
Abstract
Keywords
Introduction
The caregivers of persons with dementia (PWDs) are typically the spouses or children. Family caregivers devote much of their time to helping PWDs with daily activities, allowing them to remain living at home for a longer time. Considering the irreversible and progressive nature of dementia, providing care for PWDs is a long and costly process, which can lead to changes in caregivers’ roles and responsibilities (Ducharme et al., 2009), and these changes can negatively affect caregivers’ physical and psychological health up to a significant sense of distress (Richardson, Lee, Berg-Weger, & Grossberg, 2013). Spousal caregivers’ distress is determined by different factors highlighted in the model developed by Wawrziczny et al. (2017; see Figure 1). Each factor (in bold below) was built by the combination of variables (in italic below) such as
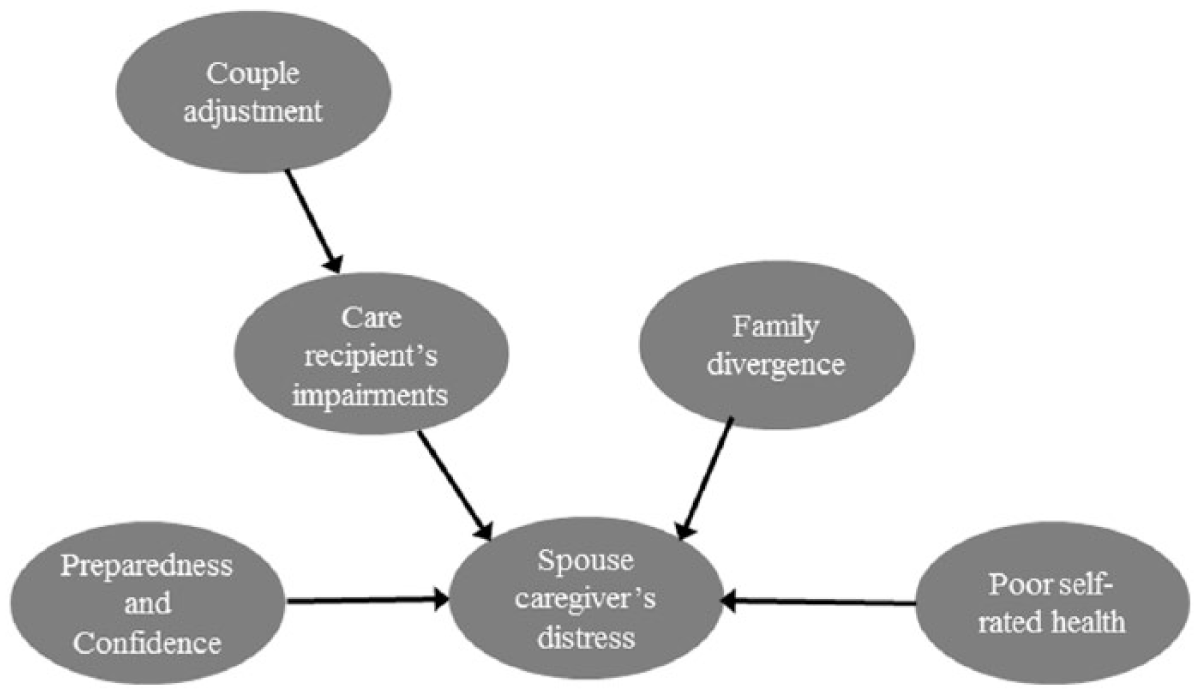
Moderated-mediator model of spousal caregiver distress (Wawrziczny et al., 2017).
These variables have been studied and can be backed by a therapeutic approach. Indeed, caregivers want to receive information regarding the ways in which they can manage PWDs’ challenging behaviors (Scott, Lewis, Loughlin, & Chambers, 2005) and caregiving situations for which they often feel insufficiently prepared (Ducharme et al., 2009). Caregivers also need to identify a social support network and ways to seek help when needed (Wawrziczny, Pasquier, Ducharme, Kergoat, & Antoine, 2017b). Finally, the progressive focus on the disease leads caregivers to a loss of identity markers and an increase of protective behaviors with the PWD until a difficult adaptation occurs at the level of help (Wawrziczny, Antoine, Ducharme, Kergoat, & Pasquier, 2016). These elements underline the importance of supporting caregivers’ transition to their new role. To this end, different types of caregiver interventions have been suggested, such as respite, support groups, psychotherapy, psychoeducational programs, and combined interventions (Brodaty, Green, & Koschera, 2003; Huis In Het Veld, Verkaik, Mistiaen, van Meijel, & Francke, 2015; Pinquart & Sörensen, 2006; Sörensen & Conwell, 2011; Sörensen, Pinquart, & Duberstein, 2002; Zarit, Bangerter, Liu, & Rovine, 2017). These interventions have mainly focused on reducing caregivers’ levels of depression, anxiety, stress, burden, and distress (Martín-Carrasco et al., 2009) by learning effective coping strategies aimed at managing PWDs’ care demands and caregiving situations in a more effective way (Cooper, Balamurali, Selwood, & Livingston, 2007; Elvish, Lever, Johnstone, Cawley, & Keady, 2013). Systematic reviews of support interventions have reported inconclusive and inconsistent results due to protocols and outcome variables that are too different to compare (Dam, de Vugt, Klinkenberg, Verhey, & van Boxtel, 2016; Huis In Het Veld et al., 2015; Pendergrass, Becker, Hautzinger, & Pfeiffer, 2015; Pinquart & Sörensen, 2006; Thompson et al., 2007). Despite the mixed results, two results appear to be constant: Multi-component interventions are most effective in relation to social support and well-being outcomes and psycho-education is integrated in most effective support interventions.
Moreover, an excessive focus on the caregiving situation also leads caregivers to give up activities that are important to them, eventually leading them to exhaustion (Brodaty & Hadzi-Pavlovic, 1990), more than positive emotions related to the caregiving situation, such as pleasure, gratification, or utility. Caregivers need to unwind and break their sense of isolation (Wawrziczny et al., 2017b). Caregivers show also difficulties in accepting external events (e.g., diagnosis, PWD’s deficits, behaviors, disturbances, etc.) and internal situations (e.g., emotions or thoughts). This failure to accept is associated with avoidant coping strategies that are ineffective for managing caregiving situations and may lead to increased feelings of distress (Márquez-González, Romero-Moreno, & Losada, 2010). The combination of mindfulness and education has been shown to reduce stress among caregivers (Oken et al., 2010), while a program for caregivers using Acceptance and Commitment Therapy (ACT) decreased depressive and anxious symptoms and significantly reduced experiential avoidance (Losada et al., 2015). Whereas classical interventions are mainly distress-centered, the ACT approach allows an emphasis on positive experiences and promotes the caregivers’ resources (Márquez-González et al., 2010).
Finally, the disease weakens the balance within the couple, as the rules established to recognize each other as a couple are no longer respected and new modes of interaction affect the relationship, the communication, the dyadic adjustment, and intimacy (Wawrziczny, Antoine, et al., 2016). Moreover, to decrease anxiety, the couple no longer plans for the future, such as preparing for the evolution of the disease and other future needs (Wawrziczny, Antoine, et al., 2016). Interventions have been implemented with couples and have targeted the relational dynamic between the two partners. Notably, Whitlatch, Judge, Zarit, and Femia (2006) emphasized the importance of practicing effective communication techniques, exploring the emotional significance and relational problems caused by the disease, and engaging in a reflection on future preferences for care.
The present study aimed to construct and test the effects of a customized intervention using a quasi-experimental design where a comparison group was recruited at a different time. This intervention combines three types of intervention strategies, that is, classical psychoeducational, ACT, and couple interventions, in an original way. The focus is on spouse caregivers, following Pinquart & Sörensen (2006, 2011), who revealed differences between the experiences of spouse and adult-child caregivers, with interventions having different effects depending on the type of relationship with PWD.
The goal of the present intervention was to reduce spouse caregivers’ distress by acting on the determinants of distress outlined in the spouse caregiver distress model developed by Wawrziczny et al. (2017). We expected our intervention to decrease the perceived severity of problems with PWD’s daily functioning (Hypothesis 1); to improve the sense of self-efficacy (Hypothesis 2) and preparedness (Hypothesis 3); to increase caregiver self-esteem related to the caregiving situation (Hypothesis 4); to decrease the impact of the caregiving situation on caregiver’s health (Hypothesis 5), day-to-day organization (Hypothesis 6), finances (Hypothesis 7), and family support (Hypothesis 8); to increase marital adjustment (Hypothesis 9); to decrease anxiety (Hypothesis 10) and depression (Hypothesis 11); and to decrease psychological distress (Hypothesis 12).
Method
The Customized Intervention
The intervention was designed to adapt to the needs and challenges of each caregiver. Indeed, interventions may be more effective if they are more flexible and customized, and combine several types of strategies to meet caregivers’ needs (Brodaty et al., 2003; Mittelman, Roth, Coon, & Haley, 2004; Zarit & Femia, 2008). The protocol of Belle et al. (2006) is very interesting in this respect: an initial assessment guided the selection of key components of the intervention designed to address the individual participant’s difficulties. From this perspective, 21 intervention modules were built on the basis of the spouse caregiver distress model developed by Wawrziczny et al. (2017) and can be used or not according to a preliminary diagnosis of the situation of the caregiver. Each module tackles a theme or issue through an exercise or scenario (see Supplemental Table).
Seven modules based on the work developed by Ducharme et al. (2011) aimed to facilitate role transition by covering the following themes: caregiver perceptions of the care situation, coping strategies, use of strengths and experience in PWD caregiving, and help-seeking.
In addition, nine modules based on ACT and mindfulness, with an emphasis on acceptance, aimed to increase psychological flexibility and promote caregivers’ engagement in values important for their well-being (Harris, Hayes, Penet, & Milleville, 2012) by limiting avoidance strategies and focusing attention on functional rather than dysfunctional aspects and on caregivers’ resources.
Finally, five modules addressed the couple relationship and aimed to help caregivers take advantage of their time with the PWD, to promote better communication within the couple, to achieve better mutual understanding, to reduce conflict, and to address fears for the future and engage in a reflection related to the evolution of the disease (Whitlatch et al., 2006). These modules may be implemented with both partners, but as the intervention was mainly spouse caregivers–oriented, the couple modules were proposed to the PWD if the caregiver agreed to invite him or her and according to the PWD’s residual cognitive skills.
The intervention consisted of seven weekly home sessions with an average duration of 1 hr 30 min. An initial semistructured interview, conducted by a therapist, allowed to identify spouse caregivers’ needs and difficulties and to select the modules to implement during the sessions (see Supplemental Table). Two or three modules were discussed during each session. Some of them were considered priorities for all caregivers, as they refer to needs and difficulties expressed by the majority of caregivers (evaluate and reduce feelings of exhaustion, identify the support network, future, caregiver’s charter, values related to the caregiving role, managing difficult situations; Wawrziczny et al., 2017b). Two workbooks, one for the therapists and one for the spouse caregivers, containing exercises to implement between each session, were developed to facilitate active participation and optimize the effect of the intervention (Pinquart & Sörensen, 2006). Indeed, when performed between sessions and discussed in the following session, the exercises allow reinforcement of the resources and strategies activated during the sessions. The seven therapists were psychologists with clinical experience in gerontology and trained in ACT. The protocol duration was 10 weeks on average (approximately one step per week: preliminary evaluation, questionnaires prior to intervention T0, seven weekly sessions, postintervention questionnaires T1).
Participants
To be included in the intervention, caregivers had to be the spouse of a person with Alzheimer’s disease (AD) or a related type of dementia (mixed dementia, frontotemporal dementia, Lewy body dementia) and had to live with the PWD.
Participants were recruited from the active clinical queues of the National Reference Center for Young Alzheimer’s (NRCYA) and the Memory Resource and Research Centers (MRRC), which allowed us to obtain and compare the characteristics (caregiver gender, PWD’s Mini-Mental State Examination [MMSE] score, and the delay between the first signs of dementia and the interview) between the final sample of participants and those who refused to participate in this study.
Patients were diagnosed by a doctor at these centers based on criteria outlined by McKhann et al. (2011), clinical criteria, and neuroimaging and neuropsychological data. Patients also underwent a MMSE conducted by one of the center’s neuropsychologists.
A total of 231 caregivers were contacted (90 for the control group and 141 for the experimental group), 86 of whom declined to participate in the study (see Figure 2). Among the eligible respondents (83 in the control group and 62 in the experimental group), 36 (10 in the experimental group and 26 in the control group) dropped out due to time conflicts, potential disruptions to the PWD during visits, and other changes in their situation. Seven participants who had incomplete questionnaires were excluded. Eventually, 102 participants were included in the analyses: 51 participants in the control group and 51 in the experimental group who attended all seven intervention sessions.
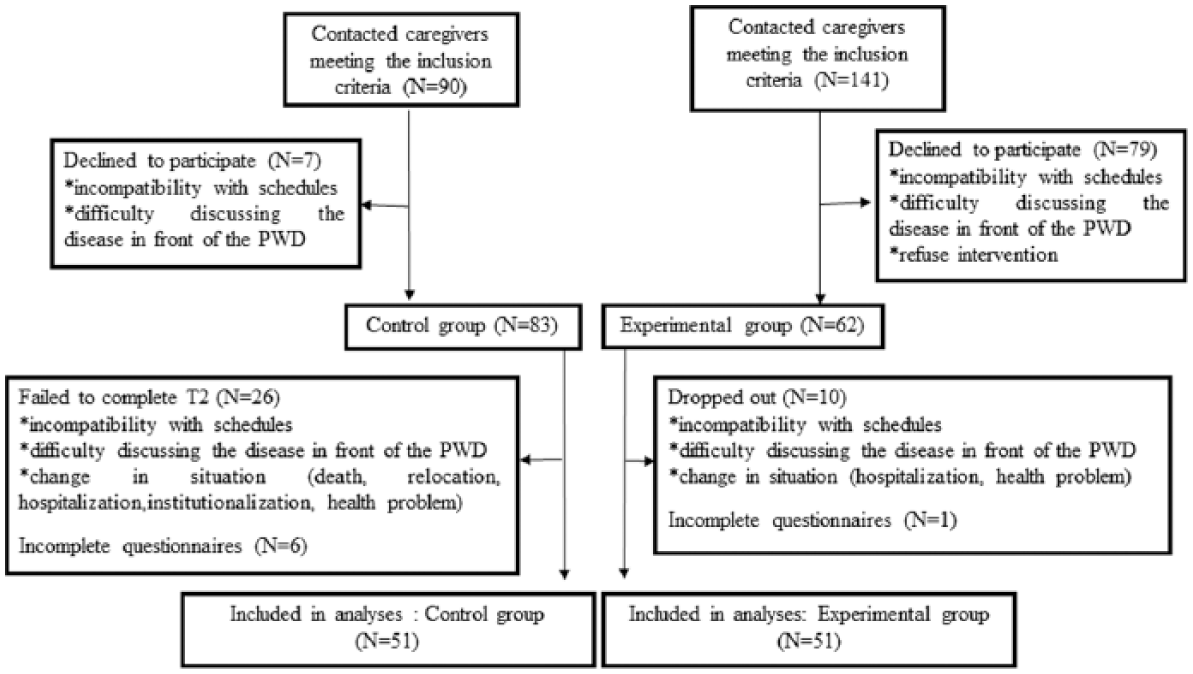
Participant flow diagram.
In the control group, 50% of the PWDs were diagnosed with AD or a related dementia, that is, 47.92% with mixed and 2.08% with frontotemporal dementia. In the experimental group, 50% were diagnosed with AD, 36.96% with mixed dementia, 2.17% with Lewy body dementia, and 10.87% with frontotemporal dementia.
Procedure
Participants were called by the intervention coordinator, who explained the intervention’s goals and procedures and requested their agreement to participate. We recruited participants at different times to constitute an experimental group and a control group (receiving usual support). The usual support for caregivers is to meet with a nurse or a social professional in the center to obtain information about available services and to provide occasional advice either by telephone or during visits to the clinics. The effects of the intervention were examined using questionnaires completed by the caregivers immediately after the intervention (T1), and these results were compared to their responses at baseline before the intervention (T0).
Ethical Issues
The study was approved by the National Ethics Committee and adhered to the tenets of the Helsinki Declaration of 1975. The participants received an informational letter and a verbal explanation of the study details, and all those who agreed to participate in the study signed a consent form.
Statistical Analyses
The analyses were performed using SPSS (IBM, Armonk, NY). In Step 1, we compared nonrespondents and the final sample using Student’s t tests and chi-square tests.
In Steps 2 and 3, we tested whether the two groups in the final sample (experimental and control groups) were equivalent at T0, using Levene’s test to verify the homogeneity of the variances (Levene’s test, p > .05). Step 2 pertained to the sociodemographic data. We calculated the means, standard deviations, and percentages for the two groups (see Table 1). Student’s t tests and chi-square tests were performed to compare the two groups regarding continuous and categorical variables, respectively. Step 3 concerned the outcome variables. We performed an independent-samples Student’s t test on all 11 outcome variables at T0 (see Table 2). We applied Bonferroni correction and considered outcome variables significant at p < .05/11 = .004 (Bonferroni-corrected, p = .004). As the significant variables at T0 (delay between first signs and interview and anxiety) were found to be correlated with various outcome variables, these factors were controlled for in all subsequent analyses.
Sociodemographic Characteristics of the Experimental and Control Groups.
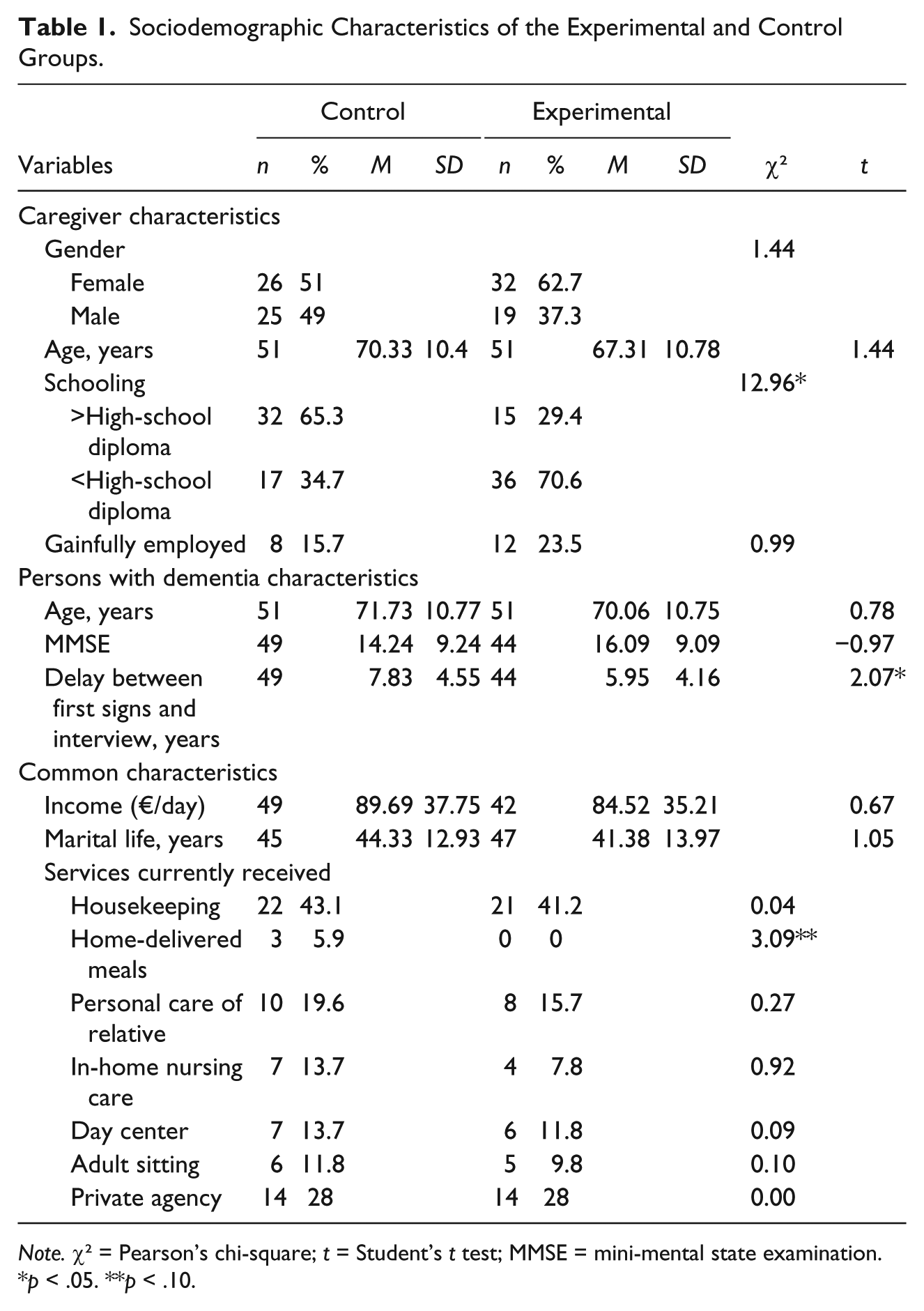
Note. χ² = Pearson’s chi-square; t = Student’s t test; MMSE = mini-mental state examination.
p < .05. **p < .10.
Comparison of Group Means at T0 Between the Control and Experimental Groups.
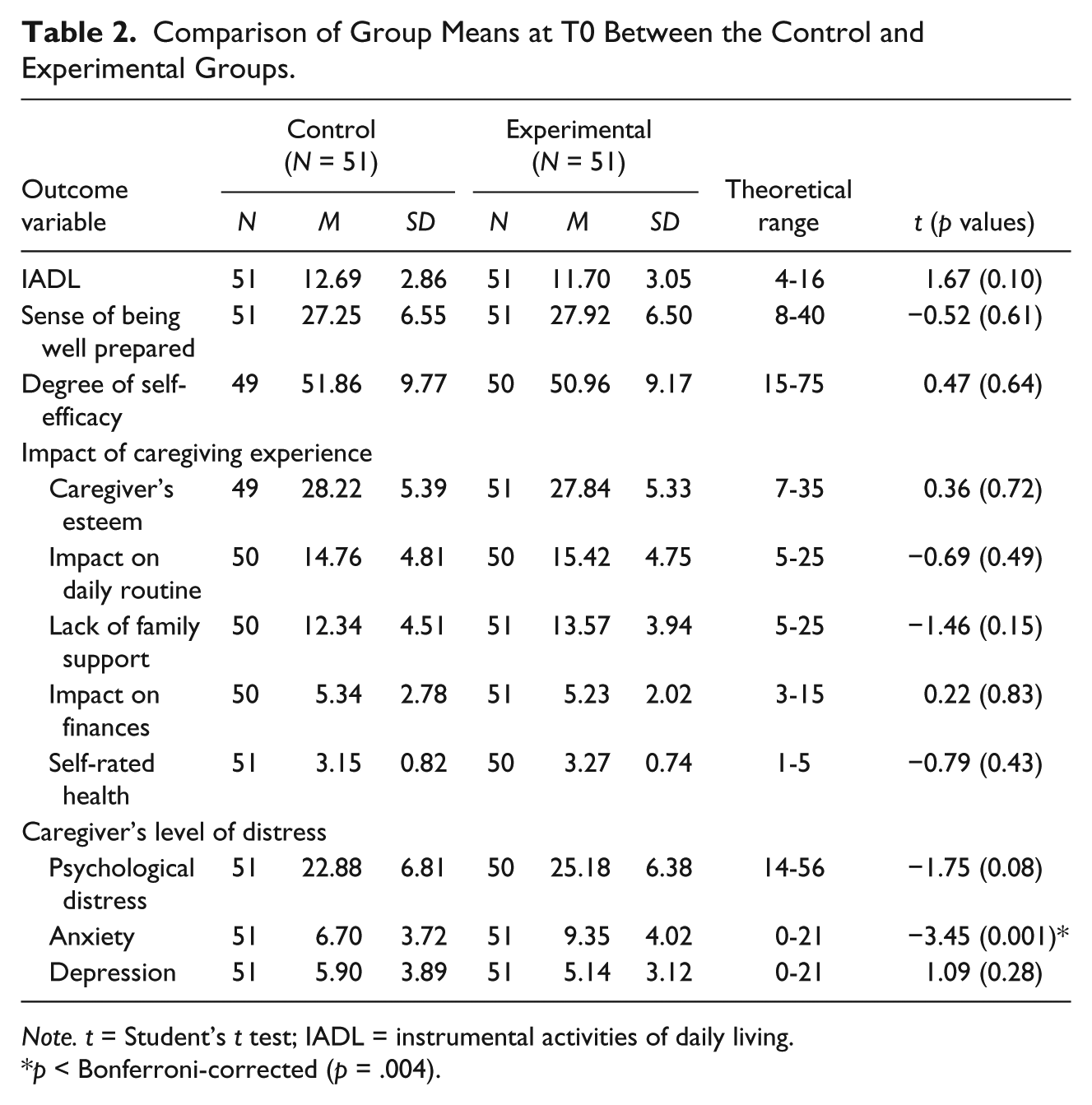
Note. t = Student’s t test; IADL = instrumental activities of daily living.
p < Bonferroni-corrected (p = .004).
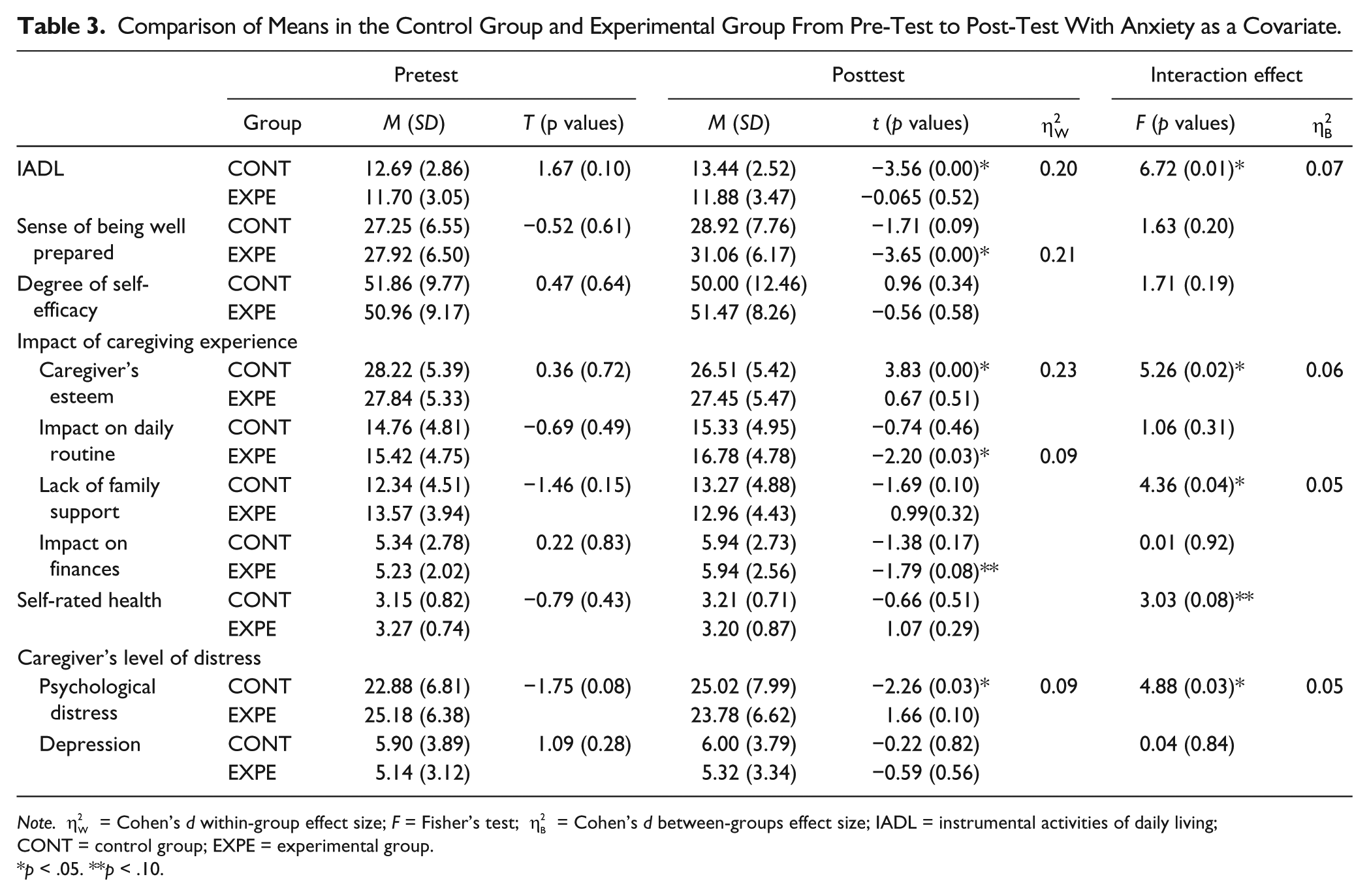
In Step 4, as there were seven therapists, we used ANOVA to verify that there were no differences at T1 based on the therapist’s effect. We then examined the differences between the experimental and control groups in all outcome measures using repeated-measures ANOVA with group (experimental vs. control) as the between-subjects factor and time (T0 vs. T1) as the within-subjects factor (see Table 3). For the significant multivariate analysis, we used paired-samples Student’s t tests to determine the direction of the observed differences. Effect sizes were also assessed with
Comparison of Means in the Control Group and Experimental Group From Pre-Test to Post-Test With Anxiety as a Covariate.
Note.
p < .05. **p < .10.
Measures
Spouse caregivers responded to a set of self-administered questions that addressed their sociodemographic status and services received (see Table 1).
Based on the model developed by Wawrziczny et al. (2017), several measures were then used to assess the determinants of spouse caregiver’s distress, including perception of the PWD’s daily functioning, sense of self-efficacy and preparedness, and effect of the disease on self-esteem, daily routine, finances, family support, marital adjustment, and self-rated health.
Caregivers’ perceptions of the PWD’s daily functioning
The PWD’s daily functioning was assessed by the caregiver using an instrument that examined instrumental activities of daily living (IADL). Caregivers rated PWDs’ performance of IADL using a four-item questionnaire (Lawton & Brody, 1969), in which each item was rated using a 4-point Likert-type scale from 1 (entirely able) to 4 (entirely unable). In the present study, the Cronbach’s alpha was .88 for the control group and .90 for the experimental group. The higher the score, the more important the restrictions in PWD’s daily functioning.
Caregiving self-efficacy and preparedness
The 15-item Self-Efficacy Scale (Kuhn & Fulton, 2004) assessed participants’ level of confidence regarding coping with caregiving demands on a 5-point response scale ranging from 1 (not at all confident) to 5 (extremely confident). In the study sample, Cronbach’s alpha was .90 for the control group and .91 for the experimental group. A higher score indicates that the caregiver feels confident.
The eight-item Preparedness for Caregiving Scale (Archbold, Stewart, Greenlick, & Harvath, 1990) was used to assess the degree of caregiver preparedness to provide care. Responses ranged from 1 (not at all prepared) to 5 (very well prepared). In the study sample, the reliability score was of .90 for the control group and .91 for the experimental group. A higher score indicates that the caregiver feels well prepared.
The effect of caregiving on caregiver experience
In the Caregiver Reaction Assessment (CRA; Given et al., 1992), five positive and negative dimensions of caregiver reactions were identified: disrupted daily routine, financial problems, lack of family support, health problems, and effect on self-esteem. This questionnaire contains 24 items and is scored on a 5-point response scale ranging from 1 (not at all confident) to 5 (extremely confident). In our sample, Cronbach’s alpha for disruption in daily routine was .79 for the control group and .82 for the experimental group. For financial problems, the corresponding values were .78 for the control group and .80 for the experimental group. For lack of family support, Cronbach’s alpha was .83 for the control group and .80 for the experimental group. The internal reliability for the effect on self-esteem was .90 for the control group and .92 for the experimental group. The Health Problems subscale had an alpha of <.60 and was therefore excluded from the analyses. A higher score indicates a negative impact on the caregiving situation, except for the “self-esteem” dimension.
Quality of couple adjustment
The Dyadic Adjustment Scale (DAS) is the most frequently used scale in the evaluation of marital adjustment (Spanier, 1976). In this study, the DAS-16 (Antoine, Christophe, & Nandrino, 2008) allowed two dimensions to be explored: the degree of agreement among the couple and the quality of their dyadic interactions. The items were rated on a 6-point scale. We decided to eliminate this scale from our analyses because in our sample, the majority of caregivers found the scale difficult to complete. Indeed, the PWD’s symptom intensity no longer allowed them to make common decisions, to agree on certain subjects or to interact.
Self-rated health
Health was assessed using two subjective questions based on the SF-36 (Ware & Sherbourne, 1992): “Would you say that your health is. . .” for general health (Ware & Sherbourne, 1992) and “When you compare yourself with other people your age, would you say your health is. . .” for health compared with people of the same age. The responses ranged from 1 (very bad) to 5 (very good). The internal reliability score of the scale in this study was .88 for the control group and .93 for the experimental group. A higher score indicates that the caregiver considers his or her health to be good.
Spousal caregiver distress
The 14-item Psychological Distress Index, an adapted version of the Psychiatric Symptom Index (Ilfeld, 1976), measures the level of psychological distress experienced. Respondents rated the items from 1 (never/almost never) to 4 (very often/always). The internal reliability (Cronbach’s alpha) was .90 for the control group and .93 for the experimental group. The higher the score, the more distressed the caregiver.
Self-assessed depression and anxiety were obtained using the Hospital Anxiety and Depression Scale (HADS; Zigmond & Snaith, 1983). This scale comprises 14 items rated on a 4-point scale from 0 to 3. In the sample, Cronbach’s alpha for the depression dimension was .83 for the control group and .85 for the experimental group. For the anxiety dimension, these values were .82 for the control group and .83 for the experimental group. The higher the score, the more anxious or depressed the caregiver.
Results
Comparison of the Final Sample and the Nonrespondents
Caregivers were mainly women. Comparisons between the participants in the final sample (experimental and control groups combined) and the nonrespondents showed a difference in the average MMSE scores between the two groups: 18.16 (SD = 6.99) for the nonrespondents versus 15.12 (SD = 9.17) for the final sample. Moreover, the range of MMSE scores in the two groups was the same, but the most common score was 0 for the final sample and 24 for nonrespondents, indicating that the PWD of the nonrespondents group had better cognitive function. No differences were observed between the groups in gender or delay between the first signs of dementia and the proposed interview.
Final Sample Description
Comparison of the experimental and control groups
Sociodemographic characteristics
Table 1 shows that the groups were comparable in terms of spouse caregivers’ gender, caregivers’ age, professional activity, PWD’s age, PWD’s MMSE score, number of years married, and most services received.
In addition, the delay between the earliest signs of the disease and the time of the interview significantly differed between the two groups: 7.83 years (SD = 4.55) for the control group compared with 5.95 years (SD = 4.16) for the experimental group.
Outcome variables at T0
Table 2 shows that the two groups did not differ with respect to the analyzed variables, including IADL, sense of preparedness, degree of self-efficacy, impact of caregiving experience, self-rated health, psychological distress, and depression.
Student’s t test showed a significant effect of anxiety (p = .001), specifically, a higher level of anxiety in the experimental group (9.35 for the experimental group vs. 6.70 for the control group).
Intervention Evaluation
Control of the effect of the therapist
No difference was observed for the 11 variables at T1 between the seven therapists (.06 ≤ p values ≤ .99), for instance, sense of being well prepared (F = 0.32, p = .92), caregiver’s esteem (F = 1.03, p = .41), lack of family support (F = 1.28, p = .29), and psychological distress (F = 0.49, p = .81).
Within-group effect
The analyses showed two significant within-group effects (see Table 3).
First, the sense of preparedness of caregivers in the experimental group significantly increased between T0 and T1 (Hypothesis 3; t = −3.65, p = .00). Second, caregivers in the experimental group perceived disruptions in daily organization between T0 and T1 (Hypothesis 6; t = −2.20, p = .03).
Between-group effect
The analyses showed four significant Group × Time effects (see Table 3).
First, there was a Group × Time effect for the IADL variable (Hypothesis 1: F = 6.72, p = .01). The perception of problems with the PWD’s IADL significantly increased from T0 to T1 in the control group (t = −3.56, p = .00); there was no significant change from T0 to T1 in the experimental group (t = −0.65, p = .52). Second, there was a Group × Time effect in caregivers’ esteem (Hypothesis 4: F = 5.26, p = .02). Caregivers’ esteem significantly decreased from T0 to T1 in the control group (t = 3.83; p = .00); there was no significant change from T0 to T1 in the experimental group (t = 0.67, p = .51). Third, there was a Group × Time effect for the lack of family support variable (Hypothesis 8: F = 4.36, p = .04). There was no significant change for perceived lack of family support from T0 to T1 in both the experimental and control groups. The analyses did not allow a determination of the direction of the observed effect. Fourth, there was a Group × Time effect for the psychological distress variable (Hypothesis 12: F = 4.88, p = .03). Psychological distress significantly increased from T0 to T1 in the control group and no significant change was observed from T0 to T1 in the experimental group.
No differences (interaction and linear effects) were observed for degree of self-efficacy (Hypothesis 2), self-rated health (Hypothesis 5), impact on finances (Hypothesis 7), or depression (Hypothesis 11).
Discussion
The study tested the effects of a flexible and customized intervention to address the varied needs of caregivers. The intervention combined three types of intervention strategies: classical psychoeducational, ACT, and couple interventions (Brodaty et al., 2003; Mittelman et al., 2004; Zarit & Femia, 2008). The goal of this intervention was to reduce caregivers’ distress by acting on its main determinants outlined in the spouse caregiver distress model proposed in Wawrziczny et al. (2017). On the basis of this model, we have selected our outcome variables. The focus was on spouse caregivers of PWDs.
The findings suggest two types of effects. First, two linear increases within the experimental group were observed: an increase in sense of preparedness and a disruption in daily routine. Second, interaction effects showed a “stabilization” effect of the intervention on the perception of PWD’s daily functioning, self-esteem related to the caregiving situation, quality of family support, and caregivers’ feeling of distress.
Observed Effects on the Determinants of Distress
We observed an effect of the intervention on variables concerning three of the five determinants of the spouse caregiver distress model: preparedness and confidence, care recipient’s impairments, and family divergence.
First, even if caregivers who benefited from the intervention had an increased perception of a disruption in the daily routine, they felt better prepared for their new role and they experienced more pleasure, gratification, and fulfillment in caring for the PWD. One of objectives of the intervention was to help caregivers find a balance between their values and their caregiving role. Indeed, caregivers’ lives become centered on their caregiving role to the point that they abandon important leisure activities and cut off social relationships (Wawrziczny et al., 2017b), becoming increasingly isolated (Kovaleva, Hepburn, & Spangler, 2016; Pertl et al., 2015). This inadequate fulfillment of their values and the resulting isolation become a source of distress, self-criticism, and guilt. By helping the caregiver regain this balance, the goal was to enhance fulfillment, satisfaction, and engagement in the relationship with the PWD.
Second, another effect concerned a change in caregivers’ perceptions of the PWD’s daily functioning. Indeed, the intervention aimed to put the disease into perspective by reinstating the identity of the PWD as a person rather than as a patient. Indeed, with the progression of the disease, caregivers become aware of changes in the identity and independence of PWDs and try to promote PWDs’ autonomy and sense of self (Wadham, Simpson, Rust, & Murray, 2016). Consequently, caregivers tend to increasingly focus on the disorders and impairments associated with the disease, and for beneficial and protective purposes, spouse caregivers gradually assume control; this process reduces the PWD’s autonomy and freedom, which can lead to conflict between the two partners (Wawrziczny, Antoine et al., 2016). By becoming aware of the PWD’s resources and by adopting a more positive perspective, spouse caregivers can focus away from the disease and involve their spouse in daily actions. This change may reduce tensions between partners. Accordingly, it would also be interesting to evaluate the intervention’s effects on the couple relationship quality using an alternative to the DAS scale that is more adapted to the evolution of the disease.
Third, the effect on perceived family support may be explained by a better identification of caregivers’ potential formal and informal support networks. Indeed, family conflicts have been suggested to occur more often in the case caregivers of persons with mild to moderate dementia (Peisah, Brodaty, & Quadrio, 2006). Caregivers often do not seek help from members of their informal network for fear of disturbing them or to prevent them from interfering with care decisions (Wawrziczny, Pasquier, Ducharme, Kergoat, & Antoine, 2017a); this lack of support increases the caregiving burden and contributes to a sense of isolation. By identifying the resources at their disposal, spouse caregivers are better able to identify the available support that could meet their existing needs, and ultimately make better use of their informal network. However, the effect of the intervention on this variable was not strong enough to determine its direction. A more substantial effect may be observed by organizing family meetings, which would allow participants to assess and define the parameters of potential family support. These meetings would also improve each family member’s understanding of the disease (Wawrziczny et al., 2017).
No Differential Changes
The intervention did not show any effect of the intervention on degree of self-efficacy, depression, impact on finances, or self-rated health.
Studies have shown that caregivers tend to live on a day-to-day basis and to not project into the future because of anxiety (Robinson, Clare, & Evans, 2005). Although the “future” module was highly used and enabled the caregiver to begin to consider the future and to address their fears related to the progression of the disease, it would be interesting to also increase engagement in the modules “management of difficult situations” and “how to ask for help?” to strengthen their degree of self-efficacy. However, the low use of these modules did not allow us to evaluate their effect and suggested that, at least in our sample, these modules were not associated with the prioritized difficulties identified in the first interview.
Finally, the intervention did not achieve any effect on the “self-rated health” or “impact on finances” variables. Indeed, no module directly targeted these dimensions. Reviews have shown no evidence that interventions have an effect on caregivers’ health (Huis In Het Veld et al., 2015). Nevertheless, we know that caregiver health is an important determinant of distress (Wawrziczny et al., 2017) and that caregivers neglect their health (Moore, Zhu, & Clipp, 2001). Moreover, previous studies have shown that financial aid is not easy to obtain and that home services are expensive. Therefore, it would be interesting to integrate this intervention into a multidisciplinary intervention by combining medical monitoring and interviews with a social professional to assess these issues.
The intervention showed an effect on the general feeling of distress but not on one of its components: depression. Given that distress is a multi-component dimension (Bandeira et al., 2007; Wawrziczny et al., 2017), of which anxiety and depression are the most prevalent among other different aspects according to the models, it may be interesting to evaluate other components of distress to see which aspect (component) of distress was affected by the intervention.
Strengths and Limitations of the Intervention
First, the main interest of our study resides in the originality of the proposed combination of already tested psychoeducational approaches with more innovative approaches such ACT or couple therapy. While a considerable proportion of the interventions are conducted in groups or alternate between individual and group sessions, the former appear to be more effective than the latter for some authors (Selwood, Johnston, Katona, Lyketsos, & Livingston, 2007; Sörensen et al., 2002). As a consequence, this intervention proposed individual sessions conducted at caregivers’ homes to fit in the best way possible the daily routine and organizational constraints of leaving the PWD alone and to minimize logistic inconvenience. Two disadvantages have been identified in this intervention format: the presence of the PWD, which might sometimes be uncomfortable for the caregiver, and the cost of sending therapists to the caregivers’ homes. Three ways to reduce these costs may be available: either a group-based intervention at the risk of losing the customizable aspect of the intervention but keeping the same principles of the intervention, either a multicomponent intervention combining group or family and individualized approaches would permit to reduce costs and address the issue of customization, or an Internet-based intervention that would cut costs and still provide a customized intervention. Indeed, recent evidence highlights the feasibility and efficacy of such a support program for caregivers (Boots, de Vugt, van Knippenberg, Kempen, & Verhey, 2014).
Second, intervention assessments have mainly focused on the negative outcomes of caregiving (Pendergrass et al., 2015). However, studies conducted over the last decade examined some beneficial effects of the caregiving situation (gratification, satisfaction; Boerner, Schulz, & Horowitz, 2004; Hilgeman, Allen, DeCoster, & Burgio, 2007; Roff et al., 2004), indicating that positive outcomes are an important variable to explore. The present study evaluated the effects of the customized intervention on caregivers’ esteem, degree of self-efficacy, and sense of being well prepared.
Finally, while the interventions may not be flexible enough to meet caregivers’ needs and their evolution during the caregiving trajectory (Nolan, Ryan, Enderby, & Reid, 2002; Zarit & Femia, 2008), the module format of this intervention allows adapting the content of the sessions as a function of the needs at each step of the caregiving trajectory.
Limitations of the Study
Several limitations of our study should be noted. Although it is important to note that the trial was not randomized, the results encourage us to set up a randomized controlled trial. Second, the results provide no information regarding the persistence of the observed positive effects. It would be interesting to conduct a follow-up at 6 and 12 months to confirm the effects of the intervention. Moreover, while the intervention addressed only spouse caregivers, its effects could also be evaluated for child caregivers. In addition, our results showed that spouse caregivers who agreed to participate in this study cared for a PWD with moderate but more pronounced dementia than the PWDs cared for by nonrespondents; this finding suggests that the participating caregivers may be more prone to seeking external help when the PWD’s disorders become severe enough to exceed their management capacity (Wawrziczny, Pasquier, Ducharme, Kergoat, & Antoine, 2016). However, Whitlatch et al. (2006) showed that reactive dyads were more disorganized and focused on fulfilling basic and immediate needs, a finding advocating for interventions with dyads in the early stages of dementia, as dyads with a proactive style appear to be better engaged, organized, and able to focus on future care needs. Finally, it would be interesting to evaluate the effects of this intervention on emotional avoidance strategies, but the French version of the Emotional Avoidance scale specific to the caregiving situation (EACQ) has not yet been validated (Losada, Márquez-González, Romero-Moreno, & López, 2014).
Conclusion
The objective of this study was to test the effects of a customized intervention for caregivers of PWDs using a quasi-experimental design. The results suggest that intervention is feasible and shows preliminary efficacy in preventing the exacerbation of caregivers’ sense of distress by acting on variables concerning three of the five determinants (Wawrziczny et al., 2017), that is, preparedness and confidence, care recipient’s impairments, and family divergence. Moreover, the intervention improved caregivers’ sense of preparedness. Although this program showed encouraging effects with an original approach, they should be viewed with caution and must be the focus of a future randomized controlled trial.
Supplemental Material
Supplemental_table – Supplemental material for A Customized Intervention for Dementia Caregivers: A Quasi-Experimental Design
Supplemental material, Supplemental_table for A Customized Intervention for Dementia Caregivers: A Quasi-Experimental Design by Emilie Wawrziczny, David Papo, Emilie Constant, Francine Ducharme, Marie-Jeanne Kergoat, Florence Pasquier and Pascal Antoine in Journal of Aging and Health
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by the Fond de Recherche du Québec-Santé (Québec), the Canadian Institutes of Health Research (Canada), and the Agence Nationale de Recherche (France) under Grant ANR-10-MALZ-0102-01. The study was supported by the Labex (laboratory of excellence) DISTALZ (Development of Innovative Strategies for a Transdisciplinary approach to ALZheimer’s disease), the MESHS (Maison Européenne des Sciences de l’Homme et de la Société, Lille, France), and the MEL (Métropole Européenne de Lille).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.