
Abstract
Introduction
The rapid rise of demand for hospital care is attributed not to aging but to the chronic diseases that are more prevalent among older adults (Strunk, Ginsburg, & Banker, 2006), and one of such chronic conditions is neurocognitive disorders. The prevalence of neurocognitive disorders in the United States has doubled in 13 years: from 2.3 million in 2002 (Plassman et al., 2007) to more than 5 million in 2015 (Alzheimer’s Association, 2015). This trend is expected to continue in the next few decades as population aging continues.
Aging is related to some irreversible physiological dysfunctions that are associated with tissue senescence in the human body. In fact, the nervous system is no longer able to repair damages or regenerate tissues. In normal aging, such a change in the nervous system can influence processing time and motor performance (Strauss & Tinetti, 2009), and some abnormal changes in advanced age can affect memory in general and cognition in particular (Galvin, 2009). Cognition incorporates five components: memory, language, attention, visuospatial skills, and executive ability. Neurocognitive disorders, previously known as dementia, represent a status in which an individual displays signs of cognitive deficits including impaired memory, language disorder, lack of attention, executive disability, and diminished visuospatial skills.
With regard to the etiology of cognitive impairment, different types of neurocognitive disorders have various etiologies. Nevertheless, some predisposing factors are common in almost all types of cognitive disorders. Cardiovascular diseases, particularly hypertension (Knopman et al., 2001), and thrombogenic factors can cause white matter lesion, and ultimately, cognitive impairments (Breteler et al., 1994). High levels of cholesterol in middle age is correlated with mild cognitive impairment (MCI) in advanced age (Kivipelto et al., 2001), and diabetes mellitus is known as one of the risk factors for neurocognitive impairment (Cheng, Huang, Deng, & Wang, 2012). Various types of neurocognitive disorders may develop different kinds of signs and symptoms. For instance, frontotemporal dementia may start with some behavioral indiscretion, growing instability in personality, or dietary changes (Galvin, 2009). In this sense, people suffering from neurocognitive disorders are especially more likely to utilize neurologic and psychiatric care in hospitals compared with those without this disorder (Tuppin, Kusnik-Joinville, Weill, Ricordeau, & Allemand, 2009).
Some transitional states are identified between normal cognitive function and neurocognitive disorders. This stage is known as MCI, in which older adults experience impairments in one or two domains of cognition (Albert et al., 2011; Petersen et al., 2001). For instance, individuals with MCI may experience altered attention, whereas other domains are still intact. Each year, 10% to 15% of MCI cases develop Alzheimer’s disease (AD) (Petersen et al., 2001), and some proportions of this population can develop other types of neurocognitive disorders. Regarding the incidence of AD, 469,000 new cases were reported in 2014 (Gaugler, James, Johnson, Scholz, & Weuve, 2014), when there were 4.7 to 6.2 million older adults with AD. Approximately, one in five adults above 71 years of age is a known case of AD (Plassman et al., 2008) in 2014. Drawing on Peterson and associates’ (2001) work, the prevalence of MCI is estimated to be at least about 47 million people, if we consider 4.7 million AD cases.
Whereas persons with dementia are more likely to be hospitalized compared with those without dementia (Toot, Devine, Akporobaro, & Orrell, 2013), hospitalization can trigger a cascade of cognitive impairment (Mathews, Arnold, & Epperson, 2014; Wilson et al., 2012). More frequent hospital admissions can worsen cognitive decline (Wilson et al., 2012). Moreover, neurocognitive disorders can significantly increase mortality during hospital admission (Guijarro et al., 2010; Sampson, Blanchard, Jones, Tookman, & King, 2009; Zuccalà et al., 2003). The purpose of this study is to examine the relationship between the extent of cognitive impairment and hospital admission frequency among older adults.
Neurocognitive Disorders and Hospital Admission
Owing to the direct effect of cognitive disorders on function, all types of neurocognitive disorders can also render disability and, accordingly, dependency in the activities of daily living (ADLs) (Gure, Langa, Fisher, Piette, & Plassman, 2013; Nanna, Lichtenberg, Buda-Abela, & Barth, 1997). For example, the loss of cognitive function can considerably increase processing time and decrease walking speed (Welmer, Rizzuto, Qiu, Caracciolo, & Laukka, 2014). As a result, the risk of falling rises when the level of cognition declines. Consequently, cognitive impairment, including MCI, can render dependency in ADL and the instrumental activities of daily living (IADLs) (Gure et al., 2013). Approximately, half of the disabilities in performing ADL coincides with cognitive impairment after age 75 (Guralnik & Ferrucci, 2009; Schulz & Albert, 2009). Conversely, limited physical activity and mobility can significantly increase the risk of neurocognitive disorders (Minami et al., 1995). This mutual cause-and-effect relationship may create a vicious cycle, in which people with neurocognitive disorders remain confined in their disorders and dependency, experiencing a downhill process.
Neurocognitive disorders are generally related to physical and mental health problems (Toot et al., 2013). Neurocognitive disorders can increase the risk of falling (Van Doorn et al., 2003), and consequently the risk of fall injuries (e.g., hip fracture, head trauma, depression). In particular, the risk of hospitalization due to falling, bone fractures, infectious diseases (i.e., respiratory and urinary) (Sampson et al., 2009), cardiovascular diseases, and neurologic and psychological disorders is higher among cases of neurocognitive disorders compared with nondementia cases. After discharge from hospital, the mortality rate of demented patients is significantly higher than that of nondemented cases (Sampson et al., 2009; Sampson, Gould, Lee, & Blanchard, 2006): about 30% in 6 months increasing to 38% in 12 months. Nearly 85% of post–hospital discharge patients are transferred to care centers, such as nursing homes (Sheehan et al., 2013). However, there are inconsistent reports about the rate of hospitalization after the incidence of a neurocognitive disorder. The relative risk of hospital admission for dementia cases compared with cases without dementia, as reported in different studies, ranges from 0.6 to 9.1, depending on the underlying diseases involved (Toot et al., 2013).
In sum, the loss of cognitive ability may be one of the predisposing factors for physical injuries and, consequently, a significant increase in hospital admission. Moreover, the level of cognition is a predictor for transferring from hospital to nursing homes; people with MCI are more likely to transfer to nursing homes after hospital admission (Sands et al., 2003). The lower the cognitive function, the greater the probability of more frequent hospital admission and lengthier hospitalization (Wilson et al., 2012). Nonetheless, we know little about how people’s varying levels of cognition may affect their hospital admission, particularly if they have MCI, which is frequently undiagnosed. Because hospitalization can increase the risk of cognitive impairment (Wilson et al., 2012), MCI cases will be more likely to transit to moderate or severe types of cognitive impairment after repeated hospitalization. This transition from MCI to moderate or severe cognitive impairment can also increase health care consumption, and, consequently, health care costs. Hence, our study aims to examine connections between the frequency of hospitalization and the extent of cognitive impairment not only to fill the gap in the literature but also to help consider some practical and financial implications for policy makers and health care providers.
Method
This study used the data collected by the National Health and Aging Trend Study (NHATS), Round 1 (2011) (N = 8,245), which was the sixth survey conducted by the Center for Studying Health System Change. The survey was a national cross-sectional study assessing access to care, quality of care, and demographic information. This database was made public by Inter-Consortium for Political and Social Research (ICPSR) in the United States in 2012.
Sampling Method
The NHATS used a three-stage stratified sampling to collect data from Medicare beneficiaries aged 65 and older (as of September 30, 2010) living in the United States. In the first stage, 95 counties or group of counties (if the number of beneficiaries was small, a group of counties was formed) were selected as the Primary Sample Units. Within each county, ZIP codes were selected as the secondary sample units. In the third stage, individuals living in each ZIP code were selected with equal probability of selection by age group and race/ethnicity (Montaquila, Freedman, Edwards, & Kasper, 2012). The sample size was adjusted with regard to adequate sample in each age category as well as race/ethnicity—non-Hispanic Black and White. The main exclusion criteria at the time of sampling were age 64 or younger as of September 30, 2010 and residency out of the United States. The weighted response rate was 71.3% with 8,245 complete cases (Montaquila et al., 2012).
Measurement
The dependent variable was the number of hospital admissions, treated as a count variable in all the analyses. The number of hospital stays (any type of stays) and the type of surgery for the 12 months period prior to the time of data collection were asked. The independent variable was the level of cognition, which was operationalized as below.
Cognitive function was measured in the NHATS by testing self-rated memory, orientation, executive function (Clock Drawing Test [CDT]), and retrieval information (delayed word recall) (Kasper & Freedman, 2015). Memory was measured by 10-word immediate word recall. There were three lists of 10 words, and the respondents were randomly assigned to one of them. The list of words was read to the respondents, and after a delay, they were asked to name the words they recalled. CDT, highly correlated with Mini Mental State Examination (Agrell & Dehlin, 1998), was performed by the respondents on the piece of paper instructed by the interviewers.
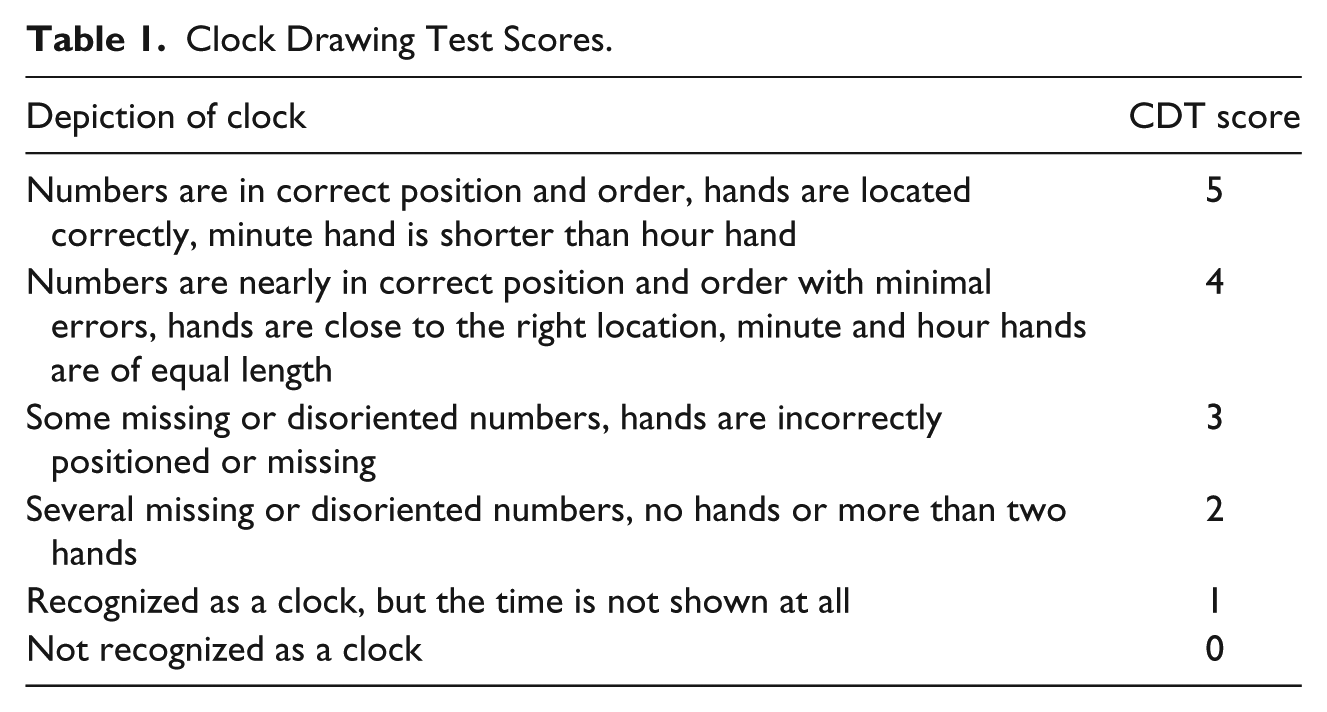
The respondents had 2 minutes for drawing a large circle, put all the numbers, and finally set the hands to show 11:10. CDT was scored in six categories on a scale from zero to five and categorized in Table 1 (Kasper & Freedman, 2015).:
Clock Drawing Test Scores.
The levels of cognition were categorized into five levels (see Table 2):
normal: CDT 5 and the number of recalled words ≥6; mild: CDT 4 and the number of recalled words between 3 and 5; mild to moderate: CDT 3 and the number of recalled words between 3 and 5; moderate: CDT 2 and the number of recalled words between 3 and 5; severe and very severe: CDT 0-1 and recalled words <3.
Frequency of CDT Score, Word Recall, and Cognitive Function.
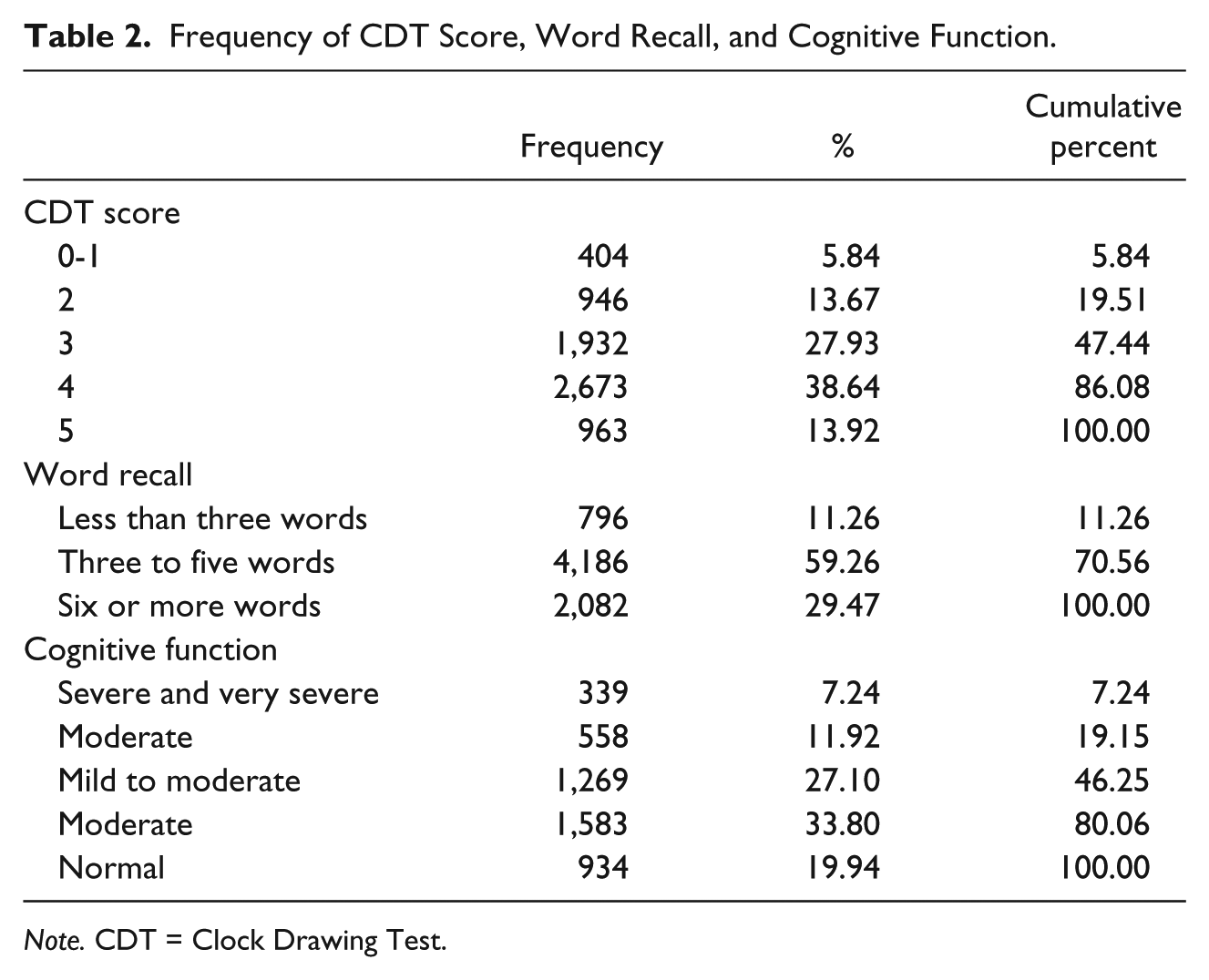
Note. CDT = Clock Drawing Test.
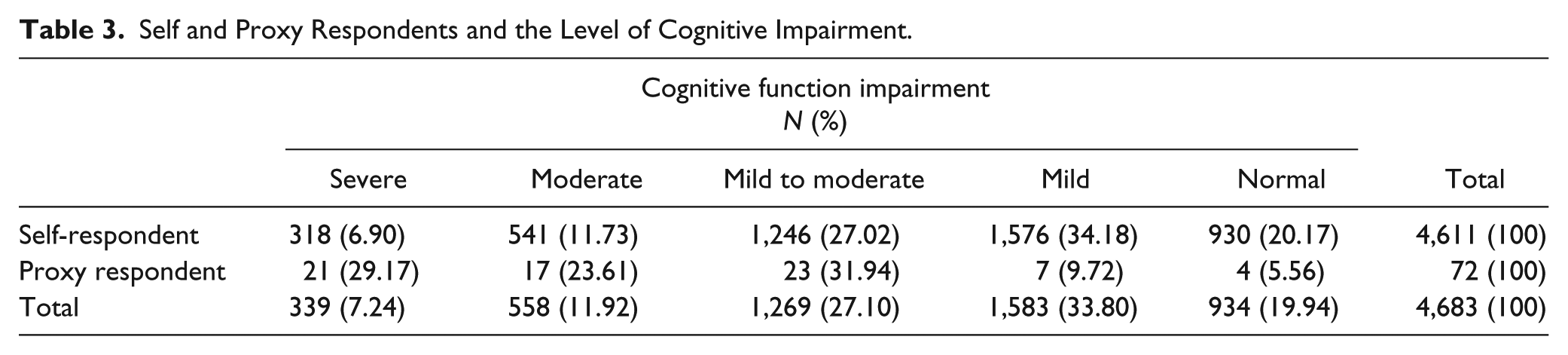
A proxy respondent was used in case of cognitive impairment, dementia, hearing problems, or severe illness. The proxy respondents were involved in routine daily activities of the patients (Montaquila et al., 2012). Table 3 shows that 18.63% of the self-respondents, who did not use a proxy, had severe or moderate cognitive impairment. Because the reliability of their responses could affect the results of regression models, these two groups of self-respondents (severe and moderate cognitive impairment) were excluded from the sample in the third regression model.
Self and Proxy Respondents and the Level of Cognitive Impairment.
Education was categorized into nine levels: “no school” (1.0%), “first to eighth grade” (10.7%), “ninth to 12th grade” (13.2%), “high school diploma” (28%), “vocational, technical, business” (7.5%), “some college” (12.8%), “associate degree” (4.6%), “bachelor’s degree” (12.1%), and master’s or doctoral degree” (10.1%).
Data Analysis
The control variables in this study were self-reported: age, gender, race, education, marital status, self-reported health status, living environment (home, residential care, nursing home), history of falling, previous surgery, and physical health problems including history of heart attack, heart diseases, high blood pressure, diabetes, lung diseases, stroke, and functional limitations in ADLs including shopping, meal preparation, money management, laundry, walking, climbing stairs, going out, moving inside home, transfer to/out of bed, using toilet, dressing, eating, and bathing (Table 4). All persons living in a residential care setting (other than nursing home) or the community were included in in-person interviews (Kasper & Freedman, 2015).
Frequency of Diseases and Functional Limitation and Regression Model Predicting the Impact of Diseases on the Number of Hospital Admission.
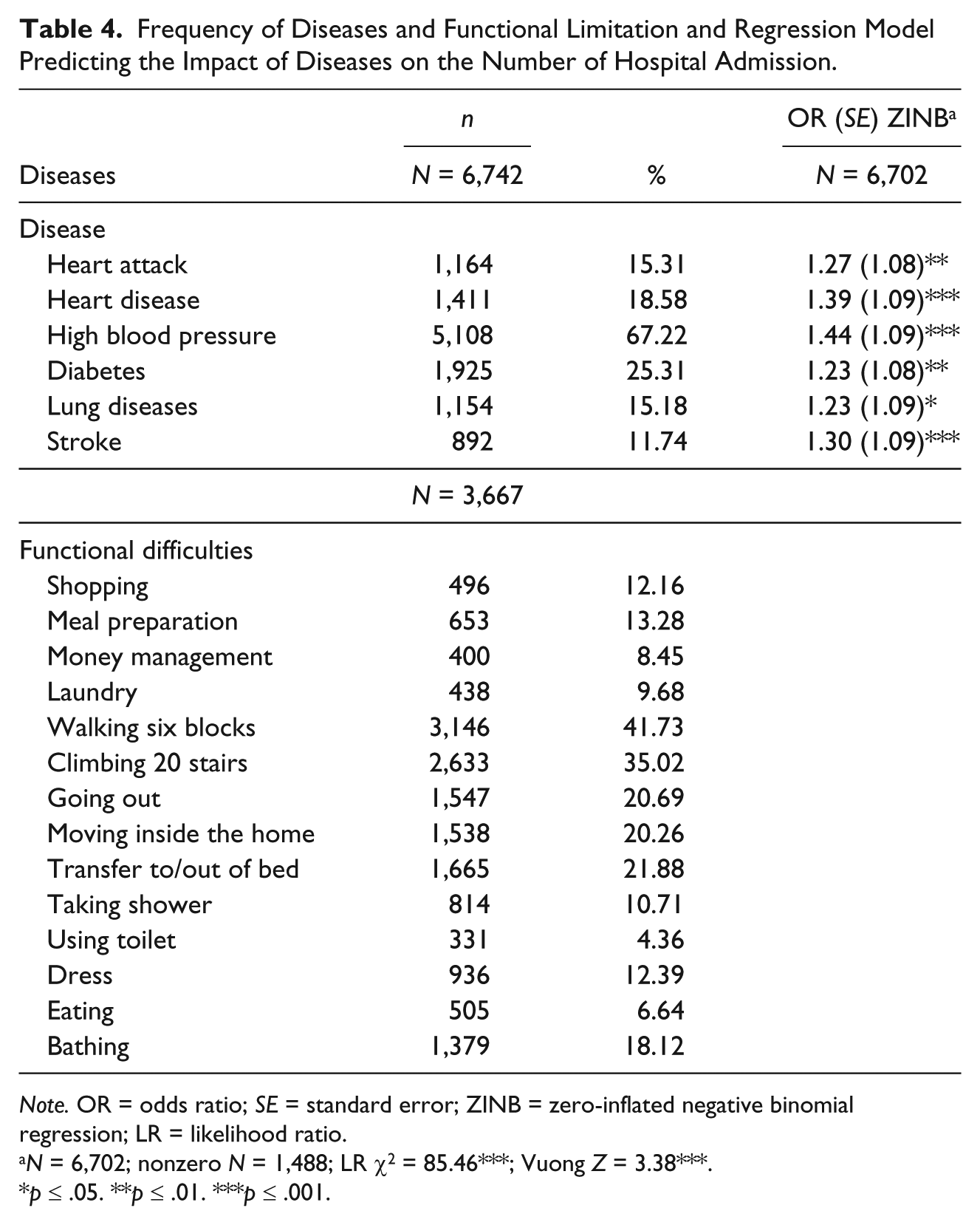
Note. OR = odds ratio; SE = standard error; ZINB = zero-inflated negative binomial regression; LR = likelihood ratio.
N = 6,702; nonzero N = 1,488; LR χ2 = 85.46***; Vuong Z = 3.38***.
p ≤ .05. **p ≤ .01. ***p ≤ .001.
As tabulated in Table 3, 6.9% and 11.73% of self-respondents had severe and moderate cognitive impairment, respectively. Because the level of cognition could interfere with the reliability of responses about the number of admission, the third statistical model was developed (Table 5).
Regression Models Predicting Total Number of Hospital Admission Among Older Adults in 2010, United States.
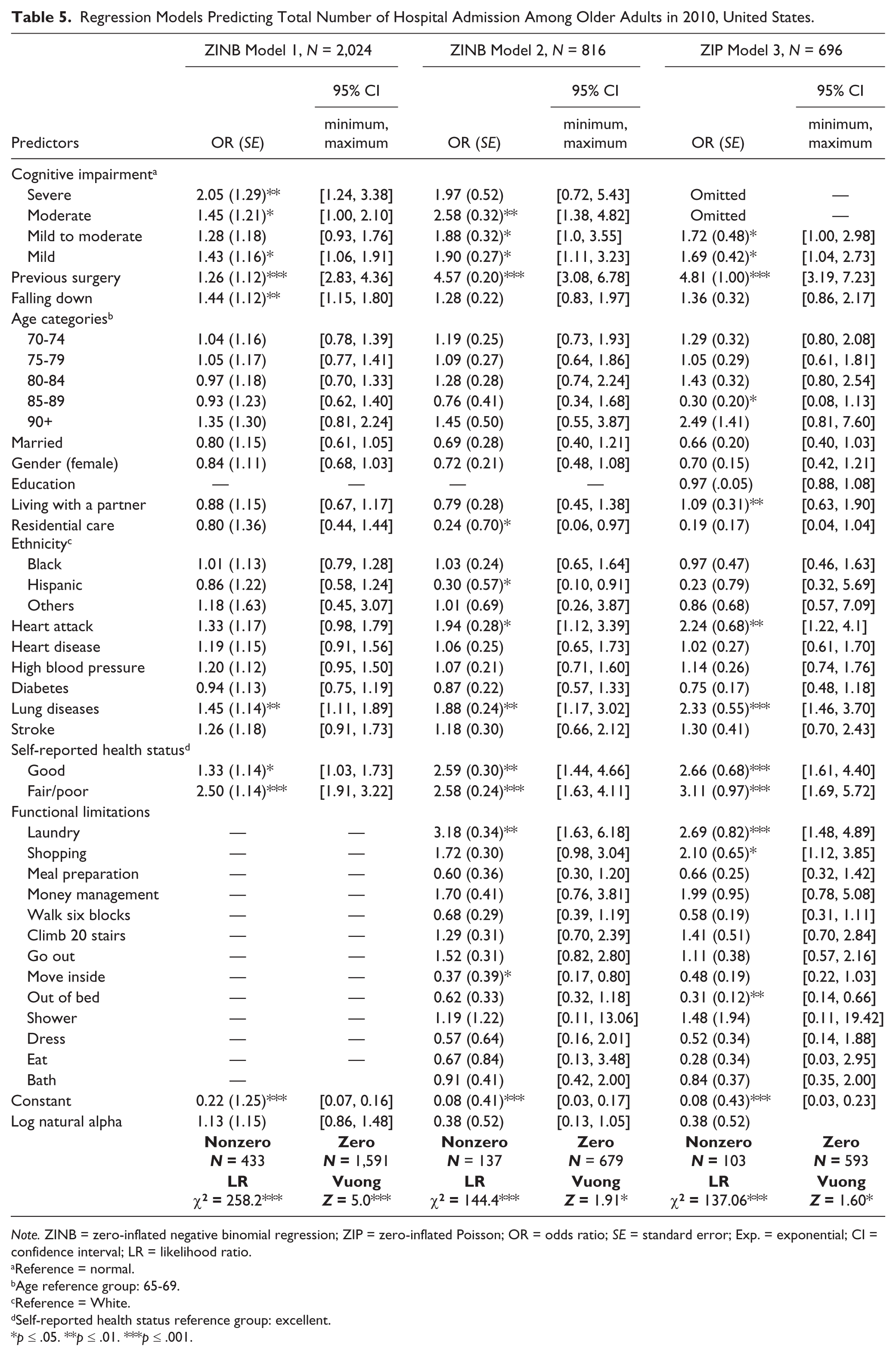
Note. ZINB = zero-inflated negative binomial regression; ZIP = zero-inflated Poisson; OR = odds ratio; SE = standard error; Exp. = exponential; CI = confidence interval; LR = likelihood ratio.
Reference = normal.
Age reference group: 65-69.
Reference = White.
Self-reported health status reference group: excellent.
p ≤ .05. **p ≤ .01. ***p ≤ .001.
Considering that the level of education influences the health status of a population through so many pathways such as income and function (Barbareschi, Sanderman, Leegte, van Veldhuisen, & Jaarsma, 2011), the collinearity in the statistical models was unavoidable, and we had to exclude the level of income from the models.
Statistical Tests
Data analysis was conducted using Stata (version 13.0). Because the dependent variable is a count variable with 78% of cases with no hospital admission (zero), the effects of overdispersion (response variance greater than mean), which can render the underestimation of standard errors of the estimates, needed to be controlled for. Hence, Poisson models are selected over ordinary or square models. However, given the excessive number of zero hospital admission, zero-inflated negative binomial regression (ZINB) and zero-inflated Poisson (ZIP) are more appropriate than other models (Institute for Digital Research and Education [IDRE], 2011). To choose between ZINB and ZIP, the Vuong test can be helpful; when it is statistically significant, ZINB can be preferred over negative binomial regression or ZIP models. In addition to the Vuong test, when the range of coefficient alpha does not contain zero, it indicates whether ZINB are more appropriate models versus ZIP (IDRE, 2011). The Vuong tests of the first, second, and third regression models were 5 (p < .001), 1.91 (p < .05), and 2.15 (p < .05), respectively. In the first and second models, the range of coefficient alpha did not contain zero; hence, ZINB was preferred over ZIP. In the third regression model, the coefficient alpha contained zero. Therefore, ZIP was run for the third regression model. Cases with missing values were excluded from the study.
Results
The total number of hospital admissions for Round 1 of the 2010 National Health and Aging Trends Study was 1,765. From the respondents, 22% had overnight hospital admission within 12 months prior to the study. The average of the frequency of admission among those respondents who had at least one admission was 1.75 (SD = 1.76; see Figure 1 for the distribution of hospital admission). From the respondents, 20% had normal cognitive function, 34% mild, 27% mild to moderate, 12% moderate, and 7% severe cognitive impairment (refer to Table 2 and Figure 2).

Distribution of hospital admissions.
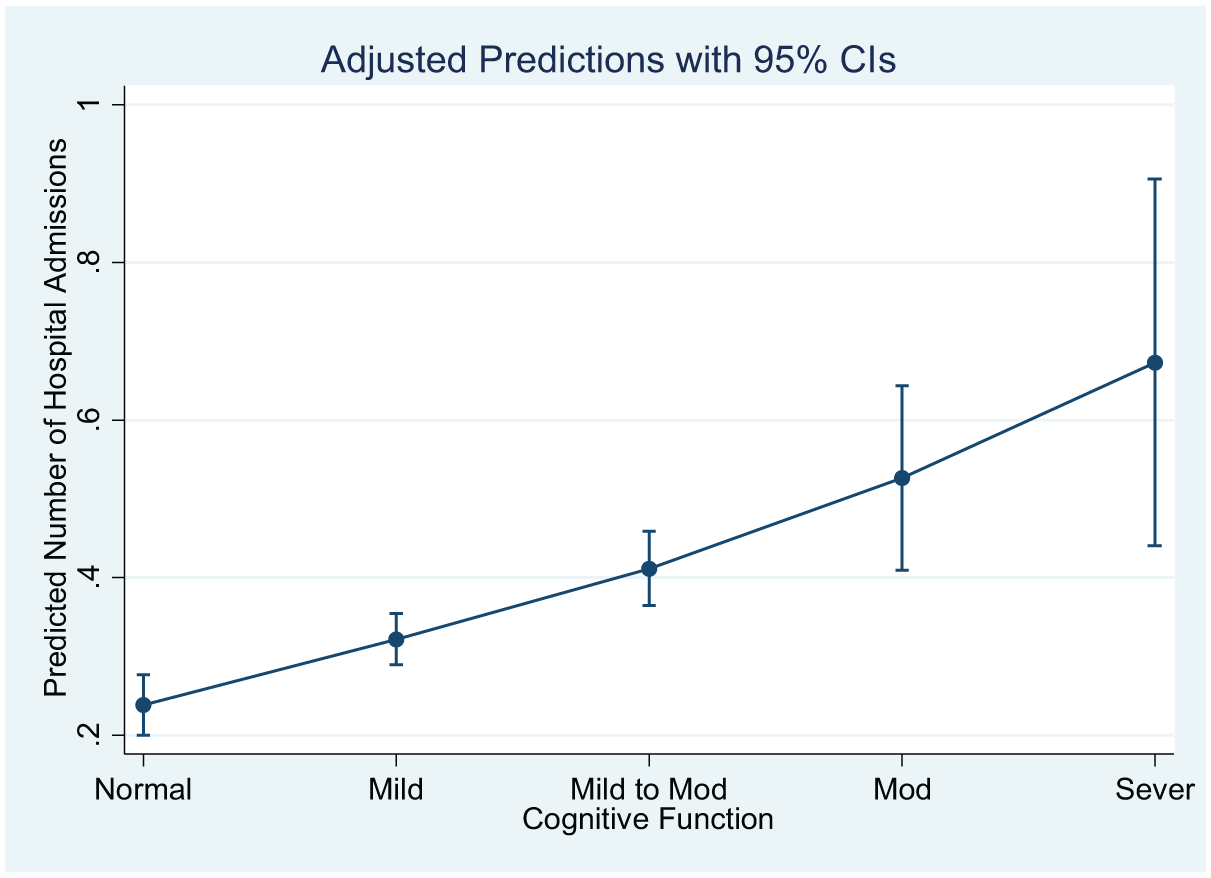
Adjusted predicted number of hospital admissions across different levels of cognitive function.
Approximately, 14.5% of the respondents were covered under Medicaid in addition to Medicare. Table 4 shows the findings for the diseases associated with increased frequency of hospital admission. In terms of self-perceived health status, 29% of the respondents rated their health status as poor or fair, 32% good, and 39% very good or excellent. From the respondents, 19% had at least one surgery (knee, hip, back, cataract, or heart) and 23% experienced falling down during the year before the study. Sixty percent of the respondents were women, 52% married, 67% living with their partners, and 12% living in a residential care center. With regard to ethnicity, 69% were White, 22% Black, 6% Hispanics, and 3% Other ethnic groups.
Of note (as shown in Table 5) is that cognitive impairment can be a significant predictor for hospital admission. Respondents with MCI were significantly likely to be hospitalized more frequently when compared with those with normal cognitive abilities in all three models (odds ratio [OR] = 1.43 in Model 1, OR = 1.90 in Model 2, and OR = 1.69 in Model 3). Respondents with mild-to-moderate cognitive impairment were likely to have more hospital admissions compared with those with normal cognitive function. Although the difference was not statistically significant in the first model (OR = 1.28), the likelihood was statistically significant in the second and third models with 1.88 and 1.77 ORs, respectively, when functional limitations were entered into the models. Cases with moderate cognitive impairment were also more likely to be more frequently hospitalized (OR = 1.45 in Model 1 and OR = 2.58 in Model 2) than those without cognitive impairment. An interesting insight is that severe cognitive impairment can double the probability of frequent hospital admissions when compared with respondents with normal cognitive function in the first model, although the significance level disappeared in the second model when functional limitations were included. Because the great majority (96%) of those respondents with severe and moderate cognitive impairment responded to the questions about hospital admission, they were omitted in the third model to omit the possibility of interference of memory with the reliability of responses about hospital admissions.
Those respondents who previously had surgery are more likely to be frequently admitted than those without previous surgeries. This likelihood increased from 1.26 in Model 1 to 4.57 and 4.81 in the second and third models, respectively, when the level of function was entered as a control variable (Table 5). Falling down was another significant predictor for hospital admission in the first model. Those who reported at least one fall event within 12 months prior to the study were at a greater risk of hospital admission (OR = 1.44, 95% CI = [1.15, 1.80]). In the second and third models, the probability of hospital admission remained higher among those respondents with a history of falling compared with those with no history of falling although the likelihood was not significant.
Of the physical health problems considered, previous lung diseases were found to significantly increase the risk of hospital admission (OR = 1.45 Model 1, OR = 1.88 Model 2, and OR = 2.33 Model 3). Heart attack was another predictor with significant difference in OR in the second and third models. Another significant predictor was the self-reported health status. Older adults who rated their health to be poor or fair were more likely to have hospital admissions relative to those who considered themselves to be of excellent health (Table 5).
In Models 2 and 3, the functional limitation in doing laundry was a significant predictor for hospital admission with ORs of 3.18 and 2.69, respectively. The ability to transfer in and out of bed independently was a predictor for hospital admission in the third model. Interestingly, dependent respondents were less likely to be hospitalized compared with independent respondents. Being dependent in moving inside can decrease the possibility of hospital admission in the second and third models, although it was not significant in the third model. A cross tabulation showed that 21% of the dependent respondents lived in the community compared with 32% living in residential care centers (χ2 = 27.56, p < .0001). Being covered by Medicaid was significantly correlated with the number of hospital admission. Those respondents with Medicaid coverage were more likely to be hospitalized (incidence rate ratio [IRR] = 1.54, p < .001). However, when this variable was entered to the models, it was not a significant predictor for hospital admission (IRR = 0.54, p = .082), which can be explained by the presence of chronic health problems.
Discussion
The population of people with dementia is growing rapidly and continues to be underdiagnosed. According to Manly et al. (2008), more than 20% of those aged 65 and above develop MCI, while only 30% of them regain their normal cognitive function. The risk of hospital admissions is higher among older adults with MCI (Callahan et al., 2015), and hospital admission is documented as a predisposing factor to cognitive decline (Wilson et al., 2012). Thus, hospital admission can render a vicious cycle, in which patients with neurocognitive disorders including MCI can be at risk of proceeding to severe forms of the disease. This rapid transition can, in turn, increase health care consumption including hospital services, which is one of the most expensive health care services in the United States. Hence, a critical question for policy makers and caregivers, particularly family members, is whether people with mild or mild-to-moderate cognitive impairment utilize more hospital services compared with those with normal cognitive ability. Another question is whether or not the severity of cognitive impairment can influence the frequency of hospital admission.
In this study, we used the National Health and Aging Trend Studies 2010 to compare the frequency of hospital admission across various levels of cognitive abilities, controlling for age, gender, marital status, ethnicity, living arrangement, chronic diseases, self-reported health status, and function. The results reveal that cognitive impairment was independently and significantly associated with frequent hospital admissions (Table 5). The likelihood of frequent hospital admissions varied across different levels of cognition. The highest likelihood of frequent hospital admissions was found among those with severe cognitive impairment—almost two times higher than admission with normal cognition, followed by moderate, mild, and mild-to-moderate levels of cognition without controlling for the level of function (Model 1, Table 5). Entering the functional indicators in the regression models changed this pattern as the likelihood of hospital admissions among respondents with moderate impairment increased and was higher than the cases with severe impairment (Model 2, Table 5). Nonetheless, in the third model, the likelihood of hospital admissions was significantly greater among mild and mild-to-moderate cases compared with those with normal cognitive ability. According to Toot et al. (2013), individuals diagnosed with dementia are at greater risk of hospital admission in different hospital departments such as orthopedics, respiratory, and urology, and this risk could have resulted from their dependency in performing some daily activities (i.e., bathing, using toilet, grooming, eating food, dressing, walking, transferring, climbing stairs, control of bowel and bladder). Our findings support what Toot et al. reported about dementia and risk of hospital admissions: People with severe neurocognitive impairment are at higher risk of hospitalization. Furthermore, our findings reveal that the risk of hospital admission varies across different neurocognitive abilities controlling for the level of function and chronic diseases (Table 5). Wilson et al. (2012) reported that cognition function represented by episodic memory and executive function significantly dropped after hospital admission among adults above age 75, whereas the pace of cognitive decline was dependent upon the disease and the length of admission. Given their study, it is plausible that persons with MCI are at risk of losing cognitive abilities at a rapid pace after frequent and longer hospital admissions, and our own results show that such persons are more likely to be hospitalized than those with normal cognitive ability are. Hence, undiagnosed people with MCI will be more susceptible to losing their cognitive function after frequent hospital admissions. Early screening for cognitive ability at admission time and subsequent interventions can slow the pace of cognitive decline among MCI patients.
Cognitive impairment can render some physical and mental disabilities (Gure et al., 2013), raising the risk of hospitalization (Greysen, Stijacic Cenzer, Auerbach, & Covinsky, 2015). This can be a reciprocal relationship that cognitive impairment increases the risk of functional dependency and, conversely, dependency in daily activities can increase the risk of hospitalization. Considering our findings, cognitive impairment can affect this relationship as a confounding factor affecting both the risk of hospital admissions and the level of function. For instance, dependency in medication management and lack of compliance can impede the improvement process and exacerbate complications, and individuals with cognitive impairment are at higher risk of nonadherence or medication mismanagement (Nazir et al., 2013).
Interestingly, those respondents who were dependent in transferring from bed to chair had significantly less frequent hospital admission. There are some possibilities that can explain this finding, although further research is required. Because the difference in living arrangement between these two groups is statistically significant, the availability of professional care can be considered as one of the factors decreasing hospital admissions.
Also, people with functional independence are less likely to be hospitalized due to pneumonia, as the risk of aspiration is lower compared with those with functional impairments (Mody, Sun, & Bradley, 2006). Our findings also revealed that respondents with lung disease are more likely to be hospitalized because both function and cognitive ability can influence the risk of infectious lung diseases. With regard to living arrangement, Nazir et al. (2013) found a higher risk of rehospitalization among seniors living in the community. Our study showed similar findings that those seniors living in residential centers were less likely (ORs = 0.8, 0.24, 0.19 in Models 1, 2, and 3, respectively) to have frequent hospital admission compared with their counterparts living in the community. Although the difference was not statistically significant in the first model, controlling for function significantly increased the likelihood in the second model. One possible reason for the difference in hospital admission between seniors living in residential centers and the community can be the availability of health care and more professional services in the former as opposed to nonprofessional and informal care provided by family members in the latter. Married people were less likely to have frequent hospital admissions, and although the difference is not statistically significant, the effect of availability of caregivers on repeated hospitalization can perhaps be explored in future research. With regard to ethnicity, Hispanic older adults were at lower risk of hospital admission compared with their non-Hispanic White counterparts. This difference could be attributable to the cultural difference in caregiving between Hispanic and non-Hispanic White Americans, with Hispanic older adults being more likely to receive care from their relatives and to live with them, contrary to their non-Hispanic White counterparts (Greenwald & Naiditch, 2008). Health status, lung diseases, previous surgery, and falling down were the other significant predictors for frequent hospital admission.
Conclusion
In conclusion, our study suggests that the severity of cognitive impairment is significantly associated with the frequency of hospital admission, and even MCI appears to increase the likelihood of hospital admission, which could, in turn, affect further cognitive decline. The results of this study point to some policy implications including the recommendation of administering screening tests such as CDT at the point of hospital admission.
There could be guidelines and training made available for caregivers and providers to help reduce physical and mental complications during hospital admission. Patients admitted due to lung diseases, functional limitations, and those who had surgery can be considered for postdischarge home care services or active case management, in particular for those living alone or staying in their homes. Considering the higher risk of hospitalization, these patients can be susceptible to cognitive impairment following frequent and lengthier hospitalization. These follow-up services may reduce the risk of frequent hospital admission and, consequently, the risk of cognitive impairment, ultimately reducing health care cost and repeated hospitalization.
Going forward, we suggest a longitudinal study focusing on the impact of active case management on hospital admission due to lung disease, falling down, and surgery, as well as considering the residential settings and living environments. Although an intervention is not likely to stop the progress of dementia, it may slow it down or keep it from accelerating. Either way, an intervention could break the cycle of chronic disease, dementia, and hospitalization. Theoretically, this repeated pattern increases costs as well as decreases the quality of life for older patients and their families.
Limitations
Cognitive function could potentially confound the reliability of answers to the questions. Having a proxy respondent for known cases of dementia could reduce this impact. In addition, in the third model, those cases with severe and moderate impairment were excluded from the models. Although the questionnaire asked “hospital stays,” respondents might potentially conflate rehabilitation admissions with hospital admissions. Combining the NHATS data set with hospital data, or adding some questions to request some hospital documents, can increase the reliability of the answers in this regard.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.