
Abstract
Introduction
With the projected increase in the aging population worldwide in the coming decades (National Institutes of Health, 2016), identifying determinants of cognitive patterns in later life has been of increasing interest in recent years. Much of the current literature, however, has focused on individual-level predictors of cognition, such as biological and demographic characteristics, and has ignored broader structural, or country-level, factors that may influence cognitive patterns. Nonetheless, there is reason to believe that country-level factors could also play a role in determining cognitive outcomes. According to stereotype embodiment theory, if a country treats its oldest citizens in a more empowered way, it is likely to generate positive age stereotypes which can lead to better self-perceptions of aging, stress management, and cognitive health (Levy, 2009). Research indicates that the content of age stereotypes can vary by country (Chiu, Chan, Snape, & Redman, 2001; Levy & Langer, 1994; Löckenhoff et al., 2015).
Previous experimental studies have demonstrated that positive and negative age stereotypes can help or hurt, respectively, the cognitive performance of older individuals (e.g., Lamont, Swift, & Abrams, 2015; Levy, 1996). Furthermore, previous longitudinal studies have demonstrated that negative age stereotypes predict worse cognition over time (Levy, Zonderman, Slade, & Ferrucci, 2012; Robertson, King-Kallimanis, & Kenny, 2016); these studies used predictors and outcomes at the individual level. In contrast, the current study examined age status as indicated by the predominant beliefs about aging that are held by a representative sample of younger and older individuals, on the country level.
In the present study, we hypothesized that in countries in which the general population has a more positive view of older adults (i.e., higher age status), the older residents will experience better cognitive performance over time than those living in lower age status countries, after adjusting for relevant covariates.
Method
Data Source and Population
Eight countries (Belgium, Denmark, France, Germany, the Netherlands, Spain, Sweden, and Switzerland) were examined using a novel combination of country-level and individual-level data. Country-level age status data were drawn from the 2008 European Social Survey (ESS; Age UK, 2011), which was a comprehensive random-probability sample multi-national survey of people over the age of 15, with 1,000 to 2,000 total respondents per country. Individual-level data were drawn from four waves of the Survey on Health, Ageing, and Retirement in Europe (SHARE) between 2004 and 2013 (Borsch-Supan et. al., 2015). SHARE assessed the demographics, health, and cognition of adults aged 50 years and older living in more than 20 European countries. All waves shared the same basic format and questionnaire content. A central coordination team and individual country teams oversaw the collection of data via interview, physical examination, and written questionnaire. All surveys were conducted in the national language of the respective countries.
To align the two datasets, we selected all of the countries that participated in both the ESS and at least three (but as many as four) waves of data collection for SHARE. We further restricted the SHARE sample to individuals above age 70 who had baseline demographic and health data, as well as cognitive variables in at least three waves of SHARE follow-up data. This age group was used because the age status predictor variable specifically referred to older adults above the age of 70. The final cohort consisted of 2,620 individuals. Table 1 lists baseline demographic information for the sample, stratified by country. As seen in Table 1, age, education level, and self-perceived health were all significantly different across the eight countries of analysis. Thus, these variables were included as covariates in the final model.
Baseline Characteristics of the Study Sample.
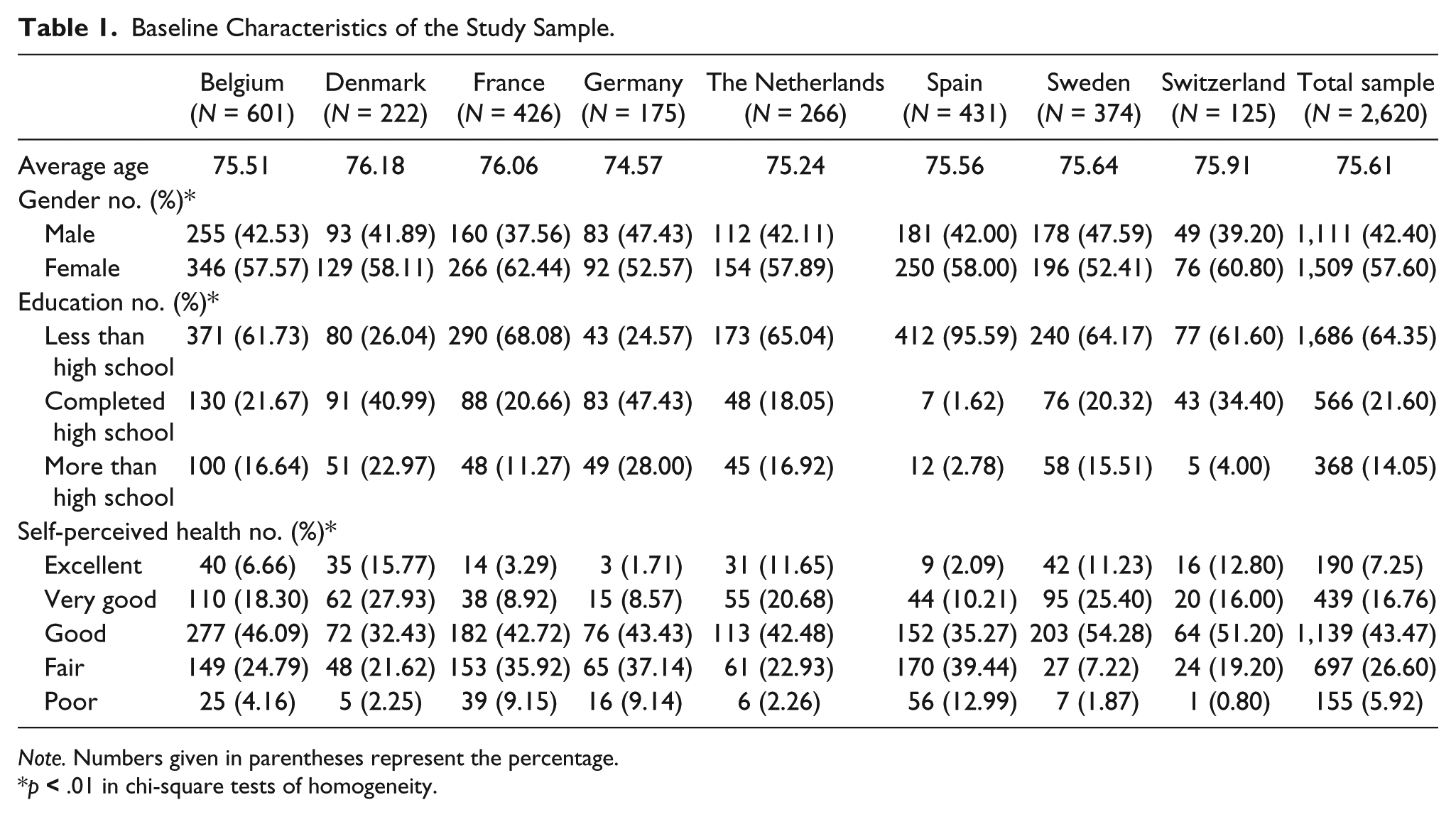
Note. Numbers given in parentheses represent the percentage.
p
Measures
Predictor: Age status
The predictor of age status was measured by asking a representative sample of adults in each of the eight ESS countries the following question: “Please tell me where most people would place the status of people over 70?” Responses were on a scale of 0 to 10, with 0 indicating very low status and 10 indicating very high status (Age UK, 2011). The range of age status scores among the eight countries ranged from 4.6 to 5.9. Each individual was assigned an age status that was equal to the average score for their respective country of residence in SHARE.
Outcome: Cognition over time
The outcome of cognition over time was based on the interviewer-assessed measures of immediate recall, delayed recall, and verbal fluency in SHARE (Borsch-Supan et al., 2015). Memory function was assessed by asking participants to listen as the questionnaire administrator read a list of 10 words and then to recall as many as possible when asked 1-min later (immediate recall) and a few minutes later (delayed recall). In the verbal-fluency task, participants were asked to name as many animals as they could think of in 1 min. In our dataset, participants named 0 to 50 animals. The scoring of these three measures followed the protocol used in a previous study of cognitive function examining the SHARE dataset (Bourassa, Memel, Woolverton, & Sbarra, 2017). For each of the three cognitive measures, the dependent variable of interest was individuals’ slope based on up to four waves of cognitive data. That is, a slope was calculated for each cognitive measure, for each individual.
Covariates
Covariates were selected that have been widely included in previous studies assessing cognitive outcomes in older adult populations (Bourassa et al., 2017; Marioni et al., 2015). Age, sex, education, and self-perceived health, measured at baseline in SHARE, were used as covariates in the final multivariate model. Sex was categorized as male or female, based on self-response. Education was measured using the International Standard Classification of Education (ISCED) ranking (UNESCO, 2012). The ISCED is a standardized system for scoring education level that was developed by the UNESCO Institute for Statistics (2012); on a scale of 0 to 7, a higher number indicates more years of education, which we categorized as less than high school (0-2), completed high school (3), or more than high school (4-7). Self-perceived health was measured on a 5-point Likert-type scale with responses ranging from excellent to poor. In addition, we examined baseline depression status using the EURO-D instrument, which is a depression scale specifically designed and validated for use in older individuals (Prince et al., 1999).
Statistical analyses
We used multilevel multivariate generalized-linear modeling to examine the association between country-level age status and individual-level changes in cognitive status over time. The multivariate model simultaneously modeled the three cognitive measures because we anticipated that age status would impact all three in a similar fashion. A nested variable of age status was included to account for clustering of participants by country (and thus, having the same country age status score). A visual inspection of the relationship between age status and change in cognition revealed it was nonlinear. To allow for curvature in the age status effect, we incorporated age status as a squared term, as well as a linear age status term (Aarts et al., 2014; Carey, 2013). In addition, we controlled for baseline age, sex, education, and self-perceived health.
We also conducted two sensitivity analyses. First, we assessed whether the addition of depression in the model would impact the observed association between age status and cognitive change. Depression was examined in this sensitivity analysis (instead of the primary analysis) because 598 participants (or 23% of our cohort) were missing depression values at baseline. The second sensitivity analysis aimed to verify the effects, if any, of baseline differences between the countries included in the analysis.
All analyses were performed using SAS software v9.4 (Cary, NC, USA, 2014).
Results
As predicted, we found that the older individuals living in countries with higher age status experienced better cognitive performance over the 10-year period than those living in lower age status countries. As seen in Table 2, the country-level age status effect remained significant even after controlling for baseline age, sex, education, and self-perceived health (Wilks’s λ = .9921, F = 6.94, p < .001).
Age Status as a Predictor of Cognition Over Time.
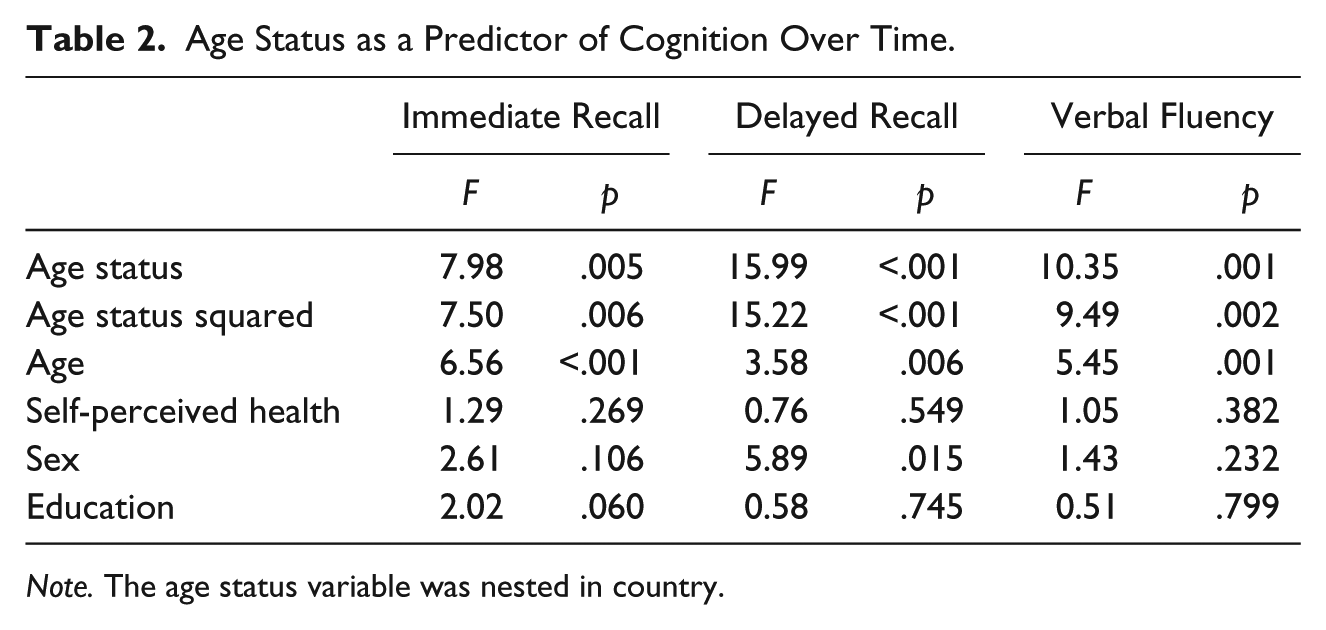
Note. The age status variable was nested in country.
In a sensitivity analysis that included depression in the model, the significant association between better age status and better cognitive performance over time was also found (Table 2; Wilks’s λ = .9915, F = 5.75, p < .001). This suggests the strength of the pattern observed in our initial model, as depression has been shown to impact cognitive decline (Paterniti, Verdier-Taillefer, Dufouil, & Alpérovitch, 2002).
In addition, to confirm that these results were not due to baseline differences associated with age status of the countries, we compared the baseline levels of our covariates (age, education, sex, self-perceived health, and depression) of the countries that were above the median age status with those below the median value of age status. These countries did not statistically differ on any of these factors.
Discussion
To our knowledge, this is the first study to report an association between more positive views of old age in the general population at the country level and individual older persons’ cognitive performance over time. The finding that a narrow range of age status scores across the eight countries led to significant associations with three types of cognitive measures suggests that a small change in the perception of old age at the population level could have a significant effect on individuals’ cognitive health. The finding is notable in view of previous research that found negative age stereotypes are reversible (Levy, Pilver, Chung, & Slade, 2014; Wolff, Warner, Ziegelmann, & Wurm, 2014).
Strengths of the current study include the integration of two well-designed independent datasets of the same countries: a longitudinal dataset of community-dwelling older individuals (SHARE) and a study of the views of its older citizens (ESS). Also, the similarities of the eight Western European countries, as well as the inclusion of the covariates included in the analysis, limit the likelihood of confounding.
Although the combination of two separate datasets (with slightly different populations and data collection methods) allowed us to explore predictor and outcome variable relationships that would not have otherwise been possible, the age status average may not apply to all individuals within a particular region. However, selecting the structural-level and individual-level variables from different datasets helped show that an independent country-level variable is associated with the cognition of the individuals residing in those countries. There is precedence for using a country-level variable to explore broader cultural effects on individuals (e.g., Pachankis et al., 2017).
Considering that the eight countries included in this analysis are from a similar geographic region, it would be interesting to extend this research by examining other countries. Ideally, the additional countries would provide a contrast to the eight—both geographically and culturally.
Several features of the current study support the assumption that age status led to change in cognitive performance, not the reverse direction. The predictor was measured before the cognitive patterns were observed. Moreover, the predictor itself is a country-level variable that is about the status of older individuals, rather than their cognitive function, so it is unlikely that the respondents to the ESS are responding to assessments of cognition.
In conclusion, this study revealed an association between age status and cognitive performance over a 10-year period in a multi-national longitudinal-cohort study of older individuals in Europe. Our findings demonstrate the potentially beneficial impact that positive age status can have on cognitive health outcomes and suggest the need for policy and public-health interventions at the country level to improve cognitive outcomes in older individuals.
Footnotes
Authors’ Note
This articles uses data from SHARE Waves 1, 2, 4, and 5 (DOIs: 10.6103/SHARE.w1.500, 10.6103/SHARE.w2.500, 10.6103/SHARE.w4.500, and 10.6103/SHARE.w5.500). The data analysis for this article was generated using SAS software, Version 9.4 of the SAS System for Windows.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by grant number U01AG032284 from the National Institute on Aging to the senior author.