 51 years and older, met the SA criteria.
One analytic goal was to consider a fuller range of life course predictors of NSA than prior studies. In Table 2, Model 1 reveals the strong influence of social structural and early childhood factors on an NSA determination; all of the examined predictors in Model 1 reached statistical significance. The strongest influences among the structural factors were associated with race and ethnicity. ORs indicate that being of Hispanic background and of Black race were associated with a 68% and 90% increased likelihood, respectively, of respondents transitioning to NSA (i.e., OR = 1.68 and 1.90, respectively). Regarding the variable for sex, the chances of transitioning to NSA were 39% higher for females than males. In addition, financial adversity experienced in childhood and poor childhood health significantly raise the risk of NSA transitions; the increased likelihood of an NSA designation associated with poor versus good or better childhood health was 74%. Finally, the advantage of good genetic make-up for SA is evident, with parental longevity associated with a significantly reduced likelihood of transitioning into NSA (an added year of parent survival predicted a 2% drop in the odds of NSA). Thus, Model 1 documents the importance of structural factors in shaping aging outcomes, consistent with Hypothesis 1. Furthermore, it provides support for Hypothesis 2 as it demonstrates that childhood disadvantage has a long reach in predicting NSA outcomes later in adulthood.
Logistic Regression Models Predicting Transitions From Successful to Nonsuccessful Aging Status.
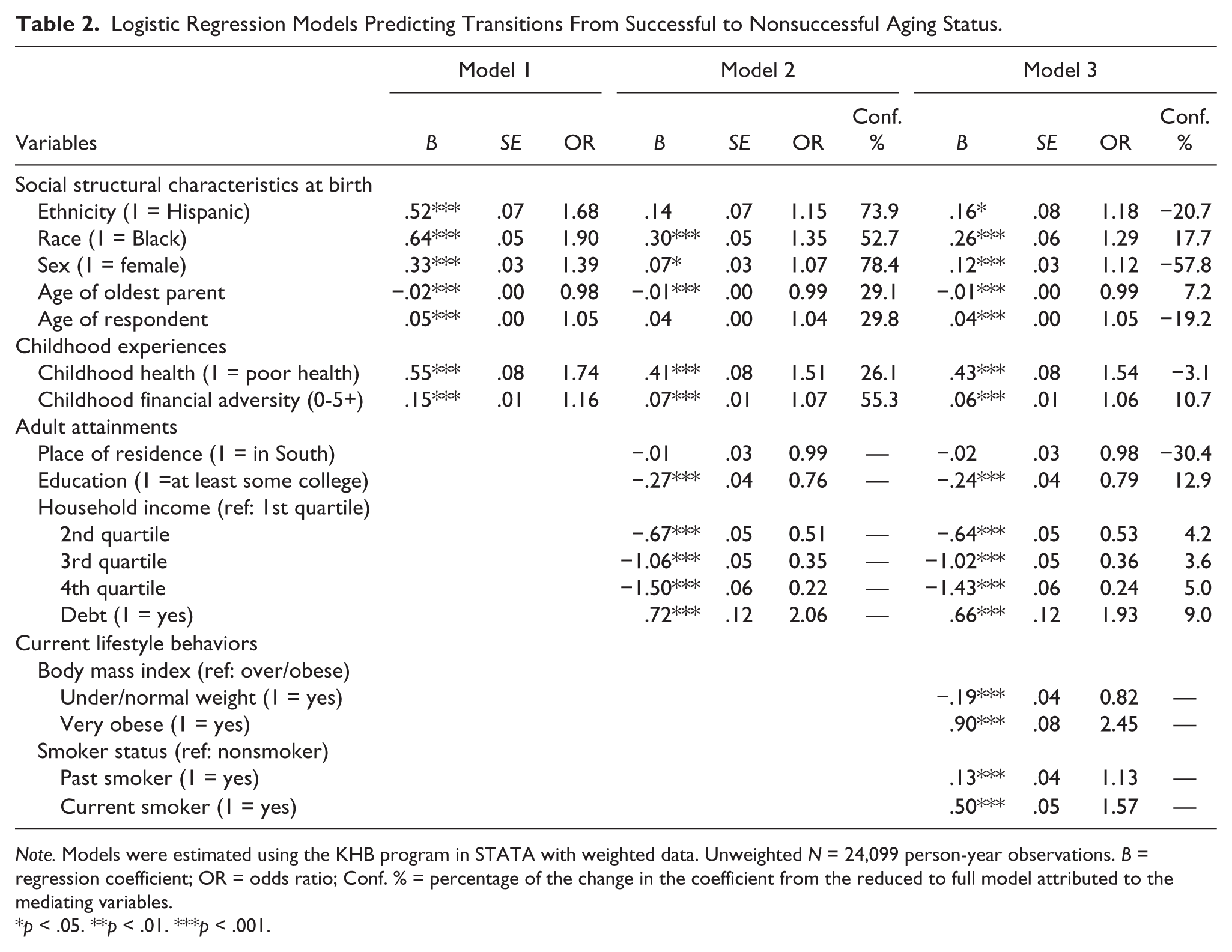
Note. Models were estimated using the KHB program in STATA with weighted data. Unweighted N = 24,099 person-year observations. B = regression coefficient; OR = odds ratio; Conf. % = percentage of the change in the coefficient from the reduced to full model attributed to the mediating variables.
p < .05. **p < .01. ***p < .001.
Model 2 estimated the NSA outcome by adding educational attainment and adult time-varying achievements to the Model 1 predictors. This model tested the sustained influences of structural conditions and early experiences once mediation via adult achievements was considered. All but one (residence in the South) of the adult achievements and experiences significantly predicted NSA, and all in the expected direction. Higher educational attainment and economic achievements were significantly predictive of respondents’ transitions to NSA status. Although education beyond high school predicted a 24% reduction in respondents’ odds of an NSA transition, having negative assets doubled their odds of experiencing a NSA transition. The import of respondents’ income was also sizable, with those in the second lowest income quartile having a 49% lower odds of NSA than the poorest respondents, and those in the highest quartile having a 78% reduced odds of an NSA transition.
In examining changes in the coefficients and ORs for the structural factors and early childhood conditions from Model 1 to 2, and the percentage of those changes due to confounding (or mediation), several important findings stand out for Model 2. Hispanic background is no longer significant in Model 2, with the added odds of NSA for Hispanic versus non-Hispanic respondents dropping to just 15% once mediators are introduced. The majority (74%) of the change in coefficients for ethnicity from Models 1 to 2 was accounted for by the adult achievements added in Model 2. This set of mediators accounted for a similar change in the influence of sex on NSA; yet, being female continued to be associated with significantly elevated odds of NSA. Similarly, the influence of race on NSA was dramatically reduced in Model 2, but remained significant after accounting for adult achievements (they contributed to ~53% of the drop in influence of race from Model 1 to 2). Finally, adult attainments strongly mediated the influence of negative childhood circumstances as well, though they did not fully eliminate the protracted influence of childhood health and financial disadvantage on NSA. In sum, findings from Model 2 provide support for Hypothesis 3 that adult attainments do partially mediate the influence of childhood disadvantage and structural factors on NSA outcomes; yet, they do not nullify their significant effects.
Model 3 added respondents’ current lifestyle factors, indexed by BMI and smoking behavior, to the prediction of NSA. The influence of lifestyle behaviors is evident by the strength and significance of these predictors, supporting Hypothesis 4. Both past and current smokers had significantly elevated odds of NSA relative to nonsmokers, though the risk was about 3 times greater for the latter group. Regarding BMI, the results show its strongest impact on NSA transitions for respondents who are very obese, followed by somewhat reduced, though significant effects for those in the overweight/obese category, relative to respondents who are underweight or of normal weight.
The results for Model 3 revealed very limited mediation of social structural factors, and early and adult experiences, via current lifestyle behaviors, as shown by the figures reported in the column for confounding percentage. Only in the case of sex is there a sizable percentage of confounding attributable to lifestyle, and in this case, in the form of a suppressor effect. These findings provide evidence in support of Hypothesis 5, substantiating the persistent significant influence of social structural factors and childhood experiences, even after accounting for subsequent adult experiences and current behaviors.
Discussion
This study empirically tested a life course model predicting transitions from SA to NSA for a representative U.S. national sample of adults above age 50. The study permits a rigorous assessment of claims as to the modifiability of SA outcomes in later life that were originally made by Rowe and Kahn (1997; Kahn, 2002). It also provides stronger empirical evidence of the relative importance of a wider set of life course factors—including social structural characteristics and childhood experiences, adult attainments, and current adult behaviors—for SA transitions in late adulthood, for a representative sample.
Consistent with prior research (McLaughlin et al., 2010; Pruchno et al., 2012), our baseline models, which also included childhood experiences, found highly significant risks of NSA for females compared with males, Blacks compared with non-Blacks, and persons of Hispanic versus non-Hispanic origin. Our findings are especially noteworthy because subsequently estimated models that included adult attainments—mostly related to resource acquisition (e.g., higher education, income)—revealed substantial reductions in the influence of these fixed social characteristics. In fact, after controlling for adult attainments, one of them—Hispanic background—was no longer a significant predictor and the risk for NSA associated with race dropped by more than half, and that for sex by even more. Moreover, over half of these reduced effects were clearly attributable to the mediation of these adult attainments. These findings speak to critique of Rowe and Kahn’s original claims that SA is largely a result of individual agency and behavior, which downplayed the role of social structural constraints (Riley, 1998). Granted, individual pursuits and adult accomplishments do matter according to our results, as they substantially attenuated disadvantage associated with race and sex, and eliminated the significance of ethnicity. Yet, the fact that adult resource attainment did not fully account for the influence of race and sex on NSA transitions suggests the intractability of discrimination and inequality in opportunities (e.g., jobs offering good benefits and pensions), and access for minorities and women. With regard to race and ethnicity, in 2003, the Institute of Medicine (IOM) documented significant inequalities in medical care. Minorities, for example, are less likely than non-Hispanic Whites to receive needed medical procedures and services, controlling for key demographic factors. Some of the racial and ethnic inequalities in treatment appear to result from implicit biases on the part of health professionals (Hall et al., 2015), which are difficult to confront and change. In addition, SA may be jeopardized by the stress experienced by these groups as a result of persistent discrimination (Thoits, 2010). Thus, although adult actions such as seeking advanced education and achieving higher earnings appear important for SA, as Riley (1998) argued over 20 years ago, social structural and institutional forces still come into play. Our results illustrate the idea of “agency within constraint” (Settersten, 2003) uniquely captured by the life course perspective.
The limits of adult attainments in shaping risk for NSA also are important to consider given persistent, significant influences of childhood adversity well into later adulthood. Both poor childhood health and early family economic problems presented significant risks for NSA, even after considering adult attainments. These findings lend support to earlier work suggesting that childhood disadvantage likely impacts aging outcomes directly through influences on developing physiological processes, as well as indirectly by influencing adult attainments (Graham, 2002; Luo & Waite, 2005), though only one quarter of the reduced impact of childhood health in our mediated models was attributed to adult attainments. Thus, although these results (and those of Hank, 2011) highlight the merit and potential of international public health efforts aimed at reducing socioeconomic differentials to combat adult health inequities (Graham, 2002), the persistent influence of early childhood experiences in our models also highlights the import of directly meeting the needs of at-risk young children. Although some may spin related policy decisions and program priorities as generational conflicts pitting the needs of young and old (Escobedo, 2014), our life course analysis suggests that investments in child well-being may substantially contribute to healthy aging for future cohorts of older adults.
An important contribution of this study was assessment of how current lifestyle behaviors impact older adults’ risk of NSA, given claims by Rowe and Kahn (1997; Kahn, 2002) that SA is modifiable and under the control of older adults. Our results indicated that indeed, greater BMI and smoking—both current and previous—significantly increase the risk of NSA. In contrast to what some literature suggests (Al Snih et al., 2007; McClintock et al., 2016), we did not find SA benefits for respondents at the low end of overweight on the BMI continuum. This could be because NSA status is a composite of several health risks; although those who are overweight may have a reduced likelihood of ADLs relative to those who are underweight (Al Snih et al., 2007), for example, being overweight is associated with increased numbers of comorbidities (Must et al., 1999). Thus, overall, we assume that behavioral modifications aimed at reducing overweight and obesity may somewhat reduce NSA risk.
The results regarding smoking also reflect the benefits to SA that smoking cessation may provide, as the risk of NSA was substantially greater for current smokers than former smokers, in comparison with nonsmokers. This finding contrasts with that of Pruchno et al. (2012) who found no difference in SA outcomes for current versus former smokers. However, their models also controlled for the amount individuals smoked in their lifetime, which may account for some of influences attributed to the current–former smoker differences in our model.
Overall, though lifestyle behaviors that individuals have control over do influence their SA classifications, as Rowe and Kahn argued, current behaviors in later adulthood do not eliminate the powerful, significant influence that social structural factors and early life course experiences have on SA. Because many of these fixed statuses and early experiences are not under the control of older adults, it is important to avoid blaming older adults for NSA status and to limit expectations as to how much interventions applied only in mid to later life may impact SA status. Although interventions like smoking cessation and weight management programs should not be abandoned, there is need for multipronged approaches to enhance SA. These methods must include policies to reduce socioeconomic inequalities and related health disparities (Graham, 2002; IOM, 2003), and address prejudice and discrimination that limit opportunities, elevate stress (Thoits, 2010), and add to life course risks (Graham, 2002).
Although this study provides new and valuable findings regarding life course influences on SA, and the relative importance of social structural factors, childhood and adult experiences, and later adult behaviors on transitions from SA to NSA, it has some limitations. One shortcoming is limiting current adult behaviors to just BMI and smoking. Unfortunately, investigating the influence of additional established lifestyle indicators, such as regular exercise, was impossible, given inconsistent measurement of this item over the eight waves of HRS data we analyzed. Adding more indicators of current behavior may somewhat reduce the impact of earlier life course factors, though the strength of their influence is such that we would not expect it to be eliminated. The high percentage of missing data for our childhood financial adversity variable is also a concern, and the bias it revealed. Although we have confidence in our imputed data, we are reserved in our individual claims about this financial adversity variable. Also of note is that we approached our research regarding influences on transitions from SA to NSA by modeling a single, nonreversible status transition as the dependent variable. The reversibility of transitions from SA to NSA is worthy of future examination, as is further testing of predictors of alternative, nonbinary conceptualizations of SA, such as that proposed by Mejia et al. (2017). Now that the classic binary SA classification proposed by Rowe and Kahn has been subjected to this broader, more rigorous test of their initial claims, these alternative approaches deserve further attention and testing.
In conclusion, this study offered valuable empirical testing of Rowe and Kahn’s SA model, which was overdue, given loose application of their criteria in past studies and limited testing with representative, longitudinal data. This life course analysis also advances the literature by addressing the relative importance of various structural factors, childhood experiences, adult attainments, and lifestyle behaviors in shaping SA, which has been missing from this literature. Finally, the findings provide solid evidence for disputing Rowe and Kahn’s initial claims emphasizing older adults’ control over SA, and support for critiques that underscore the need to recognize persistent social structural influences on SA. Such evidence is valuable to consider in future debates about the utility of this model for research, policy, and practice.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.