
Abstract
Introduction
Social, health, and economic disparities between racial/ethnic populations and the overall U.S. population remain major public health and social work concerns (Hill, Pérez-Stable, Anderson, & Bernard, 2015). Although health disparities are complex and exist in all age groups, geographic areas, and within socioeconomic groups, certain populations are more at-risk and experience greater disparities in health and income than others (Hill et al., 2015). Native Hawaiians, one of the indigenous populations in the United States, have documented poorer health profiles than the nation’s dominant White population group (Braun & LaCounte, 2015). Health disparities typically widen in older age groups, resulting in the increased need for health and long-term service and support (LTSS) in disadvantaged groups (National Institute on Aging, 2016). In this article, we briefly summarize the results of a mixed-method research (MMR) approach that examined the health and LTSS needs and care preferences of Native Hawaiian elders. We then turn to data synthesis, the primary focus of this article, and offer three practice, policy, and research directions to facilitate improvements to kūpuna health and service use. An MMR design can advance knowledge on social and health disparities in this population and other underserved elder populations.
Background and Problem Statement
The 2010 U.S. Census reported that 1,225,295 of the nation’s citizens claim Native Hawaiian and other Pacific Islander (NHOPI) ancestry, alone or in combination, representing 0.4% of the country’s population (U.S. Census Bureau, 2010). Native Hawaiians are the indigenous people of the Hawaiian archipelago. In the United States, they make up the largest subpopulation (46%) under the NHOPI label (U.S. Census Bureau, 2010). About 1.2 million NHOPI were identified in 2010, with 540,103 identified as “Native Hawaiian alone” and 681,182 as “Native Hawaiian in combination with one or more races” (U.S. Census Bureau, 2010). About 60% of the country’s Native Hawaiian population lives in the State of Hawai’i. On the continental U.S., California and Washington have the greatest numbers of Native Hawaiians (Kamehameha Schools, 2014). Compared to other ethnic groups in Hawai’i, Native Hawaiians experience significant disparities in health, such as shorter life expectancy and higher rates of disability due to chronic diseases, including heart disease, cancer, and diabetes (Ka‘opua, Braun, Browne, Mokuau, & Park, 2011; Mokuau, 2011). More Native Hawaiian elders (kūpuna) reside with families compared with other ethnic groups in the state (Kamehameha Schools, 2014), and the limited available data suggest that formal LTSS services are seldom used (Alu Like, 2005). The low utilization of services for kūpuna may result from unique socioeconomic, geographic, and cultural characteristics of Native Hawaiians (Braun, Browne, Ka‘opua, Kim, & Mokuau, 2014). The consequences of a lack of essential support for elders can result in significant and negative consequences for the elder and their family’s economic, health, and overall well-being (Pearlin, Schieman, Fazio, & Meersman, 2005; Reinhard, Feinberg, Choula, & Houser, 2015; Robison, Fortinsky, Kleppinger, Shugrue, & Porter, 2009). Thus, family caregivers are also important stakeholders when assessing LTSS needs and preferences.
This study was conducted by a university center staffed with indigenous and nonindigenous faculty researchers. The center honors community-based participatory research (CBPR) principles (Israel, 2000), is rooted in cultural competence with Native Hawaiian communities (Mokuau, Browne, Braun, & Choy, 2008), and is guided by a community advisory council comprised of Native Hawaiian health and eldercare leaders. This study aims to assist community partners identify health and LTSS needs and care preferences of kūpuna and ‘ohana caregivers and is part of a larger national assessment of indigenous elder and family LTSS needs (Braun, Kim, Ka‘opua, Mokuau, & Browne, 2014; Nakatsuka, Esquivel, Levin, Browne, & Braun, 2013).
Theoretical Frameworks on Age, Race/Ethnicity, and Indigenous Populations
Two frameworks and perspectives—life course and minority stress theory—provided a foundation to examine the health and LTSS needs and care preferences among Native Hawaiian elders and families. The life course perspective conceptualizes old age as a phase of life that is shaped by personal biography and the influence of cohort and historical time period in the individual’s life span leading up to old age (Elder, 1994; Hudson, 2016). Increasingly, researchers call for greater application of life course analysis when examining diverse aging and inequalities by race and ethnicity (Ferraro, Kemp, & Williams, 2017; Glymour, Ertel, & Berkman, 2009). Minority stress, our second theoretical framework, builds on earlier work on stress-process models that suggest that the persistent (chronic) stress often experienced by minority groups generates psychological and physiological responses that accumulate over time to produce poor health outcomes (Brandolo, Gallo, & Meyers, 2009; Kim, Jun, Lee, & Browne, 2017; Meyer, 2003; Pearlin et al., 2005; Sotero, 2006). Stressors may include experiences with institutional racism, bias, and financial insecurity. Relatedly, investigations of historical trauma acknowledge and document the role of forced colonization on the health of native peoples (Stanley et al., 2017; Walters et al., 2011). Indigenous and nonindigenous researchers thus advocate for studies with and on native populations in the United States that recognize the influence of systematic discrimination and intergenerational marginalization on their current health disparities (Brave Heart & Debruyn, 1998; Stanley et al., 2017). Populations also have resilience-based factors to help cope with stressors and their consequences, including cultural norms, values, traditions, and collective responses (Hausmann, Kressin, Hanusa, & Ibrahim, 2010). Native Hawaiian cultural values and practices, delegitimized for more than a century by those who colonized Hawai’i, are a source of resilience and have been found to improve health and well-being when built into program interventions (Kaholokula et al., 2017; Kamehameha Schools, 2014; Mokuau, Braun, & Daniggelis, 2012).
A better understanding of needs and the underlying interactions among these factors can lead to developing interventions, critical insights, and recommendations to improve health. In this article, we describe our approach to illustrate how an MMR design can be appropriate and useful to expand knowledge on social and health disparities in understudied populations. We present a brief summary of study rationale and individual study phases. We then turn to our primary focus on data integration and conclude with synthesis and practice, policy, and research directions. For a full discussion on methods, we refer the reader to a series of earlier publications (See Braun, Browne, et al., 2014; Braun, Kim, et al., 2014; Browne et al., 2014; Mokuau et al., 2015).
Method
Overview of Study Rationale and Design
Study rationale
Based on our prior research and practice with Native Hawaiians, we realized that no one method could adequately answer our primary question, which we stated as: “What are the health and LTSS needs and care preferences of Native Hawaiian elders and family caregivers?” Kūpuna, defined as those above the age of 60 years, are respected members of the Native Hawaiian community who nonetheless face a range of social and health disparities compared with other older adults (Braun, Kim, et al., 2014; Mokuau et al., 2015). Our meetings with community and university experts and an extensive literature review uncovered limited knowledge of health and LTSS needs and preferences of elder Native Hawaiians, a population that is family centric and places high importance on cultural values, traditions, and practices in everyday life (Mokuau, 2011). As an oral–aural culture, qualitative approaches have been well received in previous work (Mokuau et al., 2015). At the same time, information on health behavior, disease prevalence, and life expectancy can only be gleaned from secondary analysis of large data sets. The State of Hawai’i Department of Health publishes data from numerous sources, but has few reports on older adults by ethnic group.
Study design
We turned to an MMR design to allow us to combine elements of qualitative and quantitative data collection to gain a broad and deep understanding of the LTSS needs and preferences of Native Hawaiian elders. Researchers who utilize MMR designs reject the notion that one method of data gathering and analysis is superior to another and instead argue that “method eclecticism” can lead to better conclusions (Brannen, 2005; Curry, Nembhard, & Bradley, 2009; Happ, Dabbs, Tate, Hricik, & Erlen, 2006; Tashakkori & Teddlie, 2003; Wisdom & Creswell, 2013). An MMR approach to research often adheres to a mix of top-down deductive and bottom-up inductive processes in the same or multiphase studies. Despite concerns voiced by a number of researchers on MMR designs around philosophy, language, nomenclature, and the evolving typologies of MMR designs (Clarke, 2009; Happ, 2009; Schoonenboom & Johnson, 2017), we concluded that an MMR design would provide us with flexibility and tools to answer our practice-based research question with cultural congruence (Braun, Browne, et al., 2014; Mokuau, 2011). MMR also aligns with CBPR approaches, supporting our engagement with a variety of community and university stakeholders concerned with and affected by Native Hawaiian health.
MMR typologies
To prepare for this study, we examined the work of several researchers who developed exemplar typologies for classifying MMR approaches (Creswell & Plano Clark, 2006; Greene, Caracelli, & Graham, 1989; Onwuegbuzie & Combs, 2010; Onwuegbuzie & Teddlie, 2010). For our study philosophy, we adopted the pragmatic (vs. constructivist) approach in which qualitative and quantitative data are collected to identify solutions and solve problems (Creswell & Plano Clark, 2006). To answer our primary question, we chose three data collection approaches—key informant interviews, focus groups, and secondary analyses of large health data sets—using a QUAL-QUANT-QUAL sequential exploratory design. This required a research team expert in different approaches, and we alternated lead roles dependent on our skill sets. No data set was dominant over another; rather, each phase of data collection complemented the others to see the larger picture. This exploration was aimed at discovery in contrast to testing hypotheses. Data analysis was primarily parallel, with each data set analyzed and reported separately, and integration and syntheses followed the study completion of three phases.
Summary of Study Phases
To answer our question, “What are the health and LTSS needs and care preferences of Native Hawaiian elders and family caregivers?”we gathered data in three phases. Phases 1 and 3 were qualitative, and Phase 2 was quantitative.
Phase 1: Key informant interviews—QUAL
This phase provided descriptive and contextual data on what experts in Native Hawaiian health believed were the health and LTSS needs and preferences of Native Hawaiian elders and families. Community partners were instrumental in accruing our sample composed of social workers and health care administrators, physicians, nurses, and public health specialists on the islands of Hawai‘i, Moloka‘i, O‘ahu, Maui, and Kaua‘i. We used semistructured interview questions designed by the research team with advisory council members input and based on our collective expertise in aging, caregiving, culture, and Native Hawaiian health. These questions with the corresponding results assisted in the development of our listening study group questions (Phase 3) Browne et al., 2014).
Phase 2: Survey data from the Hawai’i Health Survey (HHS), Behavioral Risk Factor Surveillance System (BRFSS), and vital records—QUANT
Here, we documented the health status and behavioral practices of Native Hawaiian elders compared with the state’s other major ethnic groups. In partnership with the Hawai’i State Department of Health, we analyzed data from three data sets: the HHS, the Hawai’i BRFSS, and state death records. The HHS is a random sample telephone survey of adults that gathered data from a random sample of 6,000+ household members on gender, age, race, education, household size, insurance status, health status, morbidity, and food security. The Hawai’i BRFSS is part of the Centers for Disease Control and Prevention (CDC)’s BRFSS, the largest ongoing telephone health survey system tracking health conditions and risk behaviors in the United States. It identifies health behaviors and problems (e.g., smoking, drinking, and chronic diseases) and helps establish and track health objectives, support heath policies and legislation, and develop and evaluate public health programs. Death record data were used to construct life tables to estimate life expectancy.
Phase 3: Listening (focus) groups—QUAL
Six listening study groups were convened and attended by 30 Native Hawaiian elders and caregivers in the state of Hawai’i and another 30 in the Los Angeles and San Diego areas. Hawaiians on the West Coast were included because of a large portion (40%) of the Hawaiian population now resides in the continental U.S., with nearly 75,000 residing in California (Kamehameha Schools, 2014). For this third phase, a series of open-ended questions were used to identify the needs of elders and caregivers around health and LTSS needs and preferences “in their own voices.” Questions were built on the literature, from this study’s key informant phase, and community input. We also wanted to explore the role of culture in the lives, health, and care preferences of kūpuna. Recent studies on Native Hawaiian health documented positive outcomes of integrating cultural values into health promotion programming (Kaholokula et al., 2017; Tomioka, Braun, Compton, & Tanoue, 2012).
Data Analysis
The key informant and focus group phases (1 and 3, respectively) utilized established qualitative data analysis methods to identify themes and interpret the data (Lingard, Albert, & Levinson, 2008). We employed constant comparison analysis, using inductive coding to systematically reduce data to codes and then develop emerging themes from the codes.
In Phase 2, we applied the abridged method for the construction of life tables as proposed by Chiang (1984). Death record data for Hawai’i were provided by the Hawai’i State Department of Health. Numbers of death were calculated based on the mean number over a period of 3.5 years centering on April 1, 2010. Population estimates were based on the Hawai’i Census 2010, adjusted by ethnicity estimates from the HHS. Frequencies were used to compare prevalence of chronic conditions and health behaviors between Native Hawaiian and elders of other ancestries in Hawai’i.
Data integration
We followed the principle of complementarity as we sought to elaborate, illustrate, enhance, and clarify findings from one analytical phase with another (Tashakkori & Teddlie, 2003). Each phase’s data set was first analyzed and reported separately with data syntheses and integration following full study completion. We used Schoonenboom and Johnson’s (2017) definition for data integration as “the point in a study whereby two or more research components are mixed or combined in some way” to further expand answers to the study’s main question. Quantitative and qualitative data were descriptively and thematically integrated, and from data integration emerged a deeper picture of five findings of Native Hawaiian elder health and LTSS needs and care preferences.
Summary of Results and Data Integration
Results
We present here a brief summary of these findings and then move to this article’s primary focus on study integration and synthesis. Findings from Phase 1 (Native Hawaiian key informants) uncovered financial concerns of families who provided elder care, need for easy access to health and LTSS, and preferences for care that were rooted in Native Hawaiian or “local” values influenced by traditional values of kāko’o (help/support). Elders hoped to age in place with help from their ‘ohana, but identified financial barriers and geographical challenges, that is, limited public transportation (Browne, Mokuau, & Braun, 2008). In Phase 2, findings identified that health disparities were faced more by Native Hawaiians elders compared with most other ethnic groups in the state of Hawai’i, including shorter life expectancy (Wu et al., 2017) and a higher prevalence of disability, behavioral risks, and specific chronic conditions, including cancer, heart disease, obesity, diabetes, asthma, and substance abuse (Braun, Browne, et al., 2014). This group also has a lower median income, a lower rate of home ownership, and a lower percentage completing college than other groups (Braun, Browne, et al., 2014). In Figure 1, we provide our updated data on life expectancy (Wu et al., 2017). We were unable to access similar data from California that was specific to Native Hawaiians.

Life expectancy by race/ethnicity in Hawai’i.
Findings from Phase 3’s focus groups with kūpuna and caregivers were organized around four overarching themes: the respected role of hulu kūpuna (precious elder) in the family, and the genealogical link of past, present, and future; the desire to age in place with a preference for home care, education, and supportive services that reflect respect for elder and Hawaiian cultural values; health-related challenges and costs of care associated with age; and the social stressors, especially stigma and discrimination, that discouraged some from seeking and using formal services.
Study Integration
From data integration emerged four findings that were not covered in any one individual study approach. First, survey data from Phase 2 confirmed the poor health status and numerous disparities experienced by Native Hawaiian elders in Hawai’i, including lower socioeconomic status, earlier disability, and shorter life expectancy compared with other racial/ethnic populations in the state. We expected to see these results given the well-documented poor health profile of Native Hawaiians in younger age groups. But data integration exposed how little elders in our focus groups were aware of this poor health profile. There was a general lack of knowledge of their serious health disparities including a much shorter life expectancy, the greater health risks they faced compared with other racial/ethnic groups, and of services and strategies to promote health and prevent or minimize disability.
The second finding, similar to non-Native Hawaiian elders in both Hawai’i and on the continental U.S., centered on the high costs around health and LTSS needs that worried our participants. This is a national concern. However, Native Hawaiians may be more at risk due to their lower socioeconomic profile documented in Hawai’i and a propensity to reside in rural communities with fewer services.
Third, a number of kūpuna and family care preferences were similar to other populations in the United States—i.e., the desire to age in place with family assistance for elder support. What was dissimilar was their care preference for services grounded in Native Hawaiian culture, and a preference to use professionals who were knowledgeable and respectful of this heritage. Study participants voiced the pride of being Native Hawaiian, and of the strengths inherent in Native communities. In contrast to a prevalent Western view of age, aging in Native Hawaiian culture was equated with wisdom and respect for elders, and remains a strong family and community value. One study result was that cultural values and experiences shaped participant use of services and care preferences. Native Hawaiian cultural values served as a foundation for caregiving and for preferred LTSS services for kūpuna. These included the values of ‘ohana (family), kuleana (responsibility), and spirituality. Care for kūpuna was rooted in the cultural importance of koko (biological relations) but also pilina (close relationships) in the broader kinship network, which included the family, environment, and the spiritual realm. One elder who resides in California explained her desire to stay culturally connected.
We don’t have other Native Hawaiians close to us like back home. We feel like we are being assimilated in this society but want to keep our roots strong. How do we perpetuate our culture when we don’t have day-to-day contact like they do back home? It wears on you. (Browne & Braun, 2017)
Finally, information emerged from Phase 3’s qualitative data that revealed Native Hawaiian exposure to discrimination in education, employment, and access to service. Survey tools from Phase 2 did not include questions about real and/or perceived discriminatory acts. In Phase 3, listening sessions asked participants if they had experienced any barriers to care. Elders on the continental U.S. spoke freely, often, and with the intensity of the stigma and prejudicial attitudes toward Native Hawaiians growing up in Hawai’i prior to the 1970s, when Hawaiian values, traditions, language, and people began to garner increased interest and respect (Marsella, Oliveira, Plummer, & Crabbe, 1995). Kūpuna in Hawai’i voiced their concerns that few service providers were deemed sensitive to and respectful of Native Hawaiians. Both groups shared experiences of perceived and real discrimination by service providers. These findings from Phase 3 provide support for theories of minority stress and historical trauma discussed earlier.
Synthesis and Practice, Policy, and Research Directions
Health and LTSS use and care preferences are products of complex and interacting factors. From these findings, we suggest three practice, policy, and research implications and directions that may advance knowledge and facilitate kūpuna health and service use (see figure 2).
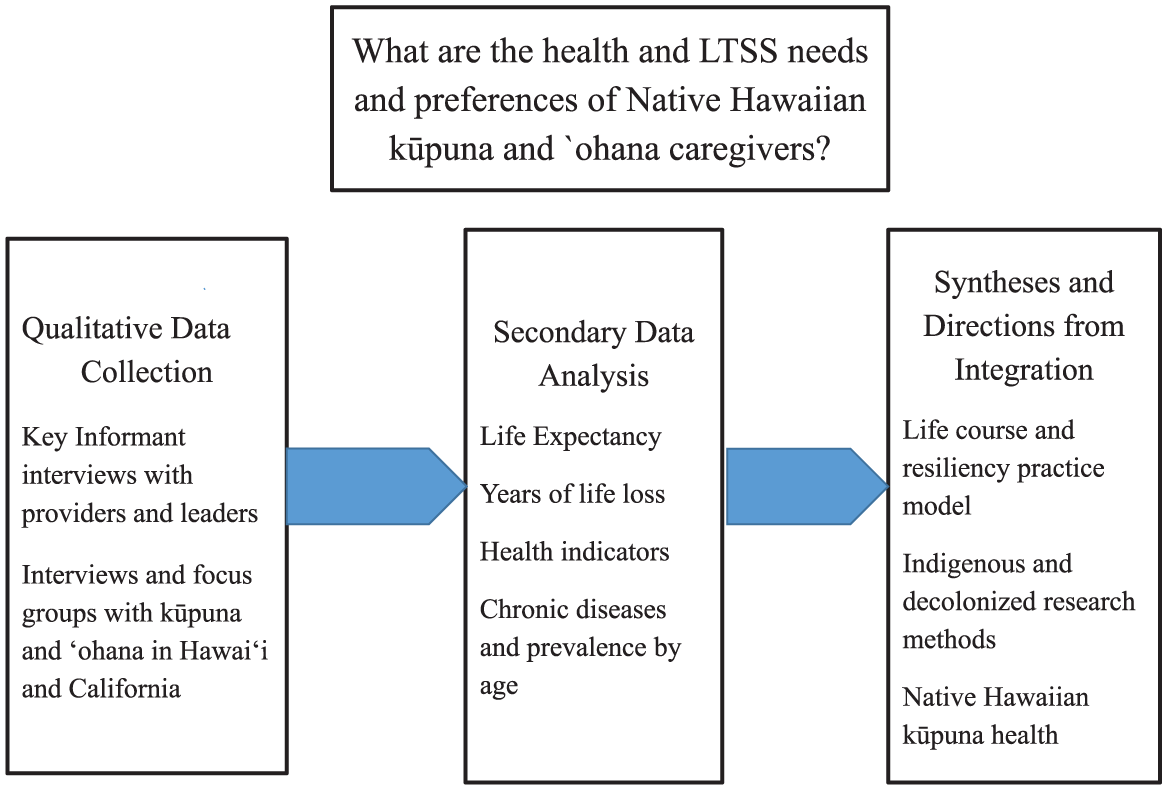
Study approaches and directions.
Life Course and Resilience Practice Model
Returning to theoretical perspectives and frameworks, life course speaks to a number of issues exposed in this study. In Hawai’i, Native Hawaiians have lower levels of educational attainment than the state’s other dominant cultures, which have led to fewer options for employment and housing. Fewer options reduce time and income for health care, nutritionally rich foods, and leisure time physical activity, which in turn have led to higher morbidity rates and shorter life expectancy in this population. Moreover, kūpuna experiences with aging and the ‘ohana’s caregiving experiences were negatively affected by stressors associated with stigma, discrimination, and poverty. The poor health and service utilization rates of Native Hawaiians are contrasted with examples of impressive individual, family, and community resilience centered around the pride of being Native Hawaiian and the strengths inherent in Native communities. These resilience factors were integrated into a conceptual practice model, Ola Pono Nā Kūpuna, which celebrates resilience while calling for policies and programs that reverse the biases in the institutional systems (e.g., education, health care) that perpetuate unequal access to resources and, thus, health disparities (Browne, Mokuau, & Braun, 2009). Suggesting a rationale for the development and implementation of culturally grounded practice solutions for kūpuna, the model underscores the need for work at the policy level to affect the change needed to improve lives. For example, Native Hawaiian shorter life expectancies point to the need for health education and primary health care to begin at younger ages, and for preventive and supportive services for elders, to start with “younger” older adults. At the same time, the Native Hawaiian cultural renaissance that began in the 1970s suggest future care preferences may be increasingly grounded in cultural values, family centered approaches, and an emphasis on aging-in-place within a “sense of place” that reflects deep identity connections to the community and land (Kaholokula et al., 2017; Mokuau, 2011). More research is needed on the measurement of resilience and other factors that promote health given the heterogeneity within the Native Hawaiian population, a changing cultural milieu, geographical differences, and generational and other changes that will alter needs and preferences.
Indigenous and Decolonized Research Methods
We explored ways of conducting research with indigenous elders, and ending up critiquing approaches, including our own, that are often used to gain knowledge of indigenous elders (Braun, Kim, et al., 2014). As we did in Phase 2 of this study, researchers often mine existing data sets to compare characteristics of indigenous populations with non-indigenous groups, and findings often reveal significant disparities. But research also has shown that data collection instruments developed for White cultures, like those used to gather the quantitative data we analyzed, may not resonate with non-White cultures. This finding should lead to the development of new tools that come from the cultural population of study, as well as examination of how standardized tools can be adapted to better fit indigenous views of the construct being measured. We also learned that the usefulness of findings from qualitative studies will depend on the interview questions and who is asking them. Participatory and decolonizing research methods appear best able to empower indigenous elders as researchers and thus obtain data of use to their own communities. Because many indigenous people have had negative experiences with Eurocentric research, research should consider the use of participatory and decolonizing approaches that acknowledge life course perspectives, minority stress theory, and resilience. Our research experiences confirmed the importance of participatory approaches in research with kūpuna, and the critical role research can play in helping to view health inequalities as an injustice that can and should be preventable and remedial (Hebert, Sisk, & Howell, 2008; Stanley et al., 2017).
Policies and Strategies to Improve Native Hawaiian Elder Health
Although our data confirmed poorer health and shorter life expectancy among Native Hawaiians, kūpuna and ‘ohana caregivers had no knowledge of these disparities. The need for health education and health promotion throughout the life course remains great for all populations, but especially those with poor social and health profiles. Strategies here can include research dissemination that targets both professional and lay audiences, community presentations in neighborhoods where high numbers and proportion of Native Hawaiians reside, and the use of community “guides” to engage elders and families in culturally anchored practices (e.g., food, customs, language) Mau et al., 2010; Mokuau, 2011; Townsend et al., 2016). Data also highlighted that concerns over care costs were similar to those found in studies of dominant U.S. cultures (Reinhard et al., 2015). Native Hawaiian families face additional problems of access due to distance from care in rural communities, perceived discriminatory attitudes by providers, and mainstream-oriented services that can be inconsiderate of Hawaiian cultural values. Programs and policies that support and attend to health by recognizing a people’s history, cultural values, and wisdom can begin to address and fight injustice and discrimination when coupled with advocacy training (Watt, Abbott, & Reath, 2016). For example, we can increase the number of Native Hawaiians who enter the social service and health professions, with the hope that they will provide more culturally grounded services in underserved communities.
Those working with native elders should become knowledgeable of the growing work of indigenous researchers and practitioners who report positive health outcomes from culturally grounded interventions (Braun, Fong, Kaanoi, Kamaka, & Gotay, 2005; Kaholokula et al., 2017; Kaholokula et al., 2011; Ka’opua, Park, Ward, & Braun, 2011; Mau et al., 2010; Mokuau et al., 2012; Townsend et al., 2016). The continued funding of Social Security, Medicare, and Medicaid are critically important policies for indigenous elders, as are programs for native elders funded through Title VI of the Older Americans Act, ACL/AoA. Access to these and other policies and programs have huge significance and implications for the health and LTSS for other racial/ethnic and underrepresented elder populations. Living below the poverty level and residential segregation that limits access to health care and health promotion affects other elder at-risk groups (Blackwell, Lucas, & Clark, 2014; Hwa, Jang, Han, & Chiriboga, 2011; Kim et al., 2017). In the end, the nurturing of internal resilience factors and the support and building of external supports require attention over the life course rather than a sole focus on the later years. Working together, a range of research, practice, and policy approaches will be most effective in helping kūpuna and their ‘ohana overcome and rebound from chronic life stressors.
Study Limitations
This MMR study was initiated in 2008 with suggestions from our advisory council, and data collection was completed in 2016. A primary challenge to this MMR design was in this study’s sequential time frame that resulted in nearly 8 years for study completion of all three phases. We addressed this in part by a reanalysis of the life expectancy data (Figure 1). A public health priority is the study of racial/ethnic and other underrepresented groups and the aim to reduce social and health disparities. This article presents this study’s contributions to understanding the health and LTSS needs and preferences in one understudied native elder population and the applicability of these data to facilitate improvements in their health and LTSS use.
Conclusion
The complex nature and persistence of health disparities among Native Hawaiian elders call for new strategies and collaborations with native peoples that may have implications with other racial and ethnic populations in the United States. The use of MMR approaches employed in this study demonstrated how research with Native Hawaiians can lead to new insights and new practice, policy, and research priorities. Other racial/ethnic, underrepresented and marginalized populations commonly omitted from research participation may find utilization in this MMR approach. Attending to health and LTSS with the goal of ultimately reducing health disparities and improving quality of life and care is complicated. Continued attention to health equity for Native Hawaiians and other populations across the life course requires a commitment by those who work with and on behalf of elders to attend to a people’s history, cultural values, and wisdom in building resilience, ending discriminatory policies, and improvements in socioeconomic status.
Footnotes
Acknowledgements
The authors gratefully acknowledge the many elder and family participants who generously gave their time for this study, and members of our Advisory Council who guide our work.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded in part by the Administration on Community Living, Administration on Aging, DHHS, Washington, DC, by Grant 90O10007-01. Grantees undertaking projects under government sponsorship are encouraged to express freely their findings and conclusions. Points of view or opinions do not, therefore, necessarily represent official government policy.