
Abstract
Introduction
Depressive symptoms increase with age, particularly in older adults. Depressive symptoms are associated with serious negative outcomes such as increased risk of depressive disorder (Beekman et al., 1997). People with cognitive impairment resulting from dementia frequently suffer from major depressive disorder (Lyketsos et al., 2002). Depressive symptoms in people with dementia reduce quality of life, worsen cognitive impairment, and increase caregiver stress (Gutzmann & Qazi, 2015). Dementia coupled with depressive symptoms leads to increased risk of adverse outcomes including early nursing home placement and all-cause mortality (Kiosses et al., 2015). Treating depressive symptoms is, thus, a clinical priority for improving the quality of life of people with dementia and their caregivers.
Limited data are available on depressive symptoms but more are available for depression, where depressive symptoms are severe enough to affect functional abilities. Studies have suggested several possible biological mechanisms linking depression and dementia including vascular disease, inflammatory processes, deficit of neurotropic factors, and hippocampus damage by alterations in glucocorticoid steroid levels (Sierksma, van den Hove, Steinbusch, & Prickaerts, 2010). The vascular depression hypothesis (Alexopoulos et al., 1997) suggests that in patients with late life depression, brain vascular disease may further instigate depressive symptoms. This leads to reduced efficacy of antidepressant therapy and worsening of cognitive impairment.
A literature review indicated that antidepressant use for managing depressive symptoms in dementia due to Alzheimer’s disease has proven to be ineffective (Banerjee et al., 2011). Several studies have assessed the effectiveness of nonpharmacological approaches such as music therapy, horticulture therapy, aroma therapy, problem-adaptation therapy, and problem-solving therapy in home care (Arean et al., 1993; Mansens, Deeg, & Comijs, 2017). The nonpharmacological approaches have shown more promising results for management of depressive symptoms and improving cognitive function in older adults with dementia.
One such nonpharmacological approach, social engagement, has been identified as a critical factor affecting cognitive function. Several previous studies have examined the relation between social ties (Crooks, Lubben, Petitti, Little, & Chiu, 2008) and social isolation (Shankar, Hamer, McMunn, & Steptoe, 2013) with cognitive function in dementia. Social engagement is associated with better cognitive function in older adults (Krueger et al., 2009). Few data are available on the association between social engagement and depressive symptoms in older adults with dementia. We are aware of one national study to determine associations between use of three different modes of social contact (in person, telephone, written, or email) and risk of depressive symptoms. The study found increased probability of having clinically significant depressive symptoms in participants with low frequency of in-person contact (Teo et al., 2015).
To our knowledge, no study has examined the utility of combining pharmacologic and nonpharmacologic approaches to reduce depressive symptoms in persons with dementia. We hypothesized that low antidepressant medication use and higher social engagement are associated with fewer depressive symptoms in older adults with dementia. To understand the feasibility of designing such a study, we conducted a cross-sectional analysis of the effect of antidepressant medication use and social engagement on the level of depressive symptoms at the time of meeting criteria for dementia. The data were collected from community-dwelling older adults at the first interview where criteria for dementia were met.
A study to estimate the effect of antidepressant medication use and social engagement on the level of depressive symptoms in this population is complicated due to the possibility of depressive symptoms and dementia causing lower social engagement. Also, the analysis to determine effect of social engagement on depressive symptoms requires understanding of the quality of the social engagement. If frequent contact involves conflict, the risk of depressive symptoms is increased. In this analysis, we used two measures of social engagement, social network size and perceived social isolation to understand the effect of a large network size and the feeling of isolation separately and together with regard to depressive symptoms at the time of dementia diagnosis.
Theoretical Background
The stress buffering hypothesis states that in times of high perceived stress, increased social support is protective against physical or psychological disorders, including depression (Cohen & Wills, 1985). For the current study, we used a biopsychosocial model (Di Benedetto, Len Burns, Lindner, & Kent, 2010). The model suggests that older age, smoker status, higher stress, and lower coping resources are associated with higher levels of depression. The model found that low coping resources or the perception of lower coping resources may create an increased risk of development and maintenance of depression. For the issue of depressive symptoms at the time of dementia diagnosis, the limited prior work has focused on pharmacologic and nonpharmacologic approaches. Pharmacologic approaches that focused on antidepressant medications have shown mixed findings (Di Benedetto et al., 2010; Nelson & Devanand, 2011). Nonpharmacologic approaches point to socialization as a potential factor associated with depressive symptoms. Figure 1 shows our hypothesized model.
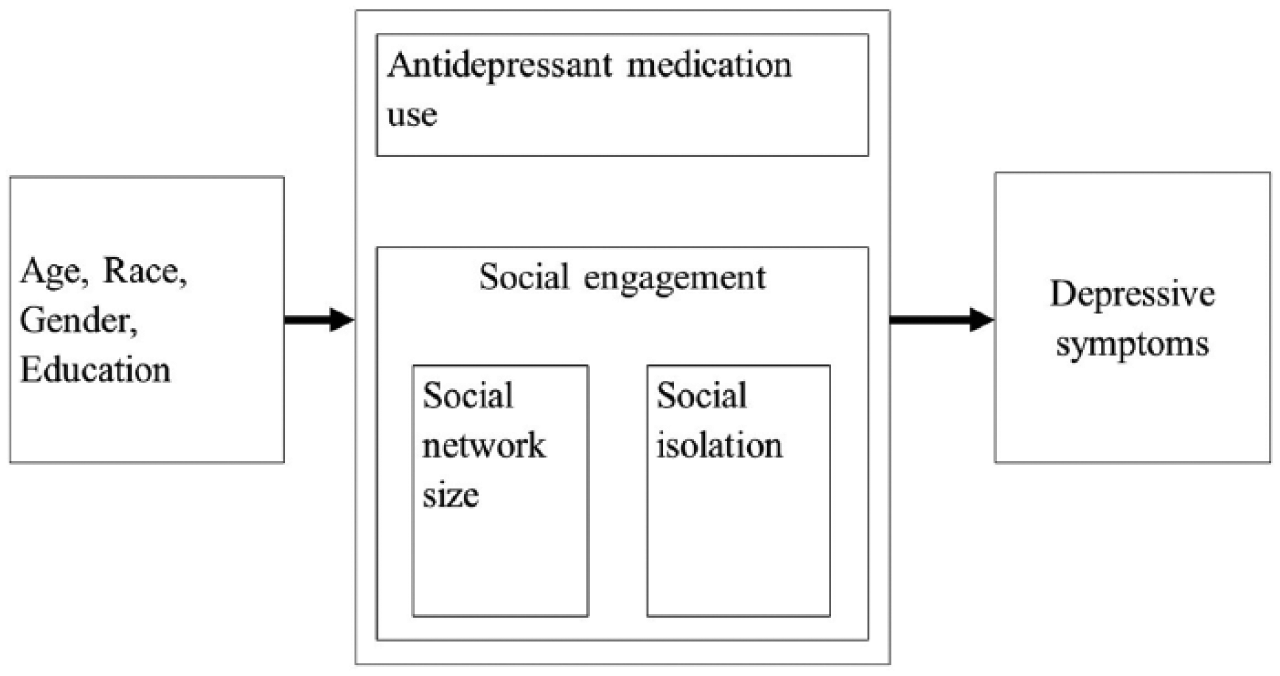
Model for effect of antidepressant use and social engagement on depressive symptoms in dementia.
Method
Study Design
The study is a cross-sectional analysis of the effect of antidepressant medication use and social engagement (social network size and perceived social isolation) on the level of depressive symptoms at the first interview where criteria for dementia were met.
Data
The study was conducted based on data collected from a combined cohort of participants enrolled in one of two longitudinal studies of aging funded by the National Institute on Aging, the Rush Memory and Aging Project (MAP; Bennett et al., 2012) and the Minority Aging Research Study (MARS; Barnes, Shah, Aggarwal, Bennett, & Schneider, 2012).
The MAP is an observational study that started in January 1997. The study includes older community-dwelling adults from more than 40 retirement communities and senior subsidized housing facilities across the Chicago metropolitan area with no known dementia at baseline. The participants undergo detailed annual clinical assessments of risk factors along with blood work. The annual clinical evaluations are performed as home visits ensuring high follow-up rates and low participant burden. The participants of continuous care retirement communities are predominantly White and are found to be more affluent. Thus, the study also includes people from housing subsidized by the Department of Housing and Urban Development and from retirement homes. Furthermore, minorities and low-income elderly are recruited through local churches and other social service agencies.
The MARS is a longitudinal, cohort study of older African Americans without known dementia. The study started in August 2004 and has allowed for better understanding of the factors contributing to any observed racial differences in the neurobiology of cognitive impairment. The participants in MARS include African Americans without known dementia at baseline undergoing annual detailed clinical evaluations such as participants in the MAP cohort.
Sample
As of 2015, data from the Memory and Aging Project, consisted of 1,780 persons and was combined with the 680 African Americans participating in the MARS. Given identical recruitment techniques and a common core of data collection across both studies, data were merged to address the research question in one analytic cohort. All participants were free of dementia at baseline. African Americans in the two studies did not differ on key demographic features. Thus, all African Americans enrolled in the MARS and the Memory and Aging Project were grouped together, and then matched 1:2 with White participants in the MAP based on age, education, gender, and length of longitudinal follow-up.
As shown in Figure 2, of the 2,460 participants included in the combined analytic sample, 484 participants had a diagnosis of dementia. An additional 82 participants were excluded for one or more of the following reasons: missing Mini-Mental State Examination (MMSE) score, missing depressive symptoms score, missing antidepressant medication use data, and/or missing social network size at the first visit where criteria for dementia were met. For social isolation models, 46 participants were excluded for missing social isolation score. Based on the above exclusions, 402 people were eligible for the analysis involving antidepressant medication use and social network size. Because of the number missing a social isolation score, 356 people were eligible for that analysis.

Composition of the study groups.
Clinical Evaluation for Dementia
Clinical diagnosis of dementia was assessed at each annual follow-up evaluation by an experienced clinician. Classification of dementia was based on the criteria of the joint working group of the National Institute of Neurological and Communicative Disorders and Stroke and the Alzheimer’s Disease and Related Disorders Association. The diagnosis requires a history of cognitive decline and impairment in at least two cognitive domains (McKhann et al., 1984).
Participants with a diagnosis of dementia and complete information on their current medications, self-reported level of depressive symptoms, social network size, and perceived social isolation were eligible for this cross-sectional analysis.
Variables
Antidepressant medication use
Prescription and over-the-counter medications were inspected and recorded at each annual evaluation. The number of medications prescribed for depression at the time of diagnosis of dementia was included in the current analysis.
Social network size
Social networks were estimated with standard questions about the number of children, family members, and friends each participant had and how often they would see them (Cornoni-Huntley et al., 1993). They were asked about the number of relatives (besides spouse and children) and other friends to whom they felt close and at ease, could talk to about private matters, and could call upon for help, and how many of these people they saw monthly. Social network size was the number of these individuals seen at least once per month (Bennett et al., 2005).
Social isolation
Loneliness was assessed at each annual evaluation with a modified version of the De Jong Gierveld Loneliness Scale (de Jong Gierveld & van Tilburg, 2008). The modified version measures emotional loneliness. Sensitivity was enhanced by asking the participants to rate agreement with the items on a 5-point scale ranging from strongly agree to strongly disagree. The items included questions assessing social isolation such as I experience a general sense of emptiness, I miss having people around, I feel like I do not have enough friends, I often feel abandoned, and I miss having a really close friend. Higher scores indicate a higher level of social isolation.
Level of depressive symptoms
Level of depressive symptoms was the outcome of interest in this study. Depressive symptoms were assessed at each annual evaluation with the 10-item version of the Center for Epidemiologic Studies Depression Scale (Kohout, Berkman, Evans, & Cornoni-Huntley, 1993). This short version of the test has been shown to be psychometrically similar to the original version of the scale (Radloff, 1977) including the ability to capture change in symptoms over time (Amieva et al., 2008; Wilson et al., 2010), but differs in two important respects: It does not include cognitive symptoms (i.e., I had trouble keeping my mind on what I was doing, I talked less than usual) and reduces participant burden (i.e., fewer items, yes/no response format). The test included subscores of negative affect (three items: I felt depressed, I felt lonely, I felt sad), positive affect (two items: I was happy, I enjoyed life), somatic symptoms (three items: I felt like everything I did was an effort, my sleep was restless, I could not get going), and interpersonal problems (two items: people were unfriendly, I felt that people disliked me). The participants were read each of the 10 symptoms and asked to indicate whether or not he or she had felt that way much of the past week. The score was the total number of symptoms experienced. This 10-item version predicts morbidity and mortality (Wilson et al., 2002; Wilson, Bienias, Mendes de Leon, Evans, & Bennett, 2003; Wilson, Mendes De Leon, Bennett, Bienias, & Evans, 2004).
The MMSE (Folstein, Folstein, & McHugh, 1975), a brief screen used to measure cognitive impairment, was included as a measure of baseline cognitive function.
Other variables
Age was calculated from the date of birth, gender was self-reported as male or female, and race was assessed by asking each participant to self-report their racial category based on questions used by the U.S. Census Bureau. Years of education was also determined by self-report.
Statistical Analysis
We first examined the descriptive statistics of the cohort (Table 1). The level of depressive symptoms was skewed at each evaluation. All subsequent analyses were adjusted for age centered at 86 years, gender, education centered at 14 years, and race.
Cohort Characteristics of 402 Participants at Time of Dementia Diagnosis.
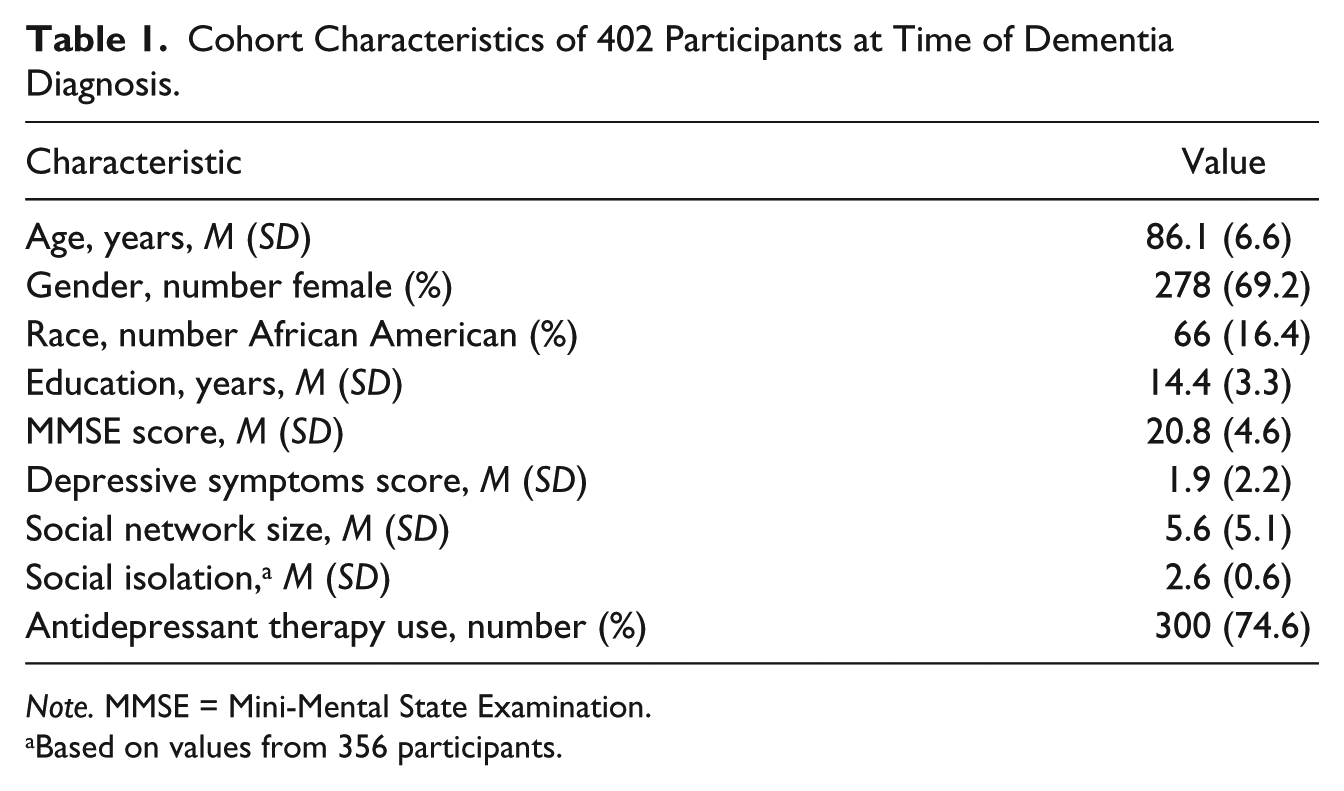
Note. MMSE = Mini-Mental State Examination.
Based on values from 356 participants.
The outcome, level of depressive symptoms, was treated as an ordinal variable with six levels (number of symptoms = 0, 1, 2, 3, 4, and >5, modeled as odds of more symptoms). The proportionality assumption, assessed with the score test for proportional odds model (Capuano & Dawson, 2013), was found to be adequately met.
First, we constructed a proportional odds model adjusted for age, education, gender, and race with the level of depressive symptoms (modeled as odds of more symptoms) as the outcome and the presence of antidepressant medication use as an independent variable. Subsequent models adjusted for demographic variables were constructed to examine the association of level of depressive symptoms with the independent variables, social network size, and social isolation score, separately and in the same model. Additional models also included an interaction term between the social engagement measures and antidepressant medication use. A final model included interaction terms between race and the independent variables.
For the next set of models, four levels of pharmacologic and nonpharmacologic therapies were created to illustrate interaction effects. We used values of our two measures of social engagement, first network size and then social isolation, to create groups of high and low levels of social engagement. Prior work from a community-based study of older African American and White participants found an average network size of seven people (Barnes, Mendes de Leon, Wilson, Bienias, & Evans, 2004) and this cut point was used for defining large and small social network sizes. Based on the social network size and antidepressant medication use, the participants were classified into four groups: (a) large social network (greater than or equal to 7) and no antidepressant medication use, (b) large social network and antidepressant medication use, (c) small social network (less than 7) and no antidepressant medication use, and (d) small social network and antidepressant medication use. A proportional odds model was used to evaluate the odds of each group having more depressive symptoms, with “large social network and no antidepressant medication use” as the reference group.
For our second measure of social engagement, social isolation, the mean social isolation score of the cohort was 2.6, so a score lower than this value was used to define the low social isolation group. Participants were classified based on their social isolation score and antidepressant medication use into four groups: (a) low social isolation score (less than 2.6) and no antidepressant medication use, (b) low social isolation score and antidepressant medication use, (c) high social isolation score (greater than or equal to 2.6) and no antidepressant medication use, and (d) high social isolation score and antidepressant medication use. Proportional odds model was used to ascertain the odds of each group having more depressive symptoms, with “low social isolation score and no antidepressant medication use” as the reference group.
Results
Descriptive Statistics
The descriptive statistics at the time of diagnosis of dementia are shown in Table 1. Participants had a mean age of 86 years (SD = 7 years), a mean education of 14 years (SD = 3 years), and a mean depressive symptoms score of 2 (SD = 2). Of the participants, 69.2% were female, 16.4% were African American, and 25.4% were using antidepressant medication. The mean social network size was 6 (SD = 5) and the mean perceived social isolation score was 2.6 (SD = 0.6).
Antidepressant Medication Use and Level of Depressive Symptoms
In the proportional odds model (Table 2) adjusted for age, gender, education, and race, antidepressant medication use was not associated with the level of depressive symptoms at the time of dementia diagnosis (odds ratio [OR] = 1.18, p = .4).
Proportional Odds Models for Antidepressant Therapy Use, Social Network Size, Social Isolation, and Race With Level of Depressive Symptoms.
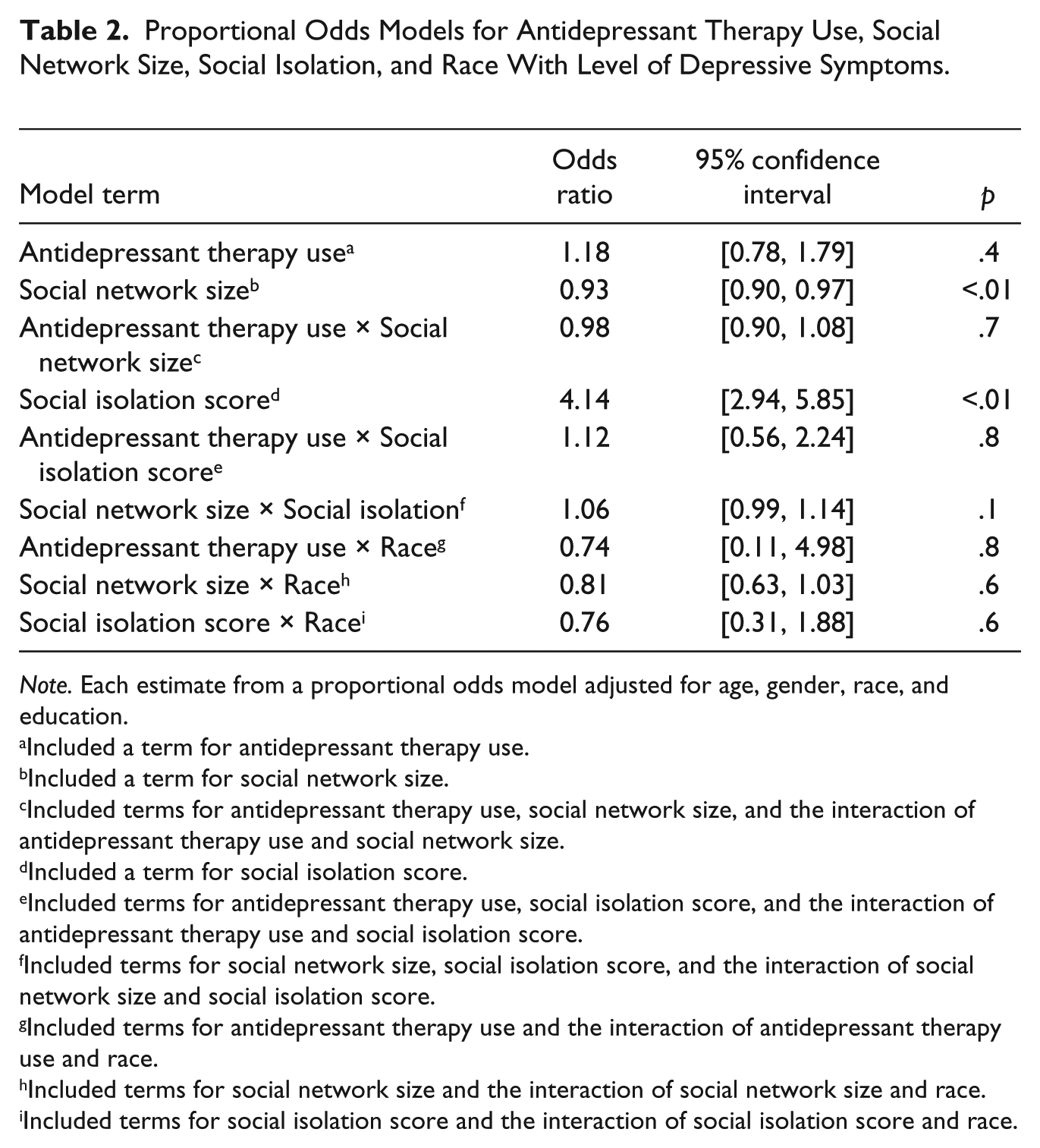
Note. Each estimate from a proportional odds model adjusted for age, gender, race, and education.
Included a term for antidepressant therapy use.
Included a term for social network size.
Included terms for antidepressant therapy use, social network size, and the interaction of antidepressant therapy use and social network size.
Included a term for social isolation score.
Included terms for antidepressant therapy use, social isolation score, and the interaction of antidepressant therapy use and social isolation score.
Included terms for social network size, social isolation score, and the interaction of social network size and social isolation score.
Included terms for antidepressant therapy use and the interaction of antidepressant therapy use and race.
Included terms for social network size and the interaction of social network size and race.
Included terms for social isolation score and the interaction of social isolation score and race.
Social Engagement and Level of Depressive Symptoms
In the fully adjusted proportional odds models with level of depressive symptoms as the outcome (Table 2), the odds of any depressive symptoms as compared with no depressive symptoms were 7% lower for each unit increase in social network size. Subsequent models added antidepressant medication use and an interaction term for social network size and antidepressant medication use. Neither association was significant. Also, in the fully adjusted model in Table 2, the odds of any depressive symptoms as compared with no depressive symptoms were 76% lower for each unit decrease in the social isolation score. The interaction term between perceived social isolation and antidepressant medication use was not significant for predicting the level of depressive symptoms. An interaction between social network size and social isolation also did not reach significance suggesting the two parameters are independently associated with depressive symptoms. Race was not associated with depressive symptoms score at the time of dementia diagnosis, OR = 1.05, 95% confidence interval (CI) = [0.63, 1.76], p = .8. None of the interaction terms with race and antidepressant medication use, social network size, or perceived social isolation was significant (see Table 2).
Antidepressant Medication Use, Social Network Size Groups, and Depressive Symptoms
The proportion of participants with a nonzero depressive symptoms score in the four groups is shown in Figure 3. One quarter of the participants were using antidepressant medication; 19% had a small network size and 6% had a large network size. Of the participants not using antidepressant medication, 56% had a small network size and 19% had a large network size. We hypothesized that the group with large social networks and no antidepressant medication use would show lower depressive symptoms at the time of initially meeting criteria for dementia and used this group as the reference. A proportional odds model with depressive symptom score as the outcome (Table 3) showed a difference in depressive symptoms score for the small social network group with antidepressant use (OR = 2.1, p = .01) and for the small social network group without antidepressant use (OR = 1.9, p = .01) as compared with the reference group.
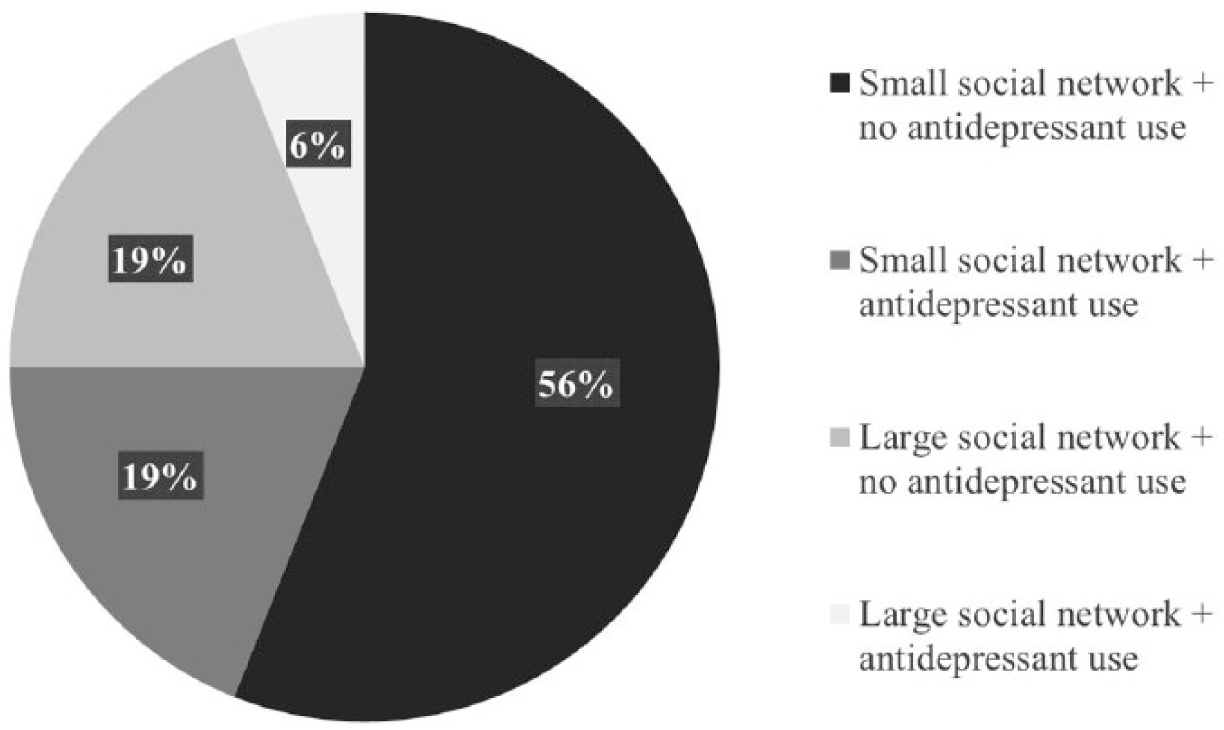
Frequency distribution of antidepressant therapy use in social network size groups.
Association a of ADT Use and (a) Social Network Size Groups or (b) Social Isolation With Total Depressive Symptom Score at Time of Dementia Onset.
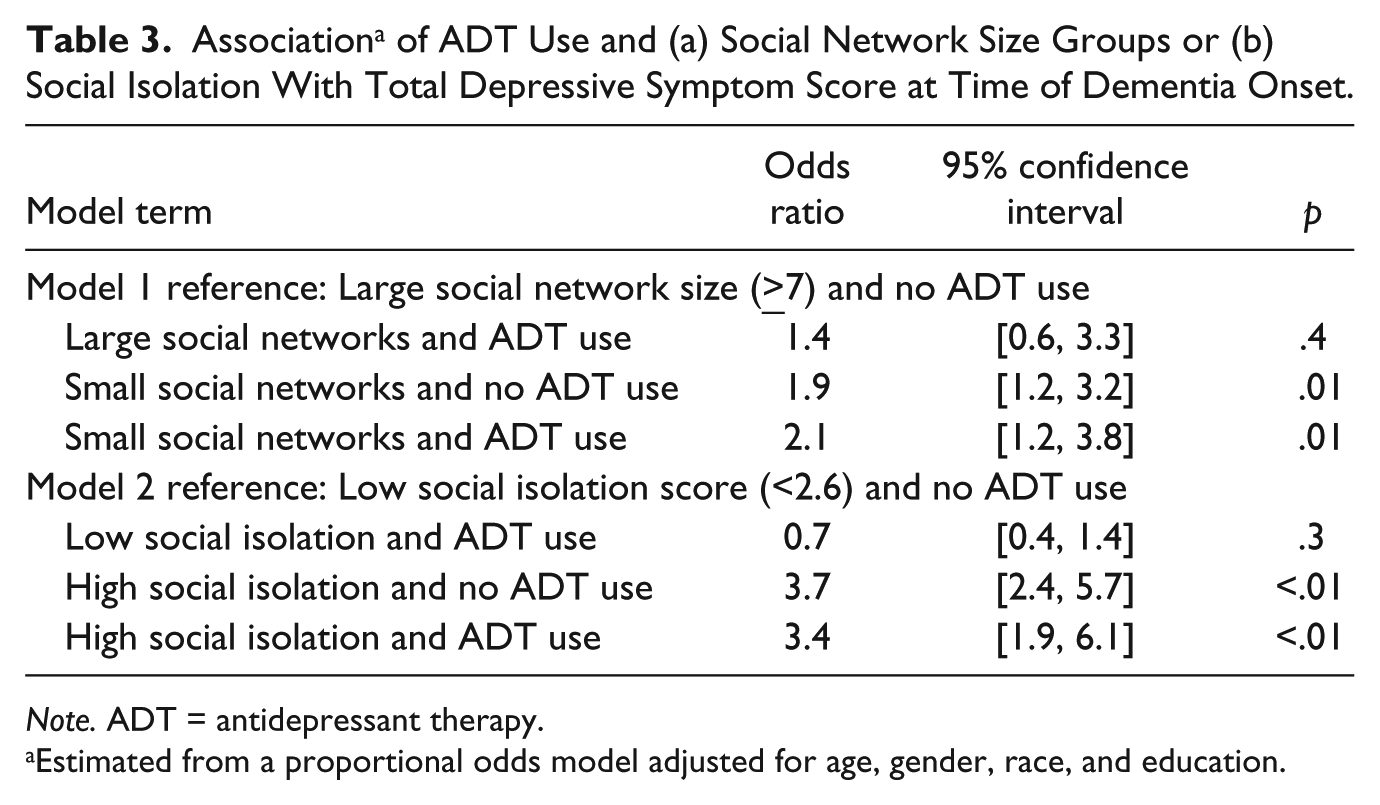
Note. ADT = antidepressant therapy.
Estimated from a proportional odds model adjusted for age, gender, race, and education.
Antidepressant Medication Use, Social Isolation Score Groups, and Depressive Symptoms
The proportion of participants with a nonzero depressive symptoms score in the four groups is shown in Figure 4. Of the participants using antidepressant medication, 14% reported high social isolation. Of the participants not using antidepressant medication, 30% reported high social isolation. A proportional odds model with depressive symptoms score as the outcome and the group with low social isolation and no antidepressant medication use as the reference (Table 3) showed a difference in depressive symptoms score for the high social isolation group without antidepressant use (OR = 3.7, p ≤ .01) and the high social isolation group with antidepressant use (OR = 3.4, p ≤ .01) as compared with the reference group.

Frequency distribution of antidepressant therapy use in social isolation score groups.
Discussion
In this study, we compared the utility of antidepressant medication use with social engagement for depressive symptoms management in dementia. In a cohort of more than 400 community-dwelling, older persons with dementia, we found an association between social engagement and severity of depressive symptoms but no association between depressive symptoms and antidepressant medication use. Larger social network size and lower perceived social isolation were associated with lower levels of depressive symptoms but antidepressant medication use was not associated with lower depressive symptoms.
Our findings on the effects of social engagement on depressive symptoms are consistent with results from previous studies (Glass, De Leon, Bassuk, & Berkman, 2006). A study of older adults in aged care facilities reported engagement in game playing in a group helped decrease loneliness in older adults by allowing for social interaction. The study proposed incorporation of activities of shared interests in care-based settings to benefit mental health. Another study of loneliness in geriatric nursing homes suggests that increased social isolation, inadequate social engagement, and decreased life satisfaction worsens loneliness (de Guzman et al., 2012). A study on the effect of volunteering on depression suggested volunteering was beneficial for mental health (Musick & Wilson, 2003). This is attributed to the social integration it encourages and improved access to social support and information. Another pilot study randomized participants with Alzheimer’s disease to an intergenerational choir to decrease social isolation (Harris & Caporella, 2014). The study reported a decrease in social isolation among older choir members. However, few data are available on the effect of antidepressant medication use compared with social engagement in depressive symptoms management in people diagnosed with dementia due to Alzheimer’s disease.
Our results fill this gap. Based on our results, social engagement may have a positive influence in management of depressive symptoms in patients diagnosed with dementia and use of antidepressant therapy may not be as impactful.
This study has several strengths. The study included a large sample size of participants. Data were derived from a combined cohort of two large epidemiologic studies with identical operational methods, allowing for examination of racial differences. We used two validated indicators of social engagement (social network size and social isolation) that incorporate the multidimensional nature of this construct. The study has important limitations as well. Analyses were based on a selected group of community-dwelling older adults with dementia. It will, therefore, be important to determine whether the results generalize to other populations of older people. Also, the group had a high level of education and, thus, the results may not apply to a population with a lower level of education. The population was not very depressed, and, thus, the distribution of depressive symptoms was highly skewed, with a high inflation of zero symptoms. With a limited number of symptoms on the scale, it also has floor and ceiling effects. For these reasons, depressive symptoms were treated as an ordinal variable. Furthermore, the data are cross sectional. Longitudinal studies will be needed to elucidate the direction of the association between social engagement and depressive symptoms. Data used were from the interview where participants first received dementia diagnosis. Thus, self-reported social engagement and depressive symptoms may need corroboration by other sources. Also, selection of the small and large social network size groups was based on estimates from the literature and not empirically based estimates from the sample.
Future Directions
The results indicate that management of depressive symptoms at the time of dementia diagnosis may benefit from an increased focus on social engagement (increasing social network size and/or reducing social isolation). A program to treat depressive symptoms in dementia may have a significant impact in improving the quality of life of people with dementia and their caregivers. It is critical to focus on management of depressive symptoms when decline in cognitive domains are first observed. The results suggest that further exploration of the link between increasing social network size and/or reducing social isolation and depressive symptoms is warranted.
The study findings suggest social engagement is associated with lower depressive symptoms. The study provides strategies for depressive symptoms management by increasing social engagement with/without antidepressant medication use. One potential intervention would be to spend time with older adults and share experiences. A study of social engagement in older adults found that family support alone did not benefit psychological and physical health (Golden, Conroy, & Lawlor, 2009). Elective relationships were found to promote health and reduce depressive symptoms in later life. Thus, programs to facilitate and promote social engagement with different types of people and encouragement to participate in activities of interest may be helpful for depression prevention and management. Furthermore, selection of social activity should include consideration of interest, having familiarity of the activity, experiencing belonging, and involving a sense of accomplishment and personal meaning. One study suggests involvement in multiple social activities should be considered to prevent depressive symptoms or treat depression (Hong, Hasche, & Bowland, 2009). It will be beneficial for care providers to ensure participation in meaningful activities to promote well-being. It is also important to ensure the new and ongoing social participation is maintained. Continuous participation is associated with fewer depressive symptoms (Chiao, Weng, & Botticello, 2011). Longitudinal studies randomizing participants to interventions aimed at increasing social engagement will contribute to a better understanding of the association between social engagement and depressive symptoms.
Footnotes
Authors’ Note
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Support for this work was provided by the Minority Aging Research Study (RF1AG022018, Barnes LL), the Rush Memory and Aging Project (RF1AG015819, Bennett DA), the Rush Alzheimer’s Disease Core Center (P30AG010161, Bennett DA), the Center of Excellence on Disparities in HIV and Aging (P20MD006886, Barnes LL), and the Illinois Department of Public Health.