
Abstract
The effective use of health information is generally viewed as key for preventing and managing ill-health over the life course. However, health information seeking is a complex process (e.g., identifying specific topics of interest, finding information sources, and evaluating the information quality; Gaglio, Glasgow, & Bull, 2012). Health literacy—“the degree to which individuals have the capacity to obtain, process, and understand basic health information and services needed to make appropriate health decisions”—is an essential skill for successful health information seeking (U.S. Department of Health and Human Services, 2010, p. 1). Yet, the majority of older Americans have insufficient health literacy skills, and this population tends to have difficulty locating and evaluating existing health information provided through a variety of sources (Malone, Jo, & Clifton, 2017; U.S. Department of Health and Human Services, 2008). From a public health standpoint, it is particularly important to ensure the access to, and effective use of, health information in later life when people are more likely to face health risks.
Research on health literacy and health information seeking is only in its infancy. Existing empirical evidence is typically based on data from relatively small samples, limited geographic areas, and qualitative interviews (e.g., Gaglio et al., 2012; Kelley, Su, & Britigan, 2016; Taha, Sharit, & Czaja, 2009; Taha, Sharit, & Czaja, 2014). Moreover, the few studies that have used nationally representative data do not specifically focus on health information seeking among middle-aged to older adults (Bennett, Chen, Soroui, & White, 2009; Chen & Feeley, 2014; Feinberg et al., 2016; Prins & Monnat, 2015; Yamashita, Bardo, Millar, & Liu, 2018). Thus, an examination of older subpopulations who have relatively high needs for health information should be an urgent research concern. The present study contributes to this emerging body of knowledge by conducting an exploratory analysis of health literacy and health information seeking with the use of a nationally representative sample of adults age 45 to 74 years.
Method
Data
Data were obtained from the 2012/2014 Program for the International Assessment of Adult Competencies (PIAAC; Rampey et al., 2016). The 2012 PIAAC only targeted those aged 16 to 65 years in the United States, whereas the 2014 PIAAC oversampled adults aged 66 years and older as well as those unemployed in the 45 to 65 years old age group. The PIAAC 2012/2014 data (released to the public in 2016) provide a unique opportunity to examine health literacy and the use of health information sources among a nationally representative sample of older adults. The PIAAC U.S. module adopted the four-stage (i.e., county, census blocks, household, and individuals) stratified area sampling method to ensure the representativeness (Hogan et al., 2016). These data include sophisticated measures for literacy and numeracy (described below), as well as detailed information on health information seeking behaviors. To broadly capture the second half of adult life, respondents age 45 years and older (up to 74 years old) were included in this study. After excluding missing information (n = 290, approximately 8.8% of the total sample), the final analytic sample consisted of 2,989 respondents.
Measures
Dependent variables—Health information sources
The use of eight health information sources (i.e., health professionals, Internet, television, friends and family, books, newspapers, magazines, and radio) was based on the question, “How much information about health issues do you get from . . .?” with four response categories that range from “none” to “a lot.” Responses were dichotomized (i.e., none & a little vs. some & a lot) based on the distributions of original responses (see Tables 1-4) and the interpretability of results in preliminary analyses.
Descriptive Summary by the Health Information Sources (Health Professionals and Internet) for the Adults Aged 45 to 74 Years.
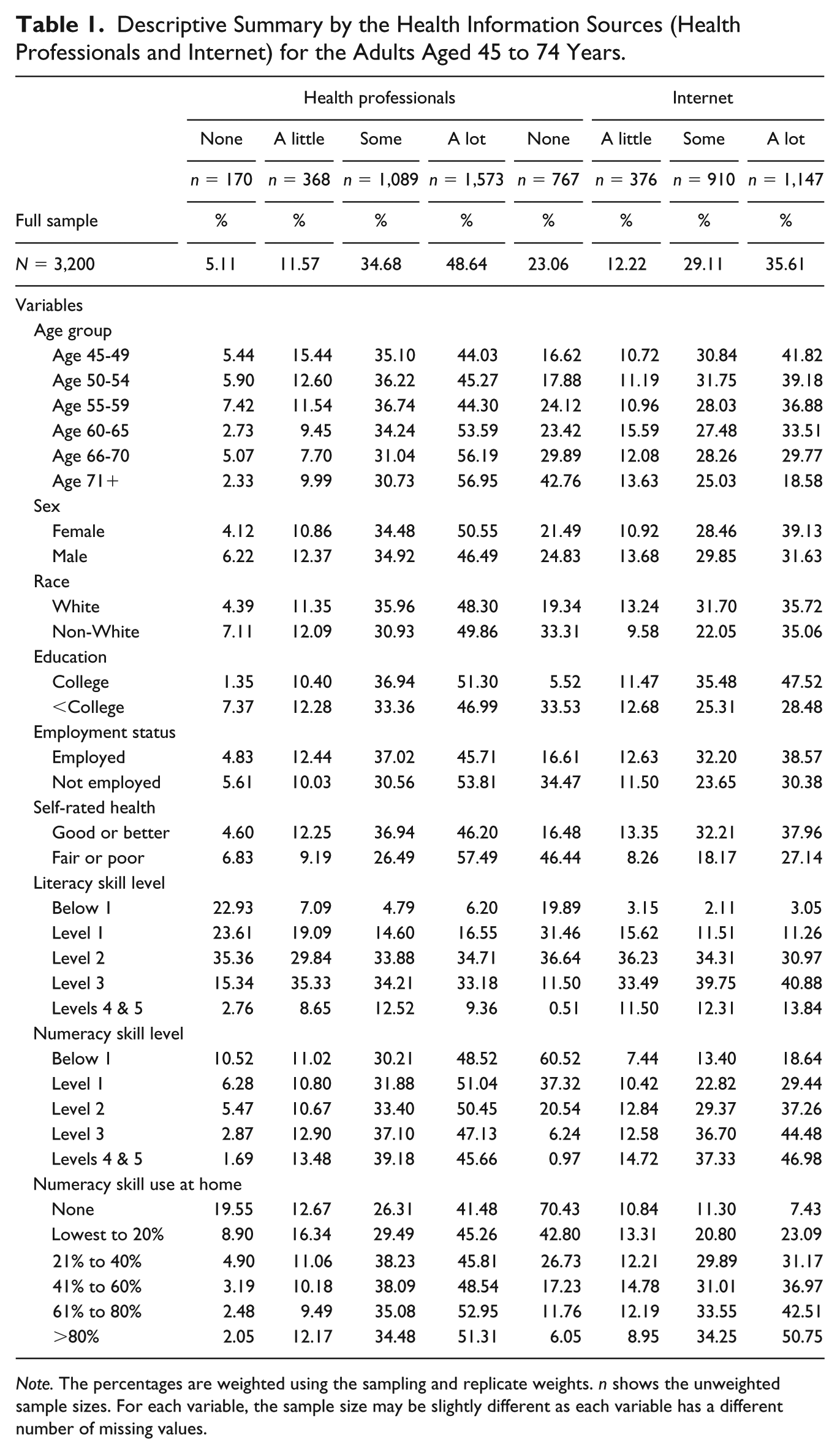
Note. The percentages are weighted using the sampling and replicate weights. n shows the unweighted sample sizes. For each variable, the sample size may be slightly different as each variable has a different number of missing values.
Descriptive Summary by the Health Information Sources (Television, and Friends and Family) for the Adults Aged 45 to 74 Years.
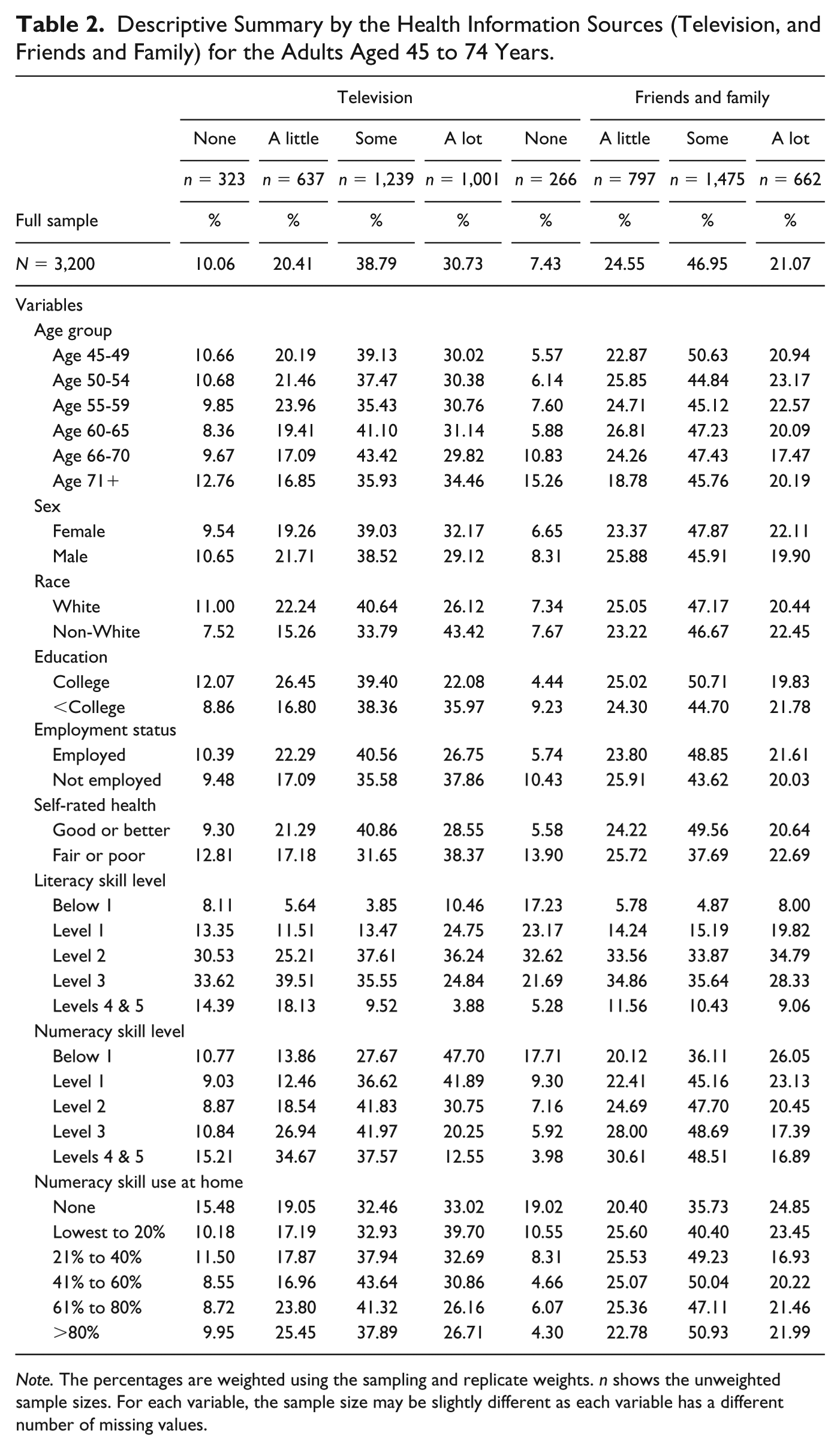
Note. The percentages are weighted using the sampling and replicate weights. n shows the unweighted sample sizes. For each variable, the sample size may be slightly different as each variable has a different number of missing values.
Descriptive Summary by the Health Information Sources (Books and Newspapers) for the Adults Aged 45 to 74 Years.

Note. The percentages are weighted using the sampling and replicate weights. n shows the unweighted sample sizes. For each variable, the sample size may be slightly different as each variable has a different number of missing values.
Descriptive Summary by the Health Information Sources (Magazines and Radio) for the Adults Aged 45 to 74 Years.

Note. The percentages are weighted using the sampling and replicate weights. n shows the unweighted sample sizes. For each variable, the sample size may be slightly different as each variable has a different number of missing values.
Independent variables—Literacy and numeracy
Given that health information broadly consists of both text and numbers, it is critical to examine both literacy and numeracy (Jensen, King, Davis, & Guntzviller, 2010; Peters, Hibbard, Slovic, & Dieckmann, 2007), which collectively reflect the main components of health literacy (Berkman, Sheridan, Donahue, Halpern, & Crotty, 2011). The PIAAC includes a set of 10 plausible values (i.e., the statistical means of estimated score distributions) based on respondents’ performance on the literacy/numeracy tasks (see National Center for Education Statistics, n.d. for specific examples). Literacy and numeracy scores are interpreted based on PIAAC-determined cut-points, which represent skill levels on a 5-point proficiency scale (i.e., 0 to 4 [Below Level 1; Level 1; Level 2; Level 3; Levels 4 & 5]; Organisation for Economic Co-operation and Development [OECD], 2012). Higher levels indicate greater proficiency. However, based on preliminary analyses, which showed the strongest relationship with the health information seeking, a 2-point proficiency scale (i.e., low vs. medium & high proficiency [Below Level 1 & Level 1 vs. Levels 2 to 5]) was employed in this study.
Covariates
A series of covariates were included based on their use in previous research (Berkman et al., 2011; Chen & Feeley, 2014; Suri, Chang, Majid, & Foo, 2014). A measure for numeracy skill use at home was constructed based on responses to six numeracy-related items (see jonas, 2018). The PIAAC-derived index for this measure was utilized, which ordered numeracy skill use into quintiles plus no use (i.e., 1 to 6; 1 = no/least use to 6 = greatest use among PIAAC respondents). Health status, due to its skewed distribution, was dichotomized based on its original 5-point scale (i.e., excellent, very good, and good vs. fair and poor). Age was recorded with the use of indicator variables that denote six approximate 5-year age groups (i.e., 45-49, 50-54, 55-59, 60-65, 66-70, and 71-74 years). A series of dichotomous variables were constructed for gender (1 = female; 0 = male), race (1 = White; 0 = non-White) and educational attainment (1 = college or higher; 0 = less than college).
Analytic Approach
A descriptive summary for all variables was generated using the final sampling weight (SPFWT0) and 80 replicate weights (SPFWT1-SPFWT80). SAS macro programs produced by the IDB Analyzer application version 4.0.8 (IEA, 2016) were utilized to incorporate sampling weights and sets of literacy/numeracy plausible values. Binary logistic regression (Hosmer & Lemeshow, 2004) was employed to model use of each health information source as a function of literacy, numeracy, and covariates. Unconditional models with literacy and numeracy were constructed first, and covariates were added to the final model. The sampling and replicate weights were incorporated into all analyses, and statistical significance was evaluated at the alpha = .05 level. Analyses were conducted using SAS version 9.4 (SAS Institute Inc., 2013).
Results
Tables 1 to 4 show the distribution of health information sources by variables of interest. To provide a detailed descriptive summary, the original response categories (none, a little, some, and a lot) were used. Overall, the most common source that individuals obtain “a lot” of health information from is health professionals (49%), followed by the internet (36%), television (31%), friends and family (21%), books (16%), radio (9%), newspapers (9%), and magazines (9%). Approximately 25% to 50% of respondents reported that they obtain “some” health information from each of the eight sources, respectively. The least common health information sources, in terms of reporting use as “none” or “a little,” are radio (63%), newspapers (60%), and magazines (53%).
Tables 5 and 6 show results from fully conditional binary logistic regression models that estimated the association between health information sources, literacy, and numeracy. Literacy was positively associated with obtaining information from health professionals and Internet. That is, adults with medium to high literacy proficiency were more likely to use health professionals and the Internet to obtain health information. Four of the eight health information sources were statistically significantly associated with numeracy skills. Specifically, those with medium to high numeracy proficiency are less likely to use television, books, newspapers, and magazines as sources for health information, net of demographic characteristics, socioeconomic status, health status, and use of numeracy skills at home.
Health Information Sources (Health Professional, Internet, Television, and Family & Friends): Estimated ORs From Binary Logistic Regression Models.
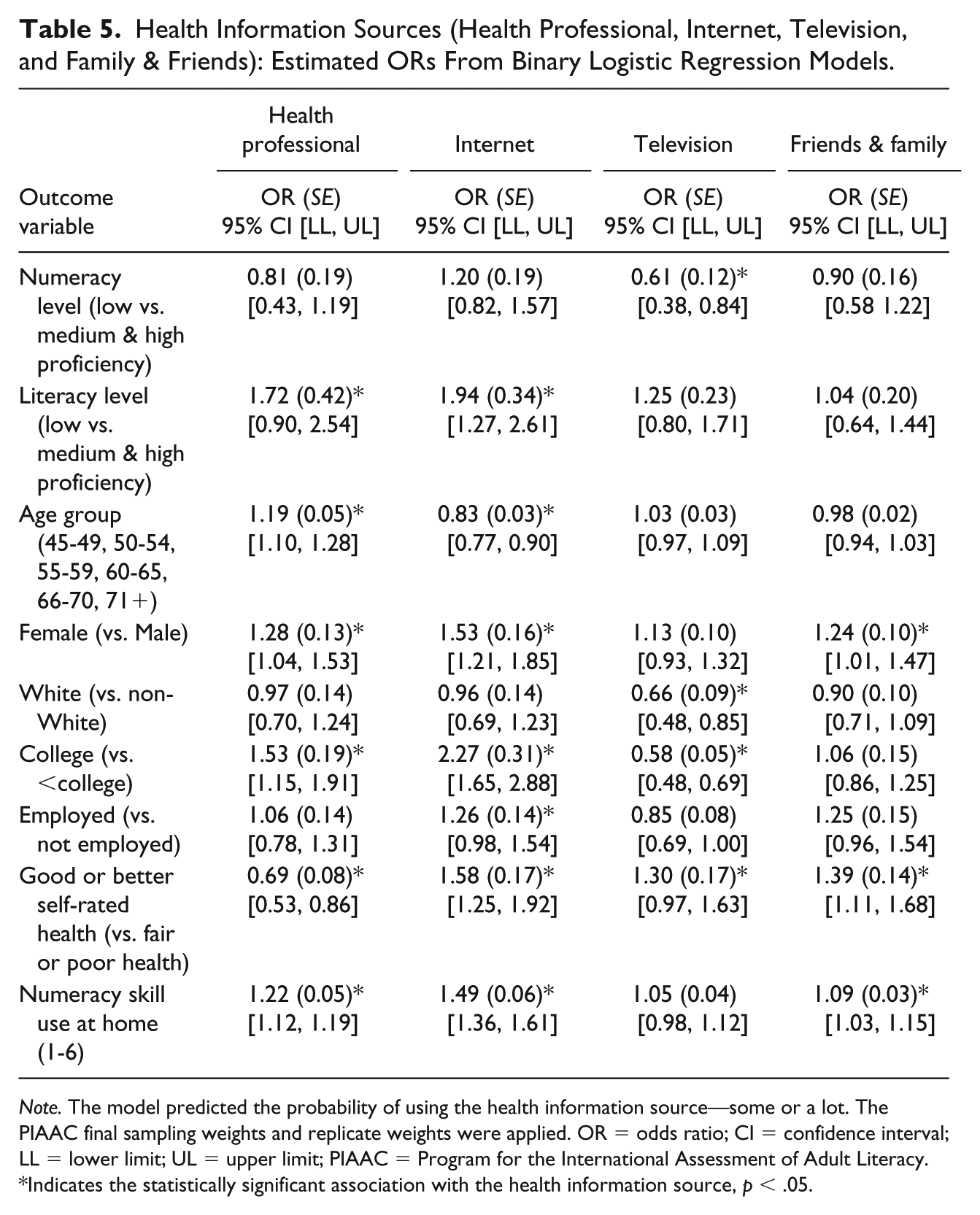
Note. The model predicted the probability of using the health information source—some or a lot. The PIAAC final sampling weights and replicate weights were applied. OR = odds ratio; CI = confidence interval; LL = lower limit; UL = upper limit; PIAAC = Program for the International Assessment of Adult Literacy.
Indicates the statistically significant association with the health information source, p < .05.
Health Information Source (Book, Newspaper, Magazine, and Radio): Estimated ORs From Binary Logistic Regression Models.

Note. The model predicted the probability of using the health information source—some or a lot. The PIAAC final sampling weights and replicate weights were applied. OR = odds ratio; CI = confidence interval; LL = lower limit; UL = upper limit; PIAAC = Program for the International Assessment of Adult Literacy.
Indicates the statistically significant association with the health information source, p < .05.
Discussion
A lack of nationally representative findings surrounding the use of health information sources and health literacy in later life is clearly a gap that needed to be addressed. This study analyzed nationally representative data of adults age 45 to 74 years and found that literacy and numeracy are uniquely associated with different health information sources. Literacy was positively associated with use of health professionals and the Internet, and numeracy was negatively associated with television, books, newspapers, and magazines. The positive effects of literacy might reflect the quality of communication with health care providers. Also, given that Internet-based health information tends to be text-based, searching for health information online likely requires sufficient literacy skills (Feinberg et al., 2016).
The negative association of numeracy with several health information sources was surprising. Numeracy is essential to accurately comprehend and use numeric health information. Particularly, precise estimation of health risks and benefits is associated with better health decisions, greater compliance with recommended practices (e.g., medication, preventive health service), and earlier access to necessary medical treatment (Peters et al., 2007; Reyna, Nelson, Han, & Dieckmann, 2009). As such, the negative association of numeracy with specific health information sources might reflect prior successful health information seeking experience (e.g., Chen & Feeley, 2014). In other words, middle-aged and older adults with proficient numeracy may not exhibit extensive and/or repetitive health information seeking behaviors across multiple sources due to their sufficient knowledge, efficiency, and confidence in their abilities to make health decisions.
This study is not without limitations. For example, omitted variable bias cannot be ruled out. Also, literacy and numeracy are not identical to the concept of health literacy. At the same time, literacy and numeracy are sound indicators of health literacy (DeWalt & Pignone, 2005). Despite such limitations, this study makes important contributions to an emerging body of knowledge, including the detailed presentation of nationally representative findings of literacy, numeracy, and other characteristics of middle-aged and older adults by health information sources. Also, we showed that literacy and numeracy have distinctive roles in the context of health information seeking. This information should be useful for health information providers (e.g., health organizations, government agencies, and health professionals) interested in improving current health communication practices (e.g., omission of required calculations in health information, use of visual aids; Peters et al., 2007). Given a lack of prior nationally representative evidence, findings from the present study reflect a foundation from which future research can build. A better understanding of literacy and numeracy is a critical step toward enhancing access to, and utilization of, quality health information in later life.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research reported here was partially supported by the Institute of Education Sciences, U.S. Department of Education, through Grant R305A170183 to Miami University and University of Maryland, Baltimore County. The opinions expressed are those of the authors and do not represent views of the institute or the U.S. Department of Education. In addition, this research was partially funded by the American Institutes for Research through a contract with the National Center for Education Statistics of the U.S. Department of Education.