
Abstract
Introduction
As America ages, an increasing number of older adults with chronic illness and disability will rely on informal caregivers (i.e., family and friends) for assistance (Centers for Disease Control and Prevention, 2016). Thus, informal caregiving has become a major focus of research, clinical work, and public policy over the past decades. It has been well documented that informal caregivers provide substantial care for disabled older adults (Reinhard, Feinberg, Choula, & Houser, 2015; Wolff, Spillman, Freedman, & Kasper, 2016), and that caregivers face many stressful challenges that can cause financial strain, psychological distress, and possibly adverse health consequences (Chari, Engberg, Ray, & Mehrotra, 2015; Wolff et al., 2016). There is also increasing research suggesting that many caregivers are resilient, with substantial numbers experiencing little distress and even psychological and health benefits from caregiving (Bertrand et al., 2012; Fredman, Cauley, Hochberg, Ensrud, & Doros, 2010; Fredman, Lyons, Cauley, Hochberg, & Applebaum, 2015; Roth, Fredman, & Haley, 2015).
Although the literature on family caregiving has developed substantially, important gaps remain in our understanding of the caregiving experience. One important area is the study of racial and ethnic differences in informal caregiving, as the older adult population is expected to become more diverse with more than half of Americans estimated to identify as being a member of a minority group by 2044 (Colby & Ortman, 2015).
Racial and ethnic differences in caregiver stress, well-being, and service use received major attention in early years of caregiving research. In particular, differences between White and African American caregivers were analyzed, and these initial results were summarized in a review by Dilworth-Anderson, Williams, and Gibson (2002) and in a meta-analysis by Pinquart and Sörensen (2005). The two aforementioned reviews concluded that African American caregivers often reported heavier caregiving demands and less psychological distress than White caregivers, despite being in generally poorer health and having lower education and income. However, there were no consistent racial differences in formal service use between White and African American caregivers. Both reviews noted that most research comparing White and African American caregivers suffered from serious methodological limitations, including the use of convenience samples, and failed to distinguish between care relationship types (e.g., caregivers of parents, caregivers of spouses). As a number of scholars have noted (Pinquart & Sörensen, 2003, 2005; Roth et al., 2015), convenience samples are not representative of the general population of caregivers and likely overrepresent caregivers who are highly distressed and seeking help. Population-based samples allow for the identification of representative samples of caregivers and may yield more generalizable results. Effect sizes for differences between depressive symptoms in caregivers and noncaregivers, for example, are much smaller in population-based studies of caregiving than in convenience samples (Pinquart & Sörensen, 2003; Pruchno et al., 2008). Caregiving research using population-based samples shows that the majority of caregivers report little or no strain (Roth et al., 2015), as opposed to research using convenience samples of caregivers who often report high levels of strain. Thus, to understand racial differences in caregiving, it is important to utilize population-based samples to avoid biases found in convenience samples of caregivers recruited from clinics, support groups, and advertisement.
Recent reviews addressing racial differences in caregiving have offered similar summaries. Capistrant (2016) summarized recent studies on caregiving and health and concluded that White, nonminority caregivers often report a more negative view of caregiving and may report more strain in comparison with ethnic or racial minority caregivers, like African American caregivers. Apesoa-Varano, Tang-Feldman, Reinhard, Choula, and Young (2015) reviewed research from 1980 to 2013 and, also, concluded that African Americans generally reported lower levels of burden and distress than White caregivers. However, neither of these reviews distinguished between results from convenience samples and population-based samples nor did they distinguish between care relationship types.
Caregivers’ risks are not uniform; some types of caregiving can be more stressful than others. For example, adult child caregivers (ACC) caring for an older parent is one of the most common forms of caregiving and has unique stressors and effects when compared with spousal caregiving (Gaugler, Reese, & Mittleman, 2015; Pinquart & Sörensen, 2011; Stephens, Townsend, Martire, & Druley, 2001). That is, while spouse caregivers may face higher stress and negative effects, recent research suggests that resilience, rather than negative effects, is a common outcome among ACC identified in population-based samples (Hansen, Slagsvold, & Ingebretsen, 2013). African Americans and White caregivers also differ in relationship types as African Americans, and other ethnic minorities, often have fewer spousal caregivers than White caregivers (Pinquart & Sörensen, 2011). Although very few population-based studies comparing White and African Americans across relationship types exist beyond what has been highlighted above, race and relationship type may also be important risk factors of caregiver stress. Dementia care is another risk factor, as caregivers of older adults with dementia often report greater strain than caregivers of cognitively intact older adults (Capistrant, 2016; Ory, Hoffman, Yee, Tennstedt, & Schulz, 1999).
Caregivers’ unique risks must be considered in analyses describing the impact of caregiving. As White and African American caregivers often vary substantially in demographic variables and in the amount of care they provide, it is important to include covariate-adjusted analyses when examining racial differences in strain and service use among caregivers (Dilworth-Anderson et al., 2002; Ory et al., 1999; Pinquart & Sörensen, 2005). Dementia care status is also important to include in analyses as dementia and nondementia caregivers may differ significantly in their types and amount of stressors and strain, and amount of care they provide.
The present study uses a population-based sample of caregivers and includes information on relationship type, dementia care status, demographics, caregiving stressors, and various dimensions of caregiving strain, health, and service use. The purpose of this study was to examine racial differences in caregiving across relationship type and dementia care status, using a nationally representative sample of White and African American caregivers of care recipients who were 50 years of age or older and community living. Based on the previous literature, which has been conducted almost exclusively in convenience samples, we predicted that African American caregivers would report more care responsibilities, lower distress, and poorer health. We also expected caregivers of older adults with dementia to report more distress than caregivers of cognitively intact older adults. Finally, we explored dementia care status and/or relationship type as potential moderators of the effects of race on strain, health, and service use. We accounted for demographic differences and indicators of caregiving stressors in all analyses to assure that the context of caregiving was appropriately considered and to identify possible mechanisms of any racial differences identified.
Method
Participants
Participants were interview respondents from the National Alliance for Caregiving and the American Association of Retired Persons’ (AARP) Caregiving in the U.S. 2015 data set. Of the 7,660 potential participants who were screened, 1,248 were self-reported caregivers and completed the interviews. Eligibility criteria for caregivers in our analyses included individuals aged 18 years or older who self-identified as either White or African American and were providing care at the time of the interview or within the previous 12 months to a community-dwelling family member or friend who was 50 years of age or older. Caregivers of spouses and partners were also excluded because, consistent with previous research (Pinquart & Sörensen, 2011; Siegler, Brummett, Williams, Haney, & Dilworth-Anderson, 2010), there were relatively few African American spouse caregivers in the sample (n = 13). From the 1,248 participants who completed interviews, 887 were eligible given our criteria and included in these analyses. The study participants included 697 White and 190 African American caregivers.
Procedure
Potential participants were selected at random through GfK’s KnowledgePanel® using telephone numbers and residential addresses to create a sample that is representative of the general U.S. population. Potential participants were invited by telephone or by mail invitation to participate in the interview. Those who agreed to be interviewed received an email with individualized log-in information to complete the online interview. GfK provided a free computer with a wireless Internet connection to participants who did not have access to either a computer or an Internet connection. Further details about the survey can be found at National Alliance for Caregiving (2015).
Measures
Demographic information regarding caregiver sex, age, income, education, and marital status was collected from survey participant self-report. Those who were currently caregivers reported on their current caregiving experiences, and those who had been caregivers over the past 12 months reported on their caregiving experiences during that period of time. Analysis suggested that adjusting for status as a current versus previous caregiver had minimal impact on the results and led to multicollinearity problems, so we did not include this as a factor in our analyses. In addition, we found that current versus prior caregivers did not differ significantly in relationship type and race. For analytic purposes, income was coded into two categories (below US$75,000 or US$75,000 or above), marital status was coded into two categories (married/living with partner or other), and education was coded into two categories (high school/less or some college/college graduate).
Race
Participants reported their race by answering the question, “Would you say you are White, Black/African American, Asian/Pacific Islander, or something else?”
Relationship type
The care recipient’s relationship to the caregiver was assessed through participant self-report. Participants were asked, “What [is/was] this person’s relationship to you? She/he is your _____?” Participants were then provided a list of various relationship types that were either relatives or nonrelatives. For the purpose of this study, the relationship type variable was recoded into three separate categories of care recipient: parent, other family, or friend.
Dementia care status
Dementia caregiving status was assessed from a composite variable created by AARP. The classification included any participant who indicated the presence of Alzheimer’s disease, dementia, or other mental confusion as the main condition or if the participant indicated the presence of the former conditions in a follow-up question (National Alliance for Caregiving, 2015).
Stressors
Caregiver activities of daily living/instrumental activities of daily living (ADL/IADL) assistance
A summary variable was produced by adding the count of ADL and IADL that participants reported assisting with. Participants were asked, “Which of these [do/did] you help your [relation] with . . . ?” The participants were then presented with seven different ADL (e.g., help bathing, dressing, or feeding; Katz, Ford, Moskowitz, Jackson, & Jaffe, 1963) and six different IADL (e.g., help with medication management, finance management, or transportation; Lawton & Brody, 1969). The internal reliability of the measure for the present study was .81.
Hours of care
Hours of care provided was assessed with the question, “Thinking now of all the kinds of help you [provide/provided] for your [relation] about how many hours [do/did] you spend in an average week, helping him/her?”
Duration of care
Caregiver duration of care was assessed by asking the participant, “How long [have you been providing/did you provide] care to your [relation]? Care duration was calculated from the number of years providing care that the participant reported.
Caregiver strain and health
Physical strain
Caregiver physical strain was assessed by asking the participant, “How much of a physical strain would you say that caring for your [relation] [is/was] for you?” Participants rated the degree of physical strain on a scale of 1 (not a strain at all) to 5 (very much a strain).
Emotional stress
Caregiver emotional stress was assessed by asking the participant, “How emotionally stressful would you say that caring for your [relation] [is/was] for you?” Participants were asked to rate the degree of emotional stress on a scale of 1 (not at all stressful) to 5 (very stressful).
Financial strain
Caregiver financial strain was assessed by asking the participant, “How much of a financial strain would you say that caring for your [relation] [is/was] for you?” Participants rated the degree of physical strain on a scale of 1 (not a strain at all) to 5 (very much a strain).
Health status
Caregiver health was assessed with the question, “How would you describe your own health?/When you were last caregiving, was your health . . . ?” Participants rated their current health as either excellent, very good, good, fair, or poor using a scale of 1 to 5, with higher ratings indicating better health. Previous research has reported that self-rated health is a valid measurement of health status (Mossey & Shapiro, 1982; Schnittker & Bacak, 2014).
Use of services
Service use
Participants were asked, “In your experience as a caregiver, have you ever . . . ,” and a list of six services was then presented to the participant. The six services included financial help, respite services, transportation, modifications to residence, health provider inquiry about care recipient needs, and health provider inquiry about caregiver needs. A sum of the services used was calculated to obtain the total service use for each participant.
Statistical Analyses
Statistical analyses were performed using the Statistical Package for Social Sciences software, version 23.0 (SPSS Inc., Chicago, IL). Primary analysis showed no duplicated cases of data in the data set. Missing data for hours of care, caregiver ADL/IADL assistance, physical strain, emotional stress, financial strain, caregiver health, duration of care, and service use were handled using the SPSS multiple imputation module. Multiple imputation consisted of three steps: first estimates of missing data were generated, then 20 iterations of imputed data sets were analyzed, and finally data were pooled to obtain results (van Burren, 2007). Descriptive and demographic data were then analyzed. Then, 3 (parent, other family, friend) × 2 (White or African American) factorial logistic regression tests were conducted to determine if there were any significant main effects or interactions on demographic variables. For logistic regression analyses, income and education were each dichotomized for analytic purposes. Also, 3 (parent, other family, friend) × 2 (White or African American) ANOVA tests were conducted to compare all continuous variables such as caregiving stressors including hours of caregiving, duration of caregiving, and caregiver assistance provided. Preliminary analyses showed that the single-item indicators of caregiving strain did not have problems with skewness and kurtosis, and that they were appropriate to analyze using ANOVA according to criteria presented by Hu and Bentler (1999). Finally, Pearson correlational analyses were conducted to identify correlates of caregiver strain, health, and service use, and to identify potential covariates (Steiner, Shadish, Cook, & Clark, 2010).
For our main analyses, 3 × 2 × 2 factorial ANOVAs adjusted for caregiver income, caregiver ADL/IADL assistance, and duration of care (covariates determined by Pearson correlation analyses) were then conducted to examine the impact of care recipient relationship type (parent, other family, friend), race (White or African American), and dementia care status (yes or no) on the dependent variables of measures of strain, health, and service use. Post hoc tests, using p < .05, were conducted for any significant interactions using the adjusted Fisher’s least significant difference (LSD) tests for pairwise group comparisons.
Results
Descriptive Information and Demographics
Results of the factorial logistic regression showed that parent care recipients were more likely to be female than either other family care recipients or friend care recipients, χ2(3) = 15.63, p < .001. There were no significant racial differences, relationship type differences, or interactions for caregiver sex, caregiver education, income, marital status, or dementia care status. Demographic characteristics of participants by race are reported in Table 1.
Caregiver Demographic and Descriptive Variables by Race.
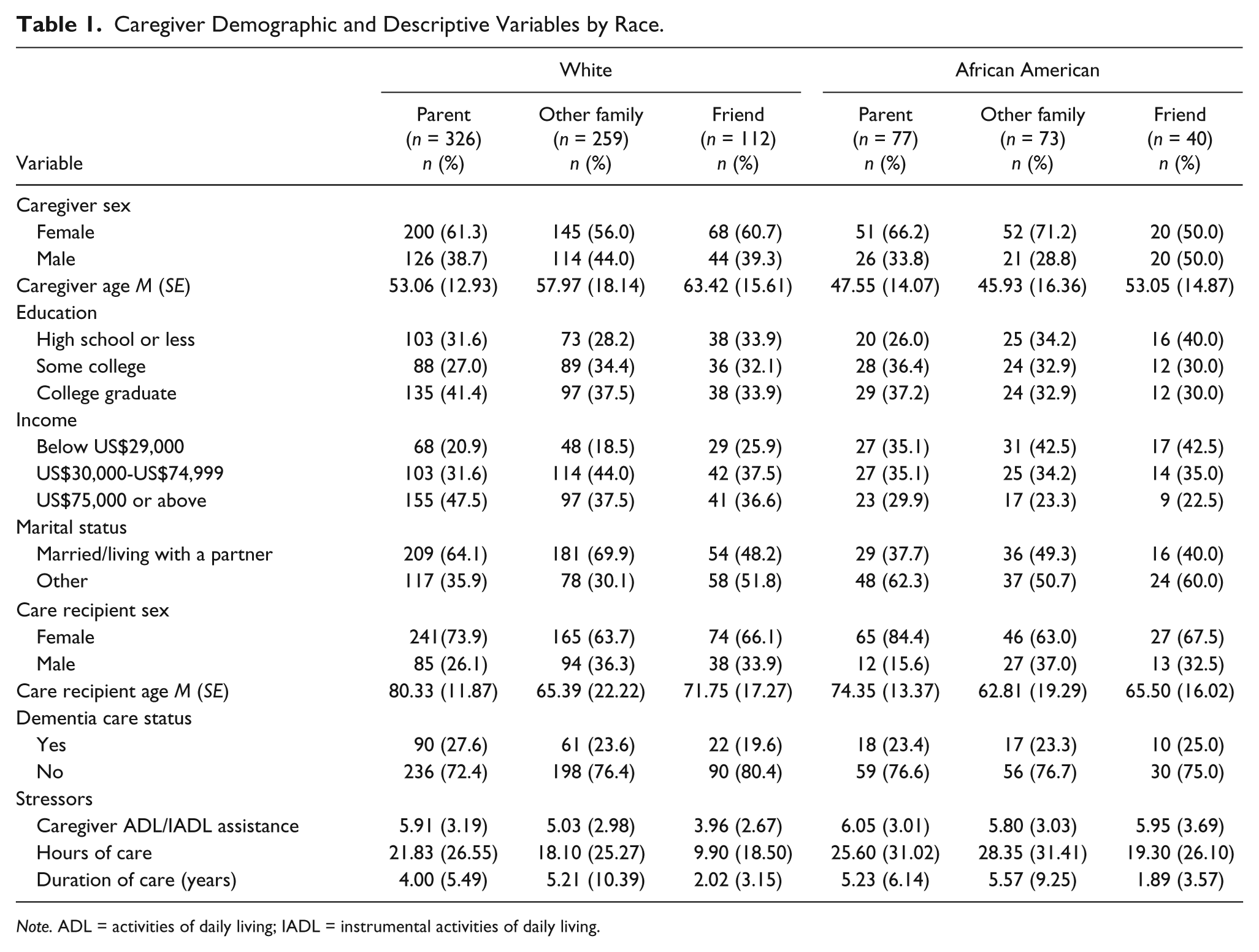
Note. ADL = activities of daily living; IADL = instrumental activities of daily living.
Caregiving stressors
We found that there were a number of differences by race and relationship in the amount of care provided, which provide an important context for studying caregiving outcomes. As shown in Table 1, we found that African American caregivers reported providing higher levels of ADL/IADL assistance (M = 5.91) than White caregivers (M = 4.96), with a significant main effect for race, F(1, 881) = 13.27, p < .001. Also, ACC reported providing higher ADL/IADL assistance (M = 5.98) than other family caregivers (M = 5.38) and friend caregivers (M = 4.95), with a significant effect for relationship type, F(2, 881) = 4.93, p = .007. There was also a significant two-way interaction for race and relationship type on caregiver ADL/IADL assistance, F(2, 881) = 3.67, p = .026. White friend caregivers reported less caregiver ADL/IADL assistance when compared with African American friend caregivers, with no racial differences for the other relationship types.
For hours of care, we found that African American caregivers reported more hours of care (M = 24.58) than White caregivers (M = 16.64), with a significant main effect for race, F(1, 881) = 11.87, p = .004. We also found that ACC reported more hours of care (M = 23.78) than other family caregivers (M = 22.88) or friend caregivers (M = 15.17), with a significant main effect for relationship type, F(2, 881) = 5.47, p < .001. There was no significant interaction.
For duration of care, other family caregivers reported providing more years of care (M = 5.45) than ACC (M = 4.67) and friend caregivers (M = 1.93), with a significant main effect for relationship type, F(2, 881) = 8.58, p < .001. There was no significant main effect of race or a significant interaction.
Correlation Analysis for Covariates
Based on guidelines presented in the literature (Steiner et al., 2010), we chose variables as covariates that were significantly correlated with at least three of the dependent variables. As expected, we found that higher levels of caregiver ADL/IADL assistance were associated with higher reports of caregiver physical, emotional, and financial strain, ps < .001. Caregivers providing more ADL/IADL assistance also reported more service use, p < .001, and poorer health, p < .05. In addition, caregivers with lower income reported less financial strain and better health, ps < .05. Finally, greater duration of care was associated with higher reports of physical strain, financial strain, and service use, ps < .05. Thus, we used income, caregiver ADL/IADL assistance, and duration of care as covariates.
Factorial ANOVA
We conducted five separate 3 × 2 × 2 factorial ANOVAs, adjusting for the covariates mentioned above, to examine the impact of care recipient relationship type (parent, other family, friend), race (White or African American), and dementia care status (yes or no) on measures of strain, health, and service use. Covariate-adjusted statistics are reported in Table 2 for dementia caregivers and Table 3 for nondementia caregivers.
Adjusted Caregiver Strain, Health, and Service Use for Dementia Caregivers by Race.

Note. Covariate adjusted for income, caregiver activities of daily living/instrumental activities of daily living, and duration of care.
Adjusted Caregiver Strain, Health, and Service Use for Nondementia Caregivers by Race.
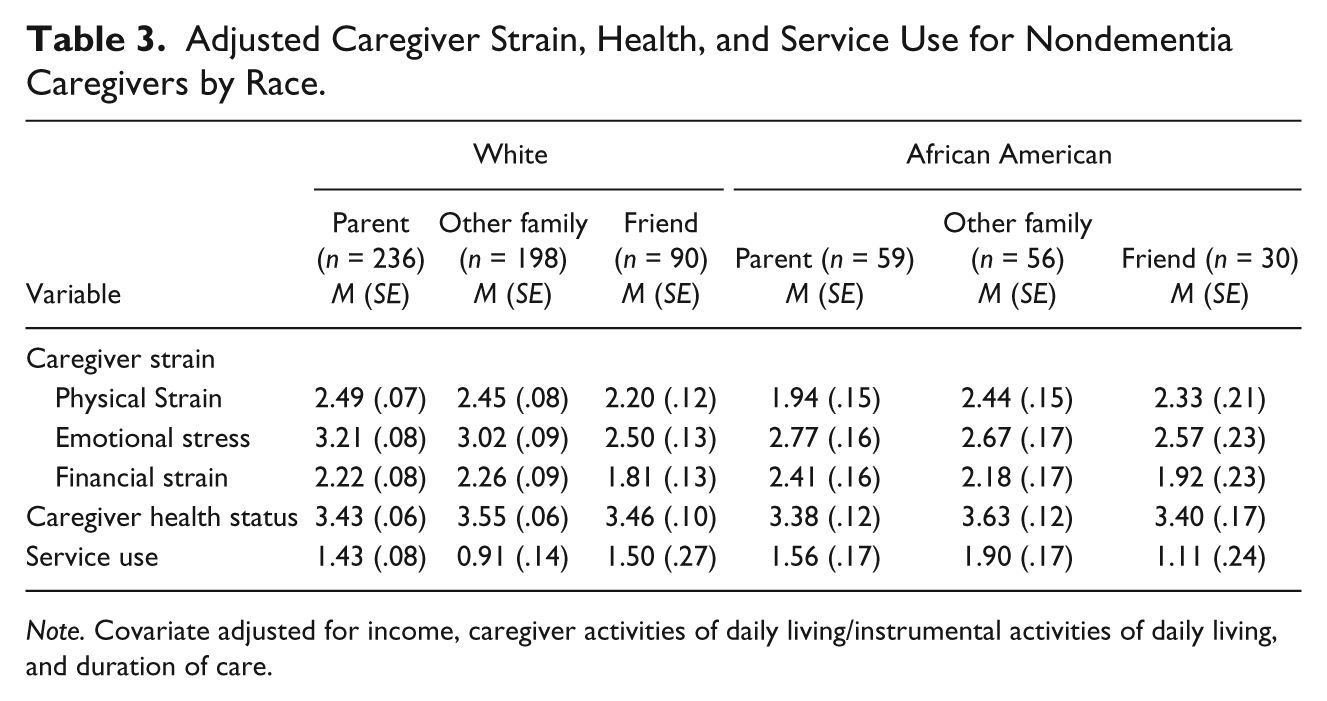
Note. Covariate adjusted for income, caregiver activities of daily living/instrumental activities of daily living, and duration of care.
Caregiver strain
Physical strain
There were no significant main effects of relationship type, race, or dementia care status on physical strain nor were there any significant two-way interactions. However, a significant three-way interaction was found for relationship type, race, and dementia care status, F(2, 872) = 4.03, p = .018 (Figure 1). All covariates had significant effects.

Interaction for Relationship Type × Race × Dementia Care Status on physical strain.
Post hoc analyses revealed that among White dementia caregivers, physical strain did not vary across relationship type. However, among African American dementia caregivers, ACC reported worse physical strain than friend caregivers. Among nondementia caregivers, White ACC reported higher physical strain than White friend caregivers, whereas African American ACC reported the lowest physical strain compared with both African American other family caregivers and friend caregivers.
Emotional stress
Analysis of caregiver emotional stress (Figure 2) showed that that there were significant main effects for relationship type, F(2, 872) = 58.88, p < .001, and dementia care status, F(1, 872) = 11.75, p < .001. ACC reported higher emotional distress (M = 3.39) than other family caregivers (M = 2.99) and friend caregivers (M = 2.49), whereas dementia caregivers reported higher emotional stress (M = 3.22) than nondementia caregivers (M = 2.70). There was also a significant three-way interaction for relationship type, race, and dementia care status, F(2, 872) = 3.08, p = .046. However, there was no significant main effect for race, or any significant two-way interactions. Caregiver ADL/IADL assistance was the only covariate that had a significant effect.

Interaction for Relationship Type × Race × Dementia Care Status on emotional stress.
Post hoc analyses examining the three-way interaction revealed that among dementia caregivers, White ACC reported worse emotional stress than both other family caregivers and friend caregivers. Among African Americans, friend caregivers reported lower emotional stress than both ACC and other family caregivers. Finally, African American dementia ACC reported worse emotional stress than African American nondementia ACC.
Among White nondementia caregivers, caregivers of friends reported less emotional stress than both ACC and caregivers of another family member. African American ACC reported lower emotional stress than White ACC.
Financial strain
Analysis for caregiver financial strain showed that there was only a significant main effect for relationship type where ACC reported higher financial strain (M = 2.25) than both other family caregivers (M = 2.22) and friend caregivers, M = 1.74, F(2, 872) = 4.21, p = .015. There was no significant main effect of race or dementia care status, and there were also no significant two- or three-way interactions. Income and caregiver ADL/IADL assistance were the only covariates that had significant effects.
Caregiver health
The analysis for caregiver health showed that there was only a significant main effect for dementia care status where dementia caregivers reported worse health (M = 3.29) than nondementia caregivers, M = 3.49, F(2, 872) = 4.129, p = .042. There were no main effects for relationship type or race, or any significant two- or three-way interactions. Income and duration of care were the only covariates that had significant effects.
Caregiver service use
The analysis for caregiver service use (Figure 3) showed that there were significant main effects for relationship type, race, and dementia care status. ACC reported higher service use (M = 1.76) than both other family caregivers (M = 1.51) and friend caregivers, M = 0.88, F(2, 872) = 10.71, p < .001. African American caregivers reported greater service use (M = 1.85) than White caregivers, M = 1.42, F(1, 872) = 8.51, p = .004. Dementia caregivers used more services (M = 2.11) than nondementia caregivers, M = 1.32, F(1, 872) = 20.10, p < .001. There was a significant two-way interaction for relationship type and dementia care status, F(2, 872) = 5.12, p = .006. There were no other significant two- or three-way interactions. Caregiver ADL/IADL assistance and duration of care were the only covariates that had significant effects. Post hoc analyses revealed that ACC who cared for a parent with dementia reported significantly more service use than ACC who cared for a parent without dementia but no differences by dementia status were found for caregivers of other family or friends.
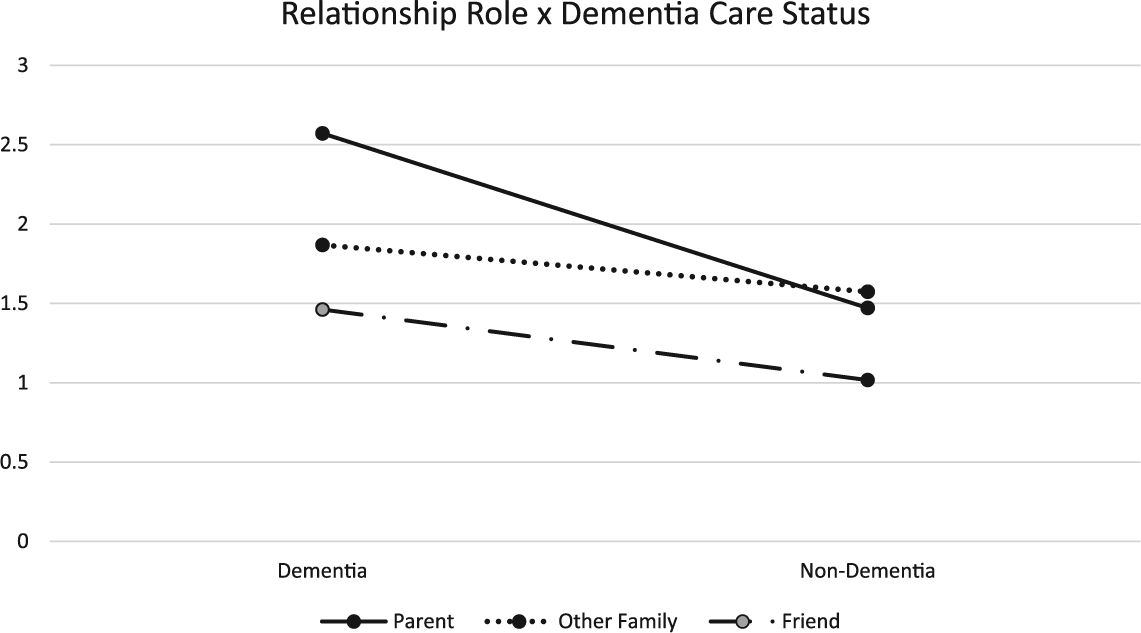
Interaction for Relationship Type × Dementia Care Status on service use.
Discussion
We compared a population-based sample of White and African American caregivers while taking into account demographics, caregiving assistance, and potential moderators of relationship type and dementia care status. Our hypothesis that African American caregivers would report greater caregiving assistance was supported by the results. African American caregivers provided higher levels of ADL/IADL assistance and greater hours of care than White caregivers. However, there were no main effects for racial differences in any of the measures of caregiver strain or health. Furthermore, our hypothesis that dementia caregivers would report more strain than nondementia caregivers was partially supported. Dementia caregivers were more emotionally stressed, had worse self-rated health, and used more services than nondementia caregivers, but there were complex interaction effects that modified these relationships. Dementia and nondementia caregivers did not differ significantly in physical strain or financial strain.
As several significant interactions showed, there were racial differences in physical strain and emotional stress across relationship type and dementia care status. African American dementia ACC reported worse physical strain in comparison with African American dementia friend caregivers. Cultural norms and relationship roles and bonds between African American parents and their children may influence the higher strain African American ACC experience from the reversal of roles and ambiguous loss of caregiving for a parent with dementia. Also, African Americans often report lower self-rated health (Dilworth-Anderson et al., 2002; Pinquart & Sörensen, 2005); therefore, preexisting health conditions might be exacerbated by the stress of providing care and may help explain the higher levels of physical strain reported by African American caregivers.
African American nondementia ACC reported less psychological stress than White nondementia ACC after adjusting for demographic variables and indicators of caregiving stressors. Research suggests that African American caregivers may have a number of assets that produce resilience in coping with caregiving, including culturally based philosophies that are supportive of being a caregiver (Dilworth-Anderson et al., 2002; Knight & Sayegh, 2010), previous experience with stress and expectations of becoming a caregiver (Haley et al., 1996), and social support (Clay, Roth, Wadley, & Haley, 2008). The results of the study also show how race may not fully explain the complex findings uncovered after covariate adjustment. For example, when comparing White and African American caregivers, living arrangements of caregivers and their care recipients do play a role in the emotional health of caregivers (Siegler et al., 2010).
In our sample, dementia ACC utilized more services than nondementia caregivers. This may be, in part, because dementia caregivers may need (and seek out) more support services in comparison with other caregivers. Research shows that dementia caregivers often use services due to strain and difficulty managing problem behaviors in care recipients with dementia (Martindale-Adams, Nichols, Zuber, Burns, & Graney, 2016).
Consistent with recent suggestions that caregivers are often resilient (Roth et al., 2015), we found relatively low reports of caregiving strain and stress in this population-based sample. For physical and financial strain, means in all subgroups were less than the midpoint of the rating scale, and for emotional stress, subgroup scores ranged from 2.18 to 3.57.
We believe that the major contribution of this study is the recognition that racial differences in caregiving may be complex and that considering other contexts of care, including relationship type, and dementia care status, are vital. The results of the current study show that African American ACC of parents with dementia reported higher physical strain in comparison with other caregiver relationship types. As African Americans often report low levels of physical health (Mays, Cochran, & Barnes, 2007; Spence, Adkins, & Dupre, 2011), they may be at an increased health risk due to the physical strain of caring for a family member with dementia. Future dementia caregiving research should examine both physical and psychological stressors in African American ACC who care for a parent with dementia.
Limitations
This study has several limitations. Although this data set is population based and includes good measures of caregiving stressors (caregiver ADL/IADL assistance, hours and duration of care) and diverse measures of caregiving strain, the data are lacking in measures that would be useful in examining theoretically relevant constructs proposed by stress process models of caregiving, such as information on internal resources (e.g., religiosity, spirituality, measures of self-efficacy and competence) and external resources (e.g., instrumental help and emotional support from support network). Another important limitation is that the measures of strain were represented by single-item measurements, which may have failed to detect real differences as they do not have the psychometric strengths of well-validated, multi-item scales. Thus, our finding of a general lack of racial differences must be viewed with caution. Also of note is that this study included both current and recent (within the last 12 months) caregivers. Whereas we found no evidence that this factor affected our results, this may be an important feature making this sample unique. Future studies should adopt the strengths of this analysis (use of a population-based sample, comparison of specific caregiver relationships) for use with a richer data set of theoretically based variables, which have better measurement characteristics. Other studies should also include other important racial/ethnic groups of caregivers, such as Hispanic Americans, although this is difficult to do in population-based studies unless they have specifically oversampled diverse participants (Rote, Angel, & Markides, 2015).
Conclusion
Our study found fewer racial differences in caregiving than has been previously described in the literature. Although African American caregivers reported higher care responsibilities, they did not significantly differ as a subgroup from White caregivers in measures of stress, strain, and health. Racial differences were found only among subgroups considering dementia case status and caregiving relationship. Previous studies reporting lower caregiving strain in African American versus White caregiving have usually not considered relationship type and dementia care as factors, and generally used convenience samples. Another important question is whether racial differences in caregiving strain may have changed over time. Caregiving strain has decreased in some groups between 1999 and 2015 (Wolff et al., 2017) although racial differences in these changes were not reported. African American ACC of parents with dementia may be particularly at risk for negative outcomes. Recent research has demonstrated that caregiver interventions that had focused on spouses can be modified and targeted toward the unique needs of adult children (Gaugler et al., 2015; Gaugler, Reese, & Mittleman, 2016), and future work should examine how such interventions can be tailored to be culturally appropriate and acceptable to ACC of minority groups. Also, research into caregiving for other health conditions, such as stroke, must incorporate analyses to examine racial differences and address unique caregiving needs (Skolarus, Freedman, Feng, & Burke, 2017). Examining how race/ethnicity affects ACC and ways that caregiver interventions can be culturally tailored to fit the needs of diverse participants (Graham-Phillips, Roth, Huang, Dilworth-Anderson, & Gitlin, 2016) remain important priorities in caregiving research.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.