
Abstract
Introduction
Scientific interest in religiosity as a social determinant of health is historic (Durkheim, 1915; George, Larson, Koenig, & McCullough, 2000; Hiltner, 1943; Koenig, 1989; Krause, 2011; Musick, 1996). The long-standing curiosity in religiosity among social scientists is understandable given religion both reflects and influences societal values and norms and subsequently behaviors. While it is not universal, the preponderance of empirical evidence indicates religiosity is salutary (Jarvis & Northcott, 1987; Koenig, 2012; Larson, Swyers, & McCullough, 1998; Moreira-Almeida, 2013). The most common dimension of religiosity referenced across these studies is participation at religious services (Bagiella, Hong, & Sloan, 2005; Hummer, Rogers, Nam, & Ellison, 1999). Such participation has been linked to a large set of physical and psychological morbidities such as hypertension, heart disease, cancer, cognition, diabetes, pulmonary disease, and depression, to name a few (Buck, Williams, Musick, & Sternthal, 2009; Corsentino, Collins, Sachs-Ericsson, & Blazer, 2009; Koenig, 2002; Kune, Kune, & Watson, 1993; McCullough & Larson, 1999; Newlin, Melkus, Tappen, Chyun, & Koenig, 2008).
How the association pertains to older persons is receiving increased attention that is timely given global population aging (Krause et al., 2002; Lawler-Row & Elliott, 2009; Lucchetti et al., 2011; Zimmer et al., 2016). Taiwan, located in East Asia, is a region that has witnessed extraordinary growth in its older population, a function of sharp fertility and mortality declines over the last several decades. In Taiwan, as in other parts of East Asia, rapidly rising numbers of older persons are occurring concomitantly with a push to slow down disability onset and functional decline (Hermalin & Myers, 2002; United Nations Population Fund [UNFPA] & HelpAge International, 2012). Diagnostics and treatment are important, but psychosocial factors, including religiosity, matter as well (House et al., 1990; Zuckerman, Kasl, & Ostfeld, 1984).
The current study examines how several measures of religiosity associate with total and disability-free life expectancy (TLE/DFLE) among older persons in Taiwan. The study advances the literature on religiosity and health by attending to two issues that have been insufficiently addressed. The first is the degree to which religiosity associates simultaneously with mortality and disability. Part of the attractiveness of examining mortality and disability together as DFLE is that it permits a contrast between quantity and quality of life (Robine & Ritchie, 1991). Defined in a conventional fashion—as having problems or an inability conducting tasks necessary for daily survival, with tasks measured as activities of daily living (ADLs; Katz, Ford, Moskowitz, Jackson, & Jaffee, 1963; Verbrugge & Jette, 1994)—studies are continually showing that living longer does not necessarily mean living longer without disability (Crimmins & Beltrán-Sánchez, 2011; Jagger et al., 2009). Thus, debates around quantity versus quality of life have become central to studies of aging societies experiencing increases in longevity. The debate often revolves around whether increasing longevity tends to proceed with a “compression of morbidity,” or the constriction of disabled time, or time lived with chronic disease, into short periods at the end of life (Zimmer, Hidajat, & Saito, 2015). If a compression of morbidity is occurring, then prevalence of chronic disease is in decline, or once there is an onset, the disease is less disabling. This could be due to new medical treatments that reduce severity, result in earlier detection, or general advances in public health such as education, exercise, diet, and so on. (Crimmins & Beltrán-Sánchez, 2011; Leveille, Guralnik, Ferrucci, & Langlois, 1999; Robine, Mormiche, & Sermet, 1998).
Religiosity would be expected to result in improvements in DFLE if it causes delay of onset of chronic disease, resulting in longer life, while rendering diseases that are experienced less disabling, resulting in a longer proportion of life lived without disability. There is good evidence for the former as religiosity has been shown to associate with longer life (Dupre, Franzese, & Parrado, 2006; Hummer, Benjamins, Ellison, & Rogers, 2010; Hummer, Ellison, Rogers, Moulton, & Romero, 2004; Jarvis & Northcott, 1987; Li, Stampfer, Williams, & VanderWeele, 2016). In contrast, studies linking religiosity and disability are fewer and mixed (Idler & Kasl, 1992, 1997; Musick, 1996; Selway & Ashman, 1998). The relationship between religiosity and disability-free life is therefore unclear.
If religion does affect the disabling nature of disease, there are a number of mechanisms through which this may occur. One has to do with social networks (Kodzi, Gyimah, Emina, & Ezeh, 2011; Koenig et al., 1997; Krause, Ingersoll-Dayton, Liang, & Sugisawa, 1999; Pirutinsky et al., 2011). Religious participation allows for establishment and continuation of social networks of individuals who share common values, interests, and concerns and provide support and practical assistance; and social support has long been considered a determinant of health (House, Landis, & Umberson, 1988; Kaplan, Cassel, & Gore, 1977). A second is through the promotion of healthy behaviors (Hill, Ellison, Burdette, & Musick, 2007; Strawbridge, Shema, Cohen, & Kaplan, 2001). Certain religions, for instance, prescribe or otherwise advocate specific behaviors like abstaining from tobacco and alcohol use. Particularly in Eastern traditions, religion promotes practices like meditation and mindfulness that have impacts on stress reduction (Davidson et al., 2003; Ernst et al., 2008; Ledesma & Kumano, 2009). A third is the impact of religion on psychological and mental health (Eichhorn, 2011; McCullough & Larson, 1999; Sinnewe, Kortt, & Dollery, 2015). This may involve life satisfaction, depression, and the ability to cope with difficult circumstances (Krause, Ellison, Shaw, Marcum, & Boardman, 2001; Pargament, Koenig, & Perez, 2000).
The second issue addressed in this study is whether and how associations between religiosity and TLE/DFLE vary across dimensions of religiosity. Religiosity is a complex multidimensional construct. Well-cited attempts at identifying constituents of religiosity, including within a Taiwanese setting, have led to little consensus around dimensions that best represent the construct (Clayton & Gladden, 1974; Cornwall, Albrecht, Cunningham, & Pitcher, 1986; Idler et al., 2003; Kendler et al., 2003; Krause, 2004; Yeager et al., 2006). Yet, several overarching notions about the dimensionality of religiosity emerge out of this literature. One is that religious participation, which relates very closely with attendance at religious services, is a common and important component that is usually reliably measured (Li et al., 2016; Musick, House, & Williams, 2004; Sullivan, 2010). Participation is a good expression of public religious activity. Private activity, in contrast, which can be measured by prayer and/or meditation practice, is often conducted at home or in other places without the oversight of a religious institution (Fang et al., 2010; Helm, Hays, Flint, Koenig, & Blazer, 2000). Private expressions therefore are not necessarily accompanied by attendance. Then there are conviction and faith aspects of religiosity. These may be highly personal and less actionable but more intrinsic, associated with ideology and philosophy, and provide principals that may be useful as coping mechanisms during difficult times (Cornwall et al., 1986; Kendler et al., 2003; Nicholson, Rose, & Bobak, 2010; Nooney & Woodrum, 2002; Pargament, 1997). Data used in the current study allow us to measure three religiosity dimensions: public practice or participation, private practice, and religious coping.
It is possible that DFLE responds to certain dimensions of religiosity and not others. The majority of published research on religiosity and health considers samples dominated by Judeo-Christian traditions where participation generally associates with a number of health outcomes (Li et al., 2016; Selway & Ashman, 1998). A recent study in fact demonstrated that participation, more so than stated importance of religion, related to total and disability-free life in a sample of U.S. men and women (Ofstedal, Chiu, Jagger, Saito, & Zimmer, 2018). There could be reverse causality at work here. The more disabled a person is, the less likely they are to be mobile enough to engage in public displays of religiosity. Those more disabled may engage in private practice through prayer or meditation. Such practices may provide mental health benefits such as stress reduction, increase in optimism, life satisfaction, and generally an ability to cope with their disability, all of which can trigger biological functions that influence mortality (Anderson, Liu, & Kryscio, 2008; O’Laoire, 1997; Sudsuang, Chentanez, & Veluvan, 1991). While there are likely impacts of prayer on mental health, the concomitant impacts on disability are unclear. Consider, however, that the current study takes place in Taiwan where the dominant religions are more so than western-based practices organized specifically around private dimensions of religiosity like meditation (Lutz, Slagter, Dunne, & Davidson, 2008). Being normative, private practice is likely engaged across a broad spectrum of society and religious followers, not just those with already disabling conditions. As such, we might expect both public and private expressions of religiosity to be associated with both longer life and longer disability-free life.
The analysis to follow considers the contextual nature of the older population in Taiwan as it relates to ethnicity. Many older persons in Taiwan migrated from Mainland China after the Chinese Communist Revolution in 1949. The result today is a division of the People’s Republic of China (Mainland China) and the Republic of China (Taiwan). Those from the Mainland have distinct characteristics that distinguish them from other Taiwanese (Zimmer, Martin, & Lin, 2005). They are less religious; a characteristic typical of those coming from a communist system of governance. Mainlanders tended to be provided jobs in the government sector when arriving in Taiwan and because of this had better access to health coverage than others. Mainlanders are also generally in better health due to access to health care and early life training as soldiers.
Method
Data and Sample
Data come from three waves (1999, 2003, and 2007) of a longitudinal data collection project, partially funded by the National Institute on Aging, and initially titled “The Study of the Health and Living Status of the Elderly in Taiwan” (Chang & Hermalin, 1989). The project began with a survey of 4,049 Taiwanese aged 60+ in 1989. The sample was drawn using a multistage probability design with registers that included institutionalized. The intent was to provide a database that would allow for examination of social, economic, physical status, and other characteristics of elders in Taiwan. Survivors from the 1989 cohort were followed up in 1993, 1996, 1999, 2003, 2007, and 2011. In 1996, a cohort aged 50 to 67 was added to expand and fill in the age range. A third cohort was added in 2003. Later waves introduced biomarker measures. This portion of the study became the Social Environment and Biomarkers of Aging Study (SEBAS; Goldman, Lin, Weinstein, & Lin, 2003).
The 1999, 2003, and 2007 waves were chosen for this article for several reasons. First, the 1999 survey is the only one to include a range of religiosity items that allow measurement of several dimensions. Second, measures for disability and valid mortality data are readily available over these waves. Disability items were repeated identically. Mortality from 1999 to 2007 was monitored through the government’s death registry and is virtually complete. Only 45 of 4,127 individuals are dropped because mortality status is uncertain. Third, the age range of the sample in 1999 allows estimates across several life course stages. This study includes those 55 and older. Use of data from this project beyond 2007 requires researchers run statistical programs at the government’s data center in Taipei, which makes data beyond 2007 restrictive.
Expectancy estimates consider each baseline and follow-up to be a single observation, with the interval referred to as a transition period. The 1999 wave contains 3,891 individuals age 55+ with one or more valid follow-up, meaning that mortality and/or disability status is known in 2003, 2007, or both. For 3,781 there is a follow-up in 2003, which is a 4-year transition period. For 110, information in 2003 is missing but they are followed up in 2007 for an 8-year period. Then, 3,260 individuals with 1999 data that survived and were observed in 2003 were observed again in 2007 for another 4-year transition period. Summed, there are 7,151 observations, all but 110 of which consider 4-year transition periods.
Measures
Mortality and disability
Estimating TLE/DFLE requires baseline disability-status and follow-up survival and, if alive, disability-status, for each individual per transition period. Wave-to-wave mortality was confirmed by referencing the Taiwan Death Registry. To assure representativeness, sample life expectancies were compared with those published by the Taiwan Directorate General for Accounting and Statistics. The two are close. Published life expectancy in 2003, the midpoint of the current study, is 27.8 for females and 24.4 for males. The sample estimates are 28.6 for females and 24.6 for males.
Disability is based on ADLs (Katz et al., 1983). Those categorized as disability-free report having no difficulty conducting any of the following by themselves, with no help from devices: bathing, dressing and undressing, eating, getting out of bed, moving about inside the house, going to the toilet. Disabled are those who report difficulty with one or more of these activities.
Religiosity
Respondents were asked how frequently they attend religious services. This question entails practicing outside the home in an institutionalized setting and therefore it is referred to as the public dimension of religiosity. A three category variable is constructed using responses, often, sometimes, and rarely/never.
Respondents were asked how frequently they worship god or Buddha at home. Since such pursuit involves practicing on one’s own and away from a public institution, this dimension is referred to as private religiosity. The variable is constructed with categories often, sometimes, and rarely/never.
Respondents answered three questions pertaining to difficult times. The items were praying or meditating when having difficulty, asking guidance of a higher power when faced with an important decision, praying or meditating to relieve worry or stress. Response categories were often, sometimes, rarely and never. These scores were summed, standardized, and divided as nearly as possible into three categories labeled as low, middle, and high. This measure is the religious coping dimension.
The three religiosity dimensions are correlated but not to a degree that indicates any two represent the same domain. The highest correlation, when omitting the unaffiliated, is .32 between coping and public dimensions.
The survey also asked respondents about affiliation. About 14% reported no affiliation, 53% Taoist, 28% Buddhist, and 5% other. Unaffiliated are not asked all of the follow-up religiosity questions. For this reason, a category is added to each religious item, and it is labeled as unaffiliated.
The measures of religiosity described above are not derived directly from previously constructed or tested scales, yet they correspond with those constructed in previous formations based on U. S. and other Western data (Clayton & Gladden, 1974; De Jong, Faulkner, & Warland, 1976; Fetzer Institute 2003; Kendler et al., 2003). In particular, they are congruent with Cornwall et al.’s (1986) dimensions of religious belief, personal religiosity, and institutional religiosity and Nicholson et al.’s (2010) dimensions of attendance, private prayer, and religious self-assessment.
Covariates
Our models adjust for Mainlander status, education, and baseline health status, as well as a series of covariates that represent three well-established pathways through which religion often impacts health outcomes: social network variables, behaviors, and psychological well-being (Strawbridge et al., 2001).
Mainlander status is dichotomous. Education is measured as none, some, or completed primary and more than primary. Self-assessed health has categories good/very good, average, and poor.
There are five social network variables. Respondents were asked about the number of friends with whom they maintain frequent contact. This is categorized into relatively equal distributions: none, 1 to 3, 4 to 8, and 9+. Second, respondents were also asked about the number of relatives with whom they maintain frequent contact. This is categorized similarly into relatively equal distributions. Third is co-residing with an offspring. Fourth is marital status, which is coded as married or other. The fifth measure is an emotional support index derived from four survey questions that ask individuals the degree to which family, relatives, or friends are willing to listen; make you feel loved; can be counted on; and satisfaction with level of emotional support received from family or relatives. Each of these items was responded to on a 5-point scale. Scores for each item are summed then standardized to a mean of zero and standard deviation of one.
Religious involvement is often linked to healthy lifestyles and behaviors (Hill et al., 2007). In this study, we adjust for smoking, exercise, alcohol consumption, and consumption of fruits and vegetables. Smoking is never, current smoker, or former. Exercise is rarely/never, at least weekly, and daily. Alcohol consumption is none, less than daily, and daily. Fruit and vegetable consumption is coded as consumed daily or not.
Religion’s link with mental health may also be a factor that explains its favorable relationship with physical health (Koenig, 2013). Two psychological well-being variables include first, the Center for Epidemiologic Studies–Depression Scale (CES-D) score, which is a commonly used scale of depression that has been validated across numerous countries and cultures and especially among Chinese (Boey, 1999; Gupta & Yick, 2002; Radloff, 1977). The second is a life satisfaction score derived from 12 questions such as has your life been better than most people’s; are you satisfied with life; and, do you find what you do to be interesting. For both, total scores are standardized to a mean of zero and standard deviation of one, with higher scores indicating healthier psychological well-being.
Descriptive statistics for all study variables are provided in Table 1.
Unweighted Descriptive Statistics for Study Variables at Baseline (N = 3,891).
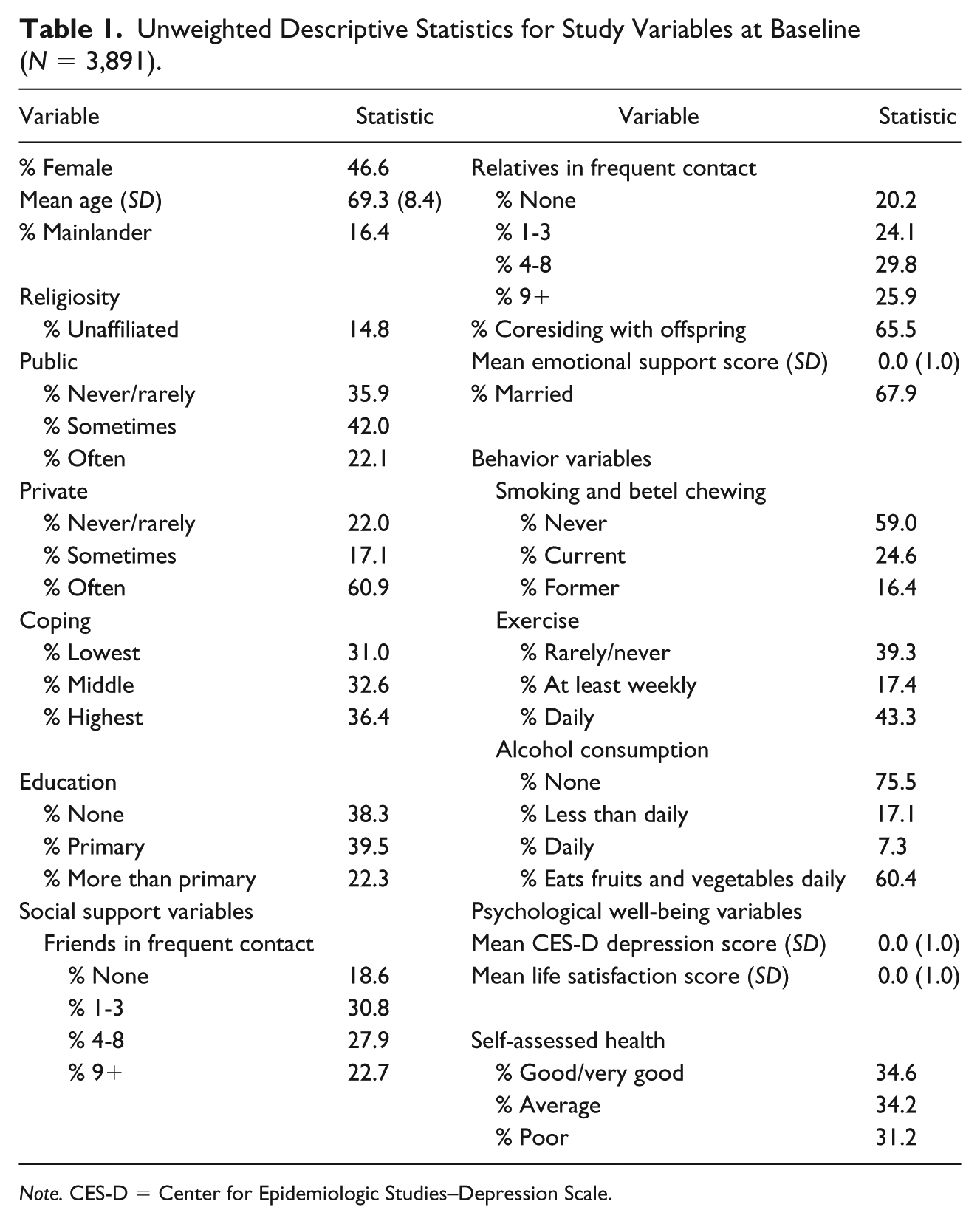
Note. CES-D = Center for Epidemiologic Studies–Depression Scale.
Estimation Strategy
Estimation of TLE, DFLE, and disabled life expectancy (DLE) uses the Stochastic Population Analysis for Complex Events (SPACE) software (Cai et al., 2010). SPACE is a multistate life table (MSLT) method (Saito, Robine, & Crimmins, 2014). Its advantage over other MSLT approaches is that it can handle a large number of covariates, an important feature for the current study given the large number of variables entered in models, and its ability to derive standard errors and confidence intervals.
MSLT approaches to estimating TLE, DFLE, and DLE involve two stages. In the first stage, a regression is fitted to determine the probability of a transition from any starting state (e.g., disabled or not disabled) to any outcome state (e.g., disabled, not disabled, or deceased) across any two waves of data. In SPACE, these probabilities are derived from separate multinomial regressions, each of which includes a sample of those beginning in one of the baseline states. Figure 1 in supplementary materials diagrams the possible transitions in the current study and Figure 2 in supplementary materials shows the transition probabilities that result from the multinomial regression used to derive baseline estimates in the current study, which is based on models using only age as a predictor and stratifying by sex.
In a second stage, transition probabilities are used as input for MSLT calculations. For SPACE, this is done as a microsimulation that tracks disability status from 1 year to the next for a hypothetical cohort of individuals. The simulation begins with a hypothetical cohort of 100,000. An initial health status is applied to each hypothetical individual based on baseline probabilities (either disabled or not disabled). Then, based on the probabilities determined in the first stage, each hypothetical person is run through a year-by-year simulation, with a transition across disability states or death in each year being a function of those probabilities. Each hypothetical individual is tracked until death. Summary statistics for the simulations result in estimates of the TLE, DFLE, and DLE.
For each estimate, a standard error is calculated by way of a bootstrapping method that executes repeated estimates through random draws. This study uses a bootstrap of 100, which through experience is deemed sufficient to produce stable standard errors.
Besides point estimates, our analysis considers additional statistics that help to assess whether and how TLE and DFLE vary across levels of religiosity. First, TLE and DFLE estimates are used to calculate the percent of life expected to be lived in a disability-free state (simply DFLE/TLE × 100). Second, by subtraction, we derive the difference between estimates of TLE, DFLE, DFE, and percent of life disability-free across levels of religiosity. This provides a way of determining the extent to which increases in religiosity provide a TLE, DFLE, or percent of life free of disability advantage. Standard errors for these procedures are determined through bootstrapping. To test whether differences in estimates across religiosity levels are statistically significant, 95% confidence intervals for the distribution of the differences are constructed. These confidence intervals display the 2.5th to the 97.5th percentile for the bootstrapped distributions.
DFLE procedures generate a vast amount of results. Part of this is because TLE, DFLE, and DLE estimates can be derived for all years of age, across both sexes, and across all levels and measures of religiosity. For an efficacious presentation, results are shown for those aged 70, which is close to the mean of the sample. Patterns for those at other ages run parallel, with younger ages having higher TLE and therefore generally higher DFLE and DLE. Some of these additional results are provided in supplementary materials.
Models Tested
The first model, called a baseline, includes no controls and provides population average estimates of TLE, DFLE, and DLE by age stratified by sex. When we begin to look at how religiosity serves to transform the estimates, we start with a model that adds Mainlander status and one of the religiosity dimensions to the baseline model, that is, public religiosity, private religiosity, or religious coping. We call this Model 1 unadjusted for control variables. To assess whether religiosity functions differently for Mainlanders versus non-Mainlanders, all Model 1s were estimated with Mainlander × religiosity interactions. None of the interactions were significant, indicating that although Mainlanders may not have the same level of TLE or DFLE as others, the way in which these estimates change by religiosity is the same for Mainlanders versus others. Because of a lack of interaction, all models are estimated with only a main effect for Mainlander.
Additional models are estimated as follows: (a) Model 1 + education; (b) Model 1 + social network variables; (c) Model 1 + behavior variables; (d) Model 1 + psychological well-being variables; (e) Model 1 + self-assessed health; (f) all variables. As different variables are added to the unadjusted Model 1, transition probabilities change, and so will point estimates, providing an assessment of the degree to which added variables explain results found in the unadjusted model.
Results
Expectancies and Transition Probabilities by Age and Sex
A standard from which to assess later estimates is provided in Figure 1, which displays base model estimates. The sum of DFLE and DLE, or height of the bars, is TLE. Also shown is percent of remaining life disability-free. Expected patterns result: TLE declines with age, DFLE declines with age, percent of life disability-free decreases with age, females live longer but a lesser proportion of life disability-free in comparison with males. For instance, at age 55, males can expect 24.6 more years, of which 22.7 or 92% are disability-free. In contrast, a 55 year-old female can expect 28.6 more years, which is 4.0 years more than the same-aged male. Of these years, 86%, or 24.6, are disability-free, meaning that the 4.0 years life-expectancy advantage for a 55 year-old woman can be broken into 1.9 extra disability-free years and 2.1 extra years with disability. By age 95, males expect 4.2 years of life, 1.5 of which or 36% of which are life disability-free. By age 95, females expect 4.7 years, but only 1.1 or 23% are disability-free. Supplementary materials Table 1 provides specific estimates for TLE, DFLE, and DLE for each single year of age.

Base model results showing expected total, disability-free and disabled years of life, and percent of life disability-free, by age and sex.
Point Estimates by Levels of Religiosity
Table 2 shows estimates for three statistics for males and females at age 70 derived from Model 1 (which controls for Mainlander status and includes religiosity dimensions): TLE, DFLE, and percent of life disability-free. Public and private practices are divided into rarely/never, sometimes, and often. Coping is divided into low, middle, and high. Each religiosity measure includes a category for unaffiliated. Estimates include standard errors in parentheses.
Total Life Expectancy Point Estimates, and Percent of Total Life Expected to be Disability-Free, at Age 70, Derived From Model 1 Unadjusted, by Level of Religiosity, Sex, and Religious Dimension, Showing Standard Errors in Parentheses.
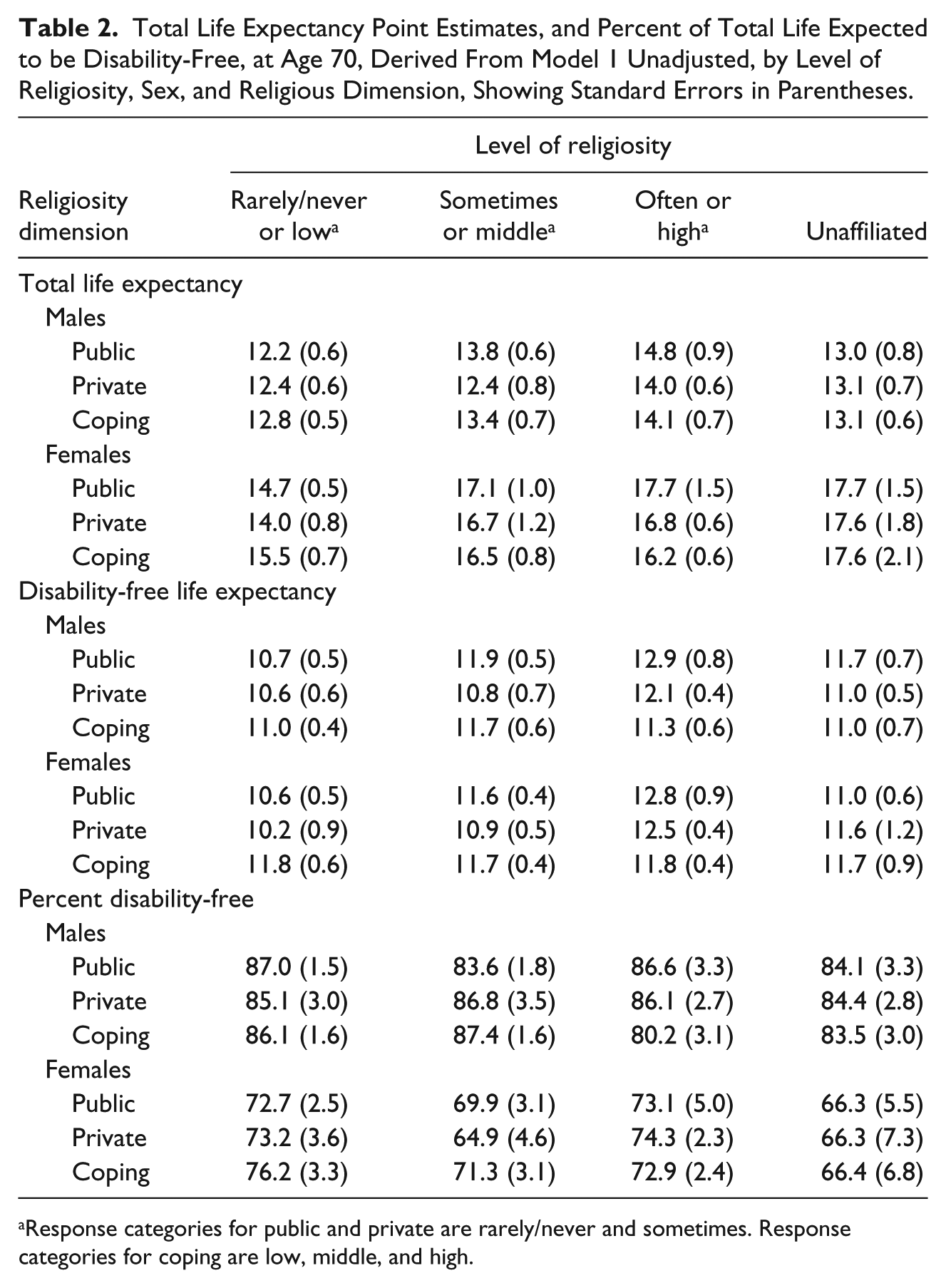
Response categories for public and private are rarely/never and sometimes. Response categories for coping are low, middle, and high.
For TLE, there is a clear gradient across levels of public religiosity for both males and females. For instance, females who engage rarely or never in public religious activity can expect to live 14.7 more years, which means living to age 84.7. Those who engage sometimes can expect 17.1 additional years of life, or a gain of 2.4 years over their rarely or never participating counterparts. Those engaging often can expect 17.7 more years, which is 0.6 more than those participating sometimes and 3.0 more than those participating rarely or never. While TLE is higher for females than males, patterns for public religiosity are similar. For instance, for males, the change in life expectancy is from 12.2 to 13.8 to 14.8 moving from lowest to highest levels of public religiosity participation. There are also gradients across private religiosity. Males who engage in private religiosity often live 14.0 years compared with 12.4 years for those who engage rarely or never. The same comparison for females is 16.8 versus 14.0.
Gradients for religious coping differ. Religious coping increases life expectancy for males, but has no association for females.
TLE for unaffiliated males is generally about 13 years, which is a total in between the highest and lowest point estimates across levels of religiosity. But, TLE for unaffiliated females is about 17.7 years, which is higher in comparison with other estimates. Being unaffiliated therefore appears to be benign for males but advantageous for females.
Estimates for DFLE at age 70 for males and females generally concur with TLE in that there are gradients across public and private religiosity and less clarity across religious coping. For instance, the increase in DFLE for females across categories of public activity is 10.6 to 11.6 to 12.8 years moving from the lowest to highest level of engagement. For private activity, the numbers run from 10.2 to 10.9 to 12.5. The same pattern exists for males. In contrast, there is not much difference in DFLE estimates across low, middle, and high levels of coping for either males or females.
When DFLE and TLE are converted in to a percent of life expected disability-free, there is barely any gradient. For instance, males who engage in public religious activity never/rarely, sometimes, and often expect 87.0%, 83.6%, and 86.6% of life to be disability-free, respectively. As such, while public activity increases total and disability-free life for males, the increases are moving in tandem; when religiosity results in more years of total life, the gain is divided proportionately into disability-free and disabled years. The exception is for males engaging in religious coping. There is somewhat of a negative trend here where those who have the highest level of coping live the smallest proportion of life disability-free.
Although females have higher TLE, as indicated in the upper panel, the percent of life disability-free for females is much lower than it is for males. For instance, males who engage in public religious activity never/rarely can expect 87.0% of remaining years to be disability-free compared with 72.7% for their female counterparts.
More detailed results can be found in Table 2 of supplementary materials, which provides point estimates and standard errors for males and females aged 55, 70, and 85.
Advantage Accrued to Those With Higher Levels of Religiosity
The results in Table 2 can be viewed as the net advantage in years of life when moving from lowest to highest level of religiosity across dimensions. We determine this number simply by subtracting estimates for those in the highest category from the lowest category. Results are shown in Figure 2, which also includes 95% confidence intervals as to assess whether gains or losses in years are statistically significant. The clear finding here is that public and private activity relates to significantly more years of total and disability-free life for males and females. For instance, males who engage in public religious activity often will live about 2.5 more total years and 2.0 more disability-free years than their counterparts who engage rarely/never, with 95% confidence intervals indicating that both of these estimates are statistically significant. In contrast, most of the other comparisons are nonsignificant. DLE therefore does not change significantly depending upon level of religiosity. One exception exists. Higher religious coping associates with significantly greater years of disabled life for males.
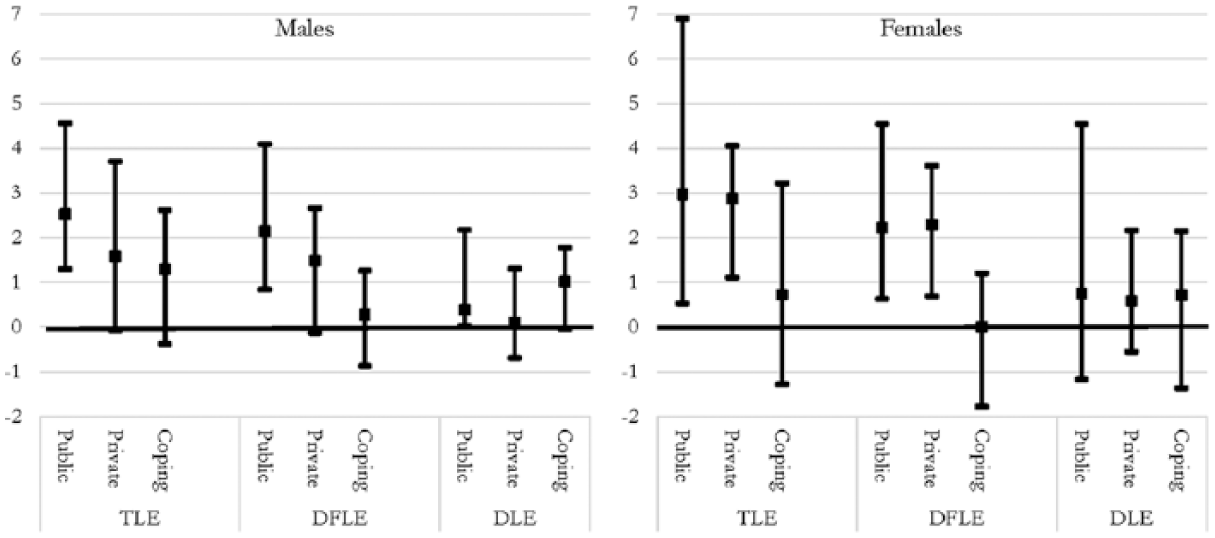
Net gain or loss in TLE, DFLE, and DLE years at age 70, comparing the highest and lowest levels of religiosity, and 95% confidence intervals of these gains or losses, by sex and religiosity dimension.
How the net gains and losses in TLE, DFLE, and DLE translate into percent of life expected disability-free is provided in Figure 3, which shows point estimates for the difference in the percent between highest and lowest level of religiosity and the 95% confidence intervals. While those engaging in public and private activity often have a total and disability-free life advantage over others, the figure indicates that this advantage does not translate into a percent of life disability-free. The only finding that nears significance is religious coping among males where those who have a high level live a smaller percent of life disability-free, a function of religious coping relating to significantly more years of disabled life for this group.
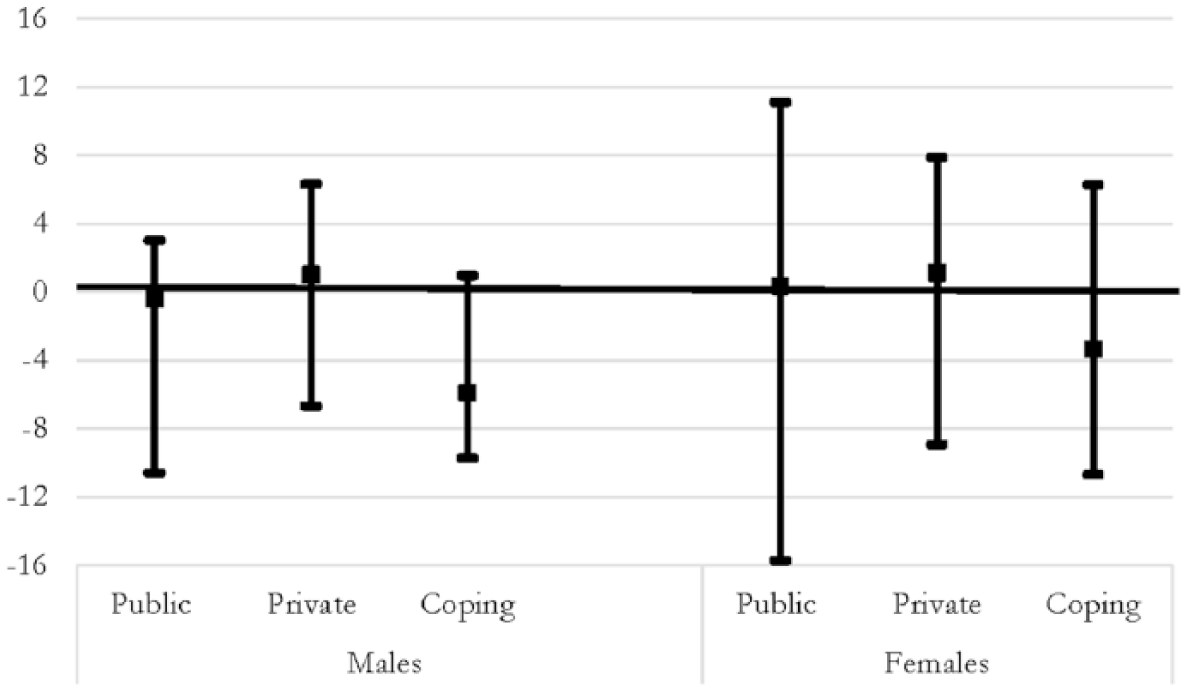
Net gain or loss in percentage points for life disability-free at age 70, comparing the highest and lowest levels of religiosity, and 95% confidence intervals of these gains or losses, by sex and religiosity dimension.
In Figure 4, we present the findings for all models to determine whether any mechanisms explain the gains or losses in TLE, DFLE, and DLE. Model 1 is the model we have been examining thus far; controlling only for Mainlander status. Models 2 through 6 add additional covariates education, social network, behaviors, psychological well-being, and self-assessed health characteristics, respectively. Model 7 includes all covariates simultaneously. Specific numbers can be found in Table 3 of supplementary materials.
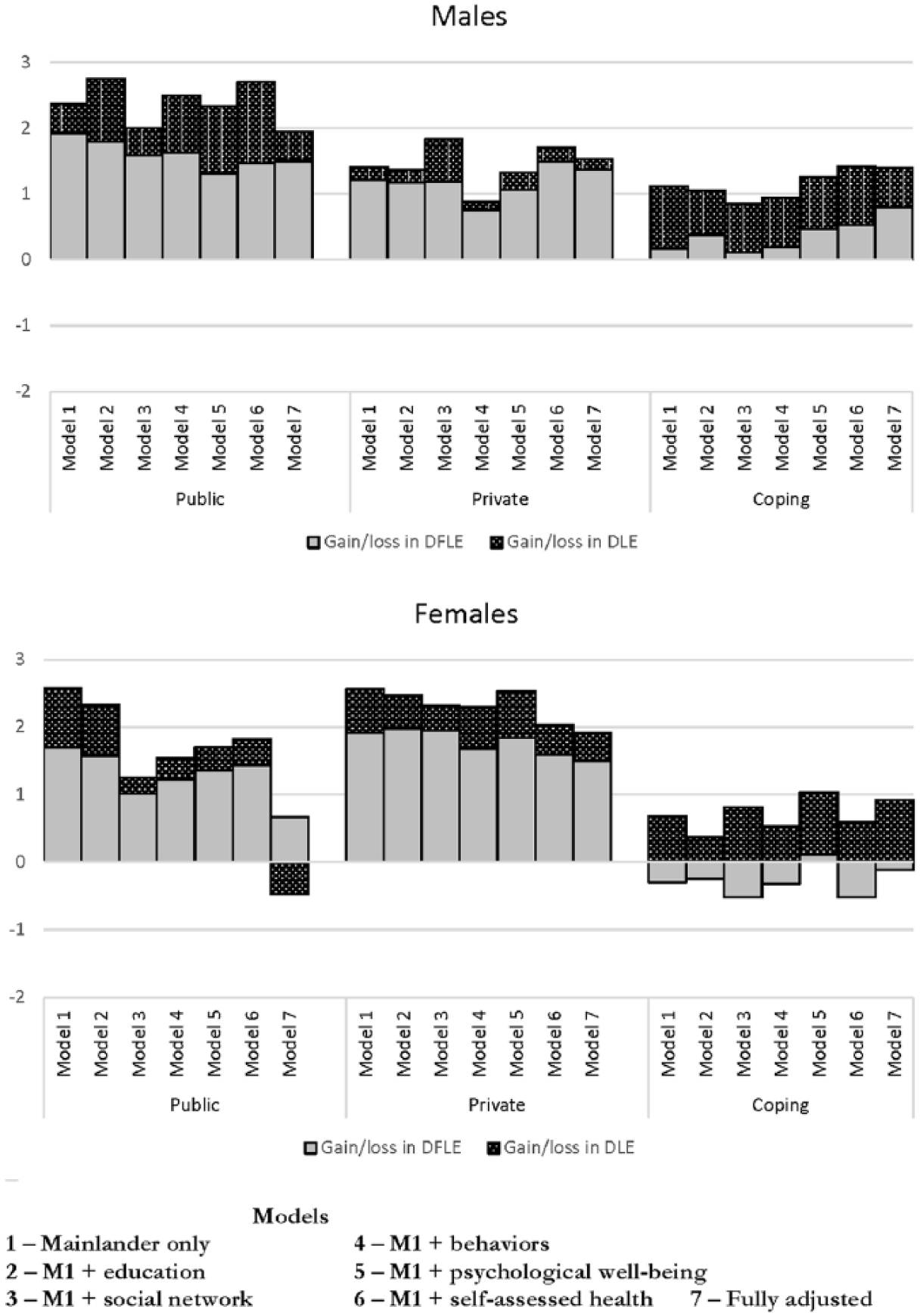
Net gain or loss in disability-free and disabled life expectancy at age 70, comparing the highest and lowest levels of religiosity, across models, by religiosity dimension and sex.
For males, the gains in DFLE, DLE, and TLE for higher levels of public, private, and coping religiosity remain consistent across models. The losses for higher levels of religious belief are also consistent across models. For example, looking at public religiosity, the gain in DFLE across models is 2.1, 2.0, 1.8, 1.8, 1.5, 1.7, 1.7, respectively. The gain in TLE, obtained by summing the gain in DFLE and DLE, across models is 2.5, 3.0, 2.2, 2.7, 2.5, 2.9, 2.0, respectively. Therefore, for both DFLE and TLE there is a slight reduction in the advantage as covariates are added, but the overall findings do not change. The conclusion for females is similar in that gains in DFLE and TLE for those reporting higher levels of public and private religiosity decline only modestly when adding covariates. For instance, looking at private religiosity, the gain in TLE across models is 2.9, 2.8, 2.6, 2.5, 2.8, 2.3, 2.1, respectively. Gains in TLE are negligible when considering religious coping, and this result is consistent regardless of which covariates are in the model.
On balance, the figure shows that whatever advantage (or disadvantage) is accrued by higher levels of religiosity is not explained very well by the covariates and the mechanisms adjusted for in across models. If anything, there is a small reduction in gains from public religiosity when considering social network characteristics and a small reduction in private religiosity among males when considering behaviors.
Discussion
While there are studies to the contrary, a long-standing literature indicates religiosity is, on balance, salutary. However, this literature, which dates back decades if not centuries, leaves some important issues unsettled (Ellison & Levin, 1998; George, Ellison, & Larson, 2002; George et al., 2000; Krause, 2011; Zimmer et al., 2016). The current article addressed two of these using a sample from Taiwan. First earlier studies have shown that longevity benefits from religious involvement, but living longer does not necessarily mean more years without disability, and the degree to which religion associates with disability and mortality simultaneously has been infrequently examined. Second, most literature attesting to a salutary influence of religiosity measures it as frequency of attendance. Yet, religiosity is a complex and multidimensional construct, and a number of dimensions have been identified in earlier classifications. The current study addressed these issues directly while examining data from a sample that identify with religions not typically considered in past studies of religion and health; Taiwanese, aged 55 and older, who, except for a small percentage of unaffiliated, identified as Taoist or Buddhist; and considering a broad range of covariates commonly thought to be the mechanisms through which religion impacts upon health.
Below are the main findings, organized according to dimensions of religiosity.
Public religiosity: There is a considerable TLE/DFLE advantage for those who participate more frequently in public religiosity, measured as frequency of attendance. Seventy-year old males who participate “often” live about 2½ years longer than those who participate “never,” of which a little more than 2 years are disability-free. For females, the gain is about 3 years of which about 2¼ are disability-free. Although the percentage of life disability-free does not change with more public religious practice, the proportionate gain in both total and disability-free years supports the notion that both quantity and quality of life is impacted upon by frequency of attendance to health in the case of Buddhist and Taoist faiths within an Asian setting.
Private religiosity: The benefits of religiosity expand beyond public attendance to private modes of expression, measured in this study by frequency of worship and prayer. While in part this may be reflecting a congruence between public and private practice, a Pearson’s correlation of.32 indicates private and public are somewhat different constructs. As such, an individual does not have to go to a place of worship to realize the health benefits of religious involvement. A 70-year old male who engages in private religiosity often has a total life advantage over those engaging never of about 1½ years, most of which are disability-free. For females, the advantage is closer to 3 years, about 2¼ of which are disability-free. Like public religiosity, those engaging often in private religiosity live longer than others and gain a proportionate number of years disability-free. We conclude that Taiwanese aged 55 and older gain similarly practicing religion by attending services or engaging in solitary practice.
Religious coping: For males, a higher level of religious coping is associated with more years of life, but the years gained are disabled years rather than disability-free years. Religious coping therefore is the one dimension wherein there is evidence that quantity and quality of life may be impacted upon differently. To be specific, 70-year old males with the highest level of religious coping live 1.3 years longer than their low-level counterparts, and of these years, 1.0 are with disability and only 0.3 are disability-free. The net result is about a 6 percentage point decrease in percentage of life disability-free. Females gain only about ¾ of a year of life through high levels of religious coping, which is not a statistically significant increase. However, it is worth noting that all of this small gain for females is disabled rather than disability-free life. There are a couple of ways in which this result could be manifest. One is suggested by Musick (1996), who proffered that religion may be a more efficacious determinant of health for those who suffer from physical health problems due to its “comfort role.” Therefore, those with physical health problems already may be more likely to engage in religious coping. The findings then indicate longer life in a disabled state. A second is the possibility that among those with health and disability problems, engagement in religious coping affects psychological conditions that may accompany poor health, such as stress, optimism, and hope for the future. This could trigger biological functions that serve to lengthen life, as has been suggested in previous research (Hank & Schaan, 2008; Jantos & Kiat, 2007; Poloma & Pendleton, 1989), but do little for disability recovery.
It is somewhat puzzling that mechanisms controlled for across a number of models explain almost none of these associations as results are robust to model specification. Therefore, greater levels of public and private religiosity increase life and DFLE consistently regardless of the covariates entered into sequential models. Reverse causality is one possibility in that it may just be that healthier people are more likely to engage in religious activity. As noted above, reverse causality may also explain the connection between religious coping and percentage of life disability-free. We tested for this with sensitivity analyses that divided the sample into those who began without disability at baseline and those who began with disability. Results are provided in supplementary materials Table 4. The tests did not prove to be explanatory as the benefits of religiosity remained stable when examining only those with no disability at baseline. We conclude that there are other mechanisms that explain this association that are left uncontrolled.
Our study adds to a very small number of earlier studies of religiosity and health in East Asian countries. Zeng, Gu, and George (2011) found little connection between religious participation and mortality among Chinese elders. Earlier Taiwan-based studies by Yeager et al. (2006) and Hidajat, Zimmer, Saito, and Lin (2013) showed associations in Taiwan differed across health outcomes. Liu, Schieman, and Jang (2011) concluded that religious beliefs and supernatural activities in Taiwan associated with more distress, while prayer was associated with less. Our study adds to these mixed findings. We find that religiosity results in overall gains to total life, but whether these gains associate with more disability-free years depends on the dimension being considered. Although frequency of attendance is the most common measure of religiosity, there are previous studies that, like ours, have suggested that the salutary influences differ across dimensions (Buck et al., 2009; Kendler et al., 2003; Nicholson et al., 2010). Since the dimensionality of religiosity has not been fully agreed upon, studies tend to define religiosity in different ways making comparisons across these studies difficult. Furthermore, the associations between religiosity and health may not only differ across dimensions but also the influence of different dimensions may differ across populations and traditions, further complicating the nexus between religiosity and health. As evidence, recent findings by Stroope and Baker (2018) indicated that the relationship between religion and health is stronger in more religious environments. While their study considered a U.S.-based population, it suggests the importance of contextualization in understanding the influence of religiosity on health.
There are a number of limitations to the current study. Measuring religiosity is difficult due to the complex nature of the construct and any measure of religiosity will be imperfect. Response categories are also at times difficult to distinguish. The difference between often and sometimes, for instance, is subjective when it comes to conducting religious activity and the distance between these categories will not be consistent across respondents. The data source we used in this analysis does not indicate that further explanation or guidelines were given to the respondent. Moreover, models that include potential mechanisms do not necessarily cover the full range of mechanisms that have been considered as explanatory factors. Our DFLE estimates using SPACE software require substantial computation time which limits the number of bootstraps that might refine the variability estimates.
At the same time, the strength of our analysis is the combination of mortality with disability and the implication that religiosity is multidimensional and represents different constructs that can have different associations with disability and mortality. Public and private religiosity in our study increased both total and disability-free life, while coping religiosity increased total and disabled life. Religiosity is a multifaceted concept that can take on different meaning across different contexts. While religion is clearly influential, the social sciences, despite many years of study, are far from understanding its force on health outcomes.
Supplemental Material
supplementary_materials – Supplemental Material for Religiosity Dimensions and Disability-Free Life Expectancy in Taiwan
Supplemental Material, supplementary_materials for Religiosity Dimensions and Disability-Free Life Expectancy in Taiwan by Zachary Zimmer, Chi-Tsun Chiu, Yasuhiko Saito, Carol Jagger, Mary-Beth Ofsteda and Yu-Hsuan Lin in Journal of Aging and Health
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by a grant from the John Templeton Foundation (grant number 57521). The first author acknowledges the support of the Social Sciences and Humanities Council of Canada through the Canada Research Chair program.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.