
Abstract
Introduction
Social participation is a key modifiable determinant of one’s health and well-being, and a vital component of successful aging (Adams, Leibbrandt, & Moon, 2011; Douglas, Georgiou, & Westbrook, 2016). Thus far, researchers have focused on establishing the causes and consequences of two main types of social participation for older adults—formal and informal. Although formal social participation usually entails involvement in formal groups and organizations in the community, informal social participation refers to the amount of contact and time that one spends with family and friends (van Ingen, 2008). Determinants of social participation such as marital status, income, and/or physical limitations (e.g., Donnelly & Hinterlong, 2010; Pinto & Neri, 2017) tend to differ between formal and informal social participation (van Groenou & Deeg, 2010), but both types of social participation seem to have an overall positive association with health outcomes. Many previous studies have found formal/informal social participation to be protective against negative health outcomes such as mortality and morbidity (e.g., Agahi & Parker, 2008; Tomioka, Kurumatani, & Hosoi, 2017), providing substantial support for countries aiming to increase social participation as a strategy to keep older adults healthy and sustain them as productive members of society (Raymond et al., 2013).
Social participation has been well studied across a range of geographical contexts and health outcomes, but two important limitations in the extant literature remain. First, less is known about whether and how social participation may aid those already in poor health, even though individuals are likely to live a greater proportion of their lives with a chronic condition compared with past generations (Crimmins, 2015). Galenkamp and Deeg (2016) have suitably pointed out that an increase in the prevalence of chronic diseases, together with the rising share of older people in the population, asks for a shift of focus from the “successful” older people with limited disease or disability to those older individuals who live with multiple chronic diseases. (p. 87)
Yet while attempts to establish the determinants of social participation for older adults living with chronic conditions are suitably made (Galenkamp & Deeg, 2016), they do not examine whether and how social participation may affect the well-being of this subpopulation through different pathways than it does among the general population. Second, even though researchers have suggested a wide range of mechanisms through which social participation may operate to influence health outcomes, existing studies seldom test these pathways empirically. Rather, the majority of research has sought to confirm the salubrious effects of social participation on health instead, neglecting to explicitly test and/or clarify the mechanisms through which this association occurs (Thoits, 2011). It, therefore, remains unclear how social participation promotes well-being, even though it is commonly accepted that it does.
One especially pertinent outcome for the chronically ill is health-related quality of life, because chronic conditions have long-term consequences and are often intrusive to everyday life (Schulman-Green et al., 2012). Health-related quality of life is a multidimensional concept that captures aspects of quality of life that are relevant to health, accommodating both subjective and objective perspectives across multiple domains of health (e.g., physical, psychological, etc.; Testa & Simonson, 1996). Health promotion efforts are thus often aimed at maximizing one’s quality of life, and its attendant measures have been used widely to compare and evaluate the effectiveness of health interventions for economic and medical decision making (Kind, Lafata, Matuszewski, & Raisch, 2009). In this context, research aimed at understanding pathways to enhance health-related quality of life can serve to inform future strategies to improve the well-being of older adults living with a chronic condition.
Social participation plays a substantial role in shaping older adults’ quality of life (Gabriel & Bowling, 2004). Participating in activities, maintaining social roles, and developing harmonious relationships help older adults perceive their lives more optimistically (Levasseur, St-Cyr Tribble, & Desrosiers, 2009), and provide a sense of belonging to the community (Aw et al., 2017). Researchers have typically found statistically significant associations between social participation and health-related quality of life, even though the strength of this association appears to vary across studies. While some studies have found the association to be relatively weak (e.g., Levasseur, Desrosiers, & Noreau, 2004; Takada, Sashika, Wakabayashi, & Hirayasu, 2016), others have established a strong association across various populations (e.g., Benka et al., 2016; He et al., 2016; Li, Lin, & Chen, 2011). This variation in effect size may possibly be addressed through a better understanding of its causal pathways, but these have remained largely opaque due to a lack of empirical work on mediating mechanisms.
Self-Management as Mediator
It is thus noteworthy that social participation may be instrumental not only in promoting quality of life by preventing the onset of chronic diseases but also in improving the self-management of these conditions for those already living with a chronic disease. Self-management has been defined as the “ability of the individual, in conjunction with family, community, and healthcare professionals, to manage symptoms, treatments, lifestyle changes, and psychosocial, cultural, and spiritual consequences of chronic diseases” (Richard & Shea, 2011, p. 257). Broadly, it is the way through which older adults manage their resources in daily life to maintain their well-being and remain independent for as long as possible, thus enabling the individual to “age successfully” (Steverink, Lindenberg, & Slaets, 2005). First, self-management training is a well-studied health intervention used by medical professionals to improve patients’ quality of life, with multiple studies supporting its efficacy (Bodenheimer, Lorig, Holman, & Grumbach, 2002; Cochran & Conn, 2008; Jonkman, Schuurmans, Groenwold, Hoes, & Trappenburg, 2016). Systematic reviews of the literature suggest that the central benefit of self-management training is that it enhances participants’ problem-solving skills, which in turn improves their psychosocial and/or mental well-being (Barlow, Wright, Sheasby, Turner, & Hainsworth, 2002; Jonkman et al., 2016). Other salubrious effects include reduced pain and disability (Grady & Gough, 2014), resulting in a better overall health-related quality of life for the individual. In the bigger picture, self-management support constitutes one of six essential elements in the Chronic Care Model, which focuses on improving disease outcomes through system-level changes within the primary health care system (Grady & Gough, 2014). Studies have found that providing better self-management support to patients tends to reduce emergency department visits and length of hospital stays (Bodenheimer, Wagner, & Grumbach, 2002), both of which may reflect improved health-related quality of life (Dominick, Ahern, Gold, & Heller, 2002).
There are several reasons why self-management may function as a major pathway through which social participation improves overall well-being. First, self-management does not occur solely at the level of the individual—its success is often dependent on influence from family and friends (Gallant, 2003). Social participation has been thought to facilitate the exchange of health information and promote better health behavior through social influence and shared norms (i.e., informal social control; Berkman, Glass, Brissette, & Seeman, 2000). In the case of chronic illness, engaging with others in the context of social activity proffers opportunities for friends and family to influence the individual (through reminders, persuasion, or encouragement etc.) into adopting healthy behavior and better management of their chronic condition(s). Furthermore, carrying out activities successfully together with others may also foster a greater sense of control and/or self-efficacy over one’s own life (Thoits, 2011), in turn promoting more active management of one’s condition through exercise and diet (Clark & Dodge, 1999), as well as improved mental health (Mikula et al., 2017). Yet while social participation and self-management have both been independently accepted as important predictors of the health and well-being of older adults, no study to my knowledge has sought to establish self-management as a possible mediator of social participation. Using data from low-income older adults living in Singapore, this study thus builds upon the extant literature on social participation and health and seeks to investigate whether (and to what extent) self-management of chronic conditions mediates the relationship between social participation and health-related quality of life.
The Singapore Context
Singapore is a multi-ethnic city-state in Southeast Asia, with a population of approximately 5.6 million and land area of 719 km2. Yet despite economic prosperity and having built up a strong public infrastructure over the past few decades, Singapore has become one of the most rapidly aging countries in the world, due to its high life expectancy and subreplacement fertility rate (Singapore National Population and Talent Division, 2015). Projected increases in the prevalence of chronic diseases such as diabetes (Phan et al., 2014) have recently become a source of anxiety for the state, due to potential spikes in health care expenditure and losses in productivity. The Singapore government has recently responded by investing in strategies aimed at helping older adults age actively in the community, in the hope that such engagement will prevent and/or delay the onset of chronic illness. However, a history of high reliance on family members for care (Mehta, 2006) and social life means that social participation for older adults continues to be predominantly structured around family interactions (i.e., informal social participation; Aw et al., 2017), rather than participation in formally organized events or activities (i.e., formal social participation). Furthermore, the majority of older adults in Singapore are not English-literate and are likely to face issues managing their illnesses even in basic tasks such as taking prescribed medication correctly (R. Malhotra et al., 2019). As a result, self-management is likely to be a key factor in determining health-related quality of life among older adults. The current study focuses specifically on those from a low-income background, and thus who are more likely to live alone (Gubhaju, Østbye, & Chan, 2018). This subpopulation of older adults is also likely to reap a greater benefit from social participation compared with those with a higher socioeconomic status (Niedzwiedz et al., 2016).
Design and Method
Study Design and Participants
For this study, data from a 2016 survey conducted among low-income, community-dwelling older adults (aged 60 and above) in Singapore were used. Respondents were occupants of public rental flats in one Housing and Development Board (HDB) Estate located near the central region of Singapore, which comprises highly subsidized public housing apartments available exclusively to low-income families earning less than 1,500 Singapore dollars (SGD) a month. Out of 1,908 unique household addresses identified and eligible for the study, 528 were uncontactable. Of the remaining, 928 (67.2%) eligible participants agreed to participate in face-to-face interviews with a structured questionnaire. Respondents free from chronic conditions (including angina/myocardial infarction, any form of heart disease, cancer, cerebrovascular disease, hypertension, diabetes, respiratory illness, digestive illness, ailments of the liver or gall bladder, chronic back pain, osteoporosis, cataract and glaucoma) and/or those with any missing information on the variables of interest were excluded, resulting in a final analytic sample of 600 older adults. In line with past research, the following hypotheses were tested:
Outcome Variable
The EQ-5D-5L was used to measure health-related quality of life (The EuroQol Group, 1990). Having been validated in many countries including Singapore, the EQ-5D-5L consists of two components: (a) the descriptive system assessing five domains (mobility, self-care, usual activities, pain/discomfort, and anxiety/depression) from which an index score can be calculated; and (b) the EQ visual analog scale (EQ VAS). For this analysis, index scores from the EQ-5D health states were computed using Singapore preference weights (Luo, Wang, Thumboo, Lim, & Vrijhoef, 2014).
The range of possible Singapore utility-based EQ-5D index scores is −0.769 to 1.00, where a higher score represents a better state of health (see Abdin, Subramaniam, Vaingankar, Luo, & Chong, 2015). Possible scores for the EQ VAS range from values of 0 to 100, where 0 represents the worst health you can imagine and 100 being the best health you can imagine.
Mediator Variable
The Partners in Health (PIH) scale—a generic self-rated measure of chronic disease self-management—was used to measure self-management. This 12-item scale was recently validated in the Asian context (Chiu, Tam, Siu, Chau, & Battersby, 2017), and is made up of three subscales measuring an individual’s knowledge, coping, and symptom management/adherence in relation to his or her health condition. Examples of items from the scale include “I am able to deal with health professionals to get the services I need” and “I manage the effect of my health condition(s) on my social life.” Each item on the scale was scored from 0 to 8, and possible scores for the PIH scale, therefore, range from 0 to 96. I standardize this measure before including it into the mediation model. The inter-item reliability for this scale in the sample was satisfactory (α = .84).
Predictor (or “Treatment”) Variable
As highlighted earlier, social participation is commonly categorized as formal or informal (Levasseur, Richard, Gauvin, & Raymond, 2010). For formal social participation, respondents were asked how often (in the past 6 months) they had (a) attended a community event organized by grassroots associations (e.g., Resident’s Committee, Community Development Council etc.), (b) took part in activities at Senior Activity Centers, or (c) attended a place of worship (e.g., church, mosque etc.). Informal social participation was assessed by asking respondents how often (in the past 6 months) they had gone out with family members or friends. This variable was dichotomized using the cut-off point of at least once a week in line with previous research establishing a link between social participation and health among Singaporeans and elsewhere (see Ang, 2016; Ng, Broekman, Niti, Gwee, & Kua, 2009; Sørensen, Waldorff, & Waldemar, 2008). The causal mediation framework (explained in further detail below) emulates the experimental setting by splitting the observations into two groups (i.e., treatment and control), and then weighting for self-selection into the groups based on observed covariates. In this case, those with formal/informal social participation levels of at least once a week (coded as 1) were considered the treatment group, while the rest became part of the control group (coded as 0).
Covariates
Covariates used in this analysis include sociodemographic variables such as age, gender (male/female), ethnicity (Chinese/nonChinese), education (no formal education/primary/secondary and above), marital status (not married/married), number of living children, and work status (not working/working). Because the severity of one’s health condition may confound the relationship between social participation and quality of life, several measures of health are also included in the analysis. These are the number of chronic conditions diagnosed by a medical professional (1-2/3+), including the presence of any limitation (no limitation/at least one limitation) in activities of daily living (ADL). ADLs assessed included taking a bath, dressing up, eating, standing up and sitting down from a bed/chair, walking around the house, going out of the house, and using the toilet.
Analytical Strategy
To estimate the effects of social participation on health-related quality of life and how much of this relationship is mediated by self-management, the causal mediation strategy proposed by Imai, Keele, and Tingley (2010) was adopted and executed using the mediation package (Hicks & Tingley, 2011) in STATA 15. The causal mediation strategy employs the counterfactual (or quasi-experimental) framework to identify mediating variables between the predictor (or treatment) and outcome variables, and allow for a causal interpretation of the observed effects even with cross-sectional data. Briefly, the counterfactual framework states that true causal effects can only be estimated after observing realized outcomes from the same individuals under different possible conditions (see Höfler, 2005 for further explanation). Although these effects can never be empirically observed (because only one outcome can be observed from each individual), statistical models adopting this framework attempt to approximate true causal effects from observational data through procedures such as propensity score matching and inverse proportionality of treatment weighting. A total of four separate sequential models using ordinary least squares regression were estimated by type of social participation and health-related quality of life outcome. Furthermore, 5,000 simulations for each model were computed to approximate parameter uncertainty and present the 95% confidence interval (CI) derived from the resulting distribution (Hicks & Tingley, 2011).
Causal interpretation of the model is dependent on an identification assumption termed sequential ignorability, consisting of two parts. First, treatment assignment is expected to be unconfounded (i.e., ignorable). To achieve unconfoundedness with the current observational data, propensity scores of engaging in each type of social participation were estimated using the covariates, and inverse proportionality of treatment weights were constructed and included in the model estimation. This quasi-experimental method approximates random assignment into treatment and control groups by adjusting for the likelihood of an individual self-selecting into the treatment group. In the context of this study, this means that the effects of formal/informal social participation can be interpreted as “treatment effects” as in the experimental context, as if one group was randomly assigned to participate at least once a week while the other served as a control group. The second part of the sequential ignorability assumption builds on the first and further assumes that the observed mediator is also ignorable. To address this, I conduct sensitivity analyses recommended by Imai et al. (2010), also using the mediation package. These sensitivity analyses address the fact that unobserved pretreatment variables may confound the relationship of interest, based on the error terms of the mediator and the outcome. Results showed that for the average causal-mediated effect to equal zero, the two error terms for each model would need to have a correlation of at least .24 (details can be found in Imai, Keele, & Yamamoto, 2010).
Results
Table 1 describes the characteristics of the analytic sample. In all, 32% of the sample participated in formal social activities at least once a week, while 25% participated in informal social activities at least once a week. Respondents reported lower EQ-5D index mean scores than the general Singapore population in a comparable age group (Abdin et al., 2015). EQ VAS scores were also lower than previously observed among diabetes patients (Wang, Tan, Tay, Thumboo, & Luo, 2015). This was anticipated given that in addition to having at least one chronic condition, the sample also comprised low-income older adults. The mean score for the PIH scale was 76.3. The majority of respondents were male (58.3%), of Chinese descent (84.3%), not married (69.8%), not working (66.3%), and had no formal education (47.8%). In terms of health, most respondents had three or more chronic conditions (60.5%). Only a minority reported having at least one ADL (22.2%), but this figure is noticeably higher than those found in previous studies of the general Singapore older adult population (C. Malhotra, Chan, Malhotra, & Østbye, 2011).
Characteristics of the Sample (n = 600).
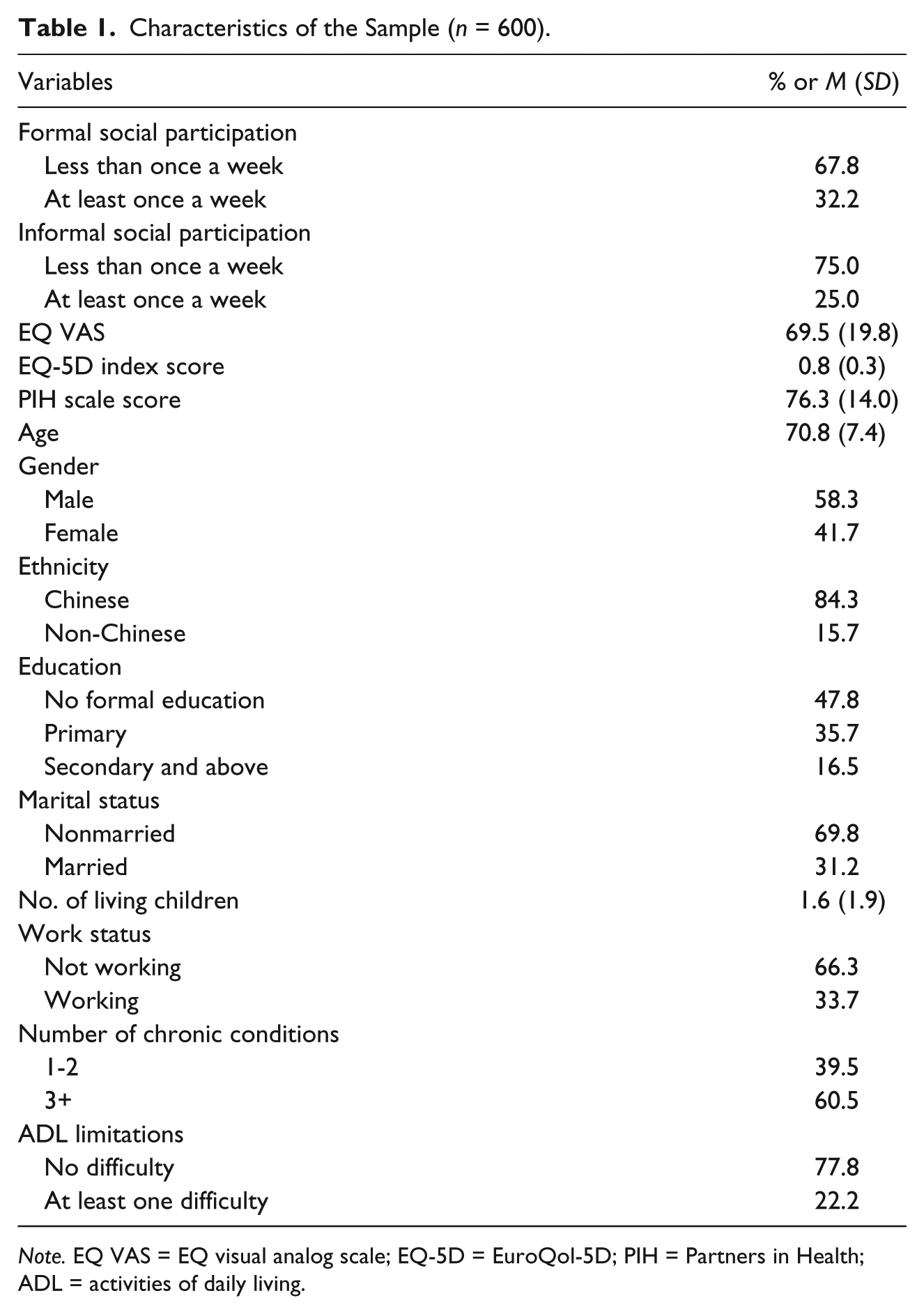
Note. EQ VAS = EQ visual analog scale; EQ-5D = EuroQol-5D; PIH = Partners in Health; ADL = activities of daily living.
Bivariate correlations of the key variables were estimated and are displayed in Table 2. These pairwise correlations provide insight as to what kinds of relationships to expect, before controlling for covariates. Statistically significant correlations were found between the PIH scale score and health-related quality-of-life measures (r = .32 for the EQ-5D index score and r = .31 for the EQ VAS). Informal social participation was also found to be significantly correlated with the PIH scale score (r = .17) and the EQ VAS (r = .10). These correlations imply that the association between informal social participation and health-related quality of life may be mediated by self-management. No significant correlations between formal social participation and the other variables of interest were observed, suggesting that formal social participation may not be associated with self-management or health-related quality of life.
Pairwise Correlations Between the Variables of Interest.

Note. PIH = Partners in Health; EQ-5D = EuroQol-5D; EQ VAS = EQ visual analog scale.
*p < .05.
Results from the full model are shown in Table 3. After controlling for covariates, the mediation model for informal social participation showed a significant total effect on both the EQ-5D index score (β = 0.038) and the EQ VAS (β = 3.613). Approximately 67% (β = 0.026) and 45% (β = 1.667) of the total effects were mediated by the PIH scale score, respectively. The remaining direct effect of informal social participation on health-related quality of life was not statistically distinguishable from zero, suggesting a complete mediation by self-management. The direct and total effects of formal social participation on the EQ-5D index score were significant. Both effects were negative, indicating that net of self-management, formal social participation leads to a decrease in health-related quality of life.
Results From Models Estimating the Mediation of the Social Participation−Quality of Life Association by Self-Management.
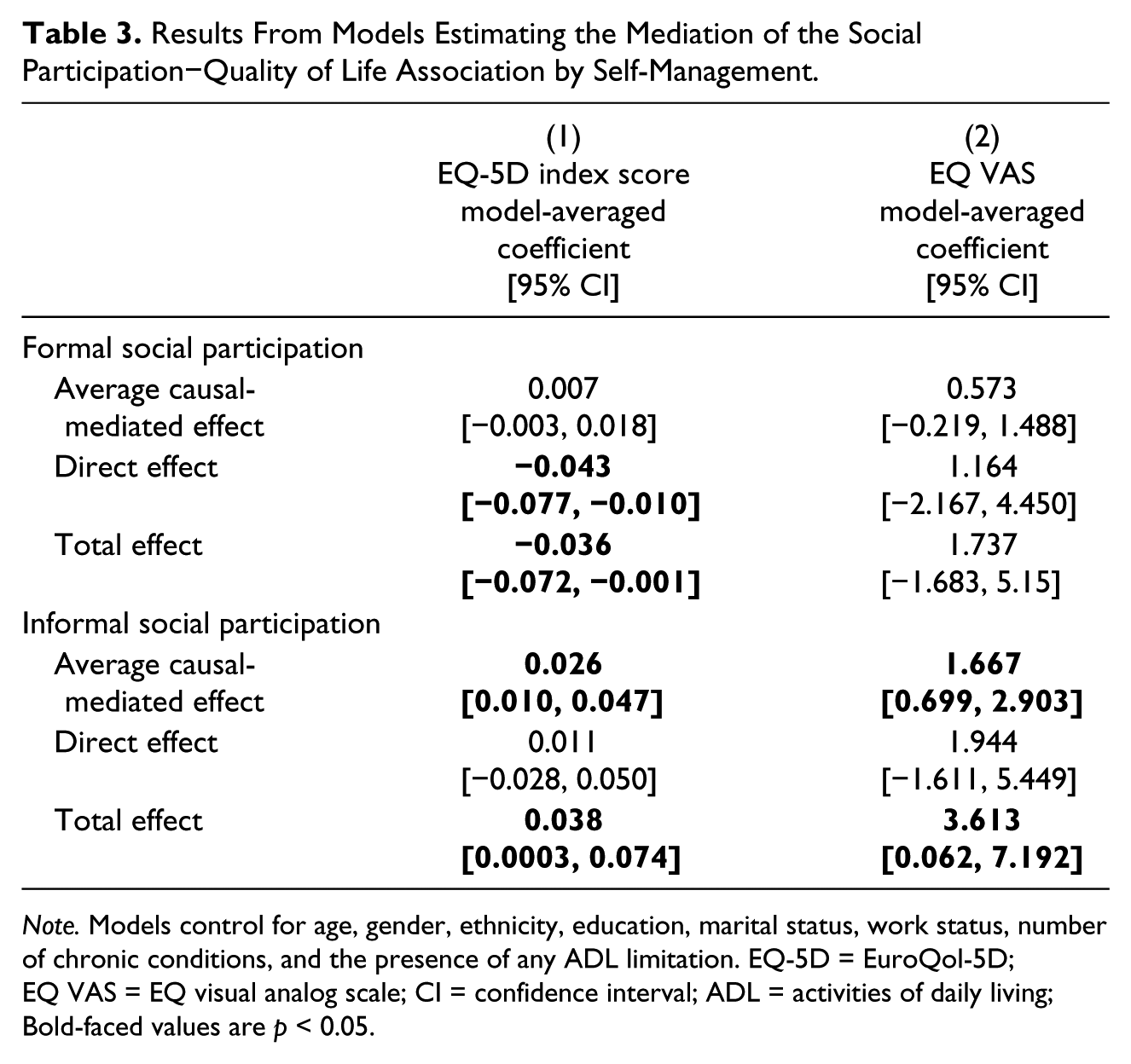
Note. Models control for age, gender, ethnicity, education, marital status, work status, number of chronic conditions, and the presence of any ADL limitation. EQ-5D = EuroQol-5D; EQ VAS = EQ visual analog scale; CI = confidence interval; ADL = activities of daily living; Bold-faced values are p < 0.05.
To juxtapose the effects of social participation by type, path diagrams of the estimated models are presented in Figure 1, focusing on the EQ-5D index score as the outcome. The figure illustrates that self-management “suppresses” (see MacKinnon, Krull, & Lockwood, 2000) the direct effect of formal social participation on the EQ-5D index score. By contrast, the total effect of informal social participation was mediated by self-management. The size of these effects fall within the range of a “minimum clinically important difference (MCID)” for the EQ-5D (MCIDs are scores that indicate the smallest meaningful change for a patient) found in previous studies (Coretti, Ruggeri, & McNamee, 2014), indicating its substantive importance.
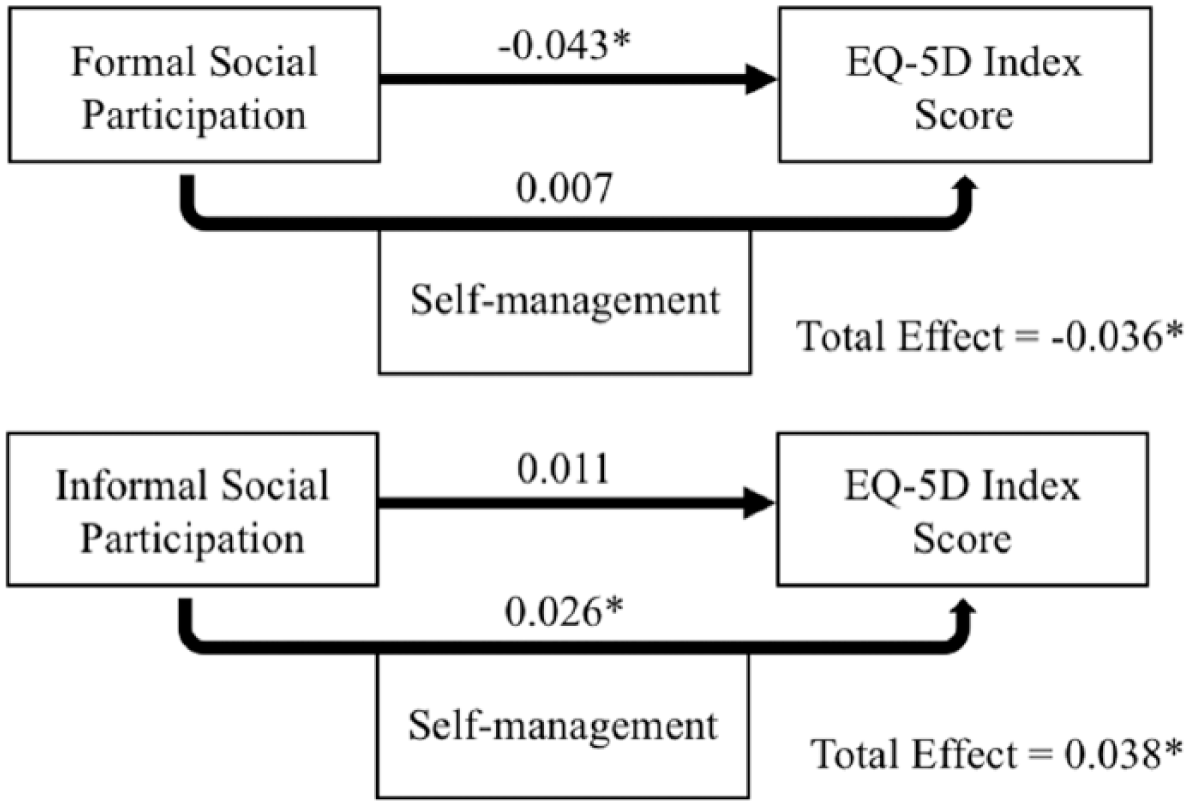
Path diagram between social participation, self-management, and the EQ-5D index score.
Discussion and Implications
The purpose of this study was to determine whether self-management mediates the association between social participation and health-related quality of life, and to what extent. Utilizing the counterfactual framework for causal mediation analysis, evidence supporting the hypothesis that self-management acts as an important pathway and mediator through which social participation affects health-related quality of life was found. This relationship, however, differs by the type of social participation (i.e., formal or informal) considered.
Self-management mediated a large proportion of the total effect for informal social participation, such that the remaining direct effect on health-related quality of life was found to be statistically nonsignificant (i.e., complete mediation). First, this provides support to the theory that increased contact with friends and family promotes well-being primarily through social control mechanisms on health behavior (Thoits, 2011). For individuals with a chronic illness, this translates into better self-management of one’s condition. The findings build upon existing studies suggesting that family involvement in health promotion and intervention are likely to be beneficial for those living with one or more chronic conditions (Martire, Lustig, Schulz, Miller, & Helgeson, 2004). Such an approach may be especially efficacious in countries with a strong emphasis on the family (e.g., Singapore, Hong Kong), where older adults often wish to avoid being a burden to other family members (Cheng, Chan, & Chan, 2008) and may feel a greater propensity to take action toward this end (e.g., by better managing their health). Second, the findings provide insight into how higher rates of hospital readmission and utilization among the low-income population (Low et al., 2016) may possibly be addressed by the health system. Although support from family and friends has been given relatively little attention in the literature on the Chronic Care Model thus far (Davy et al., 2015), findings here suggest that health care providers utilizing the Chronic Care Model to improve care delivery should more carefully consider (and adapt to) the role of informal support from family and friends in promoting self-management and overall well-being (Grady & Gough, 2014; Rosland & Piette, 2010). Finding ways to encourage informal social participation among those with chronic illnesses can improve self-management, which may, in turn, reduce hospital readmission/utilization among the low-income population. Given the strong emphasis on family responsibility in the Singapore context (Mehta, 2006), it is highly likely that self-management is largely shaped through informal social participation, rather than through trainings in formal settings. This is fairly evident in the findings on formal social participation (discussed below).
For formal social participation, self-management appeared to function as an inconsistent mediator (also known as a suppressor; MacKinnon et al., 2000) with the EQ-5D index score (but not the EQ VAS) as an outcome. This suggests that for the formal social participation, its direct (and negative) effect on health-related quality of life appears to be masked by its indirect (and positive) effect through self-management. Only partial evidence for inconsistent mediation was found, however, as the latter (indirect) effect did not achieve statistical significance. The direct negative effect of formal social participation on health-related quality of life (although only on the EQ-5D index score but not the EQ VAS) contradicts the findings of other studies conducted in Asia, where most have found positive effects instead (e.g., He et al., 2016; Li et al., 2011). One possible explanation for this is that given strong ideals of meritocracy in Singapore, low-income individuals are often faced with a challenging institutional environment where they are met with bureaucratic complications and a general lack of empathy toward their plight (Suen & Thang, 2018). Even though social assistance for various needs is available, Suen and Thang (2018) noted that for individuals from low-income groups, “the experience of obtaining social support from formal sources was described [by potential recipients] as being almost tantamount to a violation of their dignity and sense of self-worth.” (p. 12) The general frustration and/or dissatisfaction toward formal organizations may extend to social activities that occur within formal contexts, negating any potential benefits that may be obtained from participating in them. Such an interpretation aligns with Abramson’s (2015) observation that the meaning and efficacy of social participation is often contingent on the organizational context through which it occurs. Therefore, even though prior studies in other countries (e.g., Brody et al., 2002; Wattana, Srisuphan, Pothiban, & Upchurch, 2007) have demonstrated that self-management training can help to improve health outcomes, it is unclear whether conducting this training in a formal setting will be effective within the Singapore context. More attention to how low-income groups engage in formal settings is certainly needed.
Main strengths of this study include the use of a relatively large sample (n = 600) of community-dwelling older adults with at least one chronic condition, as well as the use of a counterfactual framework that is able to support a causal interpretation of mediation mechanisms. In the past, similar studies have typically relied on a sample of a specific disease population and/or a much smaller set of observations (e.g., Benka et al., 2016; Li et al., 2011). A majority of these studies also fail to address reverse causation in their analyses, a notable shortcoming given that social participation and health share a reciprocal relationship (Griffith et al., 2017). This study has attempted to address issues of causality through a quasi-experimental design, but the use of longitudinal data in future research will better support the current findings. Also, while a key limitation of the current study is that data were not drawn from a random sample of all low-income older adults in Singapore, the housing estate under consideration is likely to represent a typical case of low-income elderly in Singapore. As the public rental scheme is administered by the HDB with its strict eligibility requirements, the sociodemographic makeup of public rental flat estates is likely to be similar across regions, especially because housing policy remains a fundamental way through which the Singapore government manages social integration (Sim, Yu, & Han, 2003). It is improbable that there will be substantial differences in accessibility to health care services by geographical area, given Singapore’s small size and efficient health care system. Furthermore, the social participation measures here are not exhaustive, and should not be treated as such. For instance, other forms of informal contact such as phone calls or home visits were not assessed. Those considered in this analyses, however, reflect an important set of social activities in the Singapore cultural context (Aw et al., 2017) that have been used in various national surveys linking social participation to health (Ang, 2016), and are likely to be satisfactorily indicative of total social participation. Finally, certain variables which may lie on the causal pathway such as personal mastery/self-efficacy were not measured in the survey, and thus could not be included in the models. Future research should seek to clarify how these constructs may influence the relationship between social participation, self-management, and health-related quality of life.
In sum, among low-income older adults with at least one chronic condition, informal social participation (but not formal social participation) was positively related to health-related quality of life. Self-management mediated the positive effect of informal social participation on health-related quality of life, but “suppressed” the negative direct effect of formal social participation instead. These results are in line with a prior study finding protective effects for informal social participation against 4-year mortality (Ang, 2016), reflecting the central role of family and friends in determining outcomes for health and well-being. Findings show that this positive effect occurs through self-management—an important pathway to improved well-being among those with chronic illnesses. However, strategies to engage older adults in the community would benefit from further research on causal mechanisms. Insights gleaned from such studies are likely to highlight how best to optimize the benefits from formal social participation (and reduce any of its possible negatives), especially where chronic care is concerned. This is pertinent for members from low-income groups, who are more likely to face both estrangement from family members (Aw et al., 2017) and hostility from formal organizations (Suen & Thang, 2018).
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The author acknowledges use of the services and facilities of the Population Studies Center at the University of Michigan, funded by NICHD Center Grant R24HD041028. The data utilized for this article are from a community survey funded by Singapore Health Services Pte Ltd and Duke-NUS Medical School.