
Abstract
Introduction
Cognitive impairment has a significant impact on mortality and disability of older population. It also weakens quality of life in both patients and their caregivers. According to the estimation, 24.3 million people are suffering from dementia globally further, and 4.6 million new dementia cases are diagnosed every year (Ferri et al., 2005). China had 9.2 million people with dementia in 2010 (Chan et al., 2013), and will have the most people with dementia in the world by 2025 (Ferri et al., 2005). Possible risk factors for cognitive impairment, such as age, gender, lower socioeconomic status (Bogin & Varela-Silva, 2010), and cardiovascular disease (Heys et al., 2009), were reported by previous studies. Furthermore, biological attributes, such as brain size or synaptic connectivity, as well as aspects of life experiences, such as education or occupational characteristics, have been suggested as elements of reserve, protecting against the functional consequences of dementia neuropathology (Stern, 2009). Protection warranted by anatomical attributes has been referred to as brain reserve (Katzman, 1993), and compensatory mechanisms based on innate intelligence and life experience have been defined as cognitive reserve (Fratiglioni & Wang, 2007; Stern, 2002).
Studies in Western countries have demonstrated that an overall high level of mental demands decreased dementia risk (Andel et al., 2005; Dekhtyar et al., 2015; Karp et al., 2009; Kroger et al., 2008). However, some evidence on mental demands in the work environment suggested that some types, but not all, of mental demands may be particularly effective in reducing dementia risk (Then, Luck, Luppa, Thinschmidt et al., 2014). Studies which tested the association between Mental Work Demands (MWDs) and cognitive impairment were rarely seen in Chinese older population.
The Shanghai Aging Study intended to identify the prevalence and the incidence of dementia and mild cognitive impairment (MCI) among a cohort with older adults residing in an urban community in Shanghai, China (Ding et al., 2014). The hypothesis of the current study was that MWDs would be related to late-life cognition.
Method
Recruitment of Participants
The target population was permanent residents who were 50 years old or above in the Jingansi community, Shanghai. Participants were excluded if they were (a) residing in nursing homes or other institutions, (b) suffering from mental retardation or severe schizophrenia abstracted from their medical record or diagnosed by neurologists, or (c) suffering from severe hearing, vision, or verbal impairment so that could not take part in the neuropsychological evaluation. Detailed process of the recruitment has been published elsewhere (Ding et al., 2014).
This study was approved by the Medical Ethics Committee of Huashan Hospital, Fudan University, Shanghai, China. All participants and/or their legal guardian gave their written informed consent to participate in the study.
Demographic Characteristics and Medical History
Participants were interviewed face-to-face by trained research nurses and neurologists to obtain information on their demographic characteristics, including age, gender, education, current average monthly income, weight, and height. The participant’ height and weight were used to calculate the body mass index (BMI: the weight in kilograms divided by the square of the height in meters). Lifestyle factors were also obtained. Living alone was defined as living by oneself without other family members. A current smoker was defined as a person who had smoked daily within the past month. A current drinker has had at least one episode of alcohol drinking weekly during the past year. Their history of chronic diseases, such as physician-diagnosed hypertension, diabetes, and heart disease (including coronary artery disease and arrhythmia), was asked and confirmed from their medical records.
MWDs
Occupational information of each participant was obtained through questionnaire by trained research nurses. Questions included longest held work, work title, and a description of the professional labor. Referring to People’s Republic of China Classification of Occupations ceremony (The National Vocational Classification Ceremony and the Professional Qualification Committee, 2015) and the Occupational Information Network (O*NET; Then et al., 2017; Then, Luck, Luppa, Arelin, et al., 2014; U.S. Department of Labor/Employment and Training Administration, 2017), we matched the participants’ occupations to O*NET 21.2 standard occupational classification categories. The O*NET database was developed by the National Center for O*NET Development (https://www.onetcenter.org/overview.html). It contains 37 documents, and provides a comprehensive set of occupational descriptors including worker requirements, worker characteristics, occupational requirements, experience requirements, occupation-specific information, and workforce characteristics for every kind of occupation. The process of matching the participants’ occupations to O*NET-SOC Codes in “Occupation Data” document was subject to strict standards, such as comparable levels of responsibilities, corresponding task descriptions, and equivalent technical equipment used. Occupations of some participants in our cohort could not be matched to an O*NET-SOC Code because they did not provide their occupational title (such as freelance worker, manager) or there was no corresponding occupational group in the O*NET database (e.g., secretary of the party committee, political work, etc.).
In addition, the “Abilities” document describes the required capabilities of various occupations. O*NET-SOC Code in “Abilities” document is the unique encoding for occupations, which is matched to the previous O*NET-SOC Code in “Occupation Data” document. The specific capabilities required by each occupation are coded by the Element ID, for instance, 1.A.1.a.1 corresponds to the ability of oral comprehension. The O*NET database gives the corresponding data value for the degree of the importance and the demand for each competency of each occupation. We created a MWDs index by using all O*NET descriptor variables of “Cognitive Abilities” at work (O*NET variables 1.A.1.a.1 to 1.A.1.g.2, see Supplemental Tables 1 and 2). To obtain the MWDs index, the average of these variables was calculated (Then, Luck, Luppa, Arelin, et al., 2014). Higher MWDs index refers to high demand of mental work. According to tertiles of the distribution of MWDs index in our cohort, we categorized the MWDs index into three categories: high (index ≥ 3.21), middle (index ≥2.76 and <3.22), and low MWDs (index < 2.76).
Neuropsychological Assessments
Cognitive function of each participant was evaluated by a neuropsychological test battery, which covers domains of global cognition, executive function, spatial construction function, memory, language, and attention. The battery contained (a) Mini Mental State Examination (MMSE), (b) Conflicting Instructions Task (Go/No Go Task), (c) Stick Test, (d) Modified Common Objects Sorting Test, (e) Auditory Verbal Learning Test, (f) Modified Fuld Object Memory Evaluation, (g) Trail-Making Test A and B, and (h) RMB (Chinese currency) test. The neuropsychological tests were administered by study psychometrists according to the education level of each participant. All tests were conducted in Chinese within 90 min. The normative data and detailed description of these tests were reported elsewhere (Ding et al., 2015; M. J. Zhang et al., 1990).
Neurological Exams
Neurologists examined each participant for their motor responses and reflexes. They also administered the Center for Epidemiologic Studies Depression Scale (CESD; J. Zhang & Norvilitis, 2002) and the Zung Self-Rating Anxiety Scale (ZSAS; Zung, 1971) to assess whether each participant met the criteria of having a major depressive (CESD ≥ 16) or anxiety (ZSAS > 44) episode within the past week. Neurologists also administered the Clinical Dementia Rating (CDR; Lim, Chong, & Sahadevan, 2007; Morris, 1993) and activity of daily living (ADL; Lawton & Brody, 1969) scale to obtain information on cognitive complaints and activities of daily living.
Consensus Diagnoses
After each clinical assessment, three study neurologists and one neuroepidemiologist reviewed the functional, medical, neurological, psychiatric, and neuropsychological data and reached a consensus regarding the presence or absence of dementia using Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV; American Psychiatric Association, 1994) criteria. Only those who were not diagnosed with dementia were considered for a diagnosis of MCI, which was defined according to Petersen’s criteria (Petersen, 2004). Diagnosis procedures were reported elsewhere (Ding et al., 2014).
Apolipoprotein (APOE) Genotype Assessment
DNA was extracted from blood or saliva collected from the study participants. APOE genotyping was conducted by the TaqmanSNP method (Smirnov, Morley, Shin, Spielman, & Cheung, 2009). The presence of at least one ε4 allele was defined as being APOE-ε4 positive.
Statistical Analysis
Continuous variables were expressed as the mean and standard deviation, and categorical variables were expressed as frequencies (%). The ANOVA and Kruskal–Wallis were used to compare continuous variables; Cochran–Mantel–Haenszel chi-square was used to compare categorical variables. Two generalized linear models (GLM) were used to detect the association between the MWDs index or levels of MWDs and MMSE score stratified by education background (≤6 years of education, and >6 years of education). Model 1 adjusted confounders of age and gender. Model 2 adjusted for additional confounders, such as current average monthly income, smoking, drinking, living status, BMI, hypertension, diabetes, heart disease, anxiety, depression, and APOE-ε4.
All the p values were estimated in two-tailed tests. Differences were considered to be statistically significant at p < .05. The data analysis was conducted by SAS 9.4 (SAS Institute Inc., Cary, NC, USA).
Results
Demographics, Lifestyles, and Medical History of the Participants With Different Cognition
From January 2010 to December 2012, the Shanghai Aging Study recruited 3,836 participants with the response rate of 70% among the eligible population. There was no statistical difference of sex, age, or educational attainment between the participants and nonparticipants. We excluded 290 (7.6%) participants (58 occupations) due to the incomplete occupational data. Among 3,546 participants, 1,569 (44.3%) were men. The mean age of all participants was 70.4 (SD = 8.9) years and the mean year of education was 11.7 (SD = 4.2) years. The interval between date of retirement and current survey period was 13.1 (SD = 8.8) years. Six hundred forty-one (23.2%) participants were diagnosed as MCI, while 145 (4.2%) were diagnosed as dementia. Characteristics, such as age, retirement length, education, score of MMSE and ADL, BMI, current average monthly income, alcohol drinking, history of heart disease, hypertension, diabetes, anxiety, and depression, were found to be significantly different across groups with cognitive normal, MCI, and dementia (Table 1).
Demographics, Lifestyles, and Medical History of the Participants With Cognitive Normal, MCI, and Dementia.

Note. MCI = mild cognitive impairment; BMI = body mass index; ADL = Activity of Daily Living scale; MMSE = Chinese Mini Mental State examination; APOE = apolipoprotein. The p value is for the comparison among three groups of participants with cognitive normal, MCI, and dementia.
MWDs of Groups With Dementia, MCI, and Cognitive Normal
The average MWDs index of all the participants was 2.9 (SD = 0.4), with the range from 1.8 to 4.2. Participants with dementia had a significantly lower MWDs index (2.8, SD = 0.5) than those with MCI (2.8, SD = 0.5) and cognitive normal (2.9, SD = 0.4; p < .001). The distribution of MWDs level was significantly different across the three groups (p < .001). Low MWDs level was reported among 44.1% of participants with dementia, while high MWDs level was reported among 25.5% of participants with normal cognition (Table 2).
MWDs of the Participants With Cognitive Normal, MCI, and Dementia.

Note. MCI = mild cognitive impairment; MWDs = mental work demands. The p value is for the comparison among three groups of participants with cognitive normal, MCI, and dementia.
Association Between MMSE Score and Age by Different Levels of MWDs
MMSE scores in groups with different level of MWDs decreased by increasing age (p trend < .001). MMSE scores in group with low MWDs level decreased more dramatically by increasing age than that in groups with middle and high MWDs level (p < .001). There was no significant difference of the MMSE scores between groups with middle MWDs level and high MWDs level (p = .177; Figure 1).
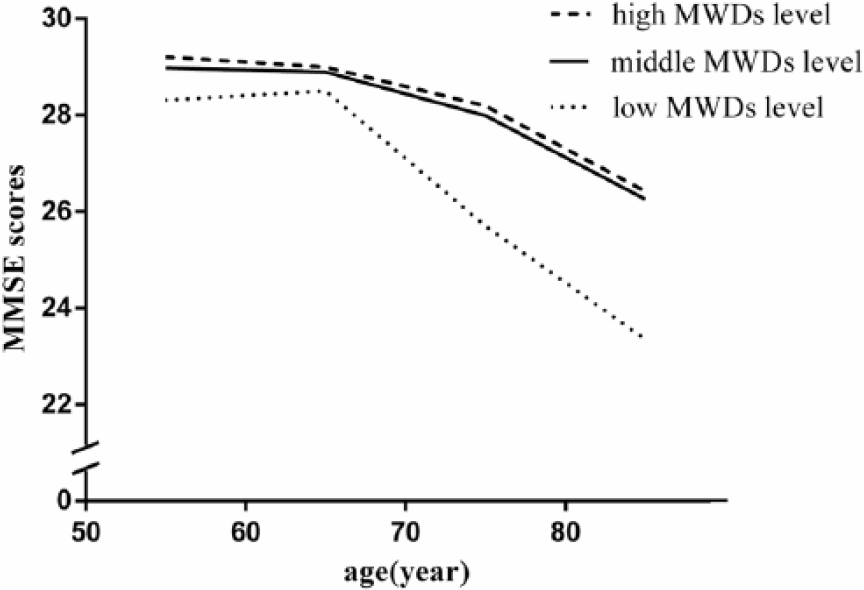
Association between MMSE scores and increasing age by different levels of MWDs.
Association Between MWDs and MMSE Score
In a subgroup of participants with more than 6 years of education, findings of multivariate analyses using GLM supported a positive correlation between mental demands (continuous variable of MWDs index or levels of MWDs) and MMSE score after adjusting for gender and age (Model 1, p < .001), and adjusting for gender, age, BMI, current average monthly income, living alone, cigarette smoking, alcohol drinking, anxiety, depression, heart disease, hypertension, diabetes, and APOE-ε4 (Model 2, p < .001). However, the significant difference was not found in a subgroup with education ≤6 years (Table 3).
Correlation Between MWDs Index and MMSE Score by Generalized Linear Model Analysis.

Note. Model 1: generalized linear model, adjusted for gender and age. Model 2: generalized linear model, adjusted for gender, age, BMI, current average monthly income per person, living alone, cigarette smoking, alcohol drinking, anxiety, depression, heart disease, hypertension, diabetes, and APOE-ε4. MWDs = mental work demands; MMSE = Mini Mental State Examination; BMI = body mass index; APOE = apolipoprotein.
Discussion
Our study indicated a positive correlation between MWDs and late-life cognitive function among older Chinese, especially in those with more than 6 years of education. One advantage of our study is the reliable diagnosis of cognitive function conducted by neurologists of top institution of neurology in China. Another advantage is that we used O*NET ratings to indicate workers’ MWDs index instead of workers’ perceptions. The O*NET database contains information on hundreds of standardized and occupation-specific descriptors, and O*NET-SOC Code Connector makes it easy to match job orders to an occupation in the O*NET-SOC system. Other advantages include the population-based study design, large sample size, and adjustment with confounders of genetic, socio-demographic characteristics, health behaviors, and medical conditions.
Our result is consistent with most of previous studies. In a U.S. case-control study, cases aged more than 60 years were recruited from clinical settings and the community and enrolled in the Alzheimer’s Disease (AD) Research Center Registry of University Hospitals of Cleveland/Case Western Reserve University, whose occupational demands were coded according to the fourth edition of the Department of Labor’s Dictionary of Occupations (DOT); mental occupational demands were found to be lower and physical occupational demands higher for 122 AD cases than for 235 control subjects using repeated-measures ANCOVA adjusted for race, gender, year of birth, and education (Smyth et al., 2004). In a case-control study of 10,079 members of the population-based Swedish Twin Registry who were participants in the HARMONY study, the result controlling for age, gender, level of education, and complexity of work with data and things suggested that higher complexity of work with people was protective against AD only (odds ratio [OR] = 0.78; confidence interval [CI] = [0.63, 0.98]), higher complexity of work with people between twins was associated with lower risk dementia (OR = 0.44; 95% CI = [0.20, 0.97]), and twins with higher complexity of work with people were at a lower risk of dementia (crude OR = 0.27; 95% CI = [0.08, 0.98]) when considering only monozygotic twin pairs. The scores reflect those from the fourth edition of the Dictionary of Occupational Titles (Andel et al., 2005).
Previous prospective studies showed similar results. Members of the NAS-NRC Twins Registry of World War II Veterans received a clinical evaluation for dementia and had job ratings from the Dictionary of Occupational Titles. After covarying for education, the results indicated that lower dementia risk was associated with greater job demands of reason (hazard ratio [HR] = 0.74, 95% CI = [0.56, 0.98]), mathematics (HR = 0.74, 95% CI = [0.58, 0.96]), language (HR = 0.76, 95% CI = [0.58, 0.99]), and vocational training (HR = 0.76, 95% CI = [0.61, 0.95]) in Cotwin-control models (n = 220 pairs), and with comparable results in case-control models (n = 425 cases). These effects were significant among twin pairs discordant for 6 or more years, but not among those discordant between 3 and 5 years. The results also suggested that dementia was not associated with greater demands of work with data, people, or things (Potter, Helms, Burke, Steffens, & Plassman, 2007). A Maastricht Aging Study (MAAS) recruited 630 men and women aged 50 to 80 years, who exhibited no cognitive impairment at baseline (1993-1995) and had mentally demanding job ratings from a job title scheme used at Statistics Netherlands, and there was a first 3-year follow-up examination (1996-1998); persons with mentally demanding jobs had lower risks of developing cognitive impairment during follow-up (36 cases), compared with persons without such jobs (HR = 0.79, 95% CI = [0.65, 0.96]) after controlling for age, sex, educational level, employment status, and length of follow-up interval (Bosma et al., 2003). The Canadian Study of Health and Aging (CSHA) was a representative population study of 3,557 persons aged 65 years or older, from 1991 to 2001 (400 with incident dementia cases: 299 with Alzheimer’s disease and 93 with vascular dementia), and the Canadian Standard Occupational Classification codes were used. In Cox regression models fully adjusted for sex, education, work-related physical activity, leisure physical exercise, hobby, alcohol consumption, smoking, family history of dementia, history of hypertension, history of diabetes mellitus, and history of coronary heart disease, the results suggested that high complexity of work with people or things reduced risk of dementia (HR = 0.66, 95% CI = [0.44, 0.98] and HR = 0.72, 95% CI = [0.52, 0.99], respectively) but not AD. For vascular dementia, HR were 0.36 (95% CI = [0.15, 0.90]) for high complexity of work with people and 0.50 (95% CI = [0.25, 1.00]) for high complexity of work with things. High complexity of work appears to be associated with risk of dementia, but effects may vary according to subtype (Kroger et al., 2008). In the longitudinal AgeCoDe study, patients aged 75+ years were recruited from general practitioners and participated in up to seven assessment waves (every 1.5 years), whose every occupational title was coded according to the 2010 Standard Occupational Classification of the O*NET database. Among 2,315 patients, a significantly lower dementia risk was observed in individuals with a higher level of “information processing” (HR = 0.89, 95% CI = [0.79, 0.99]), “pattern detection” (HR = 0.88, 95% CI = [0.78, 0.99]), “mathematics” (HR = 0.88, 95% CI = [0.78, 0.99]), and “creativity” (HR = 0.88, 95% CI = [0.78, 0.99]) after adjusting for education, gender, depression, hypertension, and having had a stroke. Yet, exposure-dependent effects were only significant for “information processing” and “pattern detection.” The longitudinal observations suggest that dementia risk may be reduced by some but not all types of MWDs. After adjusting for age, gender, depression, hypertension, and having had a stroke, its cross-sectional study showed similar results, however, which showed negative result after adjusting for additional education (Then et al., 2017).
People spend a considerable part of their adult life in their occupation, making intellectual stimulation inherent to occupation of particular interest. Complex work environments that reward cognitive effort and require decision making may motivate individuals to continue to develop their intellectual capacities (Schooler, 1984; Schooler, Mulatu, & Oates, 1999). In this sense, higher levels of mental demands—as brought about by technological changes in the working environment—may also have beneficial effects for the society as they could increase cognitive capacity levels and might even delay cognitive decline in old age (Then, Luck, Luppa, Arelin, et al., 2014). Occupations with high mental demands may represent a form of mental exercise that supports brain function in older adulthood (Katzman, 1995; Orrell & Sahakian, 1995), and may thus affect cognitive performance in older adults.
One possible process either involves a direct neuroprotective effect or involves an effect on brain reserve, thus delaying symptoms of cognitive decline, through which mental stimulation at work affects cognitive function (Katzman, 1993; Satz, 1993). It suggested that brain reserve may be affected by further change during adulthood, instead of full development in early life and stable thereafter. Another possible process through which mental stimulation at work has an effect on cognitive decline might be that cognitive aging occurs earlier in the life-course of persons with low MWDs, because of being highly vulnerable to more proximate medical, biological, behavioral, or psychosocial stressors (Elias, Elias, & Elias, 1990; Houx & Jolles, 1994; Jolles, Houx, van Boxtel, & Ponds, 1995).
Some limitations exist in our study. First, we cannot draw the causation between MWDs and cognitive impairment based on the current study with a cross-sectional design. It might be that jobs with higher “MWDs” attract people with lower dementia risk (greater cognitive reserve, higher lifelong cognitive performance). Thus, a long-term cohort study beginning in middle age would be needed to assess this alternative hypothesis. Second, similarly with the previous German study (Then, Luck, Luppa, Arelin, et al., 2014), we created a MWDs index by using all O*NET descriptor variables of “Cognitive Abilities” at work. However, in a later published paper, the same team authors selected O*NET descriptors for analysis which comprised “cognitive abilities” with the variables 1.A.1.a.1–1.A.2.c.3 and “skills and worker requirements” with the variables 2.A.1.a–2.B.5.d and 4.A.1.a.1–4.A.4.c.3 (Then et al., 2017). Therefore, our MWDs measurement may be less comprehensive without considering domains other than “cognitive abilities.” Third, we did not collect ones’ innate intelligence and life experience (e.g., hobbies, interests, leisure activities), which could also reflect cognitive reserve. Education is an important confounder due to its relation to cognition. Some researchers have found that occupation may be particularly interesting with respect to examining the potential association between intellectual stimulation and subsequent dementia, because people generally spend a substantial portion of their adult years at work (Andel et al., 2005). After stratifying by participants’ education background, we found a positive correlation between MWDs index and MMSE score, only in those with more than 6 years of education. Significant correlation could not be found in subgroups with low education, due to the very small sample size. Fourth, we have adjusted as many as potential confounders in the GLM, but still cannot exclude the possible influence of uncollected confounders. Fifth, epidemiological study only can provide a clue of phenomenon significant, such as the correlation between MWDs and MMSE score. Further studies with research of mechanism of brain reserve may present the clinically significant. Finally, our study site lies in the center of urban Shanghai and the residents had better jobs than most of others in China. Thus, our results cannot be generalized to the whole Chinese population.
Our results suggest that long-time mental work stimulation during adulthood would have potential benefits to late-life cognition. The association between MWDs and cognitive impairment needs to be further validated by long-term prospective studies with larger sample size in older population.
Supplemental Material
Supl_Table_1and2_JAH-17-497.R3 – Supplemental material for Mental Work Demands and Late-Life Cognitive Impairment: Results From the Shanghai Aging Study
Supplemental material, Supl_Table_1and2_JAH-17-497.R3 for Mental Work Demands and Late-Life Cognitive Impairment: Results From the Shanghai Aging Study by Xiaoniu Liang, Zhao Chen, Xinqi Dong, Qianhua Zhao, Qihao Guo, Li Zheng, Wei Deng, Jianfeng Luo, and Ding Ding in Journal of Aging and Health
Footnotes
Acknowledgements
The authors thank all the neurologists, coordinators, research nurses, and technicians for their hard field work and all participants for their cooperation.
Authors’ Note
The authors can share their relevant raw data supporting their findings. If any scientist wishes to use them for non-commercial purposes, without breaching participant confidentiality, he or she can contact the authors directly, and they will share their raw data freely with him or her.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was funded by Shanghai Brain-Intelligence Project from STCSM [grant number 16JC1420500], Scientific Research Project from STCSM [grant number 17411950701, 17411950106], Natural Science Foundation and Major Basic Research Program of Shanghai [grant number 16JC1420100], and National Natural Science Foundation of China [grant number 81773513].
Supplemental Material
Supplementary material is available for this article online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.